
Cardiovascular System Response to Carbon Dioxide and Exercise in Oxygen-Enriched Environment at 3800 m

Abstract
:1. Introduction
2. Methodology and Measurements
2.1. Characteristics of the Study Subjects

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | Age (years) | Height (cm) | Weight (kg) | HR (bmp) | SBP (mmHg) | DBP (mmHg) |
|---|---|---|---|---|---|---|
| 1# | 24 | 173 | 64 | 64 | 112 | 72 |
| 2# | 26 | 175 | 66 | 67 | 116 | 78 |
| 3# | 22 | 179 | 62 | 62 | 109 | 68 |
| 4# | 25 | 170 | 63 | 69 | 110 | 76 |
| 5# | 25 | 181 | 69 | 61 | 103 | 74 |
| 6# | 28 | 172 | 65 | 66 | 114 | 69 |
| Mean ± SD | 25.0 ± 2.0 | 175.0 ± 4.2 | 64.8 ± 2.5 | 64.8 ± 3.1 | 110.7 ± 4.6 | 72.8 ± 3.9 |
2.2. Experimental Conditions
| Symbol | Altitude (m) | Barometric Pressure (mmHg) | O2 Concentration (%) | CO2 Concentration (%) | Experiment Environmental Conditions |
|---|---|---|---|---|---|
| SL | 0 | 760.4–763.6 | 21% | 0.03 | No operating vacuum pumps and chamber gate open |
| HA | 3800 | 475.3–477.4 | 21% | 0.03 | Simulating 3800 m altitude without releasing O2 and CO2 gases |
| C1 | 3800 | 476.2–477.8 | 25% | 0.5 | Releasing O2 and CO2 gases into hypobaric chamber that was simulating 3800m, and controlling the ventilation rate of hypobaric chamber and release rate of O2 and CO2 gases |
| C2 | 3800 | 476.9–478.5 | 25% | 3.0 | |
| C3 | 3800 | 476.7–478.2 | 25% | 5.0 |
2.3. Exercise Test Protocol

2.4. Measurement
2.5. Statistical Analysis
3. Results
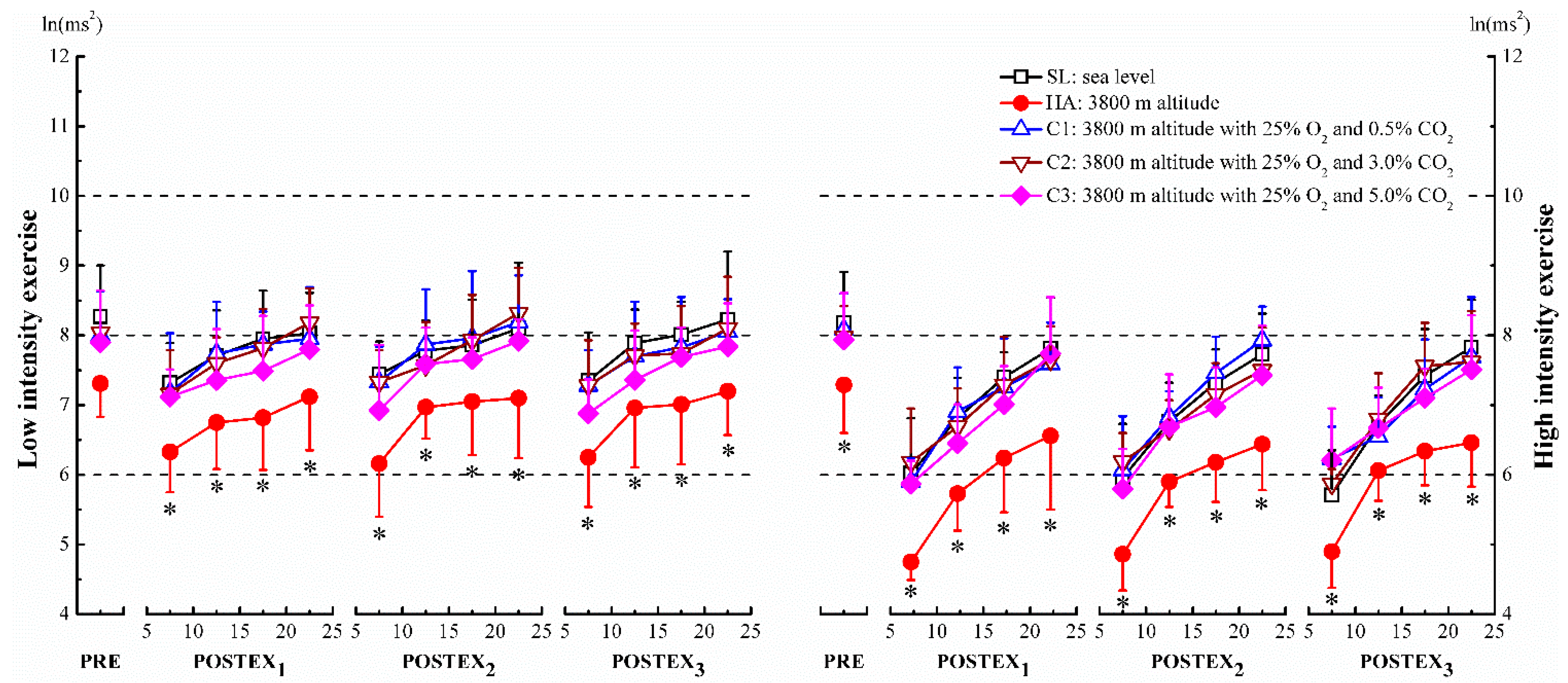
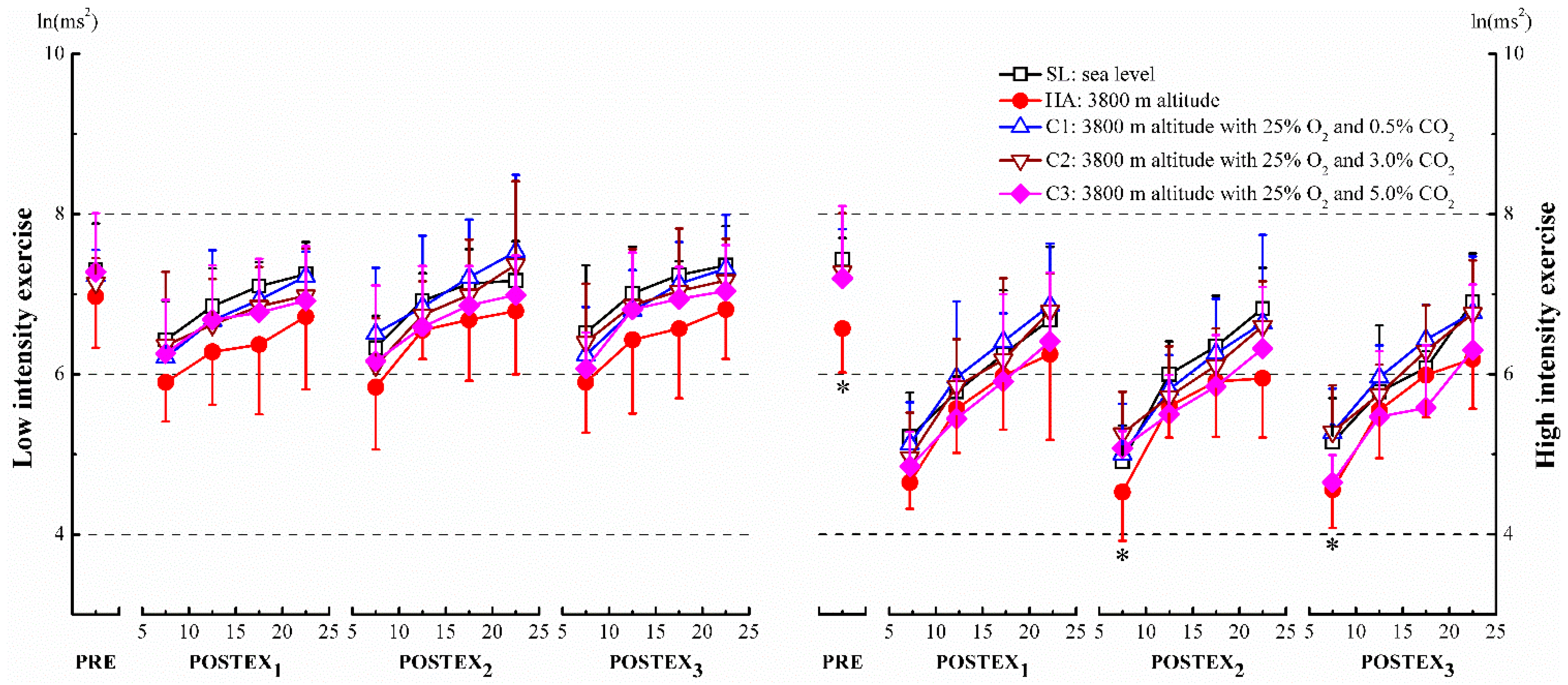
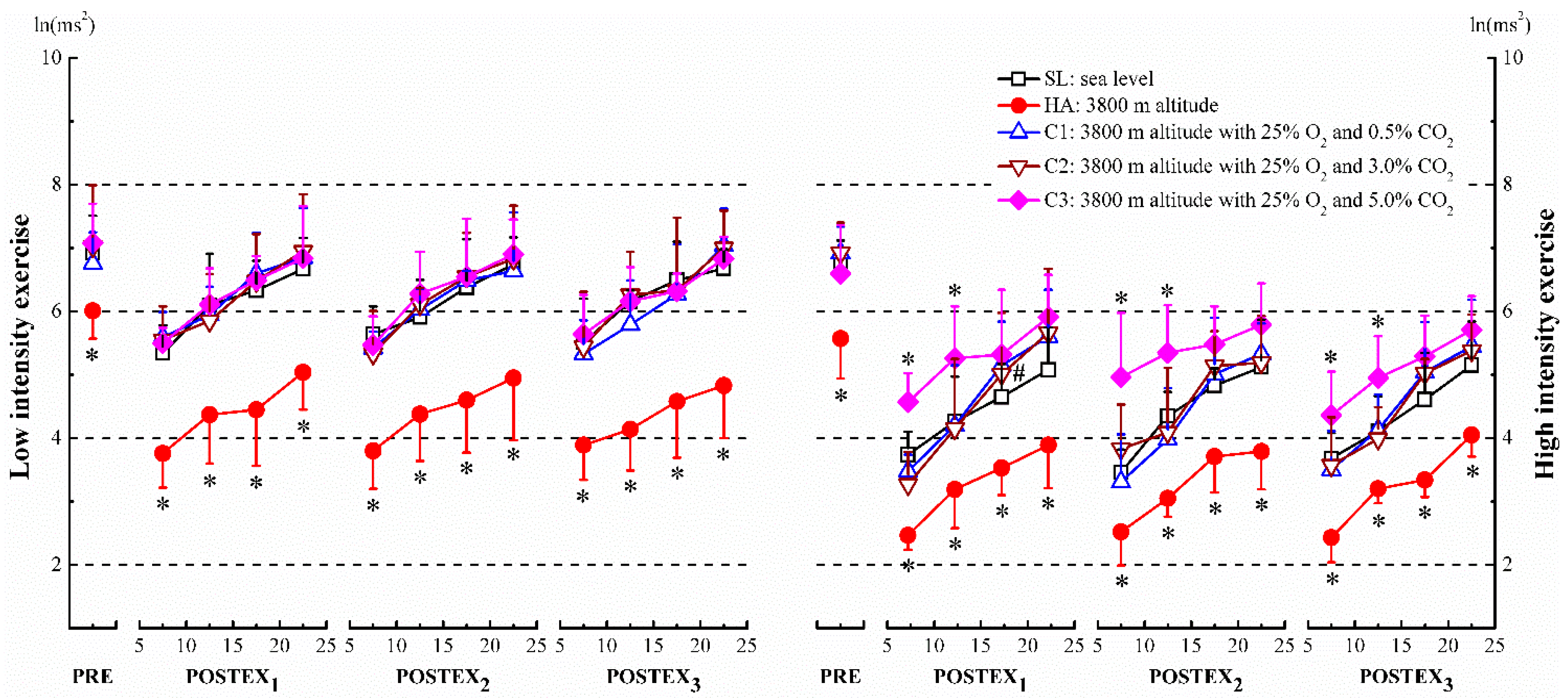
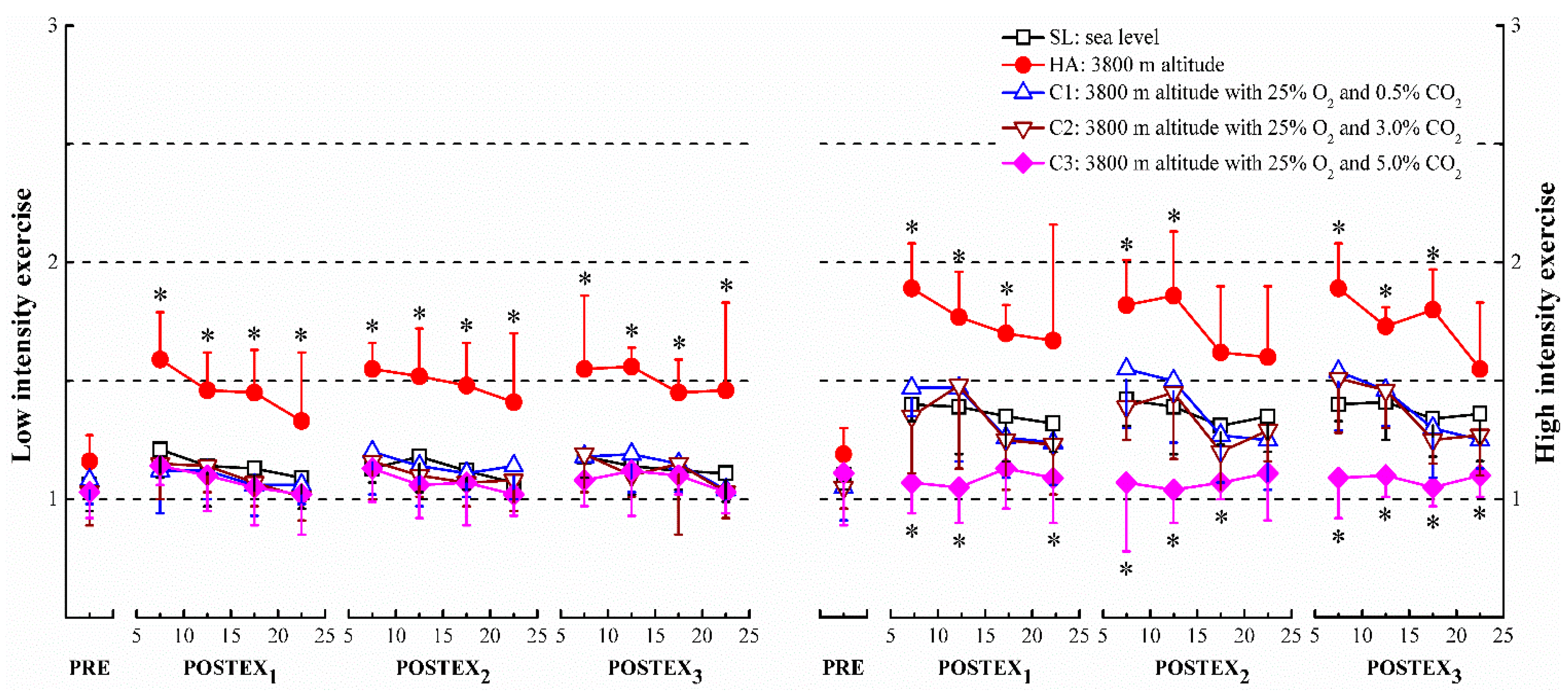
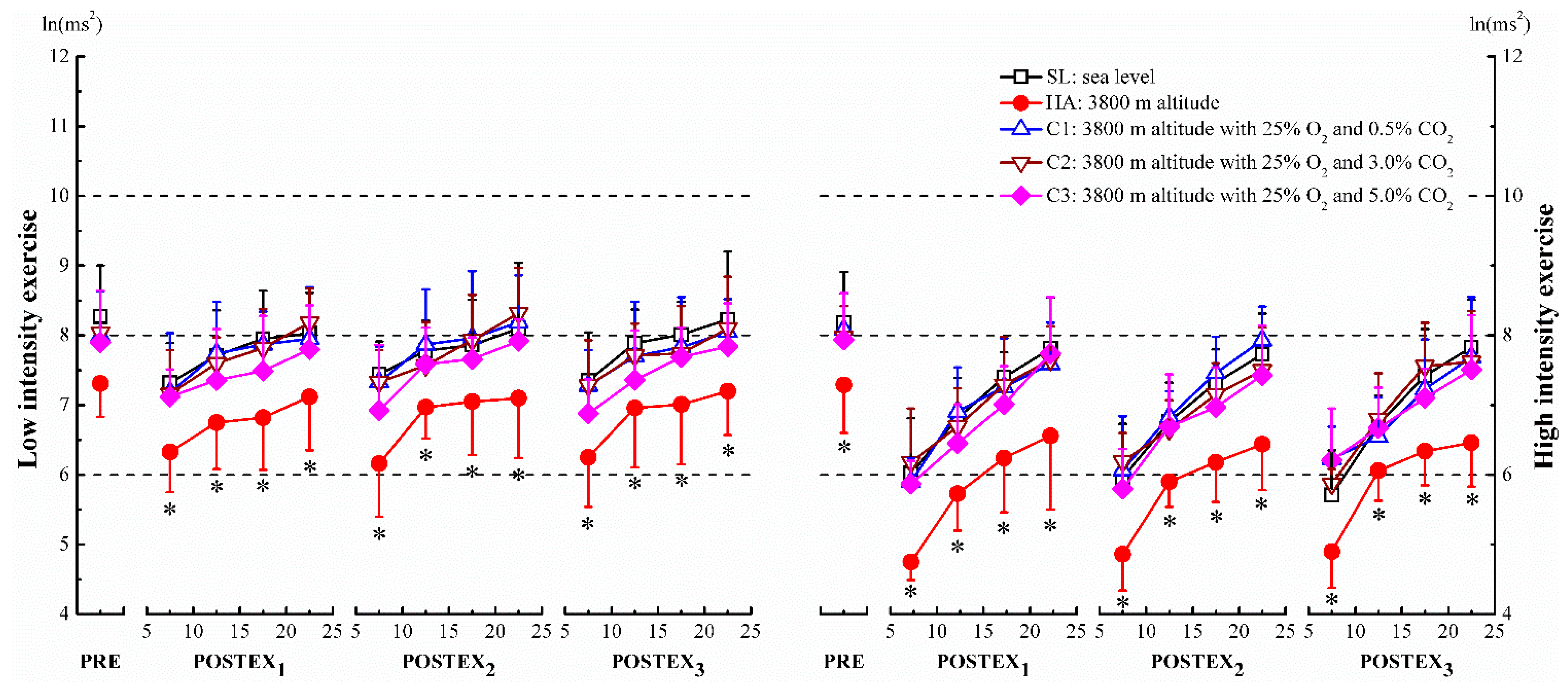
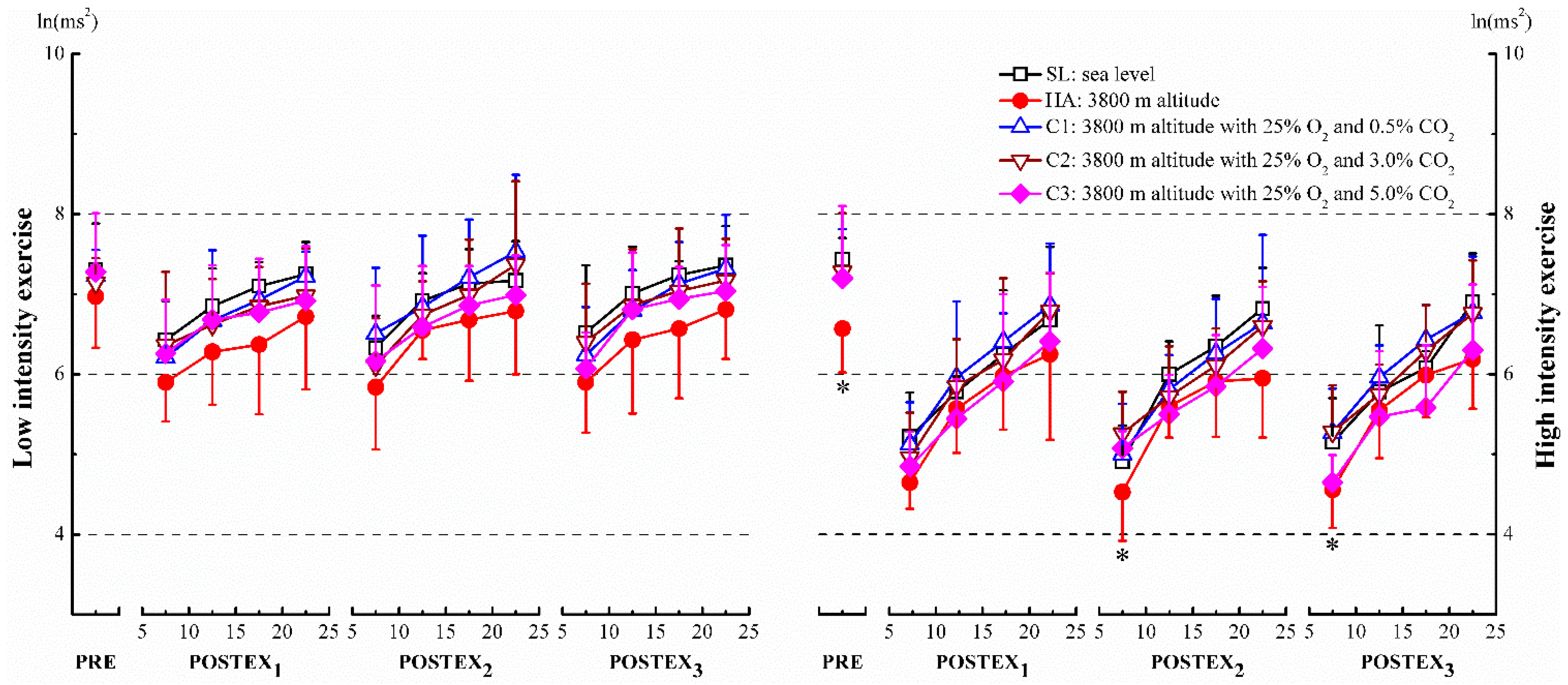
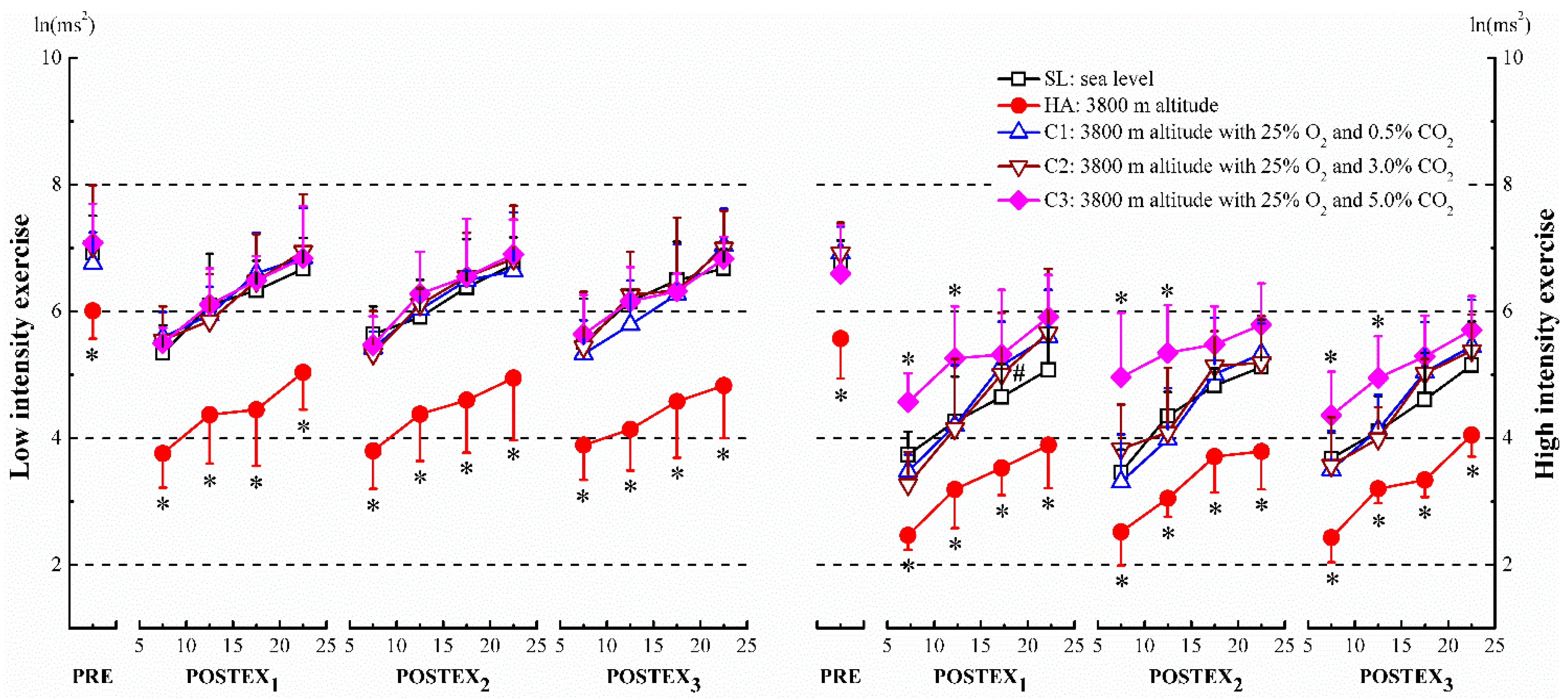
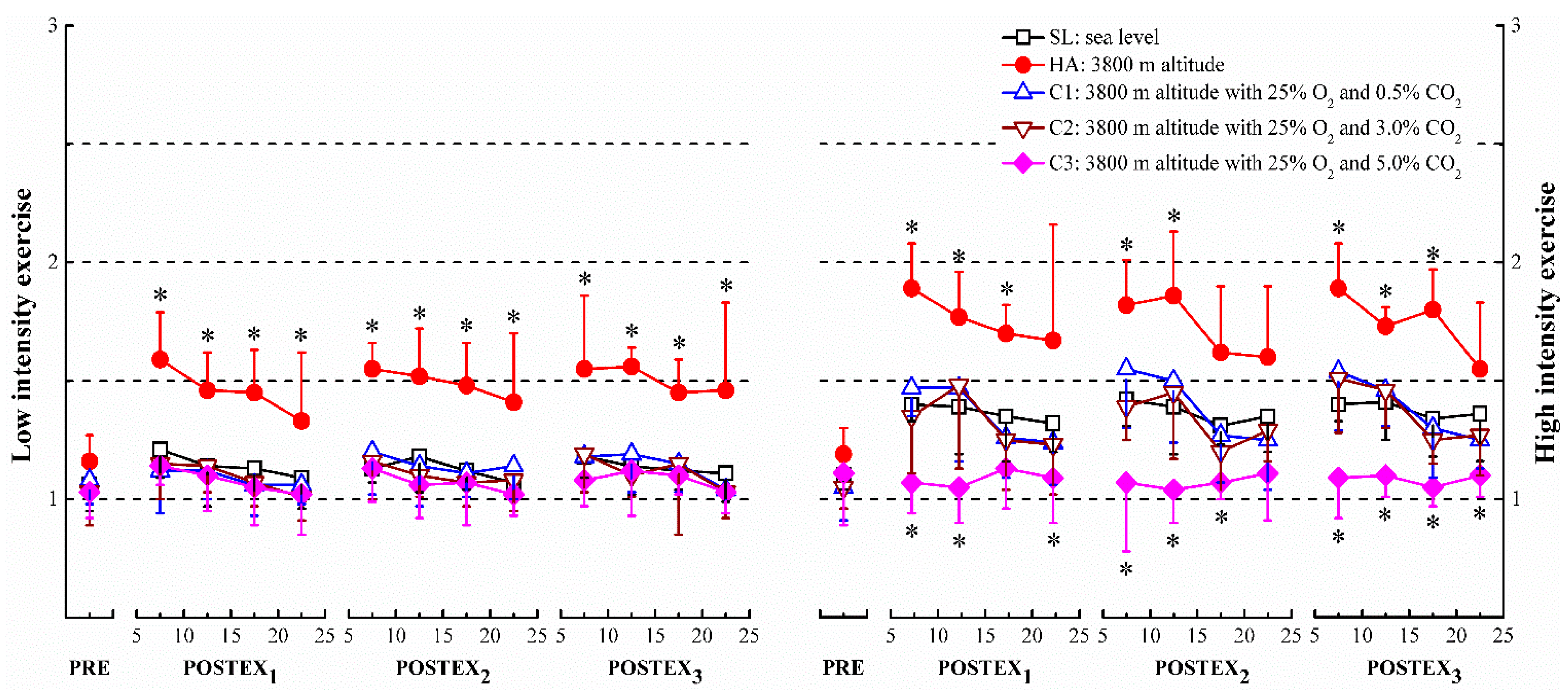
3.1. HRV Analysis
3.2. Heart Rate
| Exercise Intensity | Sea Level | 3800 m Altitude | 3800 m Altitude with 25% O2 and 0.3% CO2 | 3800 m Altitude with 25% O2 and 3.0% CO2 | 3800 m Altitude with 25% O2 and 5.0% CO2 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| S1 | S2 | S3 | S1 | S2 | S3 | S1 | S2 | S3 | S1 | S2 | S3 | S1 | S2 | S3 | |
| Maximum values of heart rate during exercise | |||||||||||||||
| LI | 109.3 (7.8) | 105.8 (4.0) | 103.5 (1.5) | 126.7 (3.7) * | 128.3 (3.4) * | 130.2 (3.3) * | 104.8 (2.1) | 107.2 (2.9) | 108.2 (4.3) | 105.3 (2.7) | 108.7 (4.5) | 106.7 (4.1) | 134.2 (4.2) * | 132.8 (3.2) * | 137.5 (4.2) * |
| HI | 140.5 (6.5) † | 142.3 (9.4) † | 138.3 (2.8) † | 158.2 (5.3) †,* | 161.7 (4.6) †,* | 164.0 (6.9) †,* | 142.8 (5.7) † | 145.0 (6.0) † | 141.3 (5.2) † | 143.2 (2.5) † | 145.8 (3.7) † | 142.7 (9.4) | 165.3 (6.2) †,* | 175.8 (5.6) †,* | 177.7 (4.3) †,* |
| Resting heart rate during post-exercise | |||||||||||||||
| LI | 141.7 (4.0) | 146.5 (3.3) | 143.2 (1.7) | 144.5 (5.6) | 144.2 (5.8) | 148.0 (6.8) | 143.2 (5.0) | 145.5 (8.1) | 147.3 (5.3) | 146.3 (6.1) | 143.7 (5.7) | 142.8 (4.5) | 156.7 (6.5) * | 158.3 (5.2) * | 160.0 (8.7) * |
| HI | 177.7 (6.3) † | 183.2 (2.3) † | 181.5 (7.2) † | 184.8 (6.2) † | 179.5 (4.7) † | 181.8 (4.2) † | 182.3 (2.9) † | 183.2 (3.2) † | 185.7 (4.5) † | 181.7 (4.6) † | 182.0 (4.4) † | 184.5 (4.9) † | 196.3 (6.8) †,* | 198.5 (6.9) †,* | 201.8 (6.5) †,* |
3.3. Blood Pressure
| Exercise Intensity | Sea Level | 3800 m Altitude | 3800 m Altitude with 25% O2 and 0.3% CO2 | 3800 m Altitude with 25% O2 and 3.0% CO2 | 3800 m Altitude with 25% O2 and 5.0% CO2 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| S1 | S2 | S3 | S1 | S2 | S3 | S1 | S2 | S3 | S1 | S2 | S3 | S1 | S2 | S3 | |
| Maximum during exercise | |||||||||||||||
| LI | 141.7 (4.0) | 146.5 (3.3) | 143.2 (1.7) | 144.5 (5.6) | 144.2 (5.8) | 148.0 (6.8) | 143.2 (5.0) | 145.5 (8.1) | 147.3 (5.3) | 146.3 (6.1) | 143.7 (5.7) | 142.8 (4.5) | 156.7 (6.5) * | 158.3 (5.2) * | 160.0 (8.7) * |
| HI | 177.7 (6.3) † | 183.2 (2.3) † | 181.5 (7.2) † | 184.8 (6.2) † | 179.5 (4.7) † | 181.8 (4.2) † | 182.3 (2.9) † | 183.2 (3.2) † | 185.7 (4.5) † | 181.7 (4.6) † | 182.0 (4.4) † | 184.5 (4.9) † | 196.3 (6.8) †,* | 198.5 (6.9) †,* | 201.8 (6.5) †,* |
| Minimum during post-exercise | |||||||||||||||
| LI | 64.3 (2.5) | 67.0 (3.9) | 65.8 (3.5) | 83.5 (3.0) * | 82.3 (4.5) * | 82.2 (5.9) * | 67.7 (4.5) | 65.2 (2.9) | 68.5 (3.2) | 65.5 (3.5) | 66.0 (3.2) | 69.5 (4.1) | 66.8 (2.9) | 67.5 (3.0) | 69.2 (3.8) |
| HI | 64.0 (5.1) | 66.5 (3.1) | 68.2 (4.3) | 81.2 (4.8) * | 80.7 (6.5) * | 82.2 (5.9) * | 66.2 (4.4) | 65.1 (2.9) | 69.3 (3.1) | 64.2 (3.9) | 68.2 (2.7) | 69.7 (5.2) | 63.7 (3.6) | 70.2 (3.6) | 61.7 (6.3) |
| Exercise Intensity | Sea Level | 3800 m Altitude | 3800 m Altitude with 25% O2 and 0.3% CO2 | 3800 m Altitude with 25% O2 and 3.0% CO2 | 3800 m Altitude with 25% O2 and 5.0% CO2 | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| S1 | S2 | S3 | S1 | S2 | S3 | S1 | S2 | S3 | S1 | S2 | S3 | S1 | S2 | S3 | |
| Maximum during exercise | |||||||||||||||
| LI | 77.3 (4.2) | 78.3 (4.2) | 72.3 (1.4) | 71.7 (1.8) | 77.5 (3.8) | 75.3 (4.6) | 76.3 (5.2) | 75.0 (6.0) | 69.7 (5.3) | 73.7 (4.3) | 71.3 (3.9) | 77.0 (3.9) | 76.7 (2.7) | 73.3 (3.6) | 77.2 (4.6) |
| HI | 77.2 (2.7) | 75.8 (2.4) | 71.0 (1.8) | 76.2 (4.4) | 77.2 (3.7) | 73.7 (3.1) | 74.3 (3.9) | 70.8 (3.9) | 76.0 (2.5) | 71.2 (3.2) | 73.3 (5.5) | 76.2 (4.4) | 77.0 (3.0) | 76.0 (6.0) | 72.7 (5.0) |
| Minimum during post-exercise | |||||||||||||||
| LI | 75.0 (2.8) | 74.7 (1.8) | 71.8 (3.1) | 70.5 (4.8) | 77.0 (3.7) | 75.8 (3.9) | 74.7 (2.3) | 75.0 (6.0) | 72.8 (2.3) | 73.0 (2.8) | 71.3 (2.1) | 76.3 (4.3) | 70.7 (4.9) | 73.0 (2.2) | 77.5 (2.3) |
| HI | 70.0 (4.7) | 74.2 (1.9) | 73.3 (1.5) | 71.0 (2.8) | 76.8 (6.0) | 74.7 (3.1) | 71.8 (2.7) | 74.0 (3.8) | 74.2 (2.9) | 72.0 (1.4) | 74.5 (5.9) | 76.2 (4.4) | 70.5 (4.3) | 74.4 (4.2) | 77.2 (5.9) |
4. Discussion
4.1. HRV Analysis
4.2. Heart Rate
4.3. Blood Pressure
5. Conclusions
6. Research Limitations
Acknowledgments
Author Contributions
Conflicts of Interest
References
- West, J.B.; Schoene, R.B.; Luks, A.M.; Milledge, J.S. High Altitude Medicine and Physiology; CRC Press: Florida, FL, USA, 2012. [Google Scholar]
- Ainslie, P.N.; Burgess, K.R. Cardiorespiratory and cerebrovascular responses to hyperoxic and hypoxic rebreathing: Effects of acclimatization to high altitude. Resp. Physiol. Neurobi. 2008, 161, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Hainsworth, R.; Drinkhill, M.J. Cardiovascular adjustments for life at high altitude. Resp. Physiol. Neurobi. 2007, 158, 204–211. [Google Scholar] [CrossRef] [PubMed]
- Hartley, H. Effects of high-altitude environment on the cardiovascular system of man. JAMA 1971, 215, 241–244. [Google Scholar] [CrossRef] [PubMed]
- Naeije, R. Physiological adaptation of the cardiovascular system to high altitude. Prog. Cardiovasc. Dis. 2010, 52, 456–466. [Google Scholar] [CrossRef] [PubMed]
- Penaloza, D.; Arias-Stella, J. The heart and pulmonary circulation at high altitudes healthy highlanders and chronic mountain sickness. Circulation 2007, 115, 1132–1146. [Google Scholar] [CrossRef] [PubMed]
- Reeves, J.T.; Groves, B.M.; Sutton, J.R.; Wagner, P.D.; Cymerman, A.; Malconian, M.K.; Rock, P.B.; Young, P.M.; Houston, C.S. Operation everest II: Preservation of cardiac function at extreme altitude. J. AppL. Physiol. 1987, 63, 531–539. [Google Scholar] [PubMed]
- Young, A.J.; Cymerman, A.; Burse, R.L. The influence of cardiorespiratory fitness on the decrement in maximal aerobic power at high altitude. Eur. J. Appl. Physiol. Occup. Physiol. 1985, 54, 12–15. [Google Scholar] [CrossRef] [PubMed]
- Brothers, M.D.; Wilber, R.L.; Byrnes, W.C. Physical fitness and hematological changes during acclimatization to moderate altitude: A retrospective study. High Alt. Med. Boil. 2007, 8, 213–224. [Google Scholar] [CrossRef] [PubMed]
- Niu, W.; Wu, Y.; Li, B.; Chen, N.; Song, S. Effects of long-term acclimatization in lowlanders migrating to high altitude: Comparison with high altitude residents. Eur. J. Appl. Physiol. Occup. Physiol. 1995, 71, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Gerard, A.B.; McElroy, M.K.; Taylor, M.J.; Grant, I.; Powell, F.L.; Holverda, S.; Sentse, N.; West, J.B. Six percent oxygen enrichment of room air at simulated 5000 m altitude improves neuropsychological function. High Alt. Med. Boil. 2000, 1, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Luks, A.M.; van Melick, H.; Batarse, R.R.; Powell, F.L.; Grant, I.; West, J.B. Room oxygen enrichment improves sleep and subsequent day-time performance at high altitude. Resp. Physiol. 1998, 113, 247–258. [Google Scholar] [CrossRef]
- McElroy, M.K.; Gerard, A.; Powell, F.L.; Prisk, G.K.; Sentse, N.; Holverda, S.; West, J.B. Nocturnal O2 enrichment of room air at high altitude increases daytime O2 saturation without changing control of ventilation. High Alt. Med. Boil. 2000, 1, 197–206. [Google Scholar] [CrossRef] [PubMed]
- West, J.B. Oxygen enrichment of room air to relieve the hypoxia of high altitude. Resp. Physiol. 1995, 99, 225–232. [Google Scholar] [CrossRef]
- West, J.B. Fire hazard in oxygen-enriched atmospheres at low barometric pressures. Aviat. Space Envir. Md. 1997, 68, 159–162. [Google Scholar]
- West, J.B. Safe upper limits for oxygen enrichment of room air at high altitude. High Alt. Med. Boil. 2001, 2, 47–51. [Google Scholar] [CrossRef] [PubMed]
- West, J.B. Commuting to high altitude: Value of oxygen enrichment of room air. High Alt. Med. Boil. 2002, 3, 223–235. [Google Scholar] [CrossRef] [PubMed]
- Guais, A.; Brand, G.; Jacquot, L.; Karrer, M.; Dukan, S.; Grévillot, G.; Molina, T.J.; Bonte, J.; Regnier, M.; Schwartz, L. Toxicity of carbon dioxide: A review. Chem. Res. Toxicol. 2011, 24, 2061–2070. [Google Scholar] [CrossRef] [PubMed]
- Baek, S.-O.; Kim, Y.-S.; Perry, R. Indoor air quality in homes, offices and restaurants in korean urban areas—Indoor/outdoor relationships. Atmos. Environ. 1997, 31, 529–544. [Google Scholar] [CrossRef]
- Ng, L.C.; Musser, A.; Persily, A.K.; Emmerich, S.J. Indoor air quality analyses of commercial reference buildings. Build. Environ. 2012, 58, 179–187. [Google Scholar] [CrossRef]
- Seppänen, O.; Fisk, W.; Mendell, M. Association of ventilation rates and CO2 concentrations with health andother responses in commercial and institutional buildings. Indoor air 1999, 9, 226–252. [Google Scholar] [CrossRef] [PubMed]
- Ventilation for Acceptable Indoor Air Quality. Available online: http://www.mintie.com/assets/pdf/education/ASHRAE%2062.1-2007.pdf (accessed on 27 May 2015).
- Bailey, J.E.; Argyropoulos, S.V.; Kendrick, A.H.; Nutt, D.J. Behavioral and cardiovascular effects of 7.5% CO2 in human volunteers. Depress. Anxiety 2005, 21, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Leibold, N.K.; Viechtbauer, W.; Goossens, L.; De Cort, K.; Griez, E.J.; Myin-Germeys, I.; Steinbusch, H.W.; van den Hove, D.L.; Schruers, K.R. Carbon dioxide inhalation as a human experimental model of panic: The relationship between emotions and cardiovascular physiology. Biol. Psychol. 2013, 94, 331–340. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, D.E.; D’Arsigny, C.; Fitzpatrick, M.; Webb, K.A. Exercise hypercapnia in advanced chronic obstructive pulmonary disease: The role of lung hyperinflation. Am. J. Resp. Crit. Care 2002, 166, 663–668. [Google Scholar] [CrossRef] [PubMed]
- Ogoh, S.; Tsukamoto, H.; Hirasawa, A.; Hasegawa, H.; Hirose, N.; Hashimoto, T. The effect of changes in cerebral blood flow on cognitive function during exercise. Physiol. Rep. 2014, 2. [Google Scholar] [CrossRef] [PubMed]
- Sato, F.; Nishimura, M.; Igarashi, T.; Yamamoto, M.; Miyamoto, K.; Kawakami, Y. Effects of exercise and CO2 inhalation on intersubject variability in ventilatory and heart rate responses to progressive hypoxia. Eur. Respir. J. 1996, 9, 960–967. [Google Scholar] [CrossRef] [PubMed]
- Bärtsch, P.; Saltin, B. General introduction to altitude adaptation and mountain sickness. Scand. J. Med. Sci. spor. 2008, 18, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Malik, M.; Bigger, J.T.; Camm, A.J.; Kleiger, R.E.; Malliani, A.; Moss, A.J.; Schwartz, P.J. Heart rate variability standards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef]
- Basualto-Alarcón, C.; Rodas, G.; Galilea, P.A.; Riera, J.; Pagés, T.; Ricart, A.; Torrella, J.R.; Behn, C.; Viscor, G. Cardiorespiratory parameters during submaximal exercise under acute exposure to normobaric and hypobaric hypoxia. Apunts. Med. I’Esport 2012, 47, 65–72. [Google Scholar] [CrossRef]
- Buchheit, M.; Richard, R.; Doutreleau, S.; Lonsdorfer-Wolf, E.; Brandenberger, G.; Simon, C. Effect of acute hypoxia on heart rate variability at rest and during exercise. Int. J. Sports Med. 2004, 25, 264–269. [Google Scholar] [PubMed]
- Fukuda-Matsuda, E.; Yamada, M.; Tanobe, K.; Saito, S. Peripheral circulation monitored by surface temperature and autonomic nervous function in hypobaric hypoxic environment: Effects of submaximal exercise. Int. J. Environ. Health res. 2007, 17, 53–60. [Google Scholar] [CrossRef] [PubMed]
- Zupet, P.; Princi, T.; Finderle, Z. Effect of hypobaric hypoxia on heart rate variability during exercise: A pilot field study. Eur. J. Appl. Physiol. 2009, 107, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Kanai, M.; Nishihara, F.; Shiga, T.; Shimada, H.; Saito, S. Alterations in autonomic nervous control of heart rate among tourists at 2700 and 3700m above sea level. Wild. Environ. Med. 2001, 12, 8–12. [Google Scholar] [CrossRef]
- Voelkel, N.F.; Hegstrand, L.; Reeves, J.T.; McMurty, I.; Molinoff, P. Effects of hypoxia on density of beta-adrenergic receptors. J. Appl. Physiol. 1981, 50, 363–366. [Google Scholar] [PubMed]
- Brown, S.; Howden, R. The effects of a respiratory acidosis on human heart rate variability. Adv. Exp. Med. Biol. 2008, 361–365. [Google Scholar]
- Pöyhönen, M.; Syväoja, S.; Hartikainen, J.; Ruokonen, E.; Takala, J. The effect of carbon dioxide, respiratory rate and tidal volume on human heart rate variability. Acta Anaesth. Scand. 2004, 48, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Amann, M.; Eldridge, M.W.; Lovering, A.T.; Stickland, M.K.; Pegelow, D.F.; Dempsey, J.A. Arterial oxygenation influences central motor output and exercise performance via effects on peripheral locomotor muscle fatigue in humans. J. Physiol. 2006, 575, 937–952. [Google Scholar] [CrossRef] [PubMed]
- Engelen, M.; Porszasz, J.; Riley, M.; Wasserman, K.; Maehara, K.; Barstow, T.J. Effects of hypoxic hypoxia on O2 uptake and heart rate kinetics during heavy exercise. J. Appl. Physiol. 1996, 81, 2500–2508. [Google Scholar] [PubMed]
- Squires, R.; Buskirk, E. Aerobic capacity during acute exposure to simulated altitude, 914 to 2286 meters. Med. Sci. Sport. Exer. 1981, 14, 36–40. [Google Scholar] [CrossRef]
- Terrados, N.; Melichna, J.; Sylvén, C.; Jansson, E.; Kaijser, L. Effects of training at simulated altitude on performance and muscle metabolic capacity in competitive road cyclists. Eur. J. Appl. Physiol. Occup. Physiol. 1988, 57, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Terrados, N.; Mizuno, M.; Andersen, H. Reduction in maximal oxygen uptake at low altitudes; role of training status and lung function. Clin. Physiol. 1985, 5, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Mollard, P.; Woorons, X.; Letournel, M.; Cornolo, J.; Lamberto, C.; Beaudry, M.; Richalet, J. Role of maximal heart rate and arterial O2 saturation on the decrement of in moderate acute hypoxia in trained and untrained men. Int. J. Sports Med. 2007, 28, 186. [Google Scholar] [CrossRef] [PubMed]
- Peltonen, J.E.; Tikkanen, H.O.; Rusko, H.K. Cardiorespiratory responses to exercise in acute hypoxia, hyperoxia and normoxia. Eur. J. Appl. Physiol. 2001, 85, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, S.R.; Bogaard, H.J.; Niizeki, K.; Yamaya, Y.; Ziegler, M.G.; Wagner, P.D. β-adrenergic or parasympathetic inhibition, heart rate and cardiac output during normoxic and acute hypoxic exercise in humans. J. Physiol. 2003, 550, 605–616. [Google Scholar] [CrossRef] [PubMed]
- Mazzeo, R.S. Physiological responses to exercise at altitude. Sports Med. 2008, 38, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Zvolensky, M.J.; Eifert, G.H. A review of psychological factors/processes affecting anxious responding during voluntary hyperventilation and inhalations of carbon dioxide-enriched air. Clin. Psychol. Rev. 2001, 21, 375–400. [Google Scholar] [CrossRef]
- Babb, T. Ventilatory response to exercise in subjects breathing CO2 or HeO2. J. Appl. Physiol. 1997, 82, 746–754. [Google Scholar] [PubMed]
- Vercruyssen, M.; Kamon, E.; Hancock, P.A. Effects of carbon dioxide inhalation on psychomotor and mental performance during exercise and recovery. Int. J. Occup. Saf. Ergon. 2007, 13, 15–27. [Google Scholar] [CrossRef] [PubMed]
- Franz, I.-W. Ergometry in the assessment of arterial hypertension. Cardiology 1985, 72, 147–159. [Google Scholar] [CrossRef] [PubMed]
- Miyai, N.; Arita, M.; Miyashita, K.; Morioka, I.; Shiraishi, T.; Nishio, I. Blood pressure response to heart rate during exercise test and risk of future hypertension. Hypertension 2002, 39, 761–766. [Google Scholar] [CrossRef] [PubMed]
- Snyder, E.M.; Olson, T.P.; Johnson, B.D.; Frantz, R.P. Influence of sildenafil on lung diffusion during exposure to acute hypoxia at rest and during exercise in healthy humans. Eur. J. Appl. Physiol. 2008, 103, 421–430. [Google Scholar] [CrossRef] [PubMed]
- Wyss, C.A.; Koepfli, P.; Fretz, G.; Seebauer, M.; Schirlo, C.; Kaufmann, P.A. Influence of altitude exposure on coronary flow reserve. Circulation 2003, 108, 1202–1207. [Google Scholar] [CrossRef] [PubMed]
- Takamata, A.; Nose, H.; Kinoshita, T.; Hirose, M.; Itoh, T.; Morimoto, T. Effect of acute hypoxia on vasopressin release and intravascular fluid during dynamic exercise in humans. Am. J. Physiol. Reg. I. 2000, 279, R161–R168. [Google Scholar]
- Ainslie, P.N.; Barach, A.; Murrell, C.; Hamlin, M.; Hellemans, J.; Ogoh, S. Alterations in cerebral autoregulation and cerebral blood flow velocity during acute hypoxia: Rest and exercise. Am. J. Physiol. Heart C. 2007, 292, H976–H983. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, K.-i.; Ogawa, Y.; Shibata, S.; Aoki, K. Acute exposure to normobaric mild hypoxia alters dynamic relationships between blood pressure and cerebral blood flow at very low frequency. J. Cerebr. Blood F. Met. 2007, 27, 776–784. [Google Scholar] [CrossRef] [PubMed]
- Naeije, R.; Huez, S.; Lamotte, M.; Retailleau, K.; Neupane, S.; Abramowicz, D.; Faoro, V. Pulmonary artery pressure limits exercise capacity at high altitude. Eur. Respir. J. 2010, 36, 1049–1055. [Google Scholar] [CrossRef] [PubMed]
- Pescatello, L.S.; Fargo, A.E.; Leach, C.; Scherzer, H.H. Short-term effect of dynamic exercise on arterial blood pressure. Circulation 1991, 83, 1557–1561. [Google Scholar] [CrossRef] [PubMed]
- Argyropoulos, S.V.; Bailey, J.E.; Hood, S.D.; Kendrick, A.H.; Rich, A.S.; Laszlo, G.; Nash, J.R.; Lightman, S.L.; Nutt, D.J. Inhalation of 35% CO2 results in activation of the HPA axis in healthy volunteers. Psychoneuroendocrinology 2002, 27, 715–729. [Google Scholar] [CrossRef]
- Bailey, J.E.; Argyropoulos, S.V.; Lightman, S.L.; Nutt, D.J. Does the brain noradrenaline network mediate the effects of the CO2 challenge? J. Psychopharmacol. 2003, 17, 252–259. [Google Scholar] [CrossRef] [PubMed]
- Wetherell, M.A.; Crown, A.L.; Lightman, S.L.; Miles, J.N.; Kaye, J.; Vedhara, K. The four-dimensional stress test: Psychological, sympathetic–adrenal–medullary, parasympathetic and hypothalamic–pituitary–adrenal responses following inhalation of 35% CO2. Psychoneuroendocrinology 2006, 31, 736–747. [Google Scholar] [CrossRef] [PubMed]
- Luksch, A.; Garhöfer, G.; Imhof, A.; Polak, K.; Polska, E.; Dorner, G.; Anzenhofer, S.; Wolzt, M.; Schmetterer, L. Effect of inhalation of different mixtures of O2 and CO2 on retinal blood flow. Brit. J. Ophthalmol. 2002, 86, 1143–1147. [Google Scholar] [CrossRef]
- Schibye, B.; Klausen, K.; Trap-Jensen, J.; Lund, J.; Hartling, O. Effects of acute hypoxia and CO2 inhalation on systemic and peripheral oxygen uptake and circulatory responses during moderate exercise. Eur. J. Appl. Physiol. 1988, 57, 519–525. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, G.; Liu, X.; Qin, Z.; Gu, Z.; Wang, G.; Shi, W.; Wen, D.; Yu, L.; Luo, Y.; Xiao, H. Cardiovascular System Response to Carbon Dioxide and Exercise in Oxygen-Enriched Environment at 3800 m. Int. J. Environ. Res. Public Health 2015, 12, 11781-11796. https://doi.org/10.3390/ijerph120911781
Liu G, Liu X, Qin Z, Gu Z, Wang G, Shi W, Wen D, Yu L, Luo Y, Xiao H. Cardiovascular System Response to Carbon Dioxide and Exercise in Oxygen-Enriched Environment at 3800 m. International Journal of Environmental Research and Public Health. 2015; 12(9):11781-11796. https://doi.org/10.3390/ijerph120911781
Chicago/Turabian StyleLiu, Guohui, Xiaopeng Liu, Zhifeng Qin, Zhao Gu, Guiyou Wang, Weiru Shi, Dongqing Wen, Lihua Yu, Yongchang Luo, and Huajun Xiao. 2015. "Cardiovascular System Response to Carbon Dioxide and Exercise in Oxygen-Enriched Environment at 3800 m" International Journal of Environmental Research and Public Health 12, no. 9: 11781-11796. https://doi.org/10.3390/ijerph120911781
APA StyleLiu, G., Liu, X., Qin, Z., Gu, Z., Wang, G., Shi, W., Wen, D., Yu, L., Luo, Y., & Xiao, H. (2015). Cardiovascular System Response to Carbon Dioxide and Exercise in Oxygen-Enriched Environment at 3800 m. International Journal of Environmental Research and Public Health, 12(9), 11781-11796. https://doi.org/10.3390/ijerph120911781