
Results of a Community Randomized Study of a Faith-Based Education Program to Improve Clinical Trial Participation among African Americans

Abstract
:1. Introduction
2. Experimental Section
2.1. Design
2.2. Participants
2.3. Intervention
2.4. Survey Measures
2.5. Measures of Intention to Participate in Clinical Trials
2.6. Statistical Analysis
3. Results
3.1. Sample Characteristics

{kind=link}
| Characteristics | n | % |
|---|---|---|
| Total | 221 | 100 |
| Gender | ||
| Male | 47 | 21.3 |
| Female | 174 | 78.7 |
| Age (Mean = 64, Median = 64, Standard Deviation = 7.7) | ||
| 50–59 | 62 | 28.1 |
| 60–69 | 108 | 48.9 |
| 70–79 | 41 | 18.6 |
| 80–89 | 5 | 2.3 |
| 90–99 | 2 | 0.9 |
| Missing | 3 | 1.4 |
| Education | ||
| Grade K–8 | 3 | 1.4 |
| Grade 9–11 | 10 | 4.5 |
| High School/GED | 66 | 29.9 |
| Technical/Vocations/Associates | 66 | 29.9 |
| Bachelor’s Degree | 37 | 16.7 |
| Master’s Degree | 33 | 14.9 |
| Doctorate | 6 | 2.7 |
| Income | ||
| <$20,000 | 61 | 27.6 |
| $20,001–$40,000 | 49 | 22.2 |
| $40,0001–$60,000 | 36 | 16.3 |
| $60,001–$80,000 | 20 | 9.0 |
| $80,001–$100,000 | 19 | 8.6 |
| >$100,000 | 13 | 5.9 |
| Missing | 23 | 10.4 |
| Relationship Status | ||
| Single/Never Married | 24 | 10.9 |
| Married/Domestic Partner | 102 | 46.2 |
| Divorced/Separated | 59 | 26.7 |
| Widowed | 35 | 15.8 |
| Other | 1 | 0.5 |
| Assigned Group | ||
| Intervention | 112 | 50.7 |
| Control | 109 | 49.3 |
| Characteristics | Control | Intervention | |||
|---|---|---|---|---|---|
| N | % a | N | % a | p–Value b | |
| Total | 109 | 49.3 | 112 | 50.7 | |
| Gender | 0.41 | ||||
| Male | 22 | 20.2 | 25 | 22.3 | |
| Female | 87 | 79.8 | 87 | 77.7 | |
| Age | 0.03 | ||||
| 50–59 | 25 | 23.1 | 37 | 33.6 | |
| 60–69 | 53 | 49.1 | 55 | 50.0 | |
| 70–79 | 29 | 26.9 | 12 | 10.9 | |
| 80–89 | 1 | 0.9 | 4 | 3.6 | |
| 90–99 | 0 | 0 | 2 | 1.8 | |
| Missing | 1 | – | 2 | – | |
| Education | 0.45 | ||||
| Grade K–8 | 1 | 0.9 | 2 | 1.8 | |
| Grade 9–11 | 3 | 2.8 | 7 | 6.3 | |
| High School/GED | 33 | 30.3 | 33 | 29.5 | |
| Technical/Vocations/Associates | 31 | 28.4 | 35 | 31.3 | |
| Bachelor’s Degree | 23 | 21.1 | 14 | 12.5 | |
| Master’s Degree | 14 | 12.8 | 19 | 17.0 | |
| Doctorate | 4 | 3.7 | 2 | 1.8 | |
| Income | 0.50 | ||||
| <$20,000 | 32 | 33.3 | 29 | 28.4 | |
| $20,001–$40,000 | 27 | 28.1 | 22 | 21.6 | |
| $40,0001–$60,000 | 16 | 16.7 | 20 | 19.6 | |
| $60,001–$80,000 | 8 | 8.3 | 12 | 11.8 | |
| $80,001–$100,000 | 6 | 6.3 | 13 | 12.7 | |
| >$100,000 | 7 | 7.3 | 6 | 5.9 | |
| Missing | 13 | – | 10 | – | |
| Relationship Status | 0.25 | ||||
| Single/Never Married | 10 | 9.2 | 14 | 12.5 | |
| Married/Domestic Partner | 47 | 43.1 | 55 | 49.1 | |
| Divorced/Separated | 36 | 33.0 | 23 | 20.5 | |
| Widowed | 16 | 14.7 | 19 | 17.0 | |
| Other | 0 | 0 | 1 | 0.9 | |
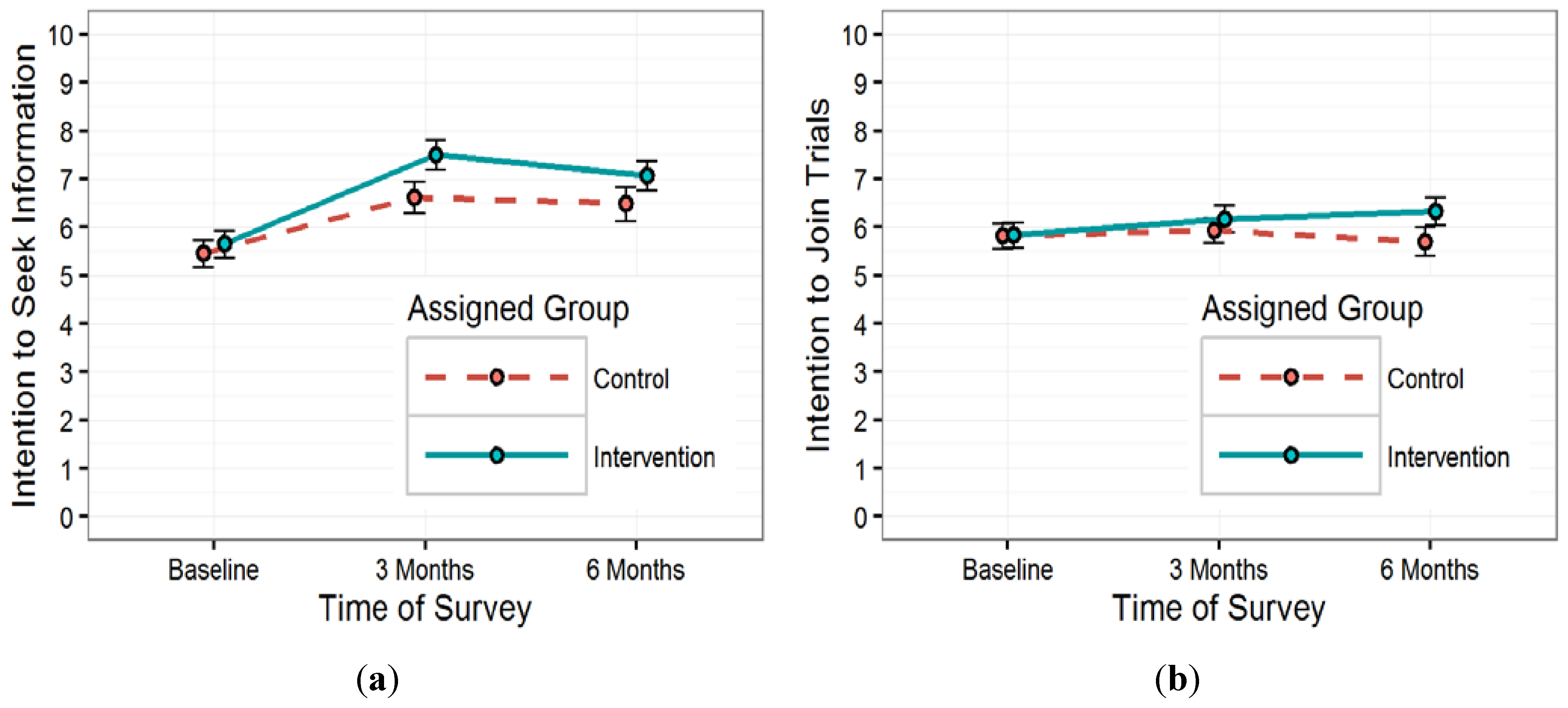
3.2. Intention to Participate in Clinical Trials

| Predictor Variable | Intention to Seek Information | Intention to Join | ||||||
|---|---|---|---|---|---|---|---|---|
| 3 Months (miss = 42) | 6 Months (miss = 43) | 3 Months (miss = 41) | 6 Months (miss = 44) | |||||
| β (95% CI) | p−value | β (95% CI) | p−value | β (95% CI) | p−value | β (95% CI) | p−value | |
| Intervention (ref = control) | 0.4 (−2.27, 3.08) a | 0.70 | 0.12 (−1.91, 2.16) d | 0.88 | 0.11 (−2.58, 2.35) b | 0.90 | 0.12 (−1.44, 1.69) d | 0.85 |
| Baseline Intention | 0.12 (−0.1, 0.34) c | 0.28 | 0.21 (−0.01, 0.43) c | 0.06 | 0.21 (0.02, 0.40) c | 0.03 | 0.12 (−0.11, 0.32) c | 0.33 |
| Age | −0.09 (−0.15, −0.02) | 0.01 | −0.11 (−0.18, −0.05) | <0.01 | −0.14 (−0.21,−0.07) d | <0.01 | −0.08 (−0.14, −0.02) | 0.01 |
| Gender (ref = male) | −0.83 (−1.96, 0.3) | 0.15 | −0.67 (−1.79, 0.45) | 0.24 | −0.76 (–1.68, 0.17) | 0.12 | −0.42 (–1.43, 0.59) | 0.41 |
| Income | 0.09 (−0.21, 0.39) | 0.57 | −0.11 (−0.41, 0.2) | 0.49 | −0.04 (−0.29, 0.21) | 0.76 | −0.27 (−0.55, 0.001) | 0.05 |
| Intervention × Baseline e | −0.14 (−0.44, 0.17) | 0.38 | −0.11 (−0.43, 0.2) | 0.48 | −0.12 (−0.40, 0.16) | 0.39 | −0.18 (−0.5, 0.13) | 0.26 |
| Intervention × Age f | --- | --- | --- | --- | −0.11 (−0.22, −0.01) | 0.04 | --- | --- |
| Mean Differences in Intention (95% CI) a | ||||||
|---|---|---|---|---|---|---|
| Assigned Group | Intention to Seek Information | Intention to Join | ||||
| Baseline and 3 Months (miss = 42) | Baseline and 6 Months (miss = 43) | 3 Months and 6 Months b (miss = 48) | Baseline and 3 Months (miss = 41) | Baseline and 6 Months (miss = 44) | 3 Months and 6 Months (miss = 46) | |
| Control | 1.08 (−0.44,2.6) | 1.02 (−0.43, 2.47) | 0.07 (−0.76, 0.9) | 0.09 (−1.15, 1.32) | −0.03 (−1.16, 1.1) | −0.18 (−1.54, 1.18) |
| Intervention | 1.98 (0.47, 3.5) * | 1.49 (0.05, 2.93) * | −0.29 (−1.11, 0.54) | 0.36 (−0.86, 1.59) | 0.52 (−0.61, 1.65) | 0.22 (−1.14, 1.57) |
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Del Carmen, M.G.; Rice, L.W. Underrepresentation of women in clinical trials: Why gynecologic oncologists are worried. Obstet. Gynecol. 2015, 125, 616–619. [Google Scholar] [CrossRef] [PubMed]
- Galvao, M. Underrepresentation of minorities in clinical trials: A current problem with escalating future implications. Heart lung 2011, 40, 391–392. [Google Scholar] [CrossRef] [PubMed]
- Peat, G.; Birrell, F.; Cumming, J.; Doherty, M.; Simpson, H.; Conaghan, P.G.; The Arthritis Research UK Clinical Studies Group for Osteoarthritis and Crystal Diseases. Under-representation of the elderly in osteoarthritis clinical trials. Rheumatology 2011, 50, 1184–1186. [Google Scholar] [CrossRef] [PubMed]
- Devlin, G. Women and elderly: Subgroups under-represented in clinical trials. Curr. Opin. Cardiol. 2010, 25, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Cox, L.; Kloseck, M.; Crilly, R.; McWilliam, C.; Diachun, L. Underrepresentation of individuals 80 years of age and older in chronic disease clinical practice guidelines. Can. Fam. Physician 2011, 57, e263–e269. [Google Scholar] [PubMed]
- Cameron, H.J.; Williams, B.O. Clinical trials in the elderly. Should we do more? Drugs aging 1996, 9, 307–310. [Google Scholar] [CrossRef] [PubMed]
- Denson, A.C.; Mahipal, A. Participation of the elderly population in clinical trials: Barriers and solutions. Cancer Control 2014, 21, 209–214. [Google Scholar] [PubMed]
- Hutchins, L.F.; Unger, J.M.; Crowley, J.J.; Coltman, C.A., Jr.; Albain, K.S. Underrepresentation of patients 65 years of age or older in cancer-treatment trials. N. Engl. J. Med. 1999, 341, 2061–2067. [Google Scholar] [CrossRef] [PubMed]
- Odden, M.C.; Coxson, P.G.; Moran, A.; Lightwood, J.M.; Goldman, L.; Bibbins-Domingo, K. The impact of the aging population on coronary heart disease in the United States. Am. J. Med. 2011, 124, 827–833. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, E.L.; Baird, E.; Sheikh, J.I. Recruitment and retention of elderly patients in clinical trials: Issues and strategies. Am. J. Geriatr. Psychiatry 2001, 9, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Velilla, N.; Formiga, F. Inclusion of the elderly in clinical trials: A need and an obligation. Rev. Esp. geriatr. Gerontol. 2014, 49, 99–100. [Google Scholar] [PubMed]
- Farkouh, M.E.; Fuster, V. Time to welcome the elderly into clinical trials. Nat. Clin. Pract. Cardiovasc. Med. 2008, 5. [Google Scholar] [CrossRef] [PubMed]
- Siu, L.L. Clinical trials in the elderly—A concept comes of age. N. Engl. J. Med. 2007, 356, 1575–1576. [Google Scholar] [CrossRef] [PubMed]
- Avorn, J. Including elderly people in clinical trials. BMJ 1997, 315, 1033–1034. [Google Scholar] [CrossRef] [PubMed]
- Older Adults. Available online: http://www.healthypeople.gov/2020/topicsobjectives2020/overview.aspx?topicid=31 (accessed on 16 August 2015).
- Reducing Health Disparities in Cancer. Available online: http://www.cdc.gov/cancer/healthdisparities/basic_info/disparities.htm (accessed on 16 August 2015).
- Meyer, J.M.; Archdeacon, P.; Albrecht, R. FDA perspective: Enrolment of elderly transplant recipients in clinical trials. Transplantation 2013, 95, 916–918. [Google Scholar] [CrossRef] [PubMed]
- Macias, F.M.; Ramsay, R.E.; Rowan, A.J. Recruitment and retention in clinical trials of the elderly. Int. Rev. Neurobiol. 2007, 81, 265–272. [Google Scholar] [PubMed]
- Provencher, V.; Mortenson, W.B.; Tanguay-Garneau, L.; Belanger, K.; Dagenais, M. Challenges and strategies pertaining to recruitment and retention of frail elderly in research studies: A systematic review. Arch. Gerontol. Geriatr. 2014, 59, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Jennings, C.G.; MacDonald, T.M.; Wei, L.; Brown, M.J.; McConnachie, L.; Mackenzie, I.S. Does offering an incentive payment improve recruitment to clinical trials and increase the proportion of socially deprived and elderly participants? Trials 2015, 16. [Google Scholar] [CrossRef] [PubMed]
- Corbie-Smith, G.; Thomas, S.B.; Williams, M.V.; Moody-Ayers, S. Attitudes and beliefs of African Americans toward participation in medical research. J. Gen. Intern. Med. 1999, 14, 537–546. [Google Scholar] [CrossRef] [PubMed]
- BeLue, R.; Taylor-Richardson, K.D.; Lin, J.; Rivera, A.T.; Grandison, D. African Americans and participation in clinical trials: Differences in beliefs and attitudes by gender. Contemp. Clin. Trials 2006, 27, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Gamble, V.N. Under the shadow of Tuskegee: African Americans and health care. Am. J. Public Health 1997, 87, 1773–1778. [Google Scholar] [CrossRef] [PubMed]
- Gorelick, P.B.; Harris, Y.; Burnett, B.; Bonecutter, F.J. The recruitment triangle: Reasons why African Americans enroll, refuse to enroll, or voluntarily withdraw from a clinical trial. An interim report from the African-American antiplatelet stroke prevention study (AAASPS). J. Natl. Med. Assoc. 1998, 90, 141–145. [Google Scholar]
- Gadegbeku, C.A.; Stillman, P.K.; Huffman, M.D.; Jackson, J.S.; Kusek, J.W.; Jamerson, K.A. Factors associated with enrollment of African Americans into a clinical trial: Results from the African American study of kidney disease and hypertension. Contemp. Clin. Trials 2008, 29, 837–842. [Google Scholar] [CrossRef] [PubMed]
- Corliss, J. Broadening recruitment for minorities, the elderly. Cancer discovery 2011, 1, 461. [Google Scholar] [PubMed]
- Gorelick, P.B.; Richardson, D.; Hudson, E.; Perry, C.; Robinson, D.; Brown, N.; Harris, Y. Establishing a community network for recruitment of African Americans into a clinical trial. The African-American antiplatelet stroke prevention study (AAASPS) experience. J. Natl. Med. Assoc. 1996, 88, 701–704. [Google Scholar] [PubMed]
- Langford, A.T.; Resnicow, K.; Beasley, D.D. Outcomes from the body & soul clinical trials project: A university-church partnership to improve African American enrollment in a clinical trial registry. Patient Educ. Couns. 2015, 98, 245–250. [Google Scholar] [PubMed]
- Frew, P.M.; Omer, S.B.; Parker, K.; Bolton, M.; Schamel, J.; Shapiro, E.; Owens, L.; Saint-Victor, D.; Boggavarapu, S.; Braxton, N.; et al. Delivering a “dose of hope”: A faith-based program to increase older African Americans’ participation in clinical trials. JMIR Res. Protoc. 2015, 4. [Google Scholar] [CrossRef] [PubMed]
- Frew, P.M.; del Rio, C.; Clifton, S.; Archibald, M.; Hormes, J.T.; Mulligan, M.J. Factors influencing HIV vaccine community engagement in the urban south. J. Community Health 2008, 33, 259–269. [Google Scholar] [CrossRef] [PubMed]
- Frew, P.M.; Archibald, M.; Diallo, D.D.; Hou, S.I.; Horton, T.; Chan, K.; Mulligan, M.J.; del Rio, C. An extended model of reasoned action to understand the influence of individual- and network-level factors on African Americans’ participation in HIV vaccine research. Prev. Sci. 2010, 11, 207–218. [Google Scholar] [CrossRef] [PubMed]
- Frew, P.M.; Archibald, M.; Martinez, N.; del Rio, C.; Mulligan, M. Promoting HIV vaccine research in the African American community: Does the theory of reasoned action explain potential outcomes of involvement? Challenge 2008, 13, 61–97. [Google Scholar]
- Frew, P.M.; Archibald, M.; Hixson, B.; del Rio, C. Socioecological influences on community involvement in HIV vaccine research. Vaccine 2011, 29, 6136–6143. [Google Scholar] [CrossRef] [PubMed]
- Kumkale, G.T.; Albarracin, D. The sleeper effect in persuasion: A meta-analytic review. Psychol. Bull. 2004, 130, 143–172. [Google Scholar] [CrossRef] [PubMed]
- Tormala, Z.L.; Clarkson, J.J. Assimilation and contrast in persuasion: The effects of source credibility in multiple message situations. Pers. Soc. Psychol. Bull. 2007, 33, 559–571. [Google Scholar] [CrossRef] [PubMed]
- Smith, C.T.; De Houwer, J.; Nosek, B.A. Consider the source: Persuasion of implicit evaluations is moderated by source credibility. Pers. Soc. Psychol. Bull. 2013, 39, 193–205. [Google Scholar] [CrossRef] [PubMed]
- Sawicki, V.; Wegener, D.T.; Clark, J.K.; Fabrigar, L.R.; Smith, S.M.; Durso, G.R. Feeling conflicted and seeking information: When ambivalence enhances and diminishes selective exposure to attitude-consistent information. Pers. Soc. Psychol. Bull. 2013, 39, 735–747. [Google Scholar] [CrossRef] [PubMed]
- Woods, G.; Levinson, A.H.; Jones, G.; Kennedy, R.L.; Johnson, L.C.; Tran, Z.V.; Gonzalez, T.; Marcus, A.C. The living well by faith health and wellness program for African Americans: An exemplar of community-based participatory research. Ethn. Dis. 2013, 23, 223–229. [Google Scholar] [PubMed]
- Brugge, D.; Kole, A.; Lu, W.; Must, A. Susceptibility of elderly Asian immigrants to persuasion with respect to participation in research. J. Immigr. Health 2005, 7, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Greenwell, C.; Spillman, D. Successful recruitment and interview techniques of free-living elderly. J. Am. Diet. Assoc. 1996, 96. [Google Scholar] [CrossRef]
- Colon-Otero, G.; Albertie, M.; Lesperance, M.; Weis, J.A.; Coles, A.; Smith, N.; Mills, L.; Woodward, T.; Aspitia, A.M.; Vishnu, P.; et al. A pilot program in collaboration with African American churches successfully increases awareness of the importance of cancer research and participation in cancer translational research studies among African Americans. J. Cancer Edu. 2012, 27, 294–298. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons by Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Frew, P.M.; Schamel, J.T.; O’Connell, K.A.; Randall, L.A.; Boggavarapu, S. Results of a Community Randomized Study of a Faith-Based Education Program to Improve Clinical Trial Participation among African Americans. Int. J. Environ. Res. Public Health 2016, 13, 41. https://doi.org/10.3390/ijerph13010041
Frew PM, Schamel JT, O’Connell KA, Randall LA, Boggavarapu S. Results of a Community Randomized Study of a Faith-Based Education Program to Improve Clinical Trial Participation among African Americans. International Journal of Environmental Research and Public Health. 2016; 13(1):41. https://doi.org/10.3390/ijerph13010041
Chicago/Turabian StyleFrew, Paula M., Jay T. Schamel, Kelli A. O’Connell, Laura A. Randall, and Sahithi Boggavarapu. 2016. "Results of a Community Randomized Study of a Faith-Based Education Program to Improve Clinical Trial Participation among African Americans" International Journal of Environmental Research and Public Health 13, no. 1: 41. https://doi.org/10.3390/ijerph13010041
APA StyleFrew, P. M., Schamel, J. T., O’Connell, K. A., Randall, L. A., & Boggavarapu, S. (2016). Results of a Community Randomized Study of a Faith-Based Education Program to Improve Clinical Trial Participation among African Americans. International Journal of Environmental Research and Public Health, 13(1), 41. https://doi.org/10.3390/ijerph13010041