
Distribution of HPV Genotype in Invasive Cervical Carcinoma and Cervical Intraepithelial Neoplasia in Zhejiang Province, Southeast China: Establishing the Baseline for Surveillance

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. HPV Detection and Typing
2.3. Statistical Analysis
3. Results
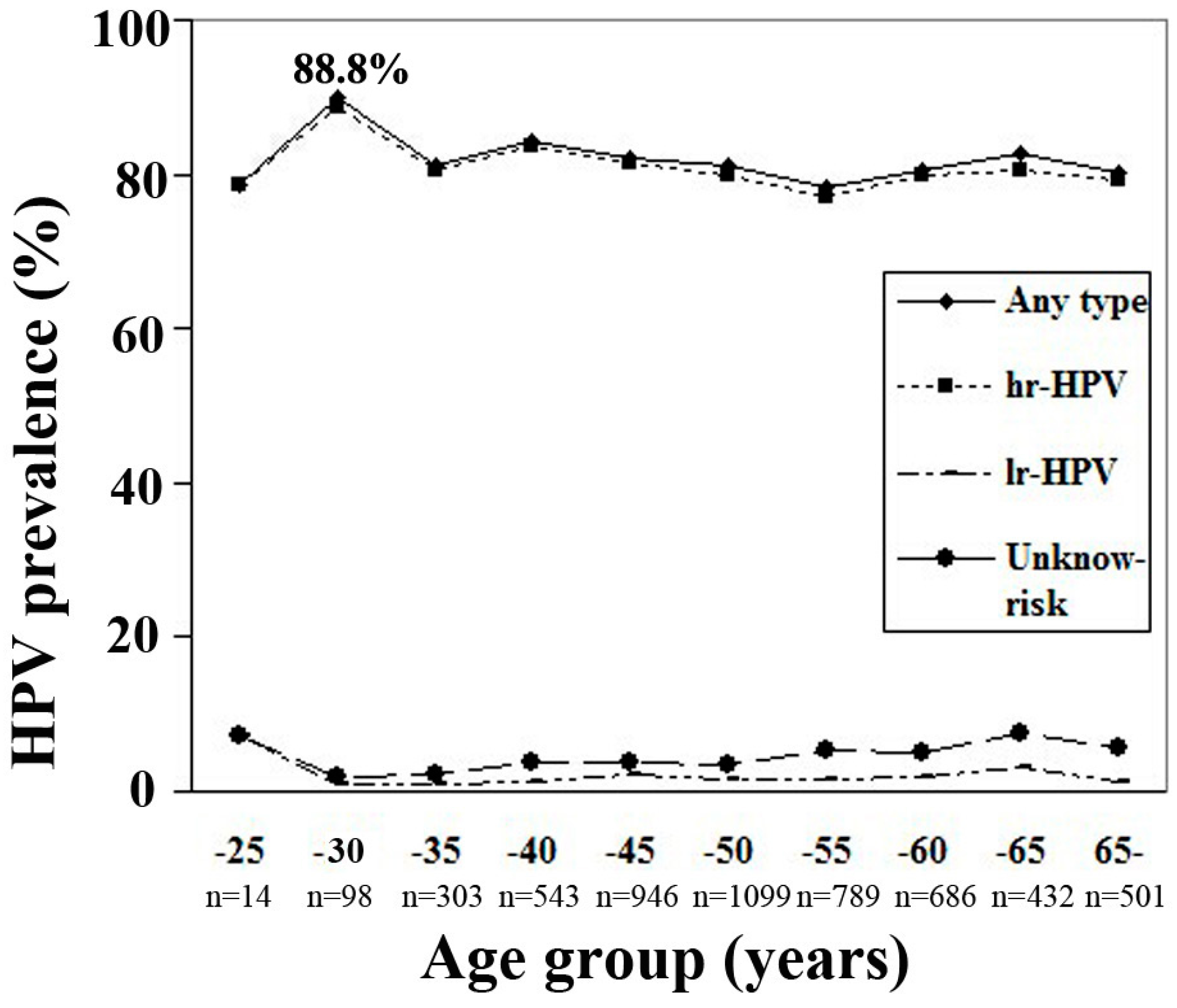
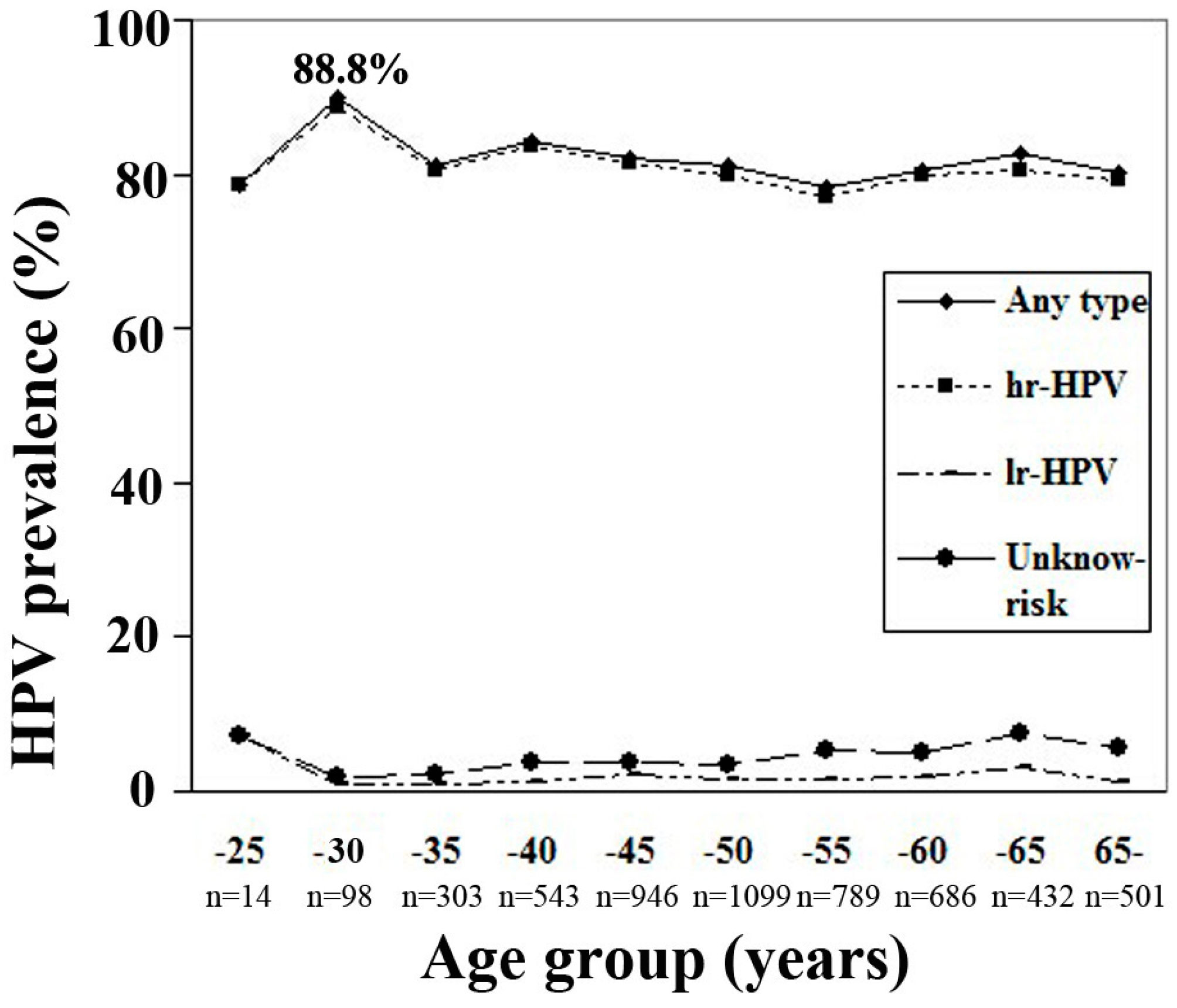
3.1. HPV Positive Rate and Infection Status

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cervical Pathology Status (Total No. Recruited) | HPV Positive Rate (%) | Single-Type Infection (%) | Multiple-Type Infection (%) | ||
|---|---|---|---|---|---|
| Co-Infection | Tri-Infection | Tetra- or More Infection | |||
| Cervical intraepithelial neoplasia (CIN) | |||||
| CIN1 (21) | 81.0 | 47.6 | 28.6 | 0 | 4.8 |
| CIN2 (240) | 81.3 | 55.4 | 17.5 | 7.1 | 1.3 |
| CIN3 (899) | 86.8 | 63.1 | 18.5 | 4.7 | 0.6 |
| Total CIN (1160) | 85.5 | 61.2 | 18.4 | 5.1 | 0.8 |
| Invasive cervical cancer (ICC) | |||||
| SCC (3870) | 81.9 | 65.6 | 13.2 | 2.8 | 0.6 |
| ADC (258) | 58.1 | 45.7 | 9.3 | 2.7 | 0.4 |
| ASC (91) | 74.7 | 56.0 | 14.3 | 4.4 | 0 |
| Other type ICC (31) | 71.0 | 41.9 | 25.8 | 3.2 | 0 |
| Total ICC (4250) | 80.1 | 61.9 | 13.1 | 28.2 | 0.6 |
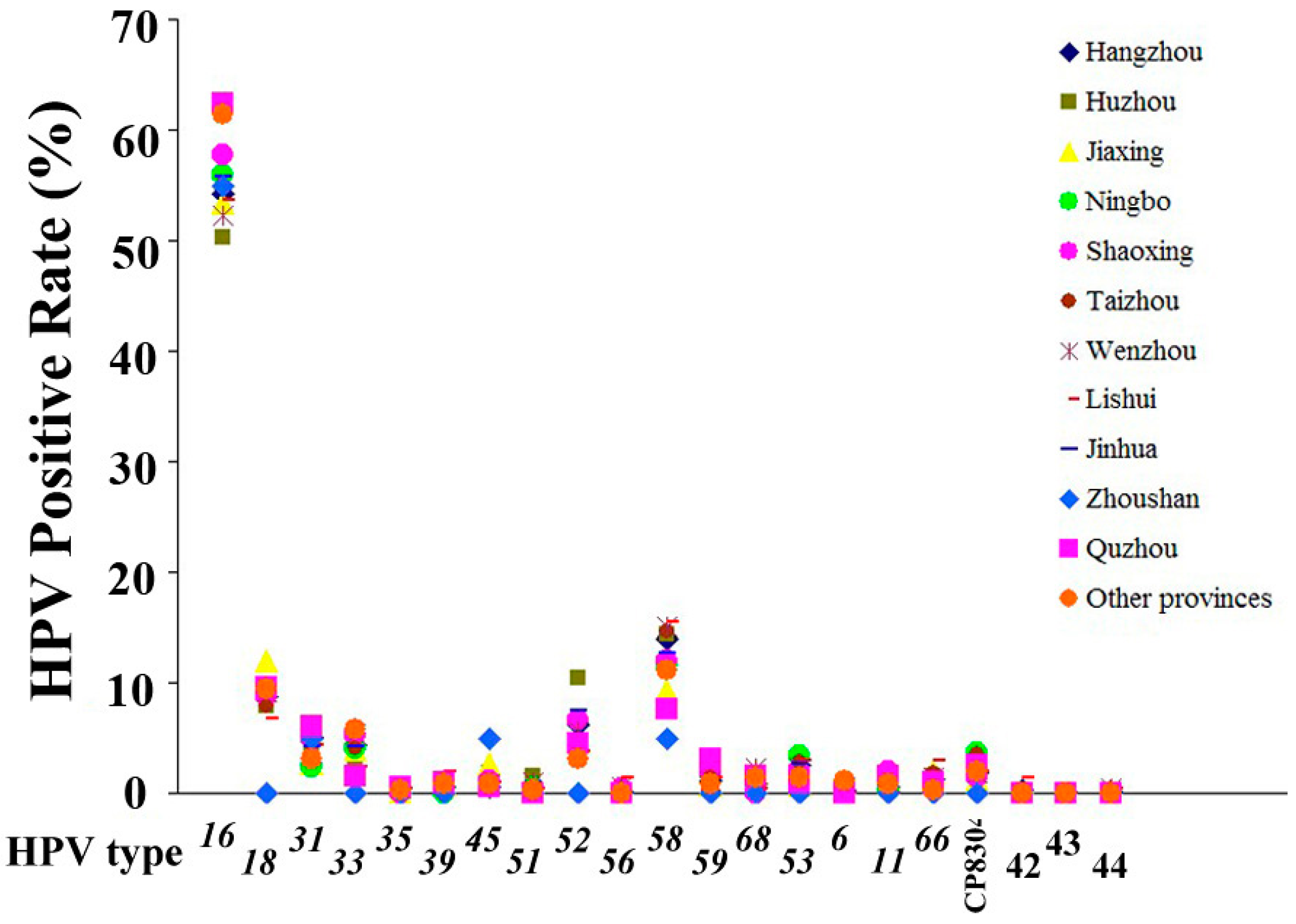
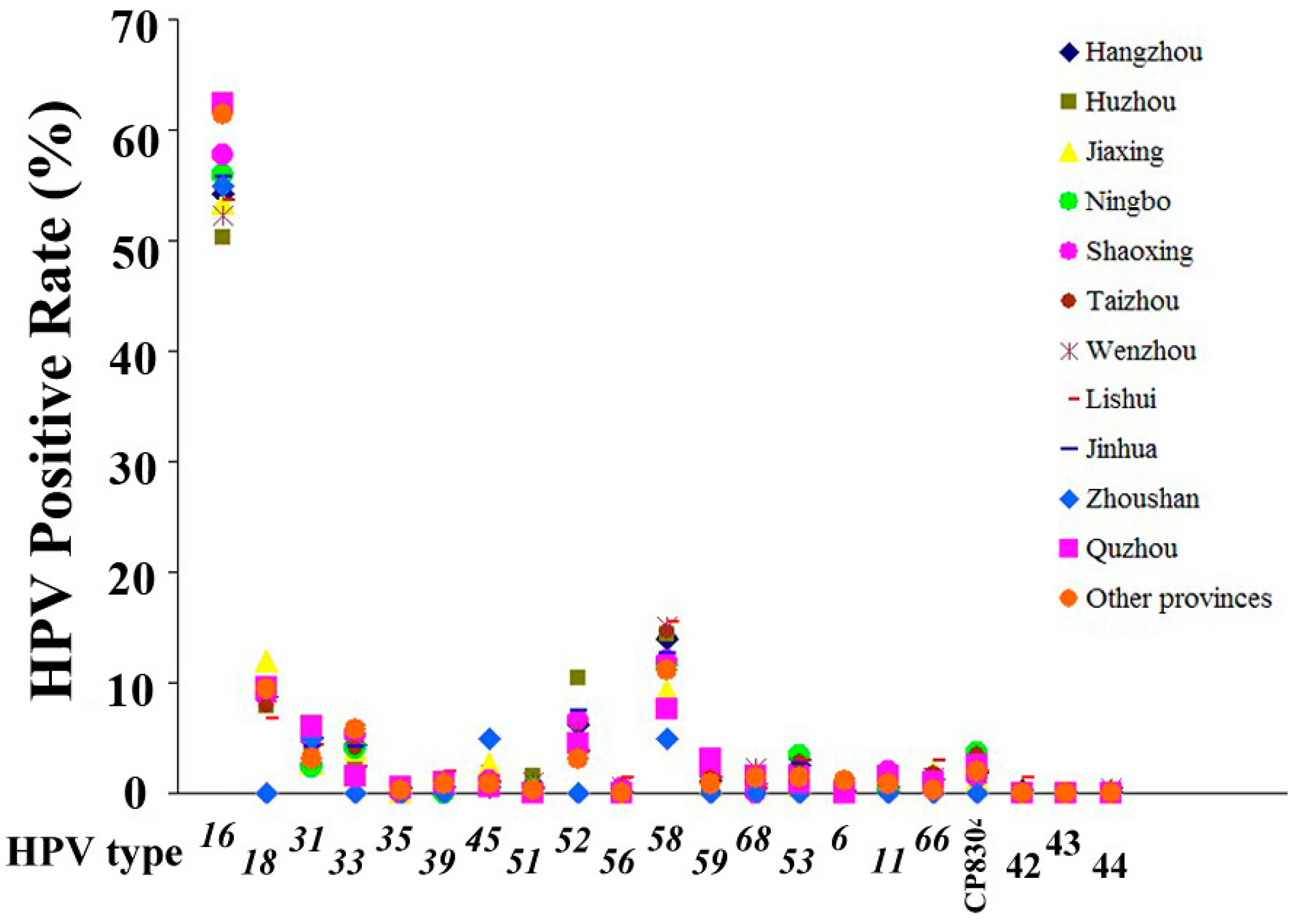
3.2. HPV Epidemiological Distribution
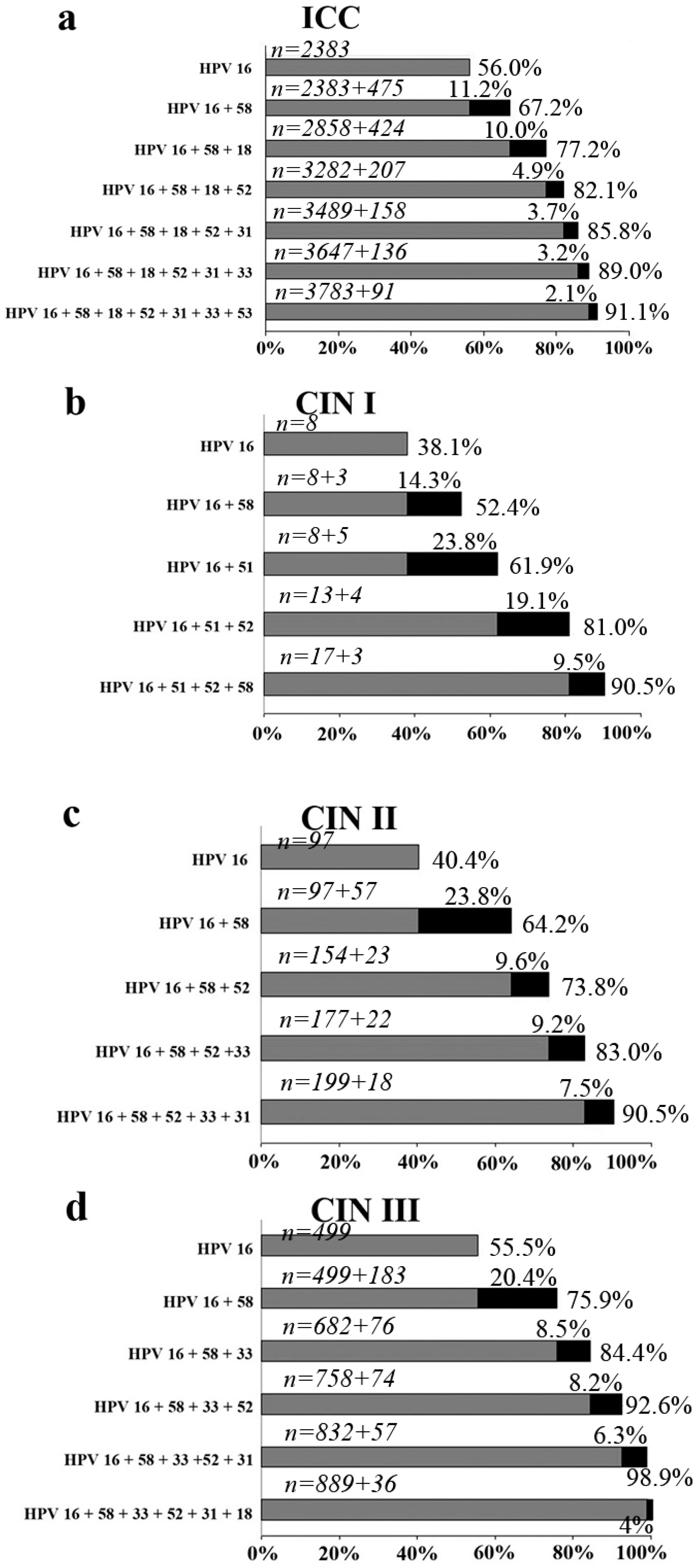
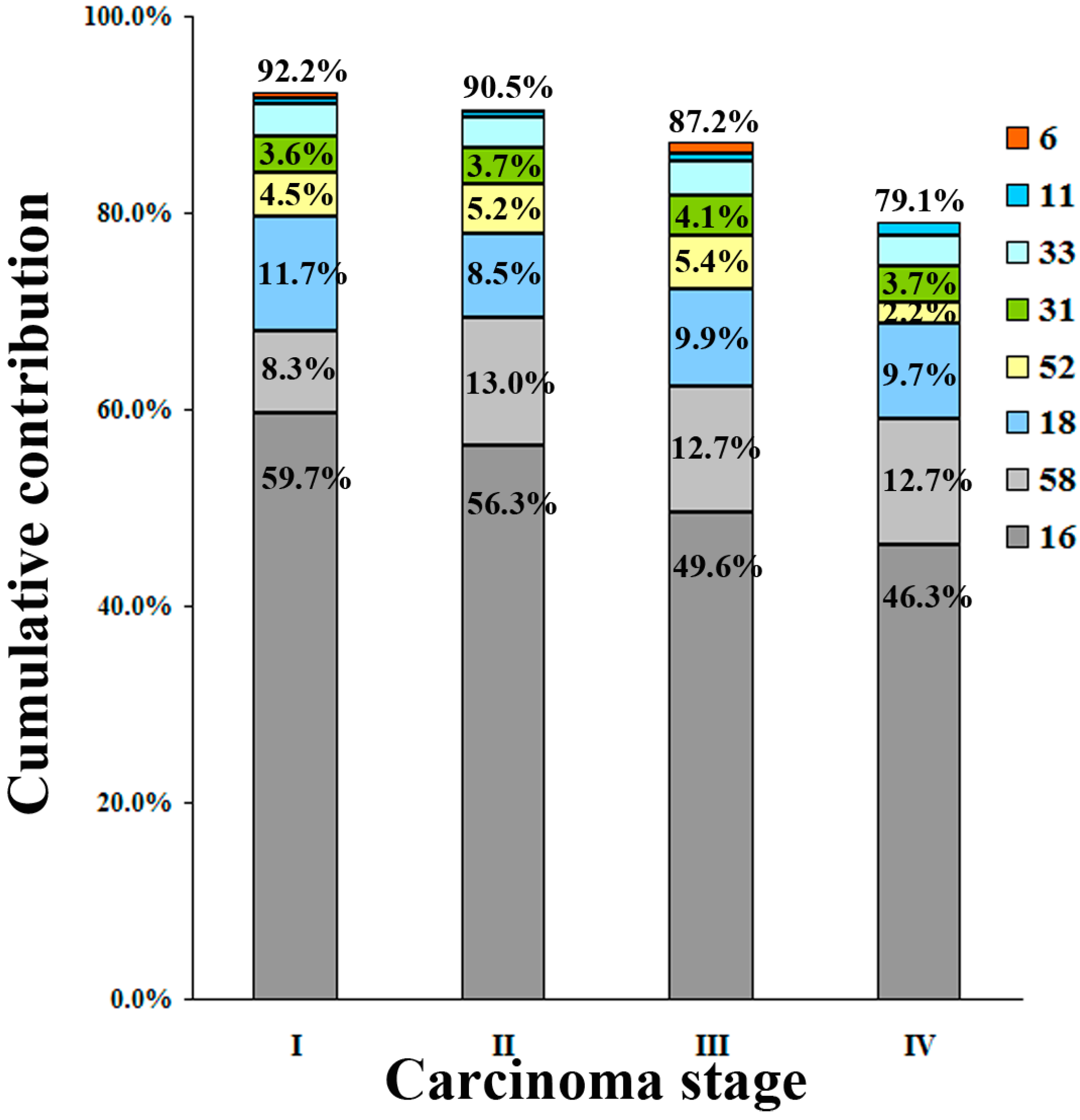
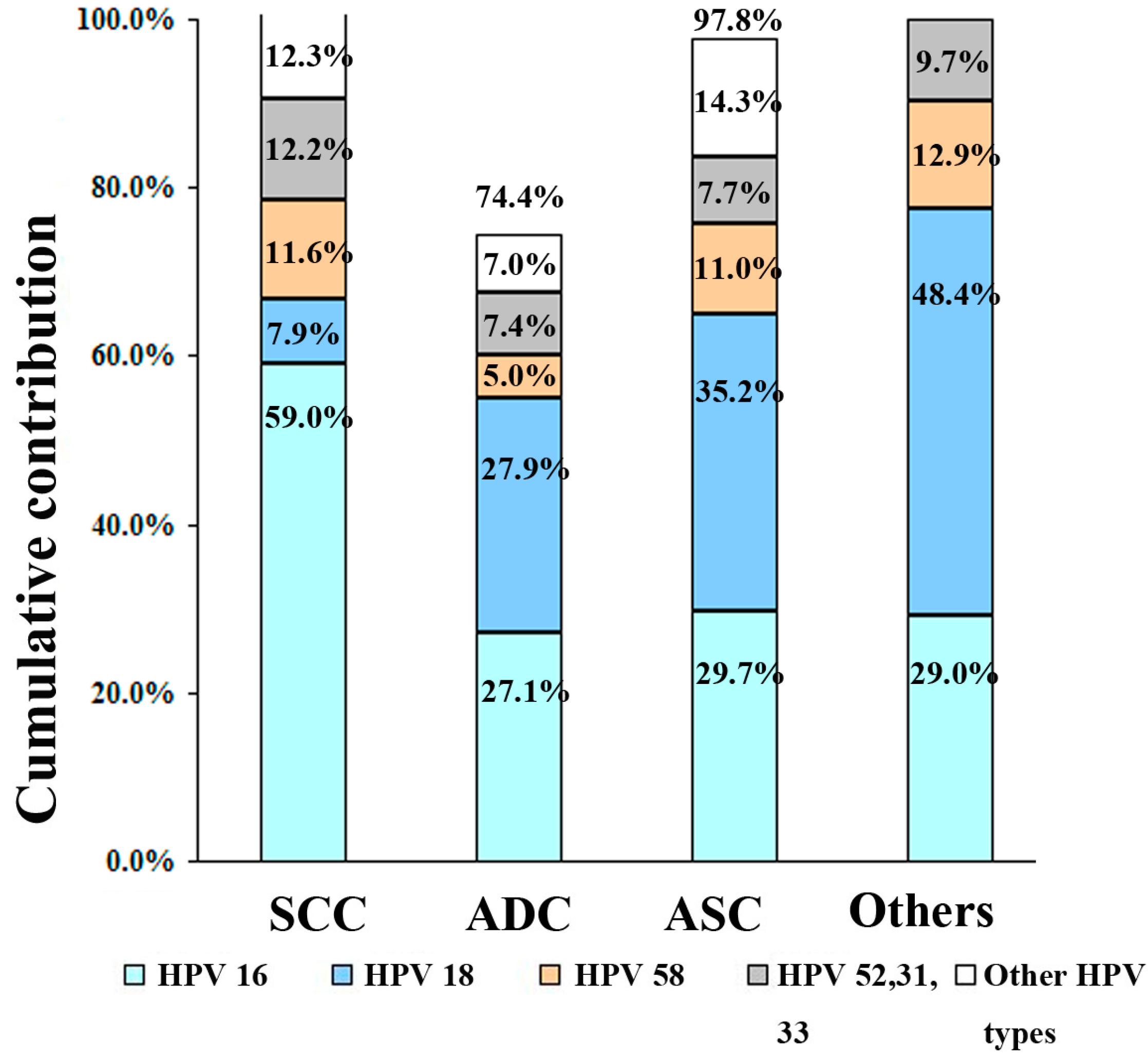
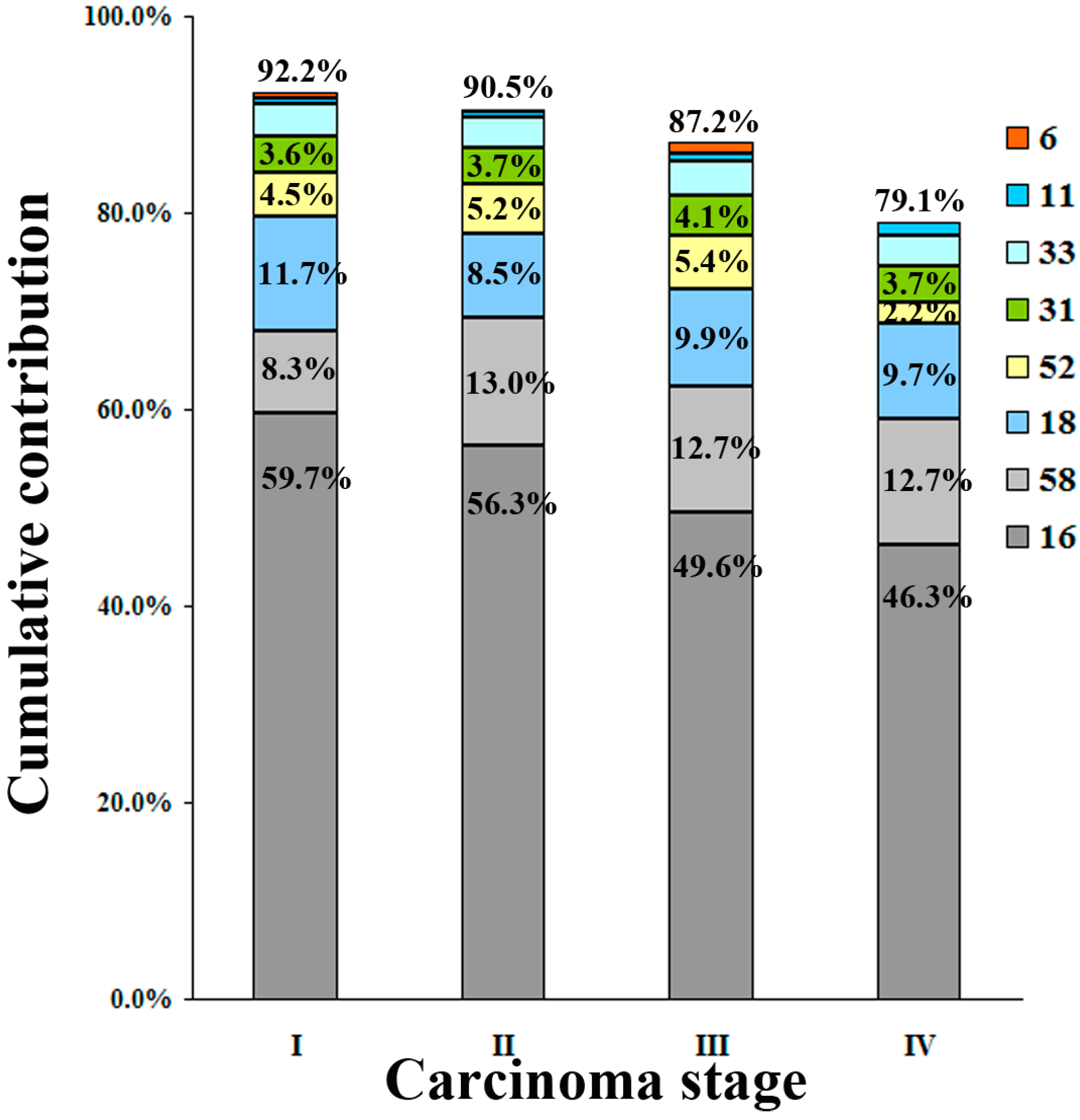
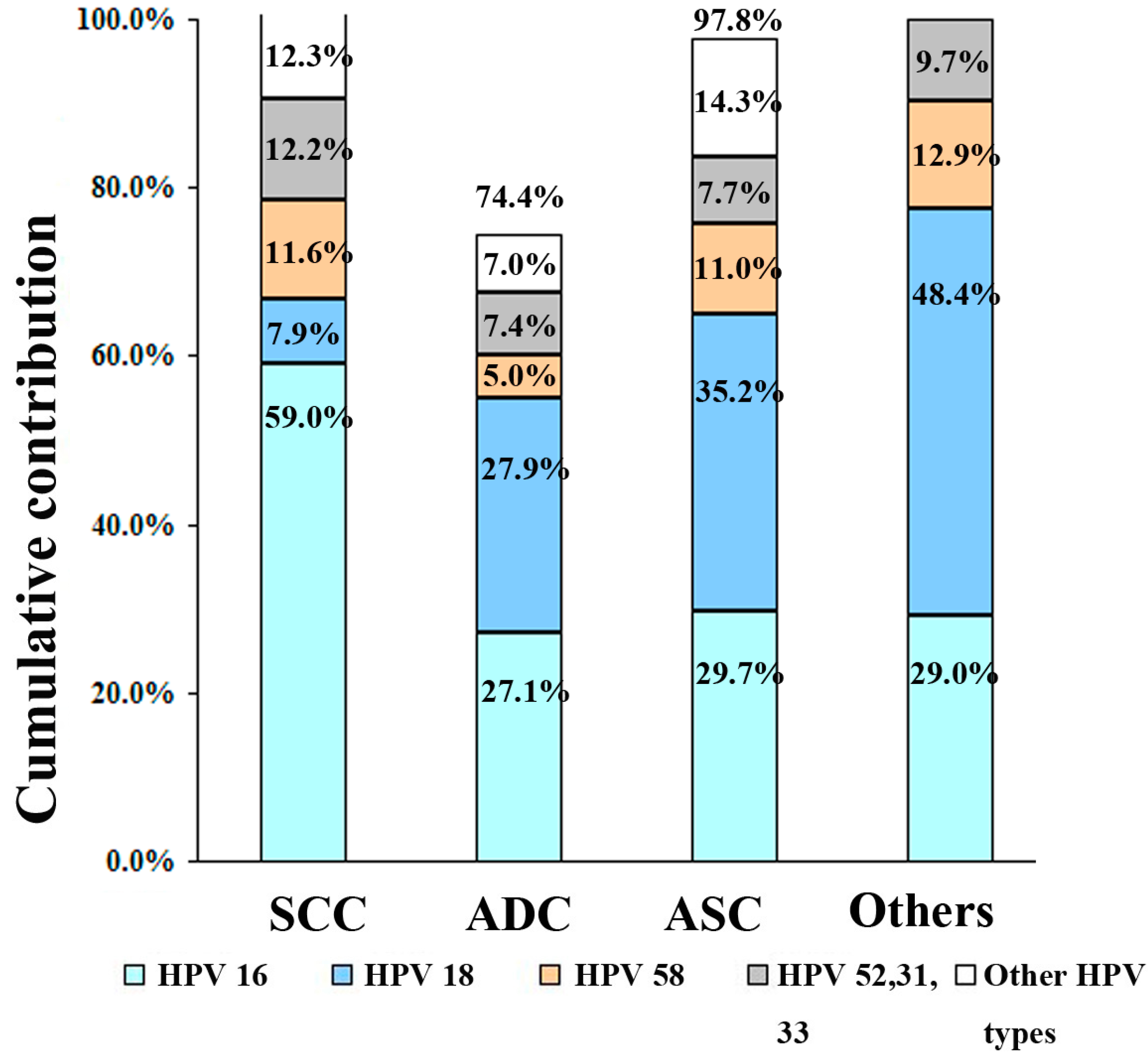
3.3. HPV Contribution in ICC
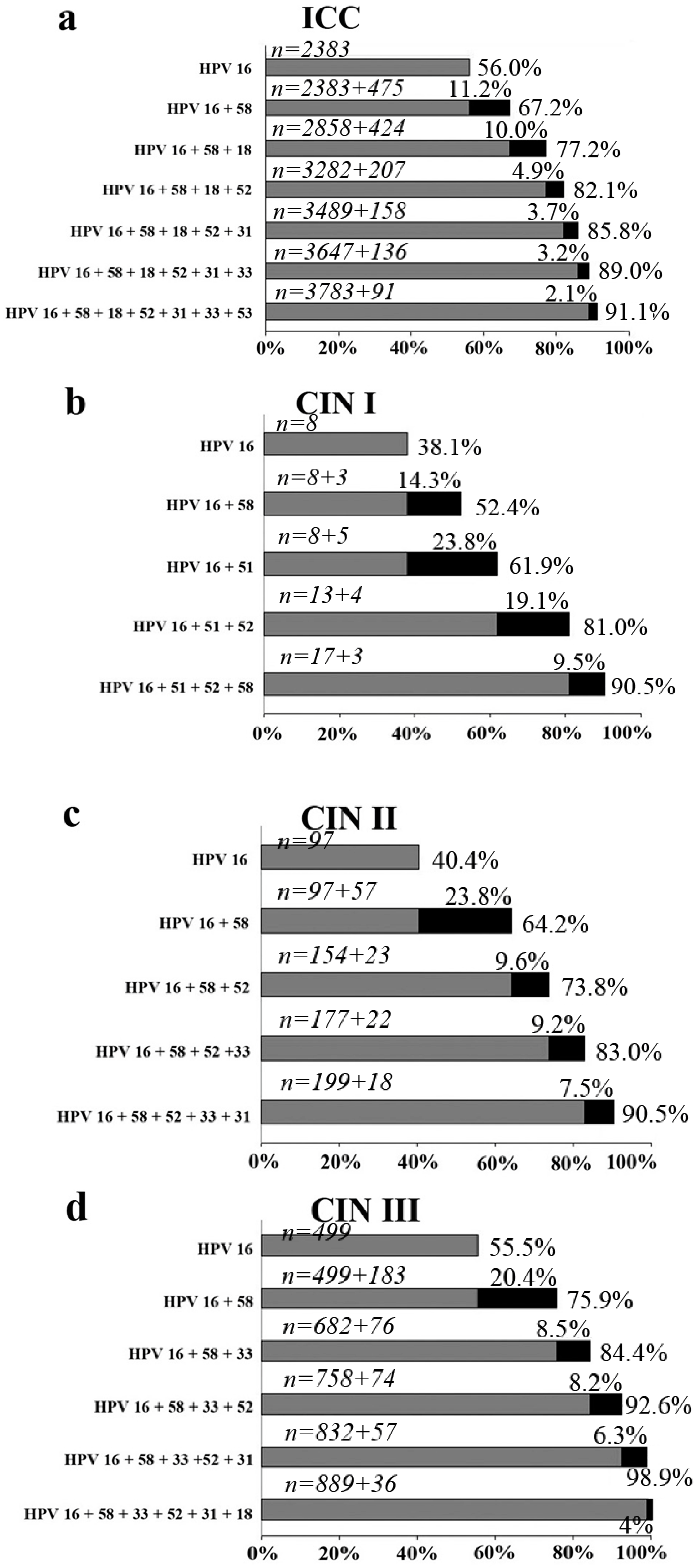
3.4. Vaccine Coverage
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| HPV | Human papillomavirus | SCC | squamous cell carcinoma | |
| hr-HPV | high-risk human papillomavirus | ADC | adenocarcinoma | |
| ICC | invasive cervical carcinoma | ASC | adenosquamous carcinoma | |
| CIN | cervical intraepithelial neoplasia |
References
- Ferlay, J.; Shin, H.-R.; Bray, F.; Forman, D.; Mathers, C.; Parkin, D.M. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int. J. Cancer 2010, 127, 2893–2917. [Google Scholar] [CrossRef] [PubMed]
- Jemal, A.; Bray, F.; Center, M.M.; Ferlay, J.; Ward, E.; Forman, D. Global cancer statistics. CA Cancer J. Clin. 2011, 61, 69–90. [Google Scholar] [CrossRef] [PubMed]
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Parkin, D.M.; Bray, F.; Ferlay, J.; Pisani, P. Global cancer statistics, 2002. CA Cancer J. Clin. 2005, 55, 74–108. [Google Scholar] [CrossRef] [PubMed]
- De Sanjose, S.; Quint, W.G.; Alemany, L.; Geraets, D.T.; Klaustermeier, J.E.; Lloveras, B.; Tous, S.; Felix, A.; Bravo, L.E.; Shin, H.R.; et al. Human papillomavirus genotype attribution in invasive cervical cancer: A retrospective cross-sectional survey. Lancet Oncol. 2010, 11, 1048–1056. [Google Scholar] [CrossRef]
- Clifford, G.M.; Gallus, S.; Herrero, R.; Muñoz, N.; Snijders, P.J.F.; Vaccarella, S.; Anh, P.T.H.; Ferreccio, C.; Hieu, N.T.; Matos, E.; et al. Worldwide distribution of human papillomavirus types in cytologically normal women in the International Agency for Research on Cancer HPV prevalence surveys: A pooled analysis. Lancet 2005, 366, 991–998. [Google Scholar] [CrossRef]
- Zur Hausen, H. Papillomaviruses and cancer: From basic studies to clinical application. Nat. Rev. Cancer 2002, 2, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Tao, P.; Zheng, W.; Wang, Y.; Bian, M. Sensitive HPV genotyping based on the flow-through hybridization and gene chip. J. Biomed. Biotechnol. 2012, 2012. [Google Scholar] [CrossRef] [PubMed]
- Freire, M.P.; Pires, D.; Forjaz, R.; Sato, S.; Cotrim, I.; Stiepcich, M.; Scarpellini, B.; Truzzi, J.C. Genital prevalence of HPV types and co-infection in men. Int. Braz. J. Urol. 2014, 40, 67–71. [Google Scholar] [PubMed]
- Walboomers, J.M.M.; Jacobs, M.V.; Manos, M.M.; Bosch, F.X.; Kummer, J.A.; Shah, K.V.; Snijders, P.J.; Peto, J.; Meijer, C.J.; Muñoz, N. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J. Pathol. 1999, 189, 12–19. [Google Scholar] [CrossRef]
- Ye, J.; Cheng, X.; Chen, X.; Ye, F.; Lü, W.; Xie, X. Prevalence and risk profile of cervical human papillomavirus infection in Zhejiang Province, southeast China: A population-based study. Virol. J. 2010, 7. [Google Scholar] [CrossRef] [PubMed]
- Safaeian, M.; Schiffman, M.; Gage, J.; Solomon, D.; Wheeler, C.M.; Castle, P.E. Detection of precancerous cervical lesions is differential by human papillomavirus type. Cancer Res. 2009, 69, 3262–3266. [Google Scholar] [CrossRef] [PubMed]
- Jaisamrarn, U.; Castellsagué, X.; Garland, S.M.; Naud, P.; Palmroth, J.; Del Rosario-Raymundo, M.R.; Wheeler, C.M.; Salmerón, J.; Chow, S.N.; Apter, D.; et al. Natural history of progression of HPV infection to cervical lesion or clearance: Analysis of the control arm of the large, randomised PATRICIA study. PLoS ONE 2013, 8. [Google Scholar] [CrossRef]
- Pista, A.; de Oliveira, C.F.; Cunha, M.J.; Paixao, M.T.; Real, O. Prevalence of human papillomavirus infection in women in Portugal: The CLEOPATRE Portugal Study. Int. J. Gynecol. Cancer 2011, 21, 1150–1158. [Google Scholar] [CrossRef] [PubMed]
- Balbi, G.; Napolitano, A.; Giordano, F.; Capuano, S.; Manganaro, M.A.; Di Martino, L.; Fusco, D.; Grauso, F.; Seguino, E. Role of the association of high-risk HPV identified by real-time PCR in cervical preneoplastic lesions. Eur. J. Gynaecol. Oncol. 2012, 33, 467–471. [Google Scholar] [PubMed]
- Trottier, H.; Mahmud, S.; Costa, M.C.; Sobrinho, J.P.; Duarte-Franco, E.; Rohan, T.E.; Ferenczy, A.; Villa, L.L.; Franco, E.L. Human papillomavirus infections with multiple types and risk of cervical neoplasia. Cancer Epidemiol. Biomarkers Prev. 2006, 15, 1274–1280. [Google Scholar] [CrossRef] [PubMed]
- Cuschieri, K.S.; Cubie, H.A.; Whitley, M.W.; Gilkison, G.; Arends, M.J.; Graham, C.; McGoogan, E. Persistent high risk HPV infection associated with development of cervical neoplasia in a prospective population study. J. Clin. Pathol. 2005, 58, 946–950. [Google Scholar] [CrossRef] [PubMed]
- Mammas, I.N.; Spandidos, D.A.; Sourvinos, G. Genomic diversity of human papillomaviruses (HPV) and clinical implications: An overview in adulthood and childhood. Infect. Genet. Evol. 2014, 21, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Nygård, M.; Hansen, B.T.; Dillner, J.; Munk, C.; Oddsson, K.; Tryggvadottir, L.; Hortlund, M.; Liaw, K.L.; Dasbach, E.J.; Kjær, S.K. Targeting human papillomavirus to reduce the burden of cervical, vulvar and vaginal cancer and pre-invasive neoplasia: Establishing the baseline for surveillance. PLoS ONE 2014, 9. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xu, X.-X.; Zhou, J.-S.; Yuan, S.-H.; Yu, H.; Lou, H.-M. Distribution of HPV Genotype in Invasive Cervical Carcinoma and Cervical Intraepithelial Neoplasia in Zhejiang Province, Southeast China: Establishing the Baseline for Surveillance. Int. J. Environ. Res. Public Health 2015, 12, 10794-10805. https://doi.org/10.3390/ijerph120910794
Xu X-X, Zhou J-S, Yuan S-H, Yu H, Lou H-M. Distribution of HPV Genotype in Invasive Cervical Carcinoma and Cervical Intraepithelial Neoplasia in Zhejiang Province, Southeast China: Establishing the Baseline for Surveillance. International Journal of Environmental Research and Public Health. 2015; 12(9):10794-10805. https://doi.org/10.3390/ijerph120910794
Chicago/Turabian StyleXu, Xiao-Xian, Jian-Song Zhou, Shu-Hui Yuan, Hua Yu, and Han-Mei Lou. 2015. "Distribution of HPV Genotype in Invasive Cervical Carcinoma and Cervical Intraepithelial Neoplasia in Zhejiang Province, Southeast China: Establishing the Baseline for Surveillance" International Journal of Environmental Research and Public Health 12, no. 9: 10794-10805. https://doi.org/10.3390/ijerph120910794
APA StyleXu, X.-X., Zhou, J.-S., Yuan, S.-H., Yu, H., & Lou, H.-M. (2015). Distribution of HPV Genotype in Invasive Cervical Carcinoma and Cervical Intraepithelial Neoplasia in Zhejiang Province, Southeast China: Establishing the Baseline for Surveillance. International Journal of Environmental Research and Public Health, 12(9), 10794-10805. https://doi.org/10.3390/ijerph120910794