
Evaluating the Effects of Temperature on Mortality in Manila City (Philippines) from 2006–2010 Using a Distributed Lag Nonlinear Model


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Site
2.2. Meteorological and Mortality Data
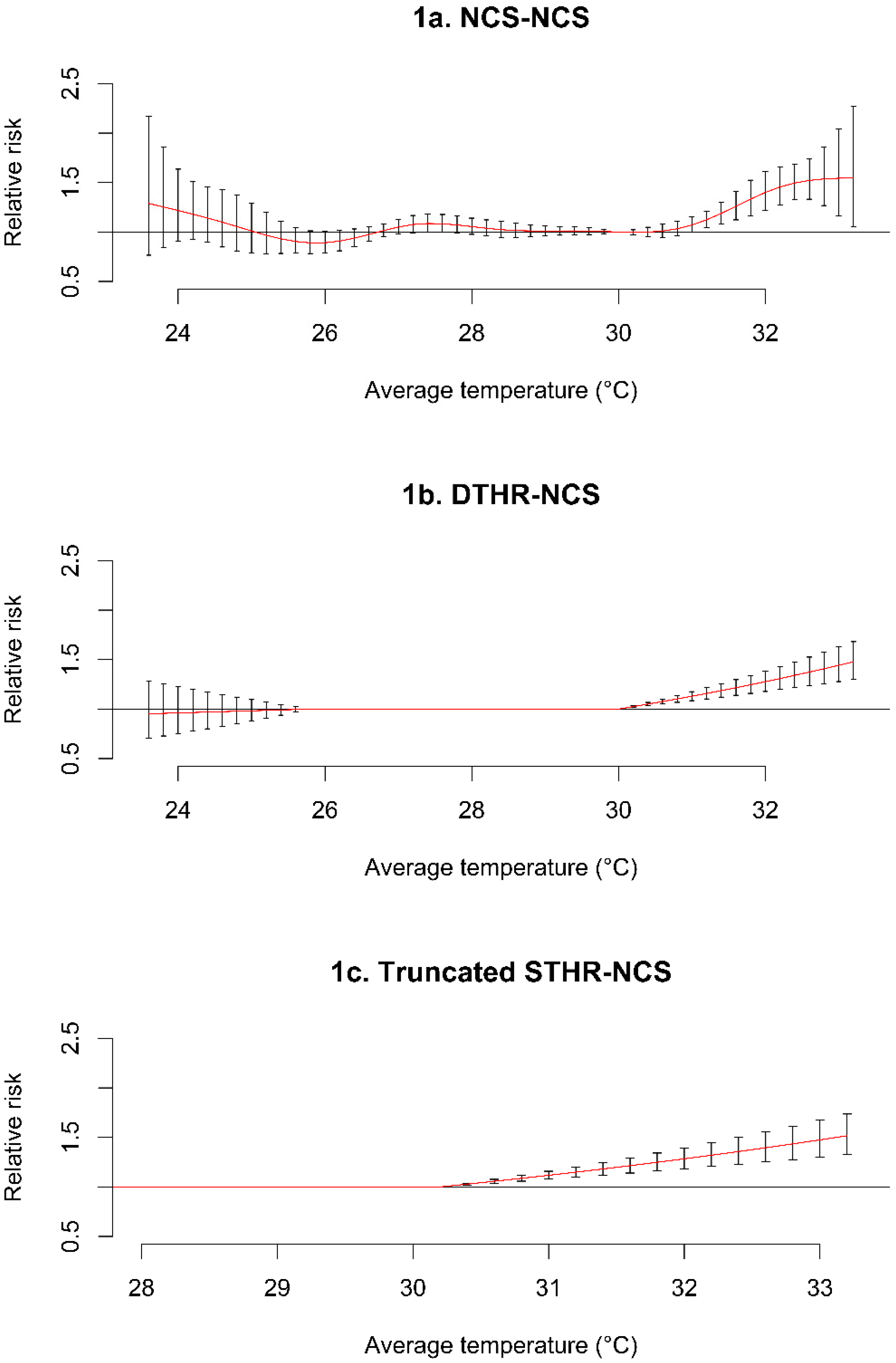
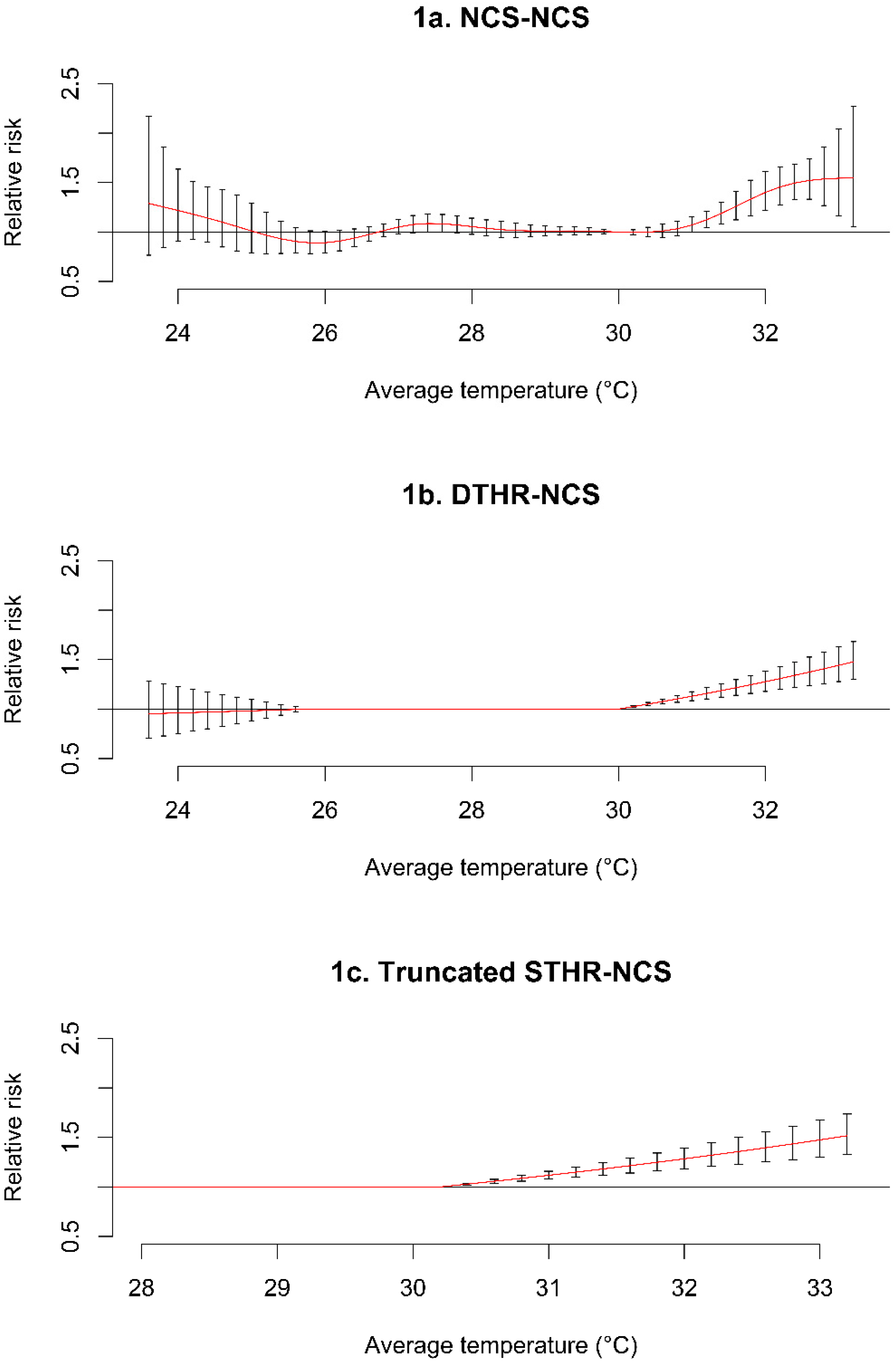
2.3. Modeling Approach
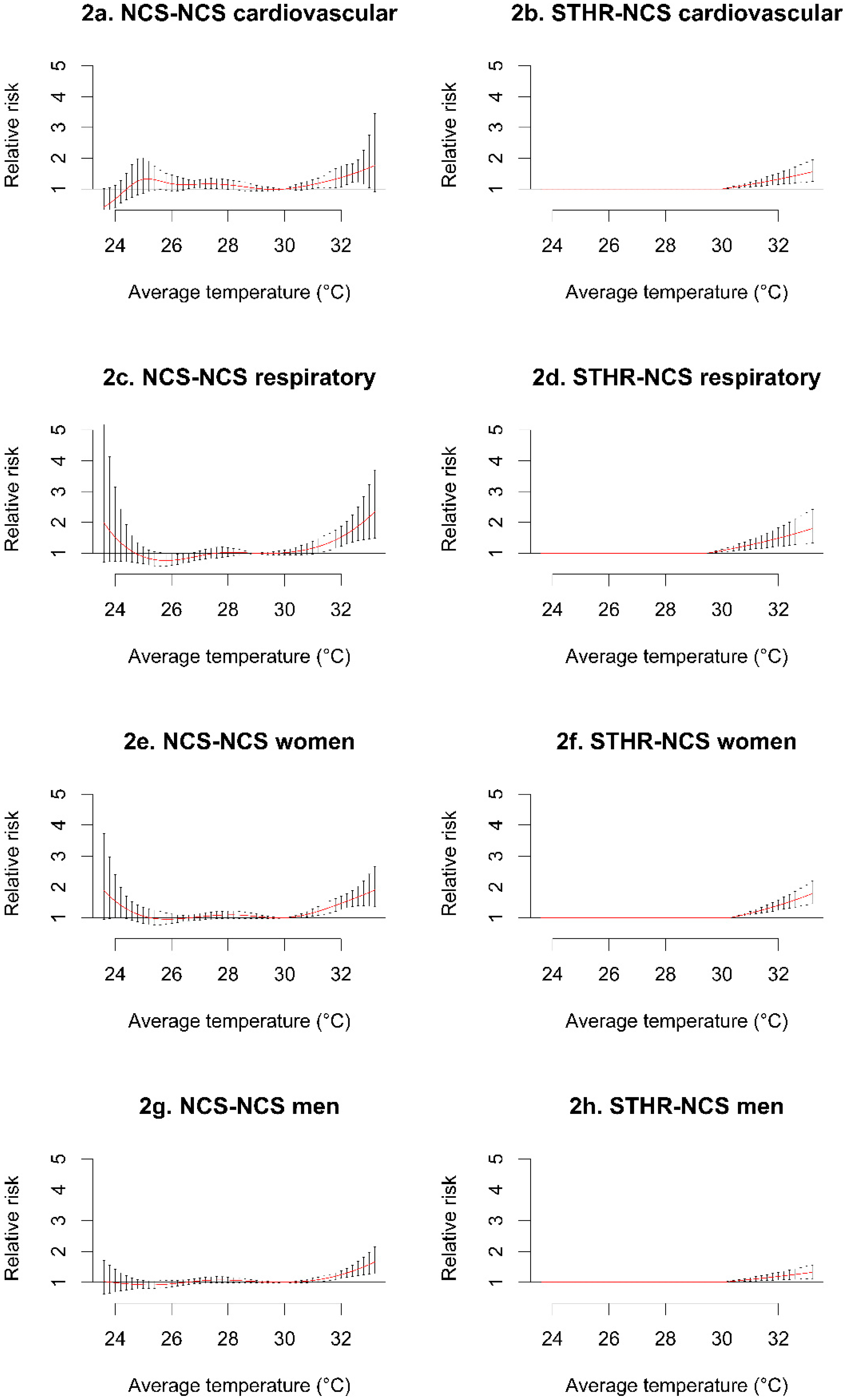
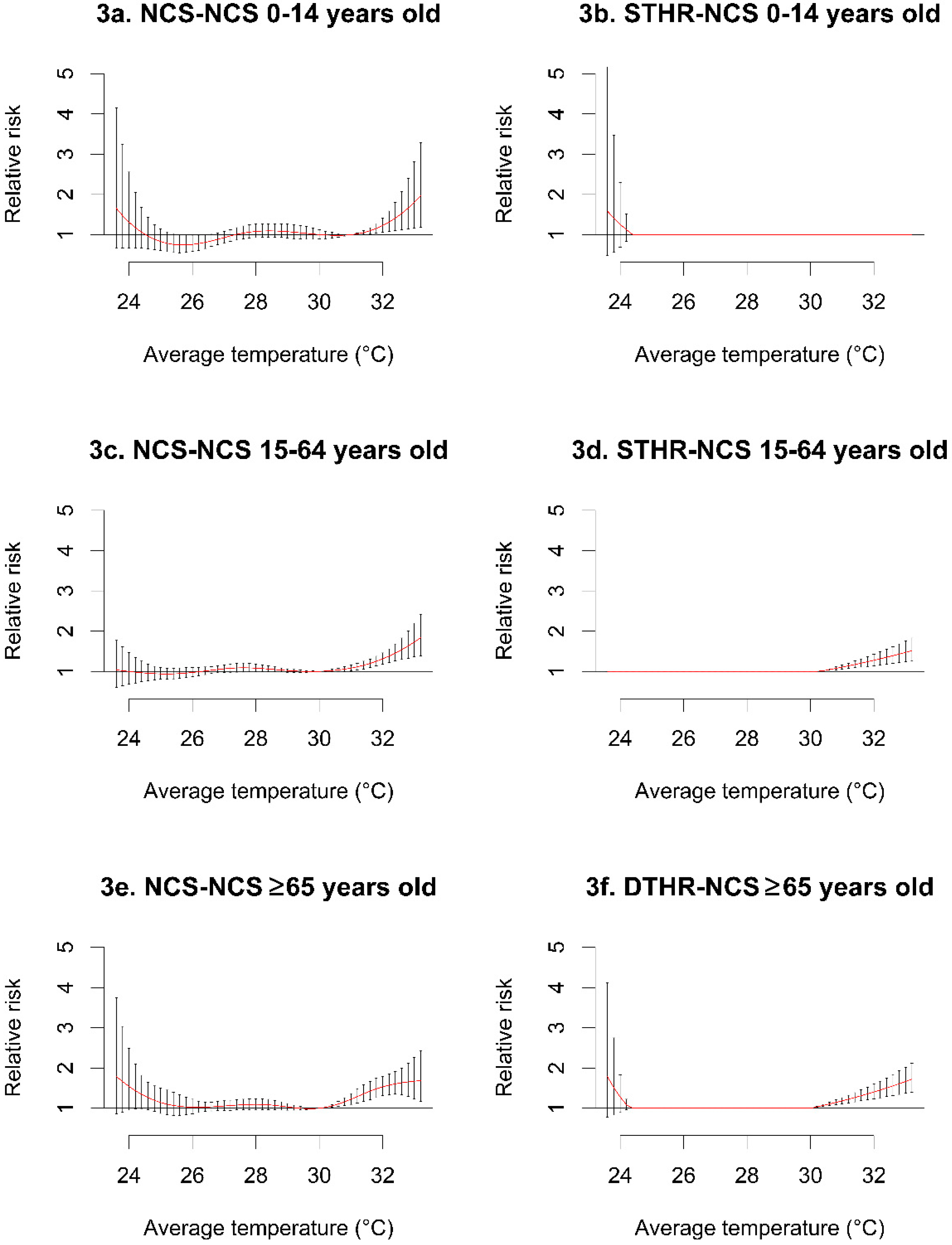
3. Results

{kind=link}
{kind=link}
{kind=link}
| Statistic | Mean | SD | Min | 10th Percentile | 50th Percentile | 90th Percentile | Max |
|---|---|---|---|---|---|---|---|
| Average temperature | 28.8 | 1.52 | 23.5 | 26.8 | 28.8 | 30.7 | 33.3 |
| Average relative humidity | 73.9 | 7.46 | 53.0 | 64.0 | 74.0 | 83.0 | 100 |
| Season-specific temperature | |||||||
| DJF | 27.6 | 1.19 | 23.5 | 26.1 | 27.6 | 29.0 | 30.5 |
| MAM | 29.8 | 1.36 | 24.8 | 28.2 | 29.8 | 31.5 | 33.3 |
| JJA | 29.1 | 1.37 | 24.8 | 27.3 | 29.2 | 30.8 | 32.5 |
| SON | 28.6 | 1.15 | 23.5 | 27.0 | 28.7 | 29.9 | 31.5 |
| All-cause mortality | 52.0 | 8.00 | 14.0 | 42.0 | 52.0 | 63.0 | 81.0 |
| Cause-specific mortality | |||||||
| Cardiovascular | 14.7 | 4.03 | 1.00 | 10.0 | 14.0 | 20.0 | 29.0 |
| Respiratory | 6.44 | 2.79 | 0.00 | 3.00 | 6.00 | 10.0 | 18.0 |
| Sex-specific mortality | |||||||
| Women | 22.3 | 5.24 | 3.00 | 16.0 | 22.0 | 29.0 | 38.0 |
| Men | 29.7 | 5.98 | 7.00 | 22.0 | 29.0 | 37.0 | 53.0 |
| Age-specific mortality | |||||||
| 0–14 years old | 8.70 | 3.23 | 0.00 | 5.00 | 9.00 | 13.0 | 21.0 |
| 15–64 years old | 26.5 | 5.68 | 6.00 | 20.0 | 26.0 | 34.0 | 48.0 |
| ≥65 years old | 16.7 | 4.31 | 2.00 | 11.0 | 16.0 | 22.0 | 31.0 |
| Season-specific mortality | |||||||
| DJF | 51.4 | 7.33 | 31.0 | 42.0 | 51.0 | 61.0 | 70.0 |
| MAM | 50.1 | 8.37 | 27.0 | 40.0 | 49.0 | 61.0 | 81.0 |
| JJA | 52.8 | 9.02 | 14.0 | 42.0 | 52.0 | 64.0 | 78.0 |
| SON | 53.3 | 8.53 | 15.0 | 43.0 | 53.0 | 64.0 | 75.0 |
| Statistic | 1st Percentile (RRFit) | 95% CI | 5th Percentile (RRFit) | 95% CI | 95th Percentile (RRFit) | 95% CI | 99th Percentile (RRFit) | 95% CI | MMT (°C) |
|---|---|---|---|---|---|---|---|---|---|
| All-cause mortality | 1.01 | (0.79–1.29) | 0.89 | (0.79–1.01) | 1.07 | (1.00–1.15) | 1.40 | (1.22–1.61) | 30 |
| Cause-specific mortality | |||||||||
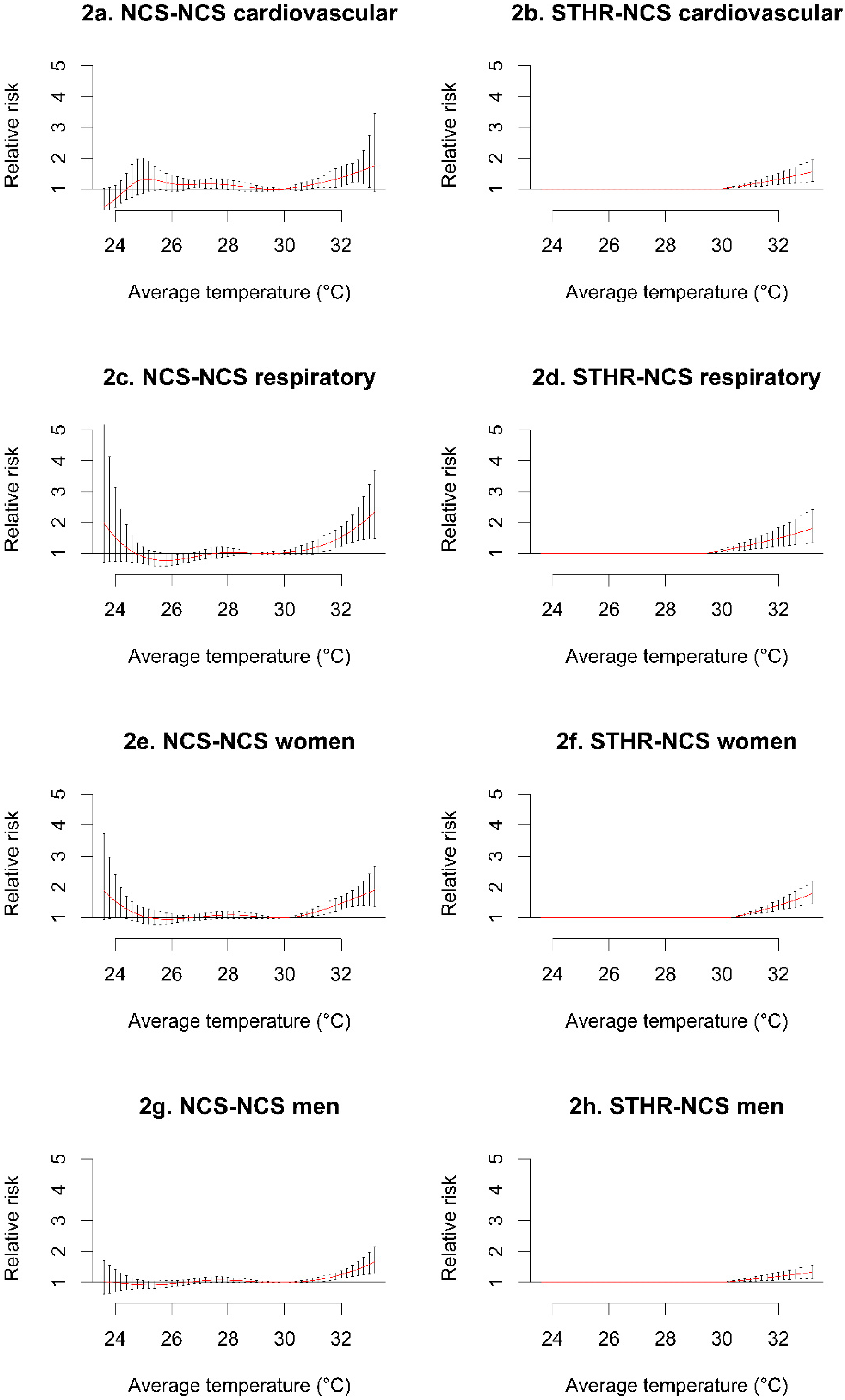
| Cardiovascular | 1.32 | (0.87–2.01) | 1.17 | (0.94–1.45) | 1.15 | (1.01–1.30) | 1.37 | (1.07–1.75) | 30 |
| Respiratory | 0.88 | (0.65–1.19) | 0.77 | (0.60–0.98) | 1.16 | (0.97–1.39) | 1.52 | (1.23–1.88) | 29 |
| Sex-specific mortality | |||||||||
| Women | 1.05 | (0.82–1.35) | 0.96 | (0.82–1.12) | 1.16 | (1.05–1.28) | 1.47 | (1.27–1.69) | 30 |
| Men | 0.92 | (0.80–1.06) | 0.95 | (0.85–1.06) | 1.06 | (0.99–1.13) | 1.24 | (1.13–1.37) | 30 |
| Age-specific mortality | |||||||||
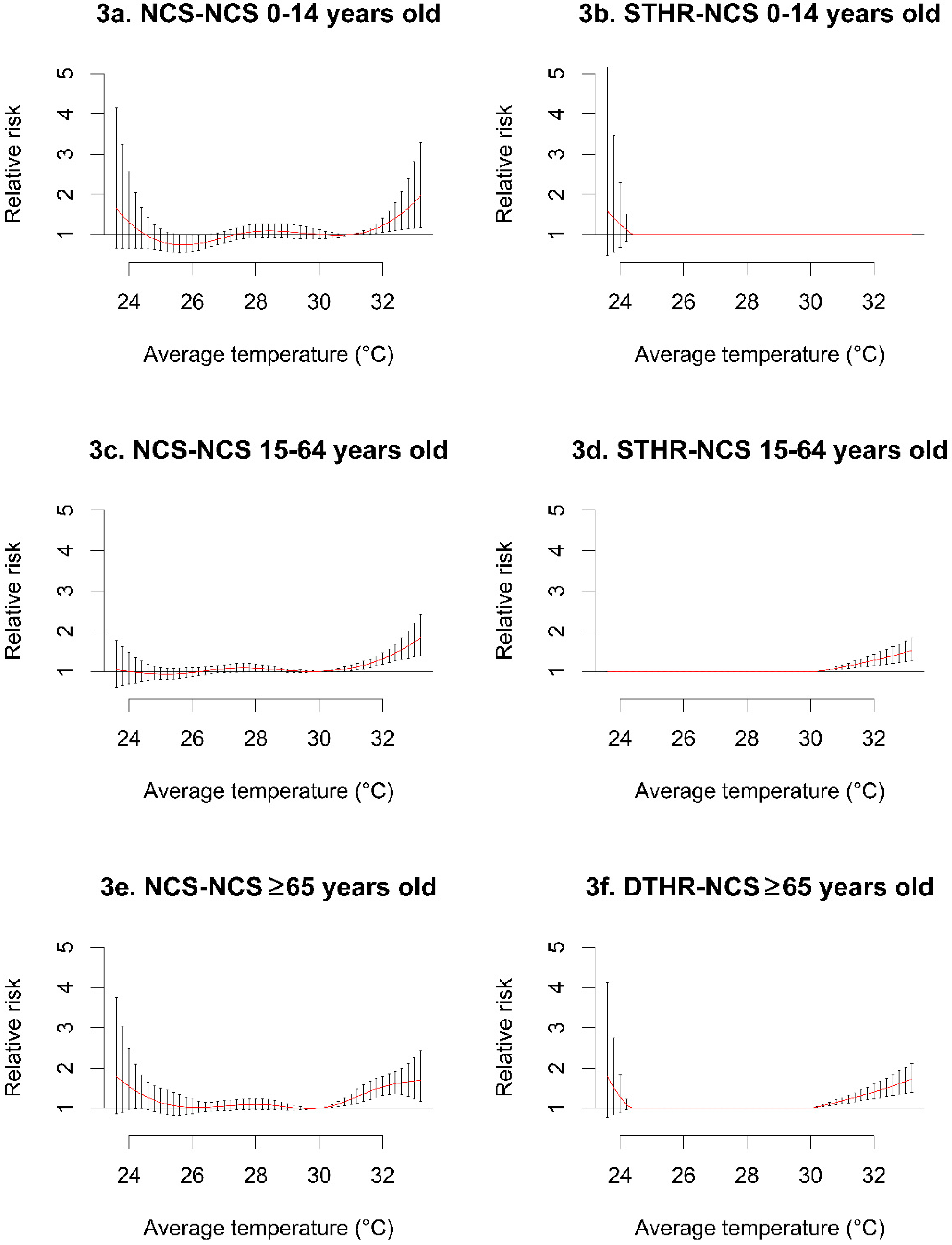
| 0–14 years old | 0.83 | (0.61–1.14) | 0.76 | (0.58–0.99) | – | – | 1.23 | (1.07–1.41) | 31 |
| 15–64 years old | 0.94 | (0.80–1.09) | 0.97 | (0.86–1.10) | 1.08 | (1.01–1.16) | 1.31 | (1.18–1.46) | 30 |
| ≥65 years old | 1.14 | (0.87–1.50) | 1.03 | (0.86–1.22) | 1.22 | (1.10–1.37) | 1.53 | (1.31–1.80) | 30 |
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Curriero, F.C.; Heiner, K.S.; Samet, J.M.; Zeger, S.L.; Strug, L.; Patz, J.A. Temperature and mortality in 11 cities of the eastern United States. Amer. J. Epidemiol. 2002, 155, 80–87. [Google Scholar] [CrossRef]
- Ha, J.; Shin, Y.; Kim, H. Distributed lag effects in the relationship between temperature and mortality in three major cities in South Korea. Sci. Total Environ. 2011, 409, 3274–3280. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Punnasiri, K.; Tong, S. Effects of temperature on mortality in Chiang Mai city, Thailand: A time series study. Environ. Health 2012. [Google Scholar] [CrossRef] [PubMed]
- Xuan, L.T.T.; Egondi, T.; Ngoan, L.T.; Toan, D.T.T.; Huong, L.T. Seasonality in mortality and its relationship to temperature among the older population in Hanoi, Vietnam. Glob. Health Action 2014. [Google Scholar] [CrossRef]
- Chung, J.Y.; Honda, Y.; Hong, Y.C.; Pan, X.C.; Guo, Y.L.; Kim, H. Ambient temperature and mortality: An international study in four capital cities of East Asia. Sci. Total Environ. 2009, 408, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Lin, Y.K.; Ho, T.J.; Wang, Y.C. Mortality risk associated with temperature and prolonged temperature extremes in elderly populations in Taiwan. Environ. Res. 2011, 111, 1156–1163. [Google Scholar] [CrossRef] [PubMed]
- El-Zein, A.; Tewtel-Salem, M.; Nehme, G. A time-series analysis of mortality and air temperature in Greater Beirut. Sci. Total Environ. 2004, 330, 71–80. [Google Scholar] [CrossRef] [PubMed]
- Huynen, M.M.; Martens, P.; Schram, D.; Weijenberg, M.P.; Kunst, A.E. The impact of heat waves and cold spells on mortality rates in the Dutch population. Environ. Health Perspect. 2001, 109, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Ishigami, A.; Hajat, S.; Kovats, R.S.; Bisanti, L.; Rognoni, M.; Russo, A.; Paldy, A. An ecological time-series study of heat-related mortality in three European cities. Environ. Health 2008. [Google Scholar] [CrossRef] [PubMed]
- Plavcova, E.; Kysely, J. Relationships between sudden weather changes in summer and mortality in the Czech Republic, 1986–2005. Int. J. Biometeorol. 2010, 54, 539–551. [Google Scholar] [CrossRef] [PubMed]
- Breitner, S.; Wolf, K.; Devlin, R.B.; Diaz-Sanchez, D.; Peters, A.; Schneider, A. Short-term effects of air temperature on mortality and effect modification by air pollution in three cities of Bavaria, Germany: A time-series analysis. Sci. Total Environ. 2014, 485, 49–61. [Google Scholar] [CrossRef] [PubMed]
- PSA-NSO. Philippine Counts—National Capital Region, 2010. Available online: http://census.gov.ph/sites/default/files/attachments/hsd/pressrelease/National%20Capital%20Region.pdf (accessed on 15 December 2014).
- Cinco, T.A.; Hilario, F.D.; de Guzman, R.G.; Ares, E.D. Climate Trends and Projections in the Philippines. In Proceedings of the 12th National Convention on Statistics (NCS); Philippine Atmospheric,, Mandaluyong, Philippines, 1–2 October 2013, Geophysical and Astronomical Services Administration (PAGASA): Quezon City, Philippines, 2013; p. 20. [Google Scholar]
- Gouveia, N.; Hajat, S.; Armstrong, B. Socioeconomic differentials in the temperature-mortality relationship in Sao Paulo, Brazil. Int. J. Epidemiol. 2003, 32, 390–397. [Google Scholar] [CrossRef] [PubMed]
- Ha, J.; Kim, H.; Hajat, S. Effect of previous-Winter mortality on the association between Summer temperature and mortality in South Korea. Environ. Health Perspect. 2011, 119, 542–546. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A.; Armstrong, B.; Kenward, M.G. Distributed lag non-linear models. Stat. Med. 2010, 29, 2224–2234. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A.; Armstrong, B. Reducing and meta-analysing estimates from distributed lag non-linear models. BMC Med. Res. Methodol. 2013, 13. [Google Scholar] [CrossRef] [PubMed]
- Gasparrini, A. Distributed lag linear and non-linear models in R: The package DLNM. J. Stat. Softw. 2011, 43, 1–20. [Google Scholar] [PubMed]
- Gasparrini, A.; Armstrong, B.; Kovat, S.; Wilkinson, P. The effect of high temperatures on cause-specific mortality in England and Wales. Occup. Environ. Med. 2012, 69, 56–61. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Barnett, A.G.; Tong, S. Spatiotemporal model or time series model for assessing city-wide temperature effects on mortality? Environ. Res. 2013, 120, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Motohashi, Y.; Takano, T.; Nakamura, K.; Nakata, K.; Tanaka, M. Seasonality of mortality in Sri Lanka: Biometeorological considerations. Int. J. Biometeorol. 1996, 39, 121–126. [Google Scholar] [CrossRef] [PubMed]
- Ballester, F.; Corella, D.; Pérez-Hoyos, S.; Sáez, M.; Hervás, A. Mortality as a function of temperature. A study in Valencia, Spain, 1991–1993. Int. J. Epidemiol. 1997, 26, 551–561. [Google Scholar] [CrossRef] [PubMed]
- D’Ippoliti, D.; Michelozzi, P.; Marino, C.; de’Donato, F.; Menne, B.; Katsouyanni, K.; Kirchmayer, U.; Analitis, A.; Medina-Ramón, M.; Paldy, A.; et al. The impact of heat waves on mortality in 9 European cities: Results from the EuroHEAT project. Environ. Health 2010. [Google Scholar] [CrossRef]
- Pell, J.P.; Cobbe, S.M. Seasonal variations in coronary heart disease. QJM 1999, 92, 689–696. [Google Scholar] [CrossRef] [PubMed]
- Son, J.Y.; Lee, J.T.; Anderson, G.B.; Bell, M.L. The impact of heat waves on mortality in seven major cities in Korea. Environ. Health Perspect. 2012, 120, 566–571. [Google Scholar] [CrossRef] [PubMed]
- Xiang, J.; Bi, P.; Pisaniello, D.; Hansen, A. The impact of heatwaves on workers’ health and safety in Adelaide, South Australia. Environ. Res. 2014, 133, 90–95. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.; Feng, W.Y.; Ostro, B.D. Characterizing temperature and mortality in nine California counties. Epidemiology 2008, 19, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Kan, H.; Kovats, S. The impact of the 2003 heat wave on mortality in Shanghai, China. Sci. Total Environ. 2010, 408, 2418–2420. [Google Scholar] [CrossRef] [PubMed]
- Zeng, W.; Lao, X.; Rutherford, S.; Xu, Y.; Xu, X.; Lin, H.; Liu, T.; Luo, Y.; Xiao, J.; Hu, M.; et al. The effect of heat waves on mortality and effect modifiers in four communities of Guangdong province, China. Sci. Total Environ. 2014, 482–483, 214–221. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.; Zeng, W.; Zhou, M.; Wang, L.; Rutherford, S.; Lin, H.; Liu, T.; Zhang, Y.; Xiao, J.; Zhang, Y.; et al. The short-term effect of heat waves on mortality and its modifiers in China: An analysis from 66 communities. Environ. Int. 2015, 75, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.; Ostro, B.D. A multicounty analysis identifying the populations vulnerable to mortality associated with high ambient temperature in California. Amer. J. Epidemiol. 2008, 168, 632–637. [Google Scholar] [CrossRef] [PubMed]
- Michelozzi, P.; Accetta, G.; de Sario, M.; D’Ippoliti, D.; Marino, C.; Baccini, M.; Biggeri, A.; Anderson, H.R.; Katsouyanni, K.; Ballester, F.; et al. High temperature and hospitalizations for cardiovascular and respiratory causes in 12 European cities. Amer. J. Respir. Crit. Care Med. 2009, 179, 383–389. [Google Scholar] [CrossRef] [PubMed]
- Carlton, E.J.; Eisenberg, J.N.; Goldstick, J.; Cevallos, W.; Trostle, J.; Levy, K. Heavy rainfall events and diarrhea incidence: The role of social and environmental factors. Amer. J. Epidemiol. 2014, 179, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, P.; Campbell-Lendrum, D.H.; Bartlett, C.L. Monitoring the health effects of climate change. In Quantitative Risk Assessment of the Effects of Climate Change on Selected Causes of Death, 2030s and 2050s; Hates, S., Kovats, S., Lloyd, S., Campbell-Lendrum, D., Eds.; WHO Press: Geneva, Switzerland, 2014. [Google Scholar]
- Chadsuthi, S.; Modchang, C.; Lenbury, Y.; Iamsirithaworn, S.; Triampo, W. Modeling seasonal leptospirosis transmission and its association with rainfall and temperature in Thailand using time-series and ARIMAX analyses. Asian Pac. J. Trop. Med. 2012, 5, 539–546. [Google Scholar] [CrossRef]
- NEC. Philippine Integrated Disease Surveillance and Response (PIDSR) Annual Report 2009; Public Health Surveillance and Informatics Division , Ed.; Department of Health: Manila, Philippines, 2009; p. 46.
- Guo, Y.; Li, S.; Tawatsupa, B.; Punnasiri, K.; Jaakkola, J.J.K.; Williams, G. The association between air pollution and mortality in Thailand. Sci. Rep. 2014, 4. [Google Scholar] [CrossRef] [PubMed]
- Bell, M.L.; O’Neill, M.S.; Ranjit, N.; Borja-Aburto, V.H.; Cifuentes, L.A.; Gouveia, N.C. Vulnerability to heat-related mortality in Latin America: A case-crossover study in Sao Paulo, Brazil, Santiago, Chile and Mexico City, Mexico. Int. J. Epidemiol. 2008, 37, 796–804. [Google Scholar] [CrossRef] [PubMed]
- Pinheiro, S.D.L.D.; Saldiva, P.H.N.; Schwartz, J.; Zanobetti, A. Isolated and synergistic effects of PM10 and average temperature on cardiovascular and respiratory mortality. Rev. Saude Publ. 2014, 48, 881–888. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seposo, X.T.; Dang, T.N.; Honda, Y. Evaluating the Effects of Temperature on Mortality in Manila City (Philippines) from 2006–2010 Using a Distributed Lag Nonlinear Model. Int. J. Environ. Res. Public Health 2015, 12, 6842-6857. https://doi.org/10.3390/ijerph120606842
Seposo XT, Dang TN, Honda Y. Evaluating the Effects of Temperature on Mortality in Manila City (Philippines) from 2006–2010 Using a Distributed Lag Nonlinear Model. International Journal of Environmental Research and Public Health. 2015; 12(6):6842-6857. https://doi.org/10.3390/ijerph120606842
Chicago/Turabian StyleSeposo, Xerxes T., Tran Ngoc Dang, and Yasushi Honda. 2015. "Evaluating the Effects of Temperature on Mortality in Manila City (Philippines) from 2006–2010 Using a Distributed Lag Nonlinear Model" International Journal of Environmental Research and Public Health 12, no. 6: 6842-6857. https://doi.org/10.3390/ijerph120606842
APA StyleSeposo, X. T., Dang, T. N., & Honda, Y. (2015). Evaluating the Effects of Temperature on Mortality in Manila City (Philippines) from 2006–2010 Using a Distributed Lag Nonlinear Model. International Journal of Environmental Research and Public Health, 12(6), 6842-6857. https://doi.org/10.3390/ijerph120606842