1. Introduction
Depressive symptoms have been in the limelight around the world. Depression has affected people from all walks of life, such as employees, college students, nurses and so on [
1,
2,
3]. Depression not only affects people’s quality of life, but it also affects workplace productivity and can lead to direct economic costs [
4,
5]. Nurses are considered an at-risk population for depressive symptoms [
6,
7]. As an indispensable part of the workforce in the healthcare system, nurses work at hospitals under immense physical and psychological pressure. The negative psychosocial factors in the job environment are linked to underdeveloped psychological and physical health in nurses of some countries. Meanwhile, depressive symptoms among nurses affect the quality of their work, which have an influence on patients’ health. It is reported that depressive symptoms of nurses were related to the perception of lower patient safety [
6]. In China, the proportion of nurses to the general population is 1:1750, which is lower than those of developed countries (1:140–1:320) and the majority of countries in the world (1:330) [
8,
9]. The huge population and the shortage of nurses is more likely to trigger depressive symptoms among Chinese nurses. Therefore, exploring the risk factors of nurses’ depressive symptoms is crucial to improve nurses’ health, and more importantly, increase the quality of health care services in China.
Among occupational groups, some social and psychological outcomes have been identified as risk factors for depressive symptoms [
6,
10]. Work-family conflict (WFC) is a bidirectional conflict that includes both WFC and family-work conflict (FWC) [
11,
12,
13]. WFC is “a form of inter role conflict in which the general demands, time devoted to and strain created by the job interfere with performing family-related responsibilities,” and FWC is “a form of inter role conflict in which the general demands, time devoted to and strain created by the family interfere with performing work-related responsibilities”. WFC and FWC have been found to be positively related to depressive symptoms in previous studies [
10,
14]. For nurses, the previous study shows that WFC had a significant connection to psychological health [
15]. In Japan, the study shows that WFC had an impact on the physical and mental health of nurses [
16].
In China, most families are dual-career couples. Compared with other occupational populations, nurses devote a great deal of time and energy to work and experience a higher level of WFC in China [
17]. Although the association between WFC and depressive symptoms has been tested in other occupational populations [
10,
18,
19], the association between WFC and depressive symptoms among Chinese female nurses is not clear. We will discuss whether WFC is the risk factor of depressive symptoms, and if controlling this risk factor can reduce nurses’ depressive symptoms. Thus, we have included WFC and FWC in our study and hypothesize that both WFC and FWC have associations with depressive symptoms among Chinese nurses.
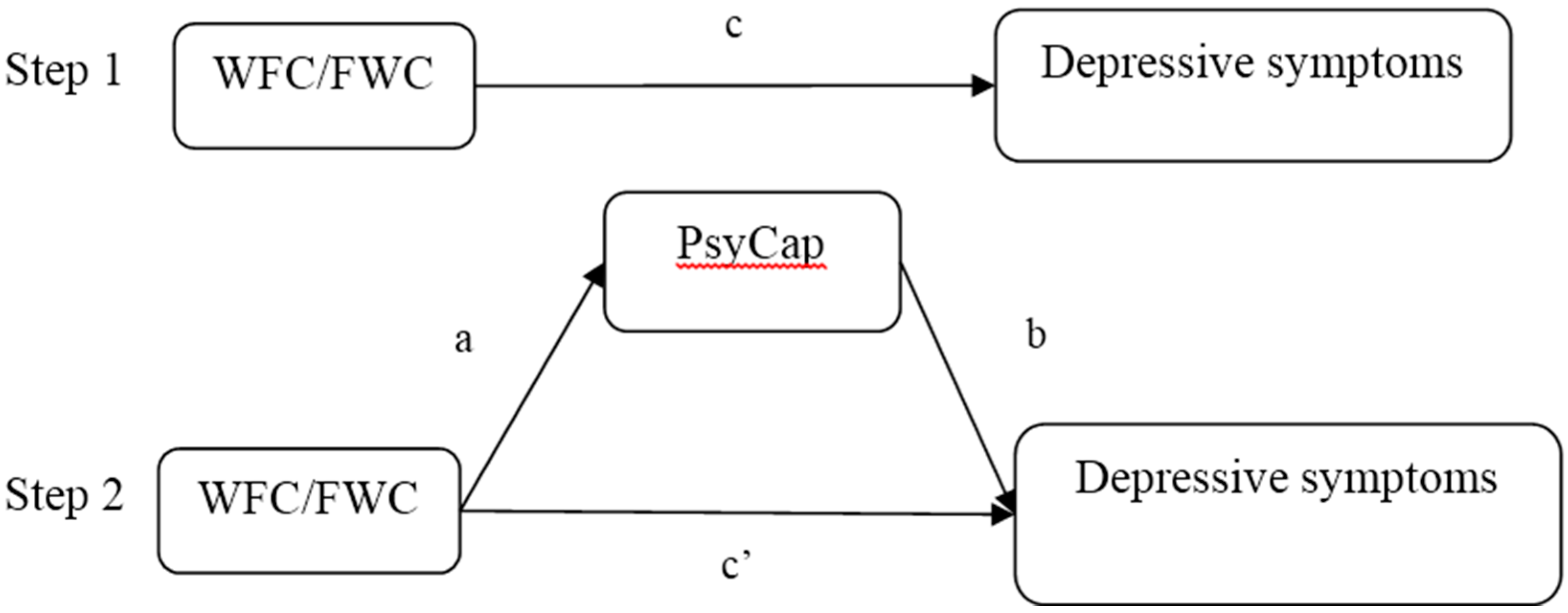
It is widely acknowledged that positive organizational behavior can improve workers’ physical and mental health by strengthening the psychological resource of workers. Psychological capital (PsyCap) has been found as a positive resource for relieving depressive symptoms [
20]. PsyCap is “a positive state of mind exhibited during the growth and development of an individual” and it includes the four core components of self-efficacy, optimism, resiliency, and hope [
21,
22]. In addition, research suggests that PsyCap reduces job burnout, depressive symptoms, occupational stress and other negative conditions. For example, PsyCap was identified as a mediator in the association between job burnout and turnover intention among Chinese nurses [
23]. A previous study shows that PsyCap partially mediated the association between occupational stress and depressive symptoms for female physicians [
20]. Another study found that PsyCap was a mediator in the relationship between WFC and burnout among Chinese nurses [
24]. Meanwhile, another study also found that PsyCap was a moderator in the association between emotional labor, burnout, and job satisfaction [
25]. Although both the relationship between PsyCap and depressive symptoms and the relationship between WFC and depressive symptoms have been investigated in previous studies [
12,
26], no sufficient studies demonstrated that PsyCap worked as a mediator or moderator in the association between WFC and depressive symptoms for Chinese female nurses.
Each of the four components of PsyCap has different characteristics. Self-efficacy is the ability to believe that one can take on challenge tasks and complete them; optimism is an explanatory style about positive self-attribution; hope is a positive motivational state about progressing from paths to goals at any time; and resiliency is a self-regulatory state that allows one to bounce back from difficult positions and adversity [
22]. The study shows that the four components of PsyCap were negatively related with WFC [
27], and another study shows that the four components of PsyCap were negatively associated with depressive symptoms [
28]. In addition, a previous study found that resilience and optimism partially mediated the relationship between perceived organizational support and depressive symptoms in frontline correctional officers [
28]. Meanwhile, another study shows that self-efficacy was a moderator in the relationship between WFC and job stress [
29]. Thus, we hypothesize that the four components of PsyCap work as a mediator or moderator in the relationship between WFC and depressive symptoms for Chinese female nurses.
The present study has two aims. First, we will test the relationship between WFC and depressive symptoms among Chinese nurses. Second, we will examine the mediating and moderating role of PsyCap and the dimensions of PsyCap in the association between WFC and depressive symptoms.
4. Discussion
In this study, subjects were selected from hospitals in Shenyang, China. A large number of samples and a high effective response rate show a good representation of our study population, and they could enhance the universalization of the conclusion in our study. Regarding the association between work-family conflict and depressive symptoms, in the present study, WFC and FWC were found to be positively related to depressive symptoms. Similar results can be found in previous studies [
10,
11,
12,
40]. One of the explanations is that work-related factors, poor relationships in the work environment, and work insecurity had a significant relationship with symptoms of depression [
41]. Another explanation is that high levels of FWC destroy one’s ability to perform effectively at work and one’s work-related self-image may be undermined, which in turn may cause psychological distress [
42]. Hospital administrators should be aware of the risk of work-family conflict demonstrated by these findings. It can be concluded that WFC has the potential to affect the quality of work. Some interventions should be made to decrease nurses’ WFC and FWC and to reduce nurses’ depressive symptoms. As an example, a better working environment and teamwork should be encouraged by measures of organizational development in hospitals [
11,
12,
24]. In addition, nurses’ working hours are long and provide little flexibility, thus, hospital administrators could adjust nurses’ working hours to reduce the level of work-family conflict. Meanwhile, hospital administrators should increase the number of staff and give nurses more chances to improve their technical skills to better accommodate a high-tech environment and to decrease the level of work-family conflict.
As an identified positive resource, PsyCap can decrease job stress and burnout in the workplace [
43,
44] and help counteract depressive symptoms in employees [
45]. In this study, PsyCap was found to be negatively related to depressive symptoms among Chinese female nurses. This finding shows that PsyCap had an effect on depressive symptoms and was a positive resource for fighting against depressive symptoms among this demographic. To our knowledge, PsyCap was identified as a mediator or moderator in some relationships [
20,
23,
24]. This study is the first one to explore the mediation and moderation of PsyCap and its dimensions in the association between work family conflict and depressive symptoms in China.
For female nurses, our study demonstrated that PsyCap partially mediated in the association between FWC and depressive symptoms. This suggests that FWC can be harmful to PsyCap, and reduce the level of nurses’ PsyCap, so as to lead to nurses’ depressive symptoms. Regarding the PsyCap components, hope and optimism partially mediated the effects of FWC on depressive symptoms. This result suggests that FWC can be harmful to hope and optimism, and may also lead to nurses’ depressive symptoms. Self-efficacy doesn’t mediate the effects of FWC on depressive symptoms. Nurses may work rigorous and taxing schedules and they may still not satisfy work demands and expectations. Therefore, the effect of self-efficacy does not work in mediating these relationships. On the other hand, it could be that low levels of FWC arise from daily events that may be more easily controlled by highly efficacious individuals. However, high levels of FWC may arise from more serious events that are less controllable or are perceived as less controllable [
46,
47]. Lastly, people who are high in self-efficacy may become disappointed by trying to control things that simply cannot be controlled.
As a product of psychological capacities, PsyCap has an impact on depressive symptoms and its mediation on the association between FWC and depressive symptoms was greater than the effects of PsyCap components among nurses. This result is in accordance with a previous study that indicated the synergistic role of PsyCap components [
45]. Thus, it is necessary to focus and invest more resources in significant components than non-significant components, and achieve maximum positive outcomes.
In addition, in this study, PsyCap had a positive moderation in the association between WFC and depressive symptoms. For the nurses with a high level of PsyCap, depressive symptoms will be increased with the increase of WFC. However, for the nurses with the low level of PsyCap, with the increase of WFC, depressive symptoms will not be obviously increased. This suggests that hospital managers should improve nurses’ levels of PsyCap, which plays a positive role, while some measures should be taken to reduce the level of WFC or the positive effects of PsyCap will be subject to a certain degree of damage. Among the PsyCap components, self-efficacy and hope had positively moderating effects in the association between WFC and depressive symptoms. The results show that the self-efficacy and hope of PsyCap play a major role in this relationship. This suggests that hospital managers should control the investment in self-efficacy and hope of PsyCap while reducing the level of WFC.
Compared to reducing nurses’ work-family conflict, it is a more effective and feasible strategy for general hospitals to develop resources increasing the PsyCap of nurses. Some interventions should be taken to develop the PsyCap in China. People should specifically pay more attention to improving hope and optimism in the PsyCap investment. For hope improvement, some appropriate and challenging job goals should be set for nurses to help them strengthen their willpower. Meanwhile, managers should help nurses create multiple pathways to reach their goals. For improving optimism, managers should encourage nurses to treat past failures and setbacks as valuable experiences, build a positive attribution style, and improve their capacity to discover and pursue different opportunities [
48,
49,
50].
5. Conclusions
To summarize, our findings revealed that work-family conflict is a risk factor that can increase nurses’ depressive symptoms, and PsyCap is a positive resource to combat nurses’ depressive symptoms. PsyCap as a moderator can aggravate the effects of WFC on depressive symptoms. Meanwhile, when PsyCap is a mediator, FWC impacts PsyCap to increase nurses’ depressive symptoms.
Several limitations of this study must be considered. First, this study is not a longitudinal study. Work-family conflict, PsyCap and depressive symptoms were measured simultaneously, so we cannot arrive at causal conclusions. Secondly, in this study, the target population we set is large hospital nurses, and this does not cover all groups of nurses, like nurses who work at small hospitals or community service centers. Next, we will study the nurses of these institutions. Third, this study was only concerned with the association between work-family conflict and depressive symptoms and controlled only for some basic social demographics. More risk factors and possible confounders should be investigated in further studies.



{kind=link}