
Evaluation of Quality of Life of Those Living near a Wind Farm


Abstract
:1. Introduction
2. Materials and Method
2.1. Selection of the Area and Number of Respondents for the Study
Participants

{kind=link}
| Variables | n = 1277 | ||
|---|---|---|---|
| Gender | Women | n (%) | 703 (55.05) |
| Men | n (%) | 574 (44.95) | |
| Age (for whole group) | n | 1277 | |
| M ± SD | 45.54 ± 16.10 | ||
| Me | 45.5 | ||
| Min, Max | 18–90 | ||
| Age | Women | n | 703 (55.05) |
| M ± SD | 46.2 ± 16.10 | ||
| Me | 46 | ||
| Min, Max | 18–94 | ||
| Men | n | 574 (44.95) | |
| M ± SD | 44.7 ± 16.00 | ||
| Me | 45 | ||
| Min, Max | 18–85 | ||
| Education | Primary | n (%) | 332 (26.00) |
| Vocational | n (%) | 440 (31.30) | |
| Secondary | n (%) | 397 (31.09) | |
| Higher | n (%) | 139 (10.90) | |
| No data | n (%) | 9 (0.70) | |
| Place of residence | Villages | n (%) | 1277 (100.00) |
| Professional activity | Employed | n (%) | 659 (51.60) |
| Disability pension—Retirement pension | n (%) | 189 (14.80) | |
| Unemployed | n (%) | 335 (26.23) | |
| Student | n (%) | 80 (6.26) | |
| No data | n (%) | 14 (1.09) | |
2.2. Survey-Based Study
| Abbreviation | Domain | Domain Description |
|---|---|---|
| PF | Physical Functioning | Limitations in physical activities because of health problems |
| RP | Role Physical | Limitations in usual role activities because of physical health problems |
| BP | Bodily Pain | Intensity of bodily pain or discomfort |
| GH | General Health | General health perceptions |
| VT | Vitality | Energy and fatigue |
| SF | Social Functioning | Limitations in social activities due to physical or emotional problems |
| RE | Role Emotional | Limitations in usual role activities because of emotional problems |
| MH | Mental Health | Psychological distress and well-being |
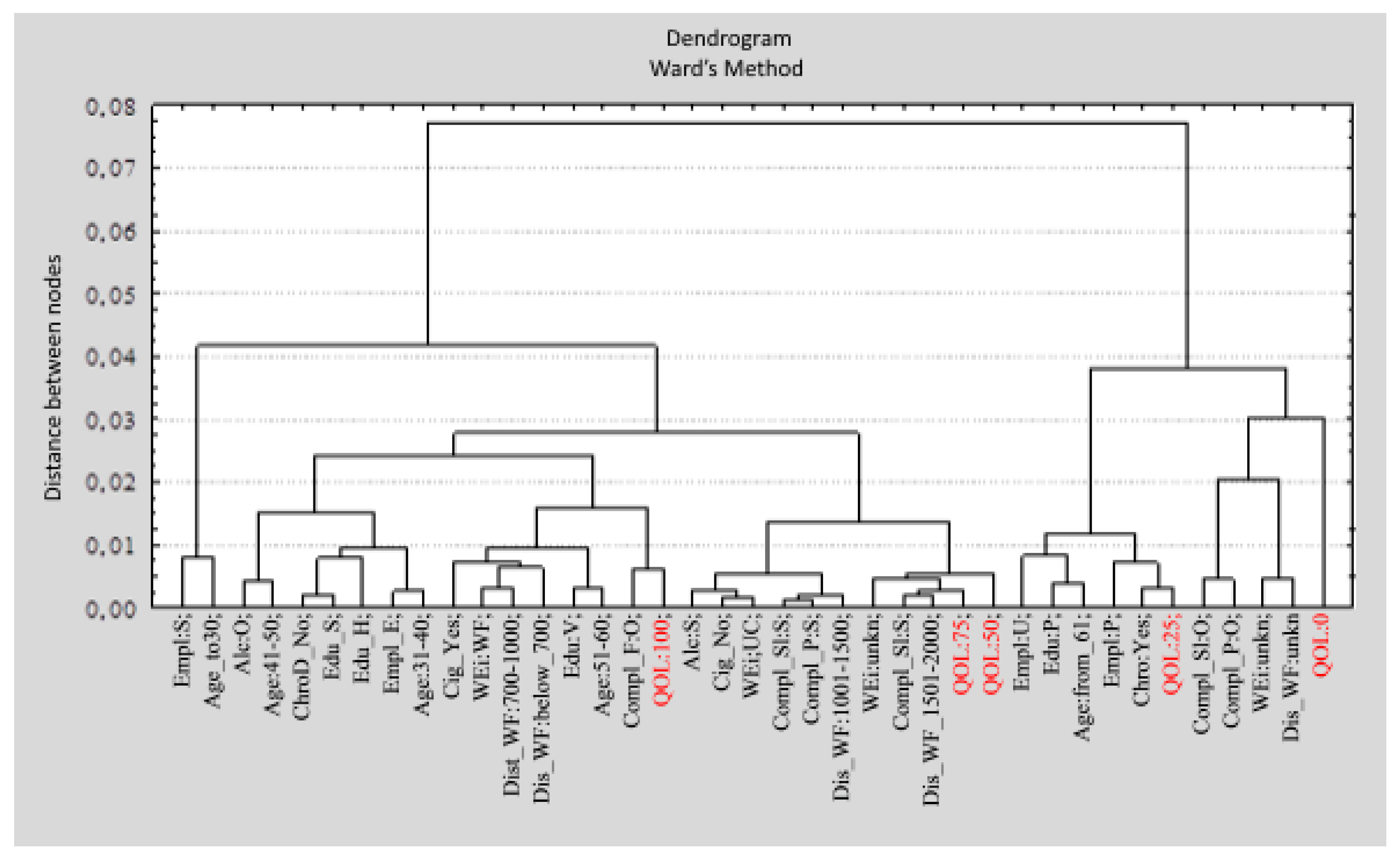
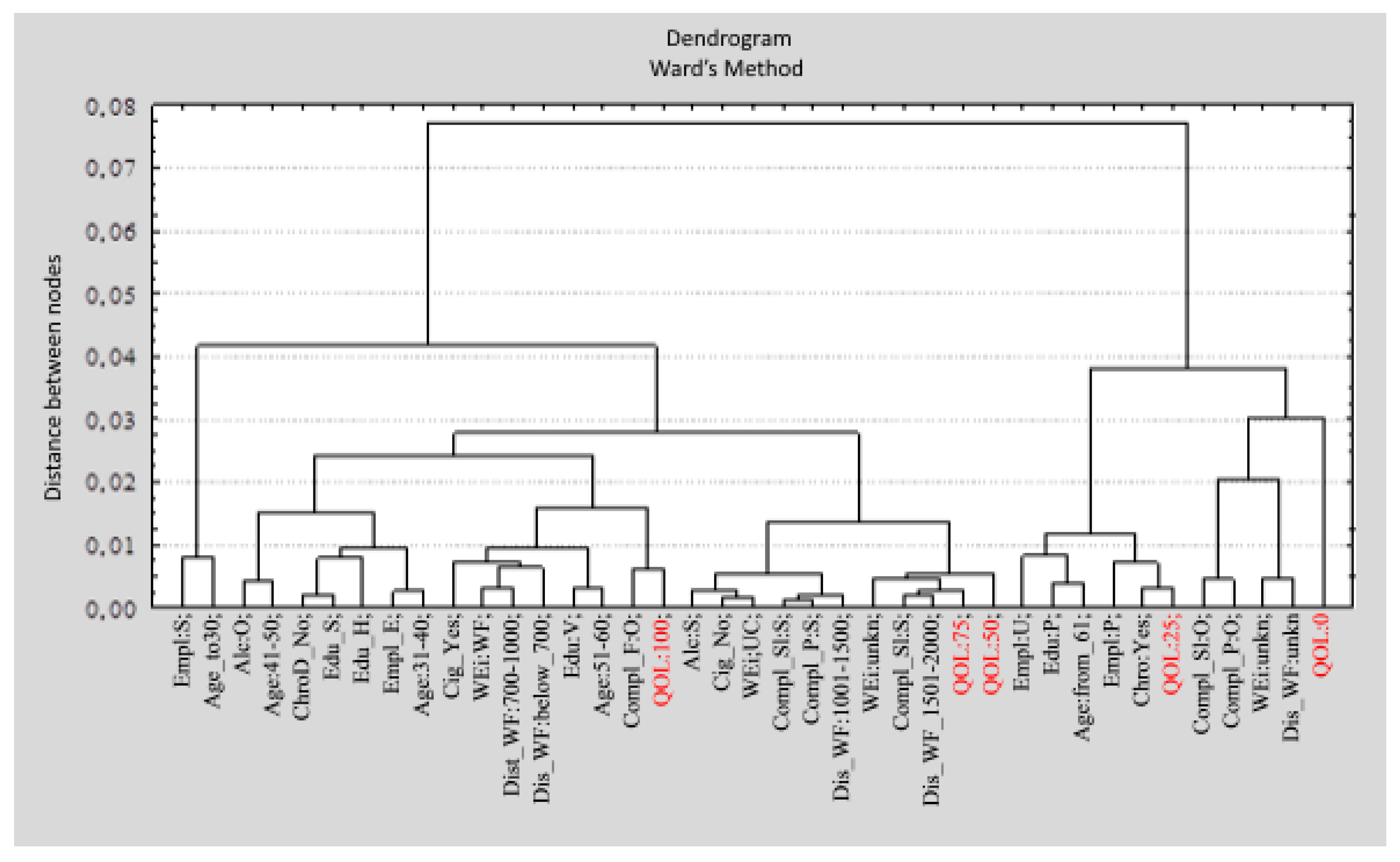
2.3. Statistical Analysis
- (1)
- QoL: quality of life (0; 25; 50; 75; 100).
- (2)
- Age (below 30; 31–40; 41–50; 51–60; over 61).
- (3)
- Gender (W: women; M: men).
- (4)
- Edu: education (P: primary; V: vocational; S: secondary; H: higher).
- (5)
- Empl: employment (E: employed; U: unemployed; S: student; P: pensioner).
- (6)
- Dist_WF: distance between residence and wind farms (below 700 m; up to 700 m; 701–1000 m; 1001–1500 m; 1501–2000 m; unkn: I do not know, but no more than 2 km),
- (7)
- WEi: wind farm status (UC: under construction; P: planned; WF: completed; unkn: I don’t know),
- (8)
- Alc: alcohol consumption (S: seldom or never; O: often),
- (9)
- Cig: smoking (DS: I don’t smoke; S: I smoke regularly),
- (10)
- Compl_P: frequency of headaches, stomach aches, or back pain during the last six months (S: seldom; O: often),
- (11)
- Compl_Ir: frequency of feeling depressed, irritated, angry, or nervous during the last three months (S: seldom; O: often),
- (12)
- Compl_Sl: frequency of having trouble falling asleep or being anxious during the last three months (S: seldom; O: often),
- (13)
- Compl_F: frequency of feeling very tired or exhausted during the last 3 months (S: seldom; O: often),
- (14)
- ChroD: being treated for chronic disease (Y: yes; N: no).
3. Results
3.1. Quality of Life of People Living in the Vicinity of Wind Farms
3.2. The Influence of Environmental Stress Factors on Assessment of Quality of Life
3.2.1. The Influence of Distance
| Variable | Anxiety | Irritation | Nervousness | Anger | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Level | Score | SD | the Wald Statistic | CI +95% | CI −95% | p | Score | SD | the Wald Statistic | CI +95% | CI −95% | p | Score | SD | the Wald Statistic | CI +95% | CI −95% | p | Score | SD | the Wald Statistic | CI +95% | CI −95% | p | |
| Stage of investment * | 1 | 0.47 | 0.11 | 16.74 | 0.24 | 0.69 | 0.000 | −0.07 | 0.11 | 0.52 | −0.28 | 0.13 | 0.70 | −0.52 | 0.10 | 24.67 | −0.73 | −0.31 | 0.000 | 0.62 | 0.11 | 32.15 | 0.40 | 0.83 | 0.000 |
| 2 | −0.25 | 0.11 | 5.59 | −0.46 | −0.04 | 0.018 | 0.04 | 0.10 | 0.14 | −0.16 | 0.24 | 0.710 | 0.31 | 0.10 | 9.57 | 0.15 | 0.51 | 0.002 | −0.40 | 0.10 | 15.82 | −0.60 | −0.20 | 0.000 | |
| 3 | −0.41 | 0.14 | 0.03 | −0.68 | −0.12 | 0.004 | 0.06 | 0.13 | 0.19 | −0.20 | 0.31 | 0.661 | 0.15 | 0.19 | 1.30 | −0.11 | 0.40 | 0.253 | −0.24 | 0.13 | 3.23 | −0.49 | 0.02 | 0.072 | |
| Distance from house to wind farms in meters ** | O1 | 0.70 | 0.20 | 12.16 | 0.31 | 1.10 | 0.000 | −0.12 | 0.16 | 0.52 | −0.44 | 0.20 | 0.470 | −0.22 | 0.16 | 1.82 | −0.55 | 0.10 | 0.178 | 0.36 | 0.16 | 4.63 | 0.03 | 0.68 | 0.031 |
| O2 | −0.08 | 0.14 | 0.33 | −0.34 | 0.19 | 0.564 | −0.11 | 0.13 | 0.70 | −0.36 | 0.14 | 0.403 | 0.09 | 0.13 | 0.56 | −0.16 | 0.35 | 0.455 | 0.03 | 0.13 | 0.04 | −0.23 | 0.28 | 0.840 | |
| O3 | −0.25 | 0.14 | 2.86 | −0.53 | 0.04 | 0.090 | 0.08 | 0.14 | 0.32 | −0.20 | 0.36 | 0.571 | 0.19 | 0.14 | 1.77 | −0.09 | 0.46 | 0.184 | −0.24 | 0.14 | 2.92 | −0.52 | 0.04 | 0.087 | |
| O4 | −0.07 | 0.11 | 0.38 | −0.30 | 0.15 | 0.539 | −0.03 | 0.11 | 0.08 | −0.25 | 0.18 | 0.769 | −0.06 | 0.11 | 0.26 | −0.27 | 0.17 | 0.606 | 0.02 | 0.11 | 0.05 | −0.19 | 0.24 | 0.828 | |
| SF-36 Scale * | X ± SD | CI −95% | CI +95% | N | W | p |
|---|---|---|---|---|---|---|
| Physical functioning | 76.12 ± 27.92 | 74.51 | 77.58 | 1277 | 0.098 | 0.0001 |
| Limitations in daily activities due to physical health (role physical) | 59.87 ± 39.26 | 57.67 | 61.98 | 1276 | ||
| Bodily pain | 63.70 ± 32.22 | 61.89 | 65.43 | 1277 | ||
| General health | 55.33 ± 24.04 | 53.96 | 56.61 | 1277 | ||
| Vitality | 58.23 ± 24.15 | 56.90 | 59.55 | 1277 | ||
| Social functioning | 58.75 ± 36.32 | 56.75 | 60.74 | 1277 | ||
| Role emotional | 62.73 ± 40.36 | 60.51 | 64.94 | 1276 | ||
| Mental health | 60.13 ± 23.06 | 58.87 | 61.40 | 1276 |
3.2.2. The Influence of the Stage of Development on Assessment of Quality of Life
3.2.3. Reactions to Learning of Wind-Farm Projects
3.3. Expectations of Benefits Associated with the Investment
3.4. Result of Correlations
| SF-36 Scale | Sociodemographic Data | Diseases | Risky Health Behavior | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| * Age | Professional Activity | Education | Arthritis | Hypertension | Heart Disease | Pulmonary Disease | Alcohol Dependency | Diabetes Mellitus | Other Diseases | Cancer | Smoking | Alcohol Consumption | ||
| PCS | β | −0.286 | 0.050 | 0.068 | −0.072 | −0.056 | 0.059 | −0.055 | 0.53 | −0.108 | ||||
| p | 0.001 | 0.04 | 0.01 | 0.01 | 0.05 | 0.05 | 0.02 | 0.02 | 0.001 | |||||
| MCS | β | −0.184 | 0.065 | |||||||||||
| p | 0.001 | 0.03 | ||||||||||||
| PF | β | −0.323 | −0.073 | 0.073 | 0.078 | |||||||||
| p | 0.001 | 0.01 | 0.01 | 0.01 | ||||||||||
| RP | β | −0.217 | −0.062 | −0.082 | −0.061 | |||||||||
| p | 0.001 | 0.03 | 0.01 | 0.02 | ||||||||||
| BP | β | −0.207 | 0.065 | −0.069 | 0.069 | |||||||||
| p | 0.001 | 0.02 | 0.01 | 0.032 | ||||||||||
| GH | β | −0.260 | −0.053 | −0.118 | −0.084 | −0.106 | ||||||||
| p | 0.001 | 0.02 | 0.001 | 0.001 | ||||||||||
| VT | β | −0.203 | −0.058 | 0.064 | −0.054 | −0.087 | ||||||||
| p | 0.001 | 0.03 | 0.019 | 0.03 | 0.001 | |||||||||
| SF | β | −0.168 | −0.131 | |||||||||||
| p | 0.001 | 0.001 | ||||||||||||
| RE | β | −0.175 | −0.064 | −0.090 | −0.072 | |||||||||
| p | 0.001 | 0.001 | 0.01 | 0.01 | ||||||||||
| MH | β | −0.079 | 0.065 | −0.058 | −0.075 | |||||||||
| p | 0.01 | 0.03 | 0.001 | |||||||||||
| SF-36 Scale | Health Problems | Stressors | ||||||||||||
| Headaches | Stomach aches | Backaches | Depression | Anxiety | Irritability | Fatigue | Exhaustion | Anger | Uneasiness | Insomnia | Distance of WF | Stage of Investment | ||
| PCS | β | −0.131 | −0.102 | −0.168 | −0.102 | 0.075 | 0.115 | |||||||
| p | 0.001 | 0.001 | 0.001 | 0.001 | 0.01 | 0.001 | ||||||||
| MCS | β | −0.175 | −0.209 | −0.098 | −0.059 | −0.108 | −0.109 | |||||||
| p | 0.001 | 0.001 | 0.01 | 0.046 | 0.001 | 0.001 | ||||||||
| PF | β | −0.122 | 0.094 | −0.097 | 0.062 | 0.015 | ||||||||
| p | 0.001 | 0.001 | 0.001 | 0.04 | 0.001 | |||||||||
| RP | β | 0.095 | −0.145 | −0.068 | −0.114 | 0.069 | 0.081 | 0.08 | −0.064 | |||||
| p | 0.001 | 0.001 | 0.03 | 0.001 | 0.04 | 0.01 | 0.02 | 0.02 | ||||||
| BP | β | −0.164 | 0.073 | −0.186 | −0.102 | 0.079 | ||||||||
| p | 0.001 | 0.001 | 0.001 | 0.001 | ||||||||||
| GH | β | −0.161 | −0.123 | −0.125 | −0.124 | −0.055 | −0.06 | −0.053 | ||||||
| p | 0.001 | 0.001 | 0.001 | 0.001 | 0.04 | 0.02 | 0.03 | |||||||
| VT | β | −0.200 | −0.202 | −0.109 | −0.104 | 0.061 | −0.062 | −0.069 | ||||||
| p | 0.001 | 0.001 | 0.001 | 0.001 | 0.04 | 0.04 | 0.01 | |||||||
| SF | β | −0.177 | −0.211 | 0.147 | ||||||||||
| p | 0.001 | 0.001 | 0.001 | |||||||||||
| RE | β | −0.099 | −0.107 | −0.146 | 0.107 | 0.064 | ||||||||
| p | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |||||||||
| MH | β | 0.217 | 0.227 | 0.078 | 0.101 | −0.125 | 0.065 | 0.088 | ||||||
| p | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | 0.01 | ||||||||
4. Discussion
5. Conclusions
- (1)
- Age is the strongest contributor to QoL levels in wind-farm areas. It is possible that QoL is simultaneously influenced by several factors, such as chronic diseases and other health problems, adverse socioeconomic factors, and environmental stress factors.
- (2)
- The lowest scores for overall QoL and general health are noted among residents of places where projects are in the planning or construction phase. In order to find ways to reduce environmental stress and its adverse effects on health, it is necessary to conduct research among the residents of places where a wind-farm project is either being planned or is under construction or has just been completed [2,34,43].
- (3)
- The presence of wind farms near residential areas has no negative influence on the QoL of residents. The highest QoL levels are noted in places where wind farms at various stages of development are located within one kilometer from the residence.
Author Contributions
Conflicts of Interest
References
- The Potential Health Impact of Wind Turbines. Chief Medical Officer of Health (CMOH) Report; Catalogue No. 014894. Available online: http://www.simcoemuskokahealth.org/Libraries/TOPIC_Environment/health_impacts_wind_turbines.sflb.ashx (accessed on 5 May 2015).
- Merlin, T.; Newton, S.; Ellery, B.; Milverton, J.; Farah, C. Systematic Review of the Human Health Effects of Wind Farms; National Health and Medical Research Council: Canberra, Australia, 2013. Available online: https://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/eh54_systematic_review_of_the_human_health_effects_of_wind_farms_december_2013.pdf (accessed on 5 May 2015).
- Nissenbaum, M.; Aramini, J.; Hanning, C. Adverse Health Effects of Industrial Wind Turbines: A Preliminary Report. In Proceedings of 10th International Congress on Noise as a Public Health Problem (ICBEN), London, UK, 24–28 July 2011.
- Knopper, L.D.; Ollson, C.A.; McCallum, L.C.; Whitfield Aslund, M.L.; Berger, R.G.; Souveine, K.; McDaniel, M. Wind turbines and human health. Front. Public Health 2014, 2, 1–20. Available online: http://dx.doi.org/10.3389/fpubh.2014.00063 (accessed on 11 May 2015). [Google Scholar]
- Van den Berg, F.; Pedersen, E.; Bouma, J.; Bakker, R. Visual and Acoustic Impact of Wind Farms on Residents; Final Report; FP6-2005-Science-and-Society-20 Specific Support Action: Project No. 044628; University of Groningen: Groningen, The Netherlands, 2008; Available online: http://docs.wind-watch.org/wfp-final-1.pdf (accessed on 5 May 2015).
- Moorhouse, A.; Hayes, M.; von Hünerbein, S.; Piper, B.; Adams, M. Research into Aerodynamic Modulation of Wind Turbine Noise: Final Report; University of Salford: Salford, UK, 2007; Available online: http://usir.salford.ac.uk/1554/ (accessed on 5 May 2015).
- Study of the Impact of Wind Turbines on Health: Report of the Panel of Independent Experts in January 2012; Developed for the Department of Environmental Protection of Massachusetts Department of Public Health of Massachusetts; Available online: http://www.wmae.pl/userfiles/file/Aktualnosci/wind_turbin.pdf (accessed on 10 September 2014).
- McCunney, R.J.; Mundt, K.A.; Colby, W.D.; Dobie, R.; Kaliski, K.; Blais, M. Wind turbines and health: A critical review of the scientific literature. J. Occup. Environ. Med. 2014, 56, 108–130. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, J.H.; Klokker, M. Health effects related to wind turbine noise exposure: A systematic review. PLoS One 2014, 9. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, E.; Larsman, P. The impact of visual factors on noise annoyance among people living in the vicinity of wind turbines. J. Environ. Psychol. 2008, 28, 379–389. [Google Scholar] [CrossRef]
- Pedersen, E. Health aspects associated with wind turbine noise. Results from three field studies. Noise Control Eng. J. 2011, 59, 47–53. [Google Scholar] [CrossRef]
- Pedersen, E.; van den Berg, F.; Bakker, R.; Bouma, J. Response to noise from modern wind farms in The Netherlands. J. Acoust. Soc. Am. 2009, 126, 634–643. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, E.; Persson Waye, K. Wind turbine noise, annoyance and self-reported health and well-being in different living environments. J. Occup. Environ. Med. 2007, 64, 480–486. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, D.; McBride, D.; Welch, D.; Dirks, K.N.; Hill, E. Evaluating the impact of wind turbine noise on health related quality of life. Noise Health 2011, 13, 333–339. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, E.; Hallberg, L.R.-M.; Waye, K.P. Living in the vicinity of wind turbines: A grounded theory study. Qual. Res. Psychol. 2007, 4, 49–63. [Google Scholar] [CrossRef]
- Fahey, T.; Whelan, C.; Maitre, B. First European Quality of Life Survey: Income Inequalites and Deprivation; Office for Official Publications of the European Communities: Luxembourg, 2005; Available online: http://www.eurofound.europa.eu/pubdocs/2005/93/en/1/ef0593en.pdf (accessed on 10 September 2014).
- Schipper, H. Quality of life: Principles of the clinical paradigm. J. Psychosoc. Oncol. 1990, 8, 171–185. [Google Scholar] [CrossRef]
- Mroczek, B.; Karakiewicz, B.; Brodowski, J.; Rotter, I.; Żułtak-Baczkowska, K. Subiective health assessment and health behaviour of adult inhabitants of towns located in the victinity of wind farms in Poland. Environ. Med. 2011, 13, 32–39. [Google Scholar]
- Tarasiuk, E.; Mroczek, B. Assessmentm of wind farms’ impact on human in the opinion of inhabitants of Wolin and neighboring towns. In Human and the Environment: Awareness and Social Acceptance; Mroczek, B., Ed.; Continuo: Wroclaw, Poland, 2011; pp. 57–66. [Google Scholar]
- Polish Wind Energy Association. Location of Wind Farms in Poland. Available online: http://www.psew.pl/pl/energetyka-wiatrowa/ewi-w-polsce (accessed on 18 October 2014).
- Ware, J.E.; Kosinski, M.; Bayliss, M.S.; McHorney, C.A.; Rogers, W.H.; Raczek, A. Comparison of methods for thescoring and statistical analysis of SF-36 health profile and summary measures: Summary of results from the medical outcomes study. Med. Care 1995, 33, 264–279. [Google Scholar]
- Ware, J.E.; Kosinski, M.; Turner-Bowker, D.M.; Gandek, B. How to Score Version 2 of the SF-12 Health Survey (with a Supplement Documenting Version 1); QualityMetric Incorporated: Lincoln, RI, USA, 2002. [Google Scholar]
- Guyatt, G.H.; Cook, D.J. Health status, quality of life, and the individual. J. Am. Med. Assoc. 1994, 272, 630–631. [Google Scholar] [CrossRef]
- Babor, T.F.; de la Fuente, R.J.; Saunders, J.; Grant, M. The Alkohol Use Disorders Indentyfication Test (AUDIT). Guidelines for Use in Primary Health Care; WHO: Geneva, Switzerland, 1989. [Google Scholar]
- Fagerström, K.O. Measuring degree of physical dependence to tobacco smoking with reference to individualization of treatment. Addict. Behav. 1978, 3, 235–241. [Google Scholar] [CrossRef]
- Banaś, J.; Machowska-Szewczyk, M.; Mroczek, B. Using the correspondence analysis to examine the impact of wind turbines on the quality of life. Res. Pap. Wroc. Univ. Econ. 2014, 328, 205–214. [Google Scholar]
- Ward, J.H. Hierarchical grouping to optimize an objective function. J. Am. Stat. Assoc. 1963, 58, 236–243. [Google Scholar] [CrossRef]
- Greenacre, M. Correspondence Analysis in Practice; Academic Press: London, UK, 1993. [Google Scholar]
- Veenhoven, R. World database of happiness. Soc. Indic. Res. 1995, 34, 299–313. [Google Scholar] [CrossRef]
- Schiller, J.S.; Lucas, J.W.; Ward, B.W.; Peregoy, J.A. Summary Health Statistics for U.S. Adults: National Health Interview Survey’ 2010; Vital Health Statistics: Hyattsville, MD, USA, 2012. Available online: http://www.cdc.gov/nchs/data/series/sr_10/sr10_252.pdf (accessed on 18 October 2014).
- Finkenauer, C.; Rimé, B. Keeping emotional memories secret; Health and subjective well-being when emotions are not shared. J. Health Psychol. 1998, 3, 47–58. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, D.; Welch, D.; Dirks, K.N.; Mathews, R. Exploring the relationship between noise sensitivity, annonyance and health-related quality of life in sample of adults exposed to environmental noise. Int. J. Environ. Res. Public Health 2010, 7, 3579–3594. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, R.S. Emotion and Adaptation; Oxford University Press: New York, NY, USA, 1991. [Google Scholar]
- Petrie, K.J.; Faasse, K.; Crichton, F.; Grey, A. How common are symptoms? Evidence from a New Zealand national telephone survey. Epidemiology 2014, 4. [Google Scholar] [CrossRef] [PubMed]
- Chapman, S.; Joshi, K.; Fry, L. Fomenting sickness: Nocebo priming of residents about expected wind turbine health harms. Front. Public Health 2014, 2. [Google Scholar] [CrossRef] [PubMed]
- Laszlo, H.E.; McRobie, E.S.; Stansfeld, S.A.; Hansell, A.L. Annoyance and other reaction measures to changes in noise exposure—A review. Sci. Total Environ. 2011, 1, 435–436. [Google Scholar] [CrossRef] [PubMed]
- Bakker, R.H.; Pedersen, E.; van den Berg, G.P.; Steward, R.E.; Lok, W.; Bouma, J. Impact of wind turbine sound on annoyance, self-reported sleep disturbance and psychological distress. Sci. Total Environ. 2012, 425. [Google Scholar] [CrossRef] [PubMed]
- Lombard, A.; Ferreira, S. Residents’ attitudes to proposed wind farms in the West Coast region of South Africa: A social perspective from the South. Energy Policy 2014, 66, 390–399. [Google Scholar] [CrossRef]
- Pedersen, E.; Persson Waye, K. Wind turbines—Low level noise sources interfering with restoration? Environ. Res. Lett. 2008, 3. [Google Scholar] [CrossRef]
- Johanson, M.; Laike, T. Intention to respond to local wind turbines: The role of attitudes and visual perception. Wind Energy 2007, 10, 435–451. [Google Scholar] [CrossRef]
- Ajzen, I. The Theory of planned behavior. Organ. Behave. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Colby, D.W.; Dobie, R.; Leventhall, G.; Lipscomb, D.M.; McCunney, R.; Seilo, M.T.; Sondergaard, B. Wind Turbine Sound and Health Effects: An Expert Panel Review; American Wind Energy Association and the Canadian Wind Energy Association: Washington, DC, USA, 2009. [Google Scholar]
- Summary of Findings from the Wind Turbine Noise and Health Study. Environmental and Workplace Health. 2014. Available online: http://www.hc-sc.gc.ca/ewh-semt/noise-bruit/turbine-eoliennes/summary-resume-eng.ph (accessed on 18 October 2014).
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mroczek, B.; Banaś, J.; Machowska-Szewczyk, M.; Kurpas, D. Evaluation of Quality of Life of Those Living near a Wind Farm. Int. J. Environ. Res. Public Health 2015, 12, 6066-6083. https://doi.org/10.3390/ijerph120606066
Mroczek B, Banaś J, Machowska-Szewczyk M, Kurpas D. Evaluation of Quality of Life of Those Living near a Wind Farm. International Journal of Environmental Research and Public Health. 2015; 12(6):6066-6083. https://doi.org/10.3390/ijerph120606066
Chicago/Turabian StyleMroczek, Bożena, Joanna Banaś, Małgorzata Machowska-Szewczyk, and Donata Kurpas. 2015. "Evaluation of Quality of Life of Those Living near a Wind Farm" International Journal of Environmental Research and Public Health 12, no. 6: 6066-6083. https://doi.org/10.3390/ijerph120606066
APA StyleMroczek, B., Banaś, J., Machowska-Szewczyk, M., & Kurpas, D. (2015). Evaluation of Quality of Life of Those Living near a Wind Farm. International Journal of Environmental Research and Public Health, 12(6), 6066-6083. https://doi.org/10.3390/ijerph120606066