
Assessment of Electromagnetic Interference with Active Cardiovascular Implantable Electronic Devices (CIEDs) Caused by the Qi A13 Design Wireless Charging Board

Abstract
:1. Introduction
2. Methods
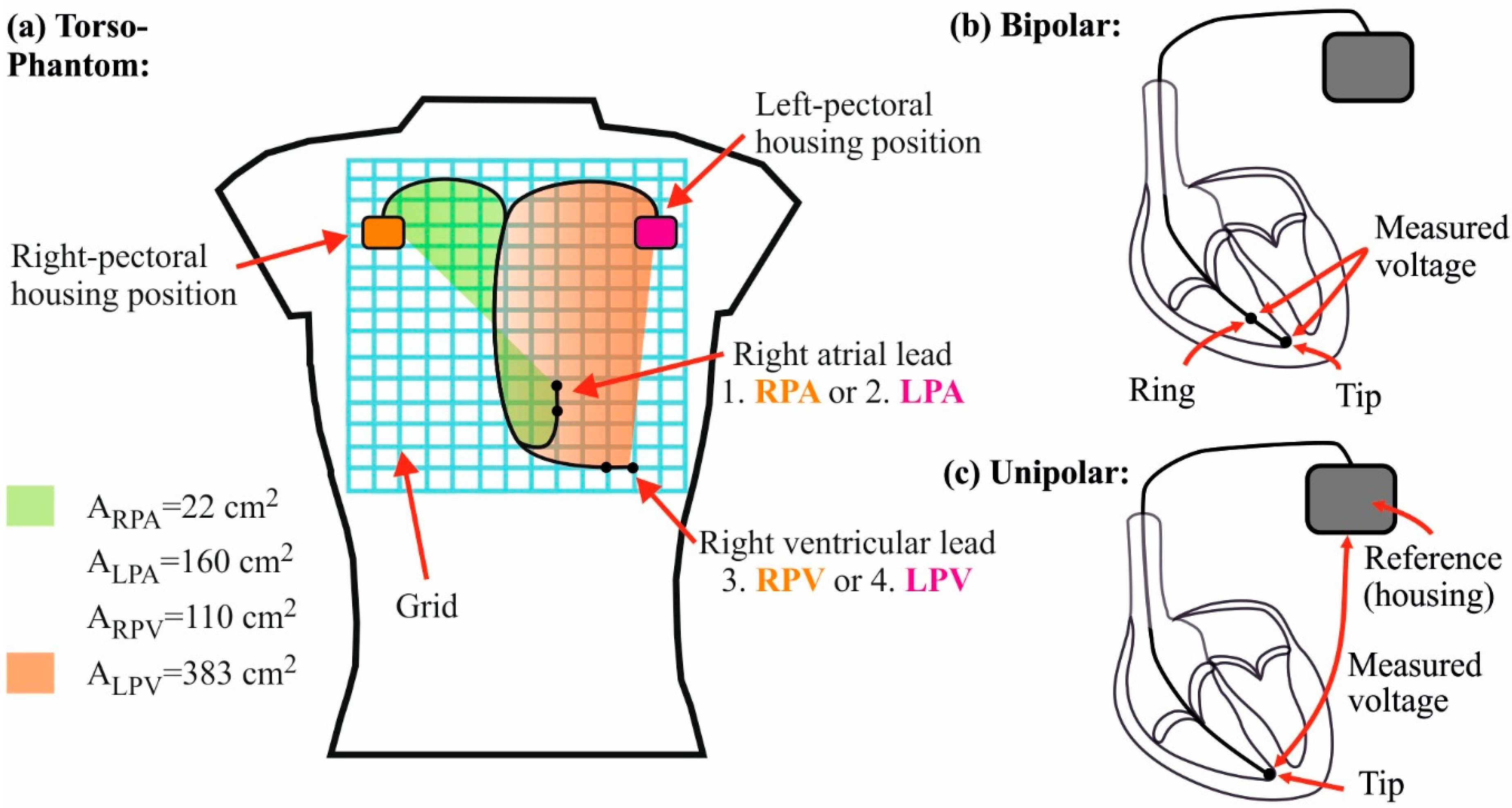
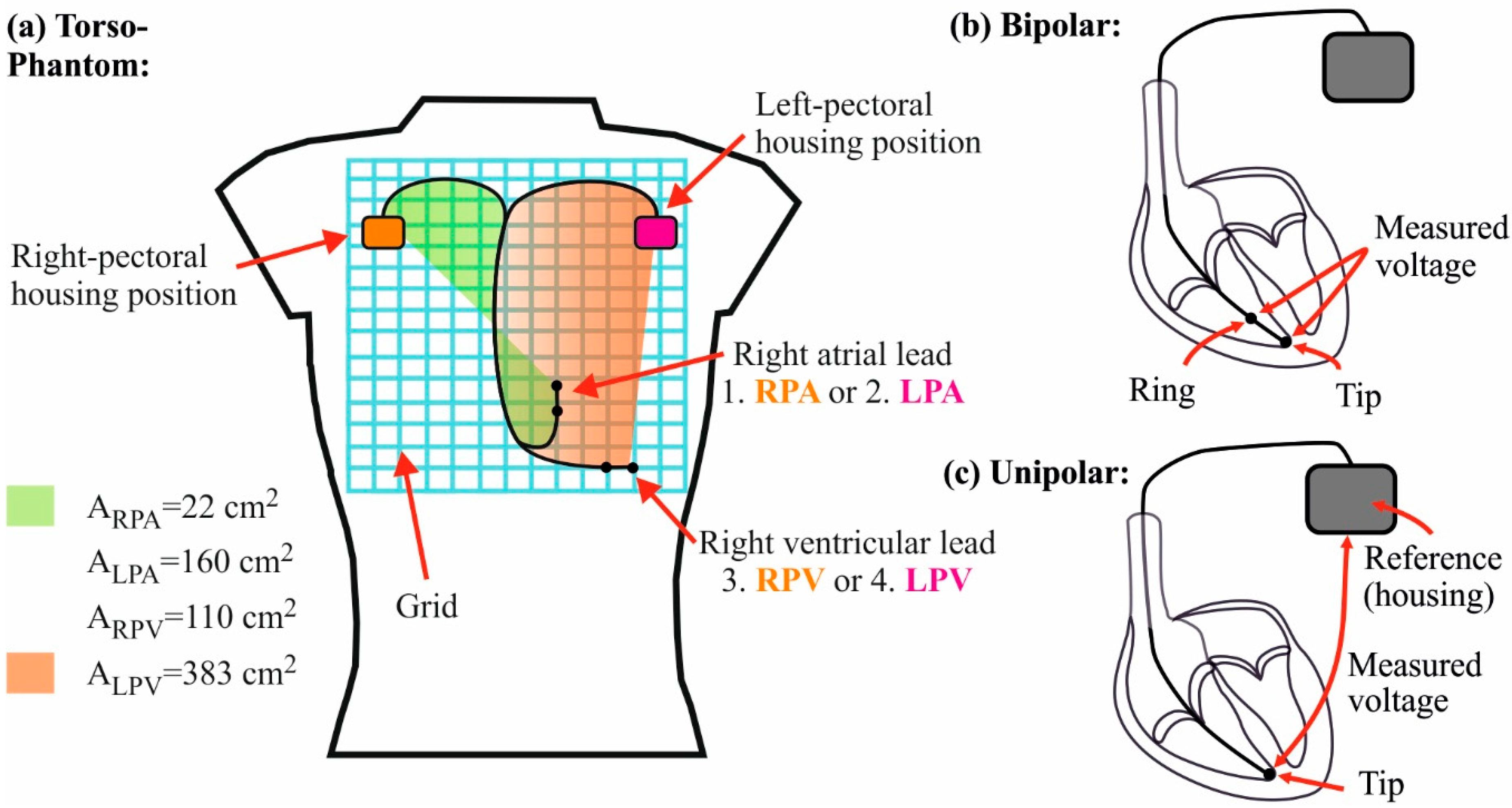
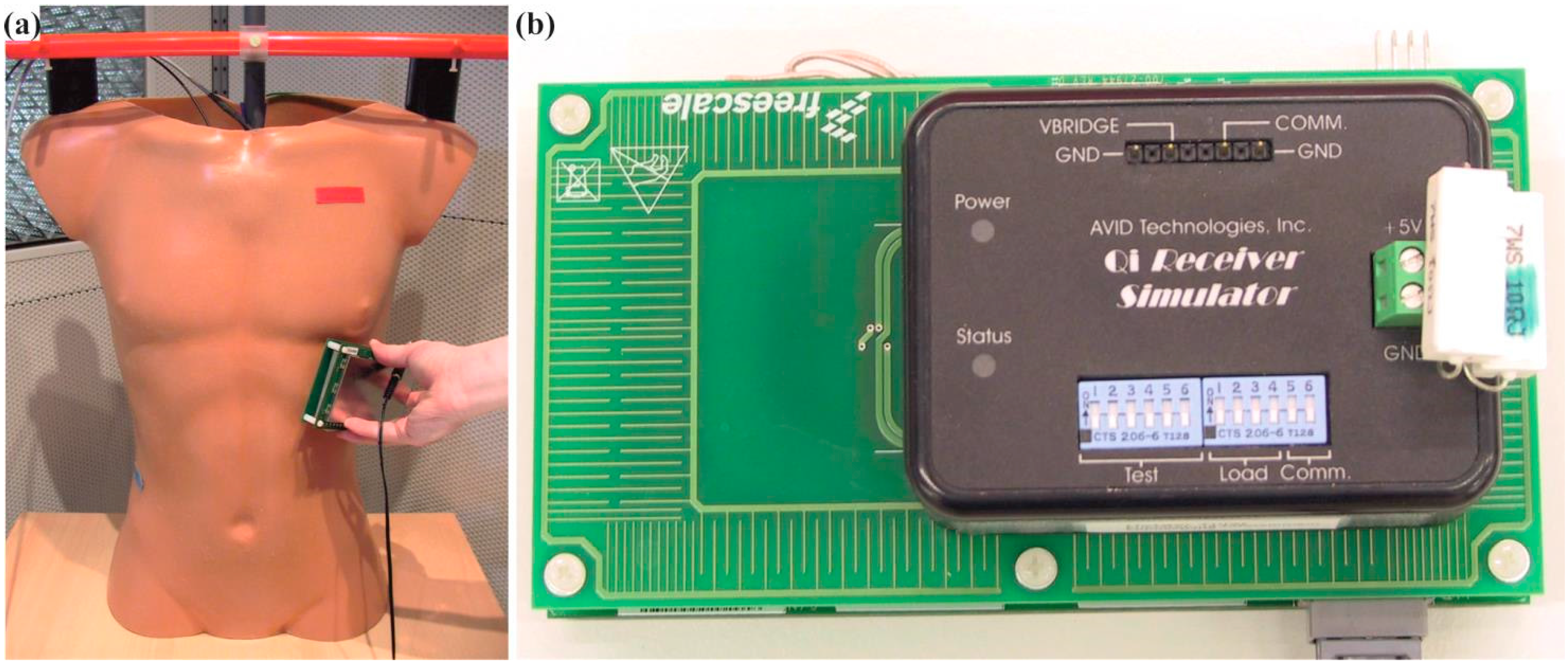
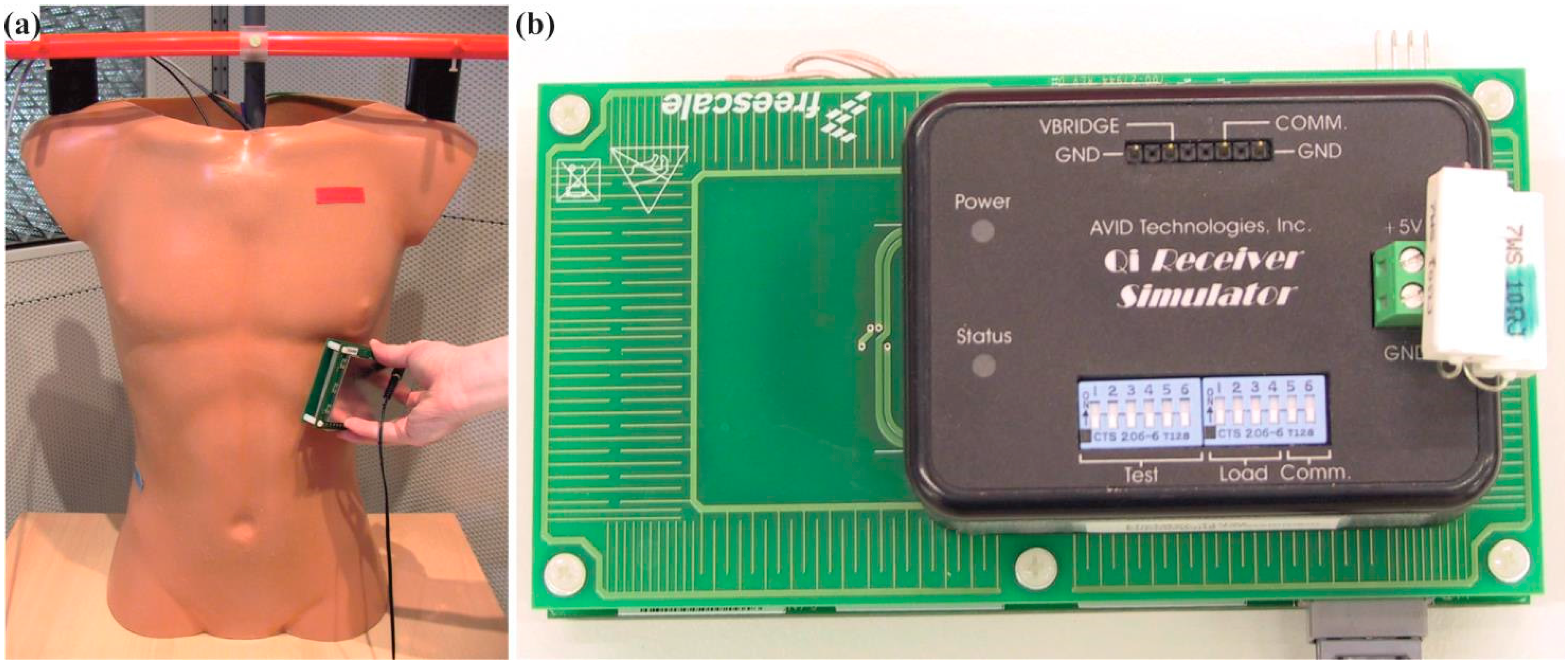
2.1. Torso Phantom and Measuring System
2.2. Homogenous Field Exposure by Using Helmholtz Coils
2.3. Inhomogeneous Field Exposure by Using the Qi-A13-Board
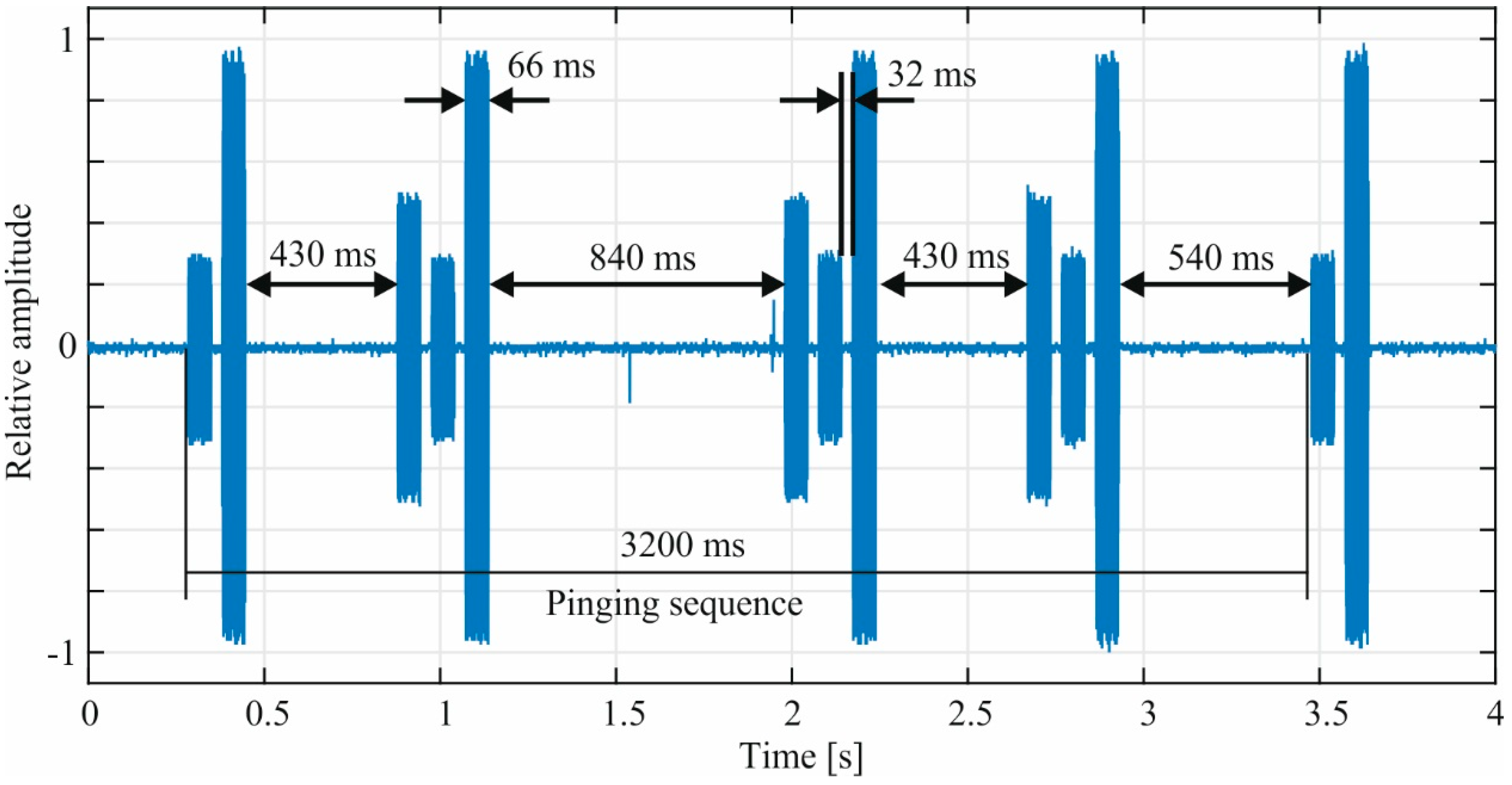
2.4. Signal Analysis
3. Results
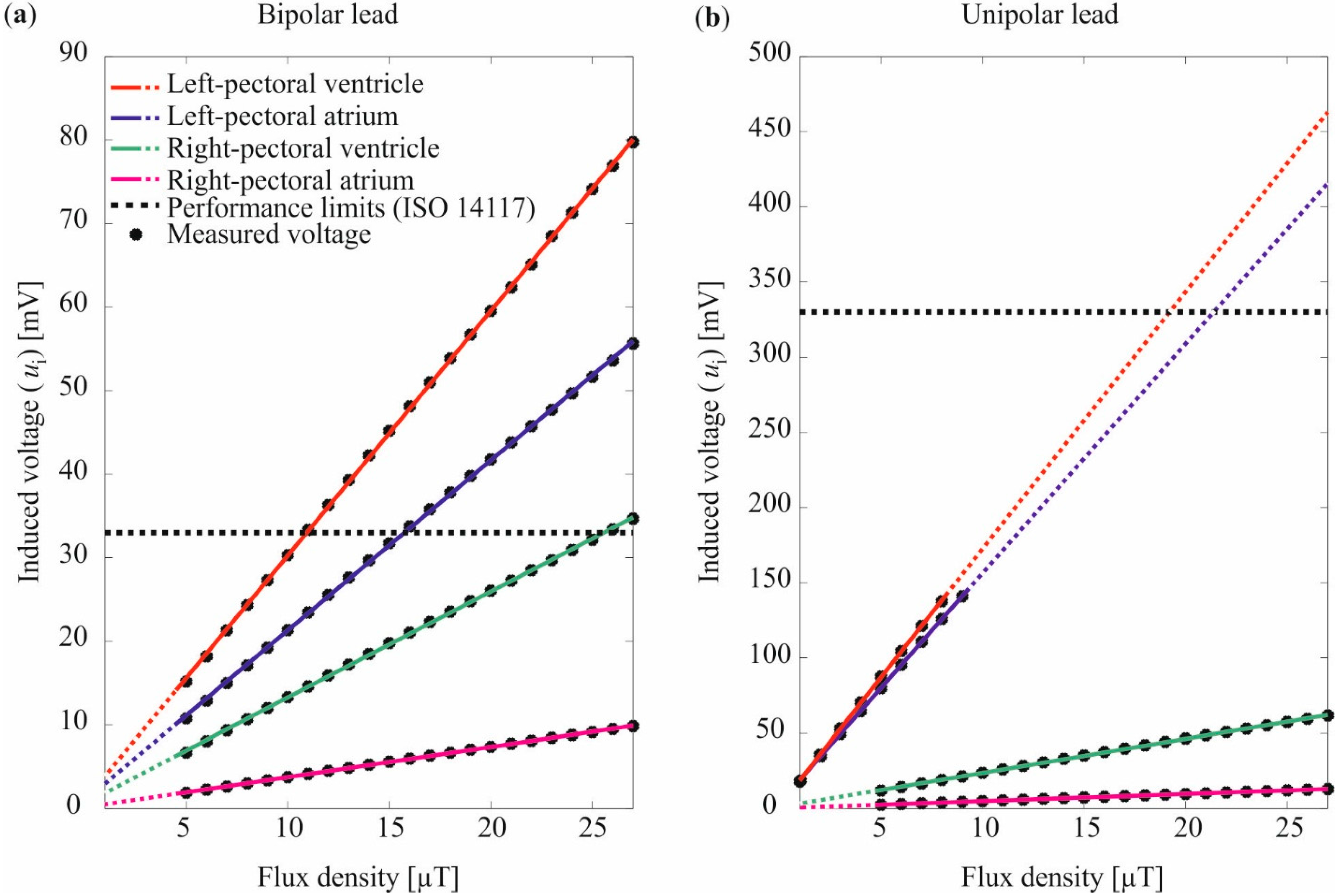
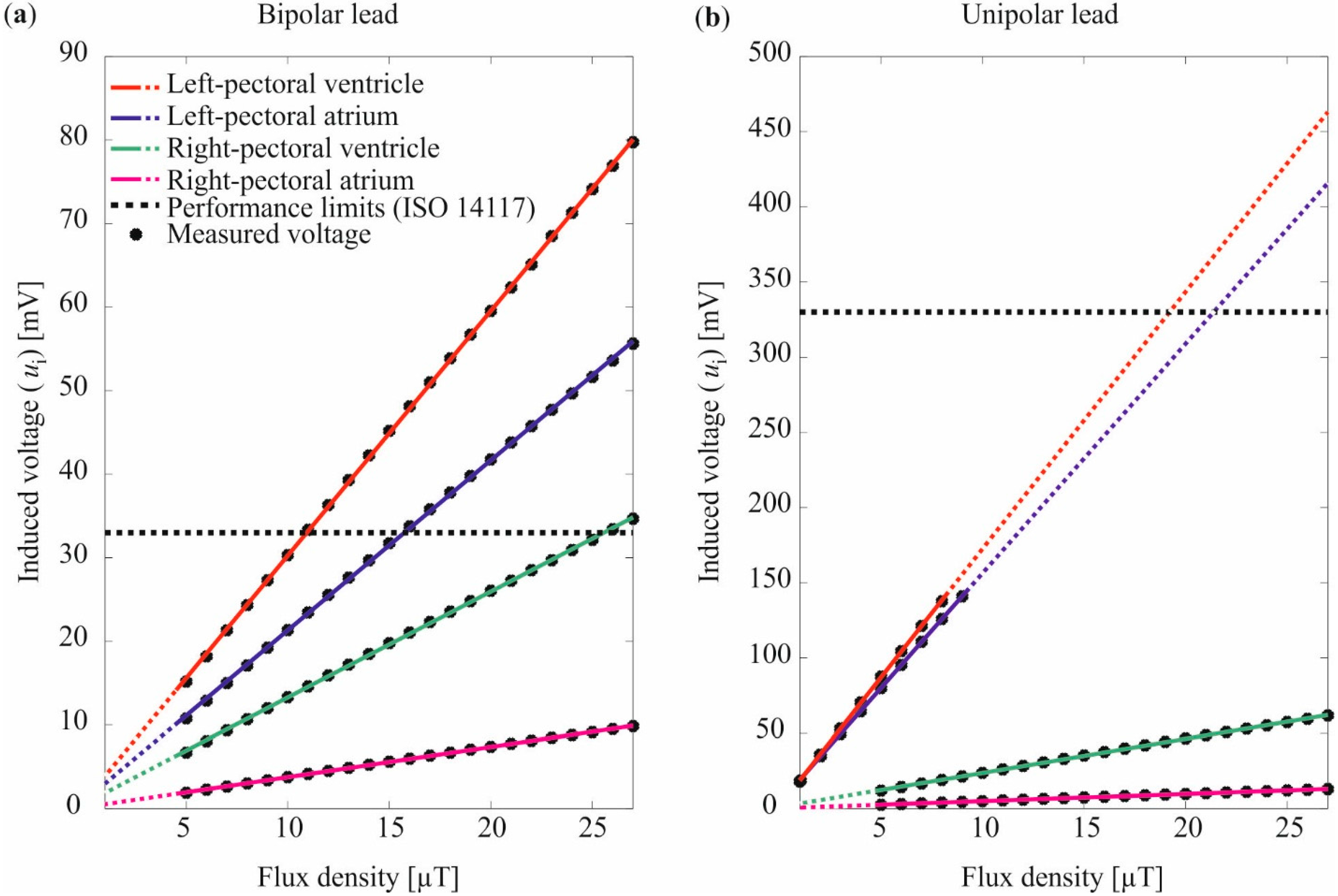
3.1. Homogenous Field Exposure by Using Helmholtz Coils

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Lead Unipolar/Bipolar | Housing Position | Lead Position | (V/mV) Equation (6) | (mV) Equation (6) | of the Linear Fit |
|---|---|---|---|---|---|
| Bipolar | Left-pectoral | Ventricle | 2.93 | 0.96 | 0.9999 |
| Atrium | 2.04 | 0.95 | 0.9998 | ||
| Right-pectoral | Ventricle | 1.27 | 0.60 | 0.9998 | |
| Atrium | 0.36 | 0.15 | 0.9998 | ||
| Unipolar | Left-pectoral | Ventricle | 17.09 | 1.68 | 0.9999 |
| Atrium | 15.55 | 1.68 | 0.9999 | ||
| Right-pectoral | Ventricle | 2.26 | 1.09 | 0.9997 | |
| Atrium | 0.48 | 0.20 | 0.9998 |
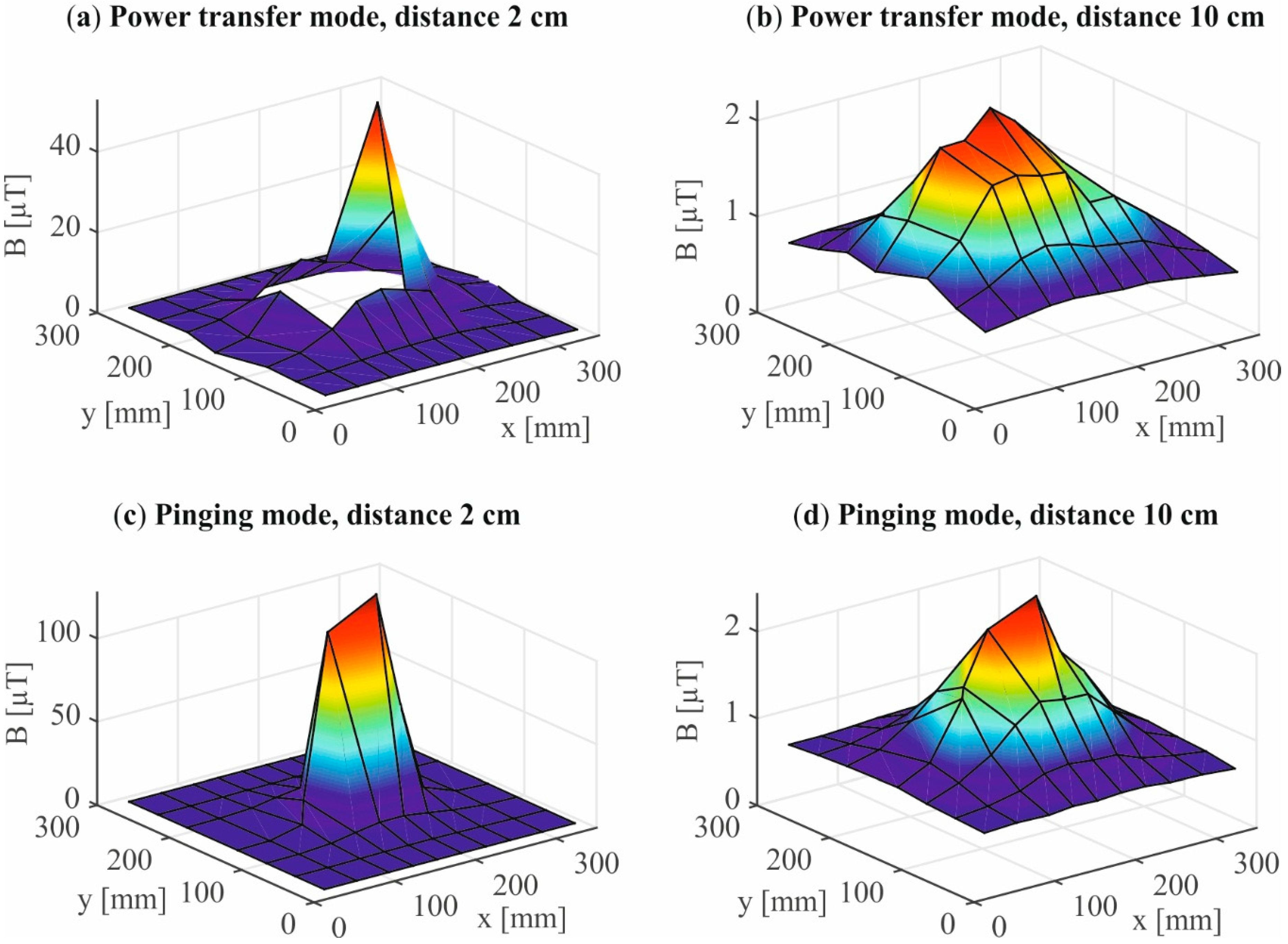
3.2. Inhomogeneous Field Distribution by Using Qi-A13-Board

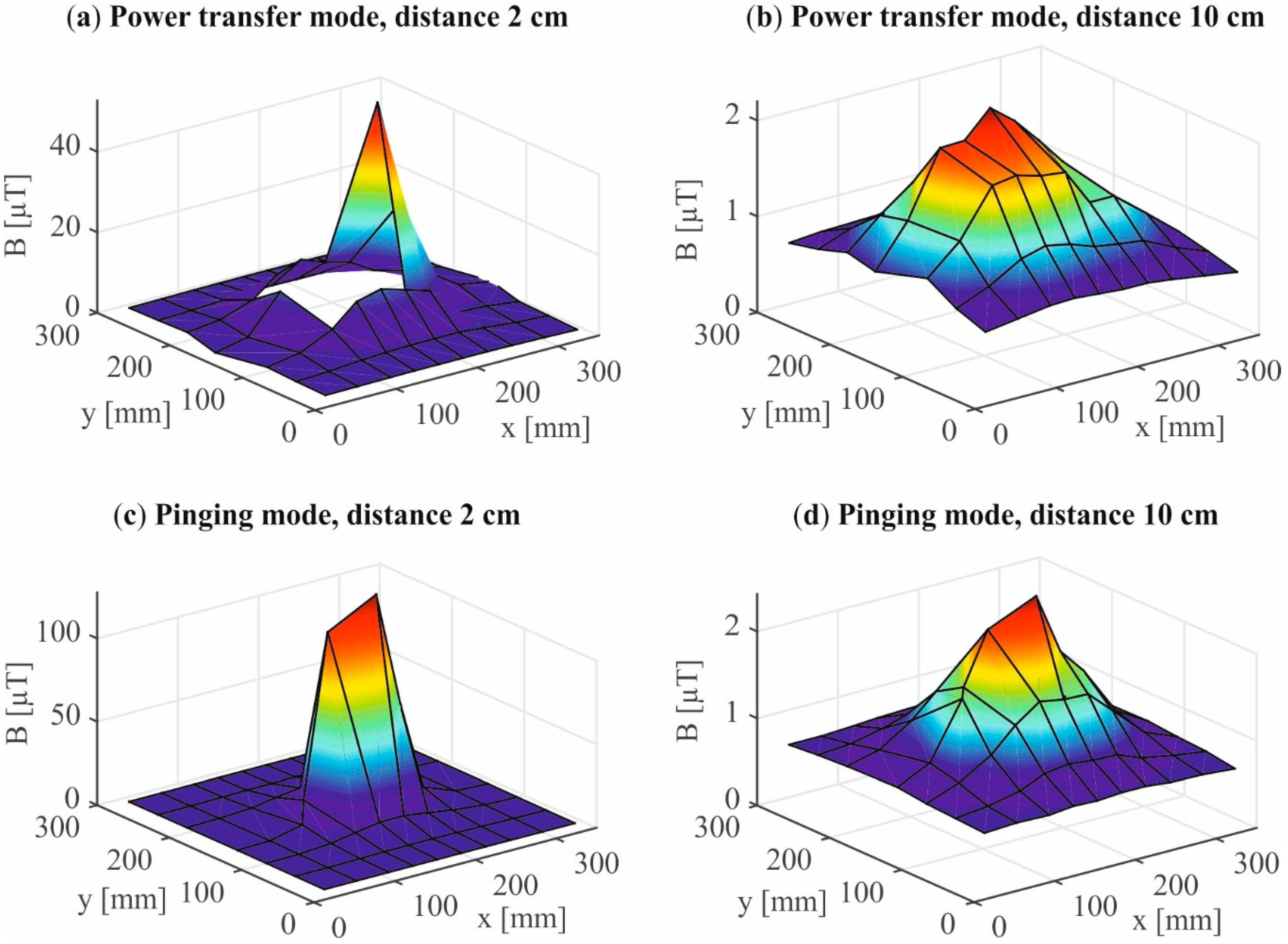
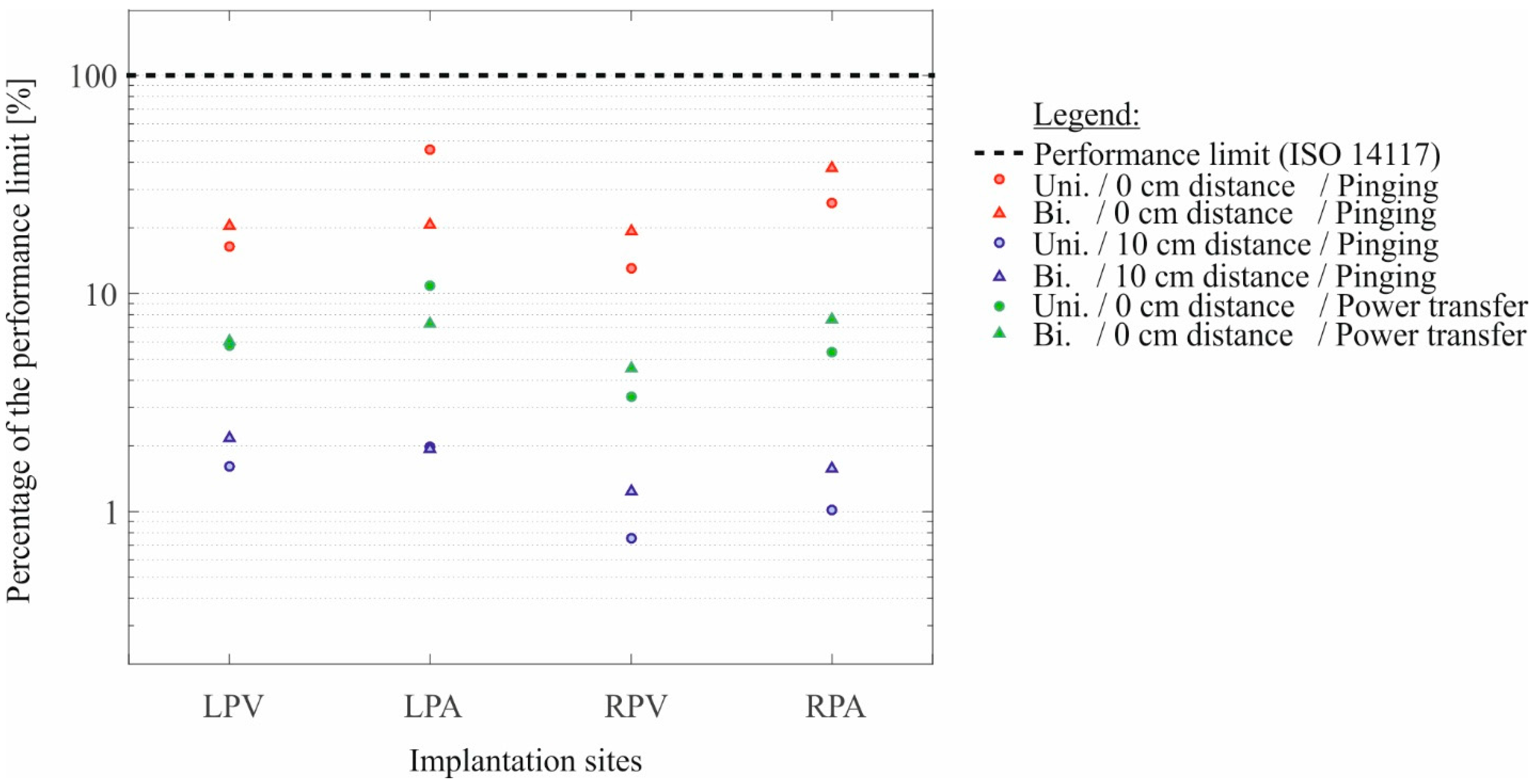
3.3. Inhomogeneous Field Exposure by Using the Qi-A13-Board in Power Transfer Mode
| Lead Type | Housing Position | Lead Position | (mV) | Percentage of the Performance Limit (%) | Relative STD (%) | Equation (5) |
|---|---|---|---|---|---|---|
| Bipolar | Left-pectoral | Ventricle | 2.0 | 6.0 | 2.3 | 0.9994 |
| Atrium | 2.4 | 7.2 | 1.3 | 0.9997 | ||
| Right-pectoral | Ventricle | 1.5 | 4.5 | 1.3 | 0.9992 | |
| Atrium | 2.5 | 7.5 | 1.4 | 0.9997 | ||
| Unipolar | Left-pectoral | Ventricle | 19.1 | 5.7 | 0.1 | >0.9999 |
| Atrium | 35.9 | 10.8 | 0.1 | >0.9999 | ||
| Right-pectoral | Ventricle | 11.1 | 3.3 | 0.1 | 0.9999 | |
| Atrium | 17.8 | 5.3 | 0.3 | 0.9998 |
3.4. Inhomogeneous Field Exposure by Using the Qi-A13-Board in Pinging Mode
| Lead Type/Setup | Housing Position | Lead Position | (mV) | Percentage of the Performance Limit (%) | Relative STD (%) | Equation (5) |
|---|---|---|---|---|---|---|
| Bipolar/0 cm distance | Left-pectoral | Ventricle | 6.72 | 20.4 | 0.2 | 0.9999 |
| Atrium | 6.84 | 20.7 | 2.8 | 0.9999 | ||
| Right-pectoral | Ventricle | 6.37 | 19.3 | 0.2 | 0.9999 | |
| Atrium | 12.40 | 37.6 | 0.1 | 0.9999 | ||
| Bipolar/10 cm distance | Left-pectoral | Ventricle | 0.72 | 2.2 | 2.0 | 0.9970 |
| Atrium | 0.64 | 1.9 | 2.2 | 0.9952 | ||
| Right-pectoral | Ventricle | 0.41 | 1.2 | 3.5 | 0.9873 | |
| Atrium | 0.52 | 1.6 | 2.7 | 0.9925 | ||
| Unipolar/0 cm distance | Left-pectoral | Ventricle | 54.12 | 16.4 | 0.1 | >0.9999 |
| Atrium | 150.72 | 45.7 | 0.1 | >0.9999 | ||
| Right-pectoral | Ventricle | 42.94 | 13.0 | 0.2 | >0.9999 | |
| Atrium | 85.38 | 25.9 | 0.1 | >0.9999 | ||
| Unipolar/10 cm distance | Left-pectoral | Ventricle | 5.31 | 1.6 | 0.3 | 0.9999 |
| Atrium | 6.56 | 2.0 | 0.3 | 0.9999 | ||
| Right-pectoral | Ventricle | 2.49 | 0.8 | 0.6 | 0.9996 | |
| Atrium | 3.37 | 1.0 | 0.5 | 0.9998 |
4. Discussion and Conclusions
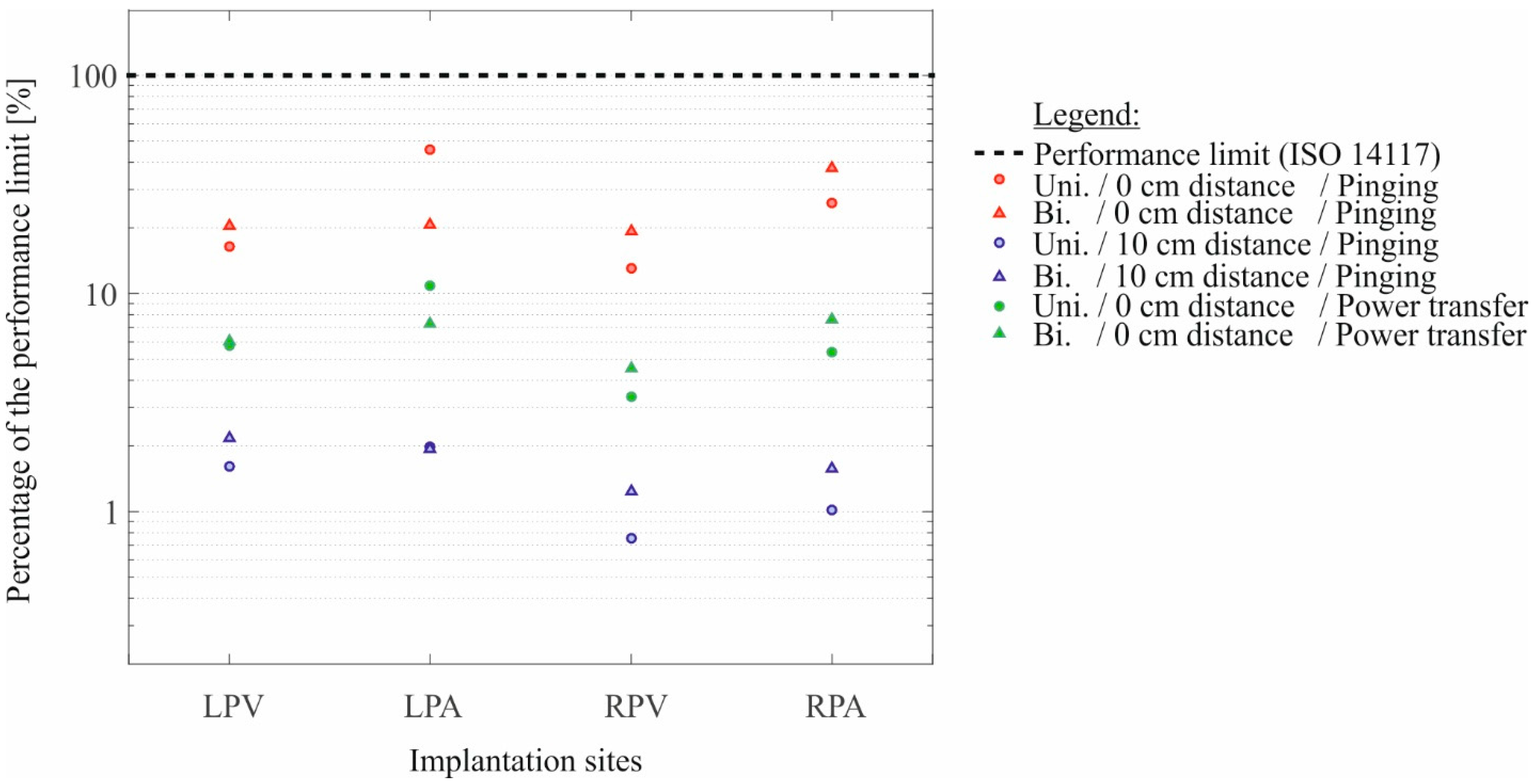
4.1. Risk Assessment of CIEDs When Exposed to Magnetic Fields at 111 kHz
4.2. Correlation between Induced Voltage and Strength of EMF
| Setup | LPV | LPA | RPV | RPA |
|---|---|---|---|---|
| Homogeneous exposure | 5.8 | 7.6 | 1.8 | 1.3 |
| Qi-A13-Board power transfer | 9.6 | 15.0 | 7.4 | 7.1 |
| Qi-A13-Board pinging (0 cm) | 8.1 | 22.0 | 6.7 | 6.9 |
Acknowledgments
Author Contributions
Conflicts of Interest
References
- WCT1001A/WCT1003A Automotive A13 Wireless Charging Application User’s Guide. 2015. Rev. 3.3. Available online: http://www.freescale.com/webapp/sps/site/prod_summary.jsp?code=RDWCT-5WTXAUTO&fpsp=1&tab=Documentation_Tab (accessed on 11 May 2015).
- System Description Wireless Power Transfer Volume I: Low Power Part 1: Interface Definition. 2013. Version 1.1.2. Available online: http://www.wirelesspowerconsortium.com/downloads/wireless-power-specification-part-1.html (accessed on 11 May 2015).
- Akhtar, M.; Bhat, T.; Tantray, M.; Lafferty, C.; Faisal, S.; Teli, S.; Bhat, H.; Raza, M.; Khalid, M.; Biekht, S. Electromagnetic interference with implantable cardioverter defibrillators causing inadvertent shock: Case report and review of current literature. Clin. Med. Insights Cardiol. 2014, 8, 63–66. [Google Scholar] [PubMed]
- Man, K.C.; Davidson, T.; Langberg, J.J.; Morady, F.; Kalbfleisch, S.J. Interference from a hand held radiofrequency remote control causing discharge of an implantable defibrillator. Pacing Clin. Electrophysiol. 1993, 16, 1756–1758. [Google Scholar] [CrossRef] [PubMed]
- McIvor, M.E.; Reddinger, J.; Floden, E.; Sheppard, R.C. Study of pacemaker and implantable cardioverter defibrillator triggering by electronic article surveillance devices (SPICED TEAS). Pacing Clin. Electrophysiol. 1998, 21, 1847–1861. [Google Scholar] [CrossRef] [PubMed]
- Seidman, S.J.; Brockman, R.; Lewis, B.M.; Guag, J.; Shein, M.J.; Clement, W.J.; Kippola, J.; Digby, D.; Barber, C.; Huntwork, D. In vitro tests reveal sample radiofrequency identification readers inducing clinically significant electromagnetic interference to implantable pacemakers and implantable cardioverter-defibrillators. Heart Rhythm: Off. J. Heart Rhythm Soc. 2010, 7, 99–107. [Google Scholar] [CrossRef]
- Seidman, S.J.; Ruggera, P.S.; Brockman, R.G.; Lewis, B.; Shein, M.J. Electromagnetic compatibility of pacemakers and implantable cardiac defibrillators exposed to RFID readers. Int. J. Radio Freq. Identif. Technol. Appl. 2007, 1, 237–246. [Google Scholar]
- Vardas, P.; Auricchio, A.; Merino, J.L. The EHRA white book. 2011. Available online: http://www.escardio.org/communities/EHRA/publications/Pages/white-book-project.aspx (accessed on 11 May 2015).
- Auricchio, A.; Kuck, K.-H.; Hatala, R.; Arribas, F. The EHRA white book. 2012. Available online: http://www.escardio.org/communities/EHRA/publications/Pages/white-book-project.aspx (accessed on 11 May 2015).
- Auricchio, A.; Kuck, K.-H.; Hatala, R.; Arribas, F. The EHRA white book. 2013. Available online: http://www.escardio.org/communities/EHRA/publications/Pages/white-book-project.aspx (accessed on 11 May 2015).
- Kuck, K.-H.; Hindricks, G.; Padeletti, L.; Raatikainen, P.; Arnar, D.O. The EHRA white book. 2014. Available online: http://www.escardio.org/communities/EHRA/publications/Pages/white-book-project.aspx (accessed on 11 May 2015).
- Mond, H.G.; Proclemer, A. The 11th world survey of cardiac pacing and implantable cardioverter-defibrillators: Calendar year 2009—A World Society of Arrhythmia’s project. Pacing Clin. Electrophysiol. 2011, 34, 1013–1027. [Google Scholar] [CrossRef] [PubMed]
- International Commission on Non-Ionizing Radiation Protection (ICNIRP). Guidelines for limiting exposure to time-varying electric, magnetic, and electromagnetic fields (up to 300 GHz). Health Phys. 1998, 74, 494–522. [Google Scholar] [PubMed]
- International Commission on Non-Ionizing Radiation Protection (ICNIRP). Guidelines for limiting exposure to time-varying electric and magnetic fields (1 Hz to 100 kHz). Health Phys. 2010, 99, 818–836. [Google Scholar] [PubMed]
- International Committee on Electromagnetic Safety (ICES). IEEE standard for safety levels with respect to human exposure to electromagnetic fields, 0–3 kHz. IEEE Std. C95.6–2002 2002. [Google Scholar] [CrossRef]
- International Committee on Electromagnetic Safety (ICES). IEEE Standard for Safety Levels with Respect to Human Exposure to Radio Frequency Electromagnetic Fields, 3 kHz to 300 GHz. IEEE Std. C95.1–2005 (Rev. IEEE Std. C95.1–1991) 2006. [Google Scholar] [CrossRef]
- Christ, A.; Douglas, M.; Nadakuduti, J.; Kuster, N. Assessing Human Exposure to Electromagnetic Fields From Wireless Power Transmission Systems. Proc. IEEE 2013, 101, 1482–1493. [Google Scholar] [CrossRef]
- International Organization for Standardization (ISO). Active implantable medical devices—Electromagnetic compatibility—EMC test protocols for implantable cardiac pacemakers, implantable cardioverter defibrillators and cardiac resynchronization devices. Available online: http://www.iso.org/iso/catalogue_detail.htm?csnumber=54472 (accessed on 11 May 2015).
- Toivonen, L.; Valjus, J.; Hongisto, M.; Metso, R. The influence of elevated 50 Hz electric and magnetic fields on implanted cardiac pacemakers: The role of the lead configuration and programming of the sensitivity. Pacing Clin. Electrophysiol. 1991, 14, 2114–2122. [Google Scholar] [CrossRef] [PubMed]
- Irnich, W. Electronic security systems and active implantable medical devices. Pacing Clin. Electrophysiol. 2002, 25, 1235–1258. [Google Scholar] [CrossRef] [PubMed]
- International Electrotechnical Commission (IEC). Exposure to electric or magnetic fields in the low and intermediate frequency range—Methods for calculating the current density and internal electric field induced in the human body—Part 3–1: Exposure to electric fields—Analytical and 2D numerical models. Available online: https://webstore.iec.ch/publication/6607 (accessed on 11 May 2015).
- Mattei, E.; Censi, F.; Mancini, M.; Napolitano, A.; Genovese, E.; Cannata, V.; Burriesci, G.; Falsaperla, R.; Calcagnini, G. Currents Induced by Fast Movements Inside the MRI Room may Cause Inhibition in an Implanted Pacemaker. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Annual Conference, Chicago, IL, USA, 26–30 August 2014.
- Berufsgenossenschaft Energie Textil Elektro Medienerzeugnisse (BG ETEM). Unfallverhütungsvorschrift Elektromagnetische Felder; BGV B11–6.01; BG ETEM: Cologne, Germany, 2002. [Google Scholar]
- ICNIRP. High Frequency Fields—Revision of the guidelines on highfrequency up to 300 GHz. Available online: http://www.icnirp.org/en/activities/work-plan/details/work-plan-hf.html (accessed on 11 May 2015).
- Irnich, W. Interference in pacemakers. Pacing Clin. Electrophysiol. 1984, 7, 1021–1048. [Google Scholar] [CrossRef] [PubMed]
- Tiikkaja, M.; Aro, A.L.; Alanko, T.; Lindholm, H.; Sistonen, H.; Hartikainen, J.E.; Toivonen, L.; Juutilainen, J.; Hietanen, M. Electromagnetic interference with cardiac pacemakers and implantable cardioverter-defibrillators from low-frequency electromagnetic fields in vivo. Europace 2013, 15, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Tiikkaja, M.; Alanko, T.; Lindholm, H.; Hietanen, M.; Hartikainen, J.; Toivonen, L. Experimental study on malfunction of pacemakers due to exposure to different external magnetic fields. J. Interv. Card. Electrophysiol. 2012, 34, 19–27. [Google Scholar] [CrossRef] [PubMed]
- Tiikkaja, M.; Alanko, T.; Lindholm, H.; Hietanen, M.; Toivonen, L.; Hartikainen, J. Interference of low frequency magnetic fields with implantable cardioverter-defibrillators. Scand. Cardiovasc. J. 2012, 46, 308–314. [Google Scholar] [CrossRef] [PubMed]
- Futatsumori, S.; Kawamura, Y.; Hikage, T.; Nojima, T.; Koike, B.; Fujimoto, H.; Toyoshima, T. In vitro assessment of electromagnetic interference due to low-band RFID reader/writers on active implantable medical devices. J. Arrhythm. 2009, 25, 142–152. [Google Scholar] [CrossRef]
- Andretzko, J.P.; Hedjiedj, A.; Guendouz, L. A model for determining the induced voltage at the terminals of a pacemaker exposed to a low frequency magnetic field. Physiol. Meas. 2008, 29, 1121–1132. [Google Scholar] [CrossRef] [PubMed]
- Hille, S.; Eichhorn, K.F.; Gonschorek, H.K. Determination of the Interference Voltage in Implantable Medical Devices with Bipolar Electrodes. In Proceedings of the 2008 International Symposium on Electromagnetic Compatibility—EMC Europe, Hamburg, Germany, 8–12 September 2008.
- Hille, S.; Eichhorn, K.F.; Gonschorek, H.K. Interference Voltage and Interference Threshold in Pacemakers with Unipolar and Bipolar Electrodes. In Proceedings of the IEEE International Symposium on Electromagnetic Compatibility, 2009 (EMC 2009), Austin, TX, USA, 17–21 August 2009.
- Mattei, E.; Censi, F.; Delogu, A.; Ferrara, A.; Calcagnini, G. Setups for In vitro assessment of RFID interference on pacemakers. Phys. Med. Biol. 2013, 58, 5301–5316. [Google Scholar] [CrossRef] [PubMed]
- Babouri, A.; Hedjeidj, A.; Guendouz, L. Experimental and theoretical investigation of implantable cardiac pacemaker exposed to low frequency magnetic field. J. Clin. Monit. Comput. 2009, 23, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Dawson, T.W.; Caputa, K.; Stuchly, M.A.; Shepard, R.B.; Kavet, R.; Sastre, A. Pacemaker interference by magnetic fields at power line frequencies. IEEE Trans. Bio-Med. Eng. 2002, 49, 254–262. [Google Scholar] [CrossRef]
- Gustrau, F.; Bahr, A.; Goltz, S.; Eggert, S. Active medical implants and occupational safety—Measurement and numerical calculation of interference voltage. Biomed. Technik. Biomed. Eng. 2002, 47, 656–659. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seckler, T.; Jagielski, K.; Stunder, D. Assessment of Electromagnetic Interference with Active Cardiovascular Implantable Electronic Devices (CIEDs) Caused by the Qi A13 Design Wireless Charging Board. Int. J. Environ. Res. Public Health 2015, 12, 5886-5904. https://doi.org/10.3390/ijerph120605886
Seckler T, Jagielski K, Stunder D. Assessment of Electromagnetic Interference with Active Cardiovascular Implantable Electronic Devices (CIEDs) Caused by the Qi A13 Design Wireless Charging Board. International Journal of Environmental Research and Public Health. 2015; 12(6):5886-5904. https://doi.org/10.3390/ijerph120605886
Chicago/Turabian StyleSeckler, Tobias, Kai Jagielski, and Dominik Stunder. 2015. "Assessment of Electromagnetic Interference with Active Cardiovascular Implantable Electronic Devices (CIEDs) Caused by the Qi A13 Design Wireless Charging Board" International Journal of Environmental Research and Public Health 12, no. 6: 5886-5904. https://doi.org/10.3390/ijerph120605886
APA StyleSeckler, T., Jagielski, K., & Stunder, D. (2015). Assessment of Electromagnetic Interference with Active Cardiovascular Implantable Electronic Devices (CIEDs) Caused by the Qi A13 Design Wireless Charging Board. International Journal of Environmental Research and Public Health, 12(6), 5886-5904. https://doi.org/10.3390/ijerph120605886