
Examining the Link Between Public Transit Use and Active Commuting

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
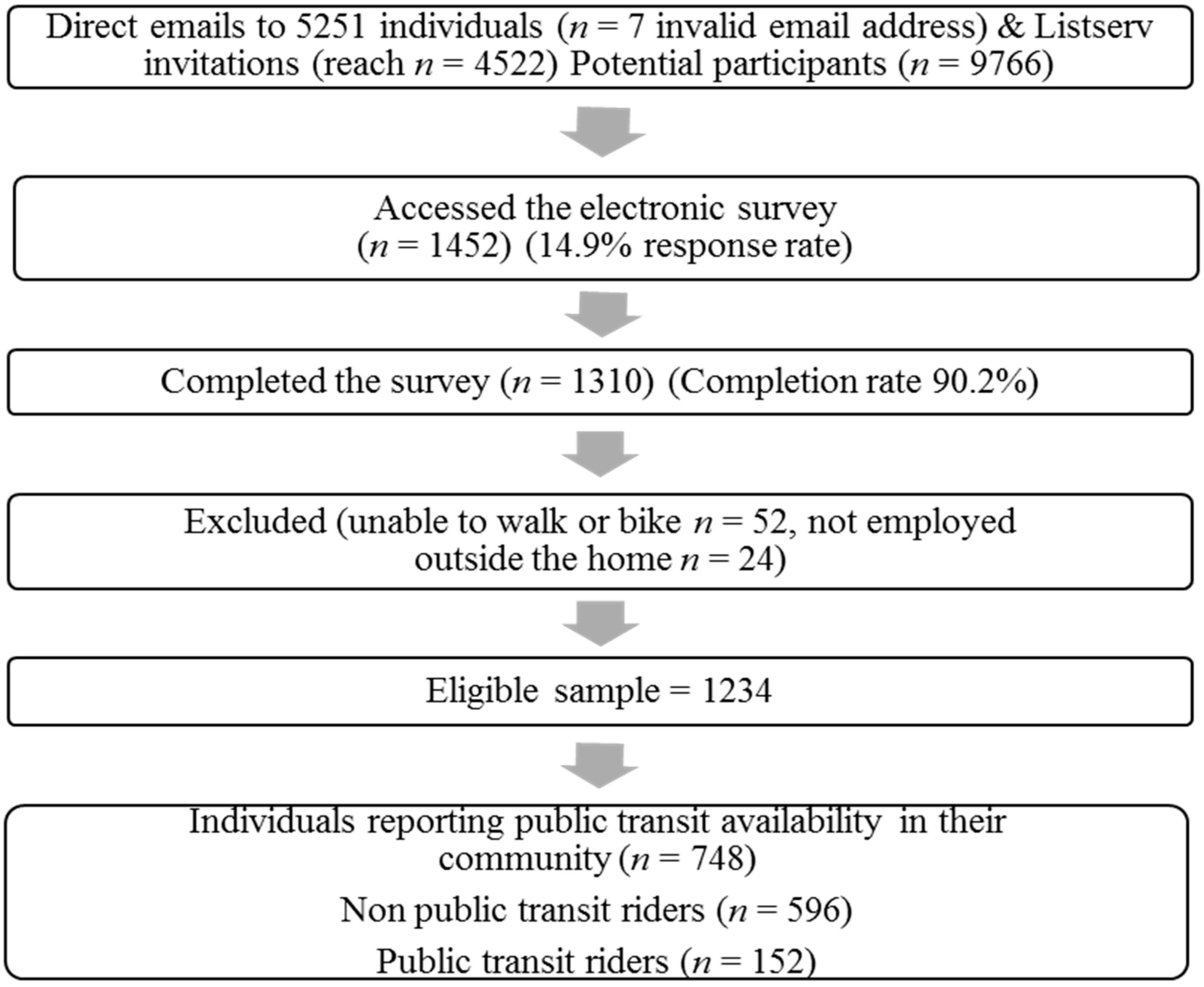
Participants and Recruitment
2.2. Measures
2.2.1. Commuting Patterns
2.2.2. Public Transit Use Patterns
2.2.3. Demographics and Medical
2.2.4. Self-Efficacy
2.2.5. Active Commuting Behavioral Beliefs
2.2.6. Perceived Behavioral Control for active commuting
2.2.7. Coworker and Spouse active commuting Behavior
2.2.8. Worksite
2.2.9. Community
2.2.10. Environmental Barriers
2.3. Analyses
3. Results
3.1. Differences between Public Transit Riders and Non-Public Transit Riders

{kind=link}
| Variable | Non Public Transit Riders (n = 596) | Public Transit Riders (n = 152) | ||
|---|---|---|---|---|
| n (%) | Mean (SD) | n (%) | Mean (SD) | |
| Individual variables | ||||
| Age *** | 43.30 (11.11) | 39.54 (12.00) | ||
| Sex ** | ||||
| Male | 184 (34.2) | 65 (46.4) | ||
| Female | 354 (65.8) | 75 (53.6) | ||
| Marital Status (% Married/partnered) | ||||
| Married/partnered | 423 (74.9) | 101 (70.1) | ||
| Single, divorced, widowed | 142 (25.1) | 43 (29.9) | ||
| Race/ethnicity * | ||||
| Non-Hispanic White | 493 (92.5) | 119 (85.6) | ||
| Non-Hispanic Black | 15 (2.8) | 6 (4.3) | ||
| All other racial/ethnic groups | 25 (4.7) | 14 (10.1) | ||
| Number of children * | 0.56 (0.85) | 0.37 (0.74) | ||
| Income level * | ||||
| <$30 K/year | 27 (5.2) | 13 (9.5) | ||
| $30–60 K/year | 148 (28.6) | 48 (35.0) | ||
| >$60 K/year | 343 (66.2) | 76 (55.5) | ||
| Education level | ||||
| High school graduate, some college | 73 (13.6) | 18 (12.9) | ||
| College degree or higher | 463 (86.4) | 122 (87.1) | ||
| Body Mass Index (kg/m2) | 25.75 (5.45) | 25.88 (5.30) | ||
| Number of reported chronic diseases | 0.71 (1.07) | 0.76 (1.07) | ||
| Number of cars in the household *** | 2.98 (0.82) | 2.29 (0.95) | ||
| Employment level (% employed full time) * | ||||
| Employed full time | 557 (93.9) | 135 (88.8) | ||
| employed part time | 36 (6.1) | 17 (11.2) | ||
| Employment category * | ||||
| Health/medical | 43 (7.2) | 9 (5.9) | ||
| Administrative/clerical | 48 (8.1) | 17 (11.2) | ||
| Education K-12 | 189 (31.8) | 2 (1.3) | ||
| Higher education/research | 126 (21.2) | 55 (36.2) | ||
| Government/civil service | 70 (11.8) | 17 (11.2) | ||
| Blue collar | 18 (3.0) | 8 (5.3) | ||
| White collar | 100 (16.8) | 44 (28.9) | ||
| Employment length *** | ||||
| less than 2 years | 109 (18.4) | 57 (37.7) | ||
| 2 years or more | 483 (81.6) | 94 (62.3) | ||
| Self-efficacy for bicycling skills (range:1–4) ** | 2.87 (1.07) | 3.23 (1.04) | ||
| AC behavioral beliefs score (range:13–91) | 69.41 (11.01) | 69.74 (12.35) | ||
| Perceived behavioral control for AC (range: 7–42) *** | 20.49 (7.97) | 26.89 (8.99) | ||
| Interpersonal variables | ||||
| Spouse AC (times/week) ** | 0.65 (2.25) | 1.21 (3.07) | ||
| Spouse PT travel (times/week) *** | 0.20 (1.23) | 1.09 (2.84) | ||
| Perceived coworker AC (range:1–5) * | 1.53 (0.74) | 1.82 (1.02) | ||
| Worksite variables | ||||
| Employer size * | ||||
| 1–100 employees | 326 (54.9) | 67 (44.4) | ||
| more than 100 employees | 268 (45.1) | 84 (55.6) | ||
| Number of employer supports for AC (range: 0–7) *** | 2.37 (1.69) | 2.96 (1.63) | ||
| Perceived employer support for AC (range: 1–5) ** | 2.66 (1.33) | 2.99 (1.23) | ||
| Perceived parking problems (range: 5–15) *** | 6.20 (3.35) | 8.69 (3.29) | ||
| Community variables | ||||
| Number of community supports for AC (range: 0–3) *** | 1.46 (0.91) | 1.94 (0.73) | ||
| Perceived community support for AC (range: 5–25) | 16.82 (4.79) | 17.12 (4.31) | ||
| Perceived pedestrian friendliness for AC (range: 1–5) | 3.51 (1.24) | 3.67 (1.23) | ||
| Perceive bicycle friendliness for AC (range: 1–5) | 3.29 (1.24) | 3.39 (1.14) | ||
| Perceived distance to work | ||||
| Less than 20 min bike ride | 210 (37.7) | 52 (35.4) | ||
| Greater than 20 min bike ride | 347 (62.3) | 95 (64.6) | ||
| Less than 20 min walk | 81 (14.8) | 14 (10.0) | ||
| Greater than 20 min walk | 467 (85.2) | 126 (90.0) | ||
| Environment variables (range 1–5) | ||||
| Lack of on street bike lanes *** | 2.90 (1.53) | 2.17 (1.30) | ||
| Lack of off street walking/biking paths *** | 2.96 (1.55) | 2.25 (1.40) | ||
| Lack of sidewalks *** | 2.87 (1.57) | 2.14 (1.43) | ||
| Speed and volume of traffic along route *** | 3.27 (1.51) | 2.81 (1.45) | ||
| Perceived crime along route | 2.04 (1.35) | 2.14 (1.34) | ||
| Difficult terrain * | 2.81 (1.46) | 2.50 (1.37) | ||
| Bad weather | 3.53 (1.34) | 3.36 (1.37) | ||
3.2. Public Transit Riders’ Distances and Habits
3.3. Factors Associated with Being an Active Commuter
| Variable | Association with AC | ||
|---|---|---|---|
| OR | CI | p | |
| Individual variables | |||
| Age | 0.94 | 0.93–0.96 | <0.001 |
| Sex | |||
| Male (referent) | 1 | ||
| Female | 0.52 | 0.36–0.74 | <0.001 |
| Marital status | |||
| Not married (referent) | 1 | ||
| Married | 0.6 | 0.42–0.87 | 0.007 |
| Number of children | 0.7 | 0.55–0.88 | 0.002 |
| Income level | |||
| <$30 K/year | 1 | ||
| $30–60 K/year | 0.58 | 0.28–1.19 | 0.14 |
| >$60 K/year | 0.46 | 0.23–0.92 | 0.03 |
| Race/ethnicity | |||
| Non-Hispanic White (referent) | 1 | ||
| Non-Hispanic Black | 0.3 | 0.08–1.08 | 0.06 |
| All other racial/ethnic groups | 2.61 | 1.30–5.23 | 0.007 |
| Employment length | |||
| less than 2 years | 1 | ||
| 2 years or more | 0.61 | 0.42–0.90 | 0.01 |
| Body Mass Index (kg/m2) | 0.91 | 0.87–0.94 | <0.001 |
| Number of reported chronic diseases | 0.73 | 0.61–0.88 | 0.001 |
| Number of cars in the household | 0.46 | 0.37–0.58 | <0.001 |
| Self-efficacy for bicycling skills | 1.99 | 1.63–2.44 | <0.001 |
| AC behavioral beliefs score | 1.04 | 1.02–1.06 | <0.001 |
| Perceived behavioral control for AC | 1.22 | 1.18–1.27 | <0.001 |
| Interpersonal variables | |||
| Spouse AC (times/week) | 1.34 | 1.23–1.46 | <0.001 |
| Spouse PT travel (times/week) | 1.06 | 0.97–1.16 | 0.22 |
| Perceived coworker AC | 1.8 | 1.46–2.22 | <0.001 |
| Worksite variables | |||
| Employer size | |||
| 1–100 employees (referent) | 1 | ||
| more than 100 employees | 0.7 | 0.50–0.98 | 0.04 |
| Number of employer supports for AC | 1.22 | 1.10–1.34 | <0.001 |
| Perceived employer support for AC | 1.43 | 1.25–1.63 | <0.001 |
| Perceived parking problems | 1.07 | 1.02–1.13 | 0.004 |
| Community variables | |||
| Perceived distance to work | |||
| Less than 20 min bike ride | 3.6 | 2.26–5.73 | <0.001 |
| Greater than 20 min bike ride (referent) | 1 | ||
| Less than 20 min walk | 7.3 | 5.31–11.79 | <0.001 |
| Greater than 20 min walk (referent) | 1 | ||
| Number of community supports for AC | 0.26 | 0.17–0.90 | <0.001 |
| Perceived community support for AC | 1.03 | 0.99–1.07 | 0.08 |
| Perceived pedestrian friendliness for AC | 1.43 | 1.23–1.66 | <0.001 |
| Perceive bicycle friendliness for AC | 1.34 | 1.16–1.56 | <0.001 |
| Environment variables | |||
| Lack of on street bike lanes | 0.64 | 0.55–0.74 | <0.001 |
| Lack of off street walking/biking paths | 0.6 | 0.52–0.69 | <0.001 |
| Lack of sidewalks | 0.63 | 0.54–0.72 | <0.001 |
| Speed and volume of traffic along route | 0.65 | 0.57–0.74 | <0.001 |
| Perceived crime along route | 0.74 | 0.63–0.87 | <0.001 |
| Difficult terrain | 0.62 | 0.54–0.73 | <0.001 |
| Bad weather | 0.82 | 0.72–0.94 | 0.004 |
3.4. Predictors of Active Commuting
| Variable | Association with AC | ||
|---|---|---|---|
| OR | 95% CI | p | |
| Individual variables | |||
| Age | 0.94 | 0.89–0.98 | 0.008 |
| Number of children | 0.49 | 0.28–0.88 | 0.02 |
| Sex | |||
| Male (referent) | 1 | ||
| Female | 0.68 | 0.28–1.63 | 0.43 |
| Race/ethnicity | |||
| Non-Hispanic White (referent) | 1 | ||
| Non-Hispanic Black | 3.61 | 0.40–32.84 | 0.25 |
| Other racial/ethnic group | 2.23 | 0.38–12.94 | 0.37 |
| Income level | |||
| <$30 K/year (referent) | 1 | ||
| $30–60 K/year | 0.55 | 0.05–6.53 | 0.64 |
| >$60 K/year | 3.14 | 0.22–45.08 | 0.4 |
| Marital status | |||
| Not married | 3.63 | 1.12–11.74 | 0.03 |
| Married (referent) | 1 | ||
| Number of cars in the household | 1.28 | 0.68–2.40 | 0.44 |
| Self-efficacy for bicycling skills | 1.11 | 0.68–1.81 | 0.67 |
| AC behavioral beliefs score | 1.02 | 0.98–1.06 | 0.35 |
| Perceived behavioral control for AC | 1.25 | 1.15–1.36 | <0.001 |
| Public transit use | |||
| NPTR (referrent) | 1 | ||
| PTR | 12.29 | 3.59–42.10 | <0.001 |
| Interpersonal variables | |||
| Spouse AC (times/week) | 1.53 | 1.19–1.96 | 0.001 |
| Perceived coworker AC | 1.45 | 0.81–2.60 | 0.21 |
| Worksite variables | |||
| Perceived employer support for AC | 1.28 | 0.90–1.84 | 0.17 |
| Community variables | |||
| Perceived pedestrian friendliness for AC | 1.17 | 0.83–1.64 | 0.37 |
| Perceived bike time to work | |||
| More than 20 min (referent) | 1 | ||
| Less than 20 min | 7.23 | 2.59–20.17 | <0.001 |
| Environment variables | |||
| Lack of on street bike lanes | 1.86 | 1.08–3.21 | 0.02 |
| Lack of sidewalks | 0.65 | 0.40–1.08 | 0.1 |
| Speed and volume of traffic along route | 0.59 | 0.37–0.95 | 0.03 |
| Perceived crime along route | 1.1 | 0.71–1.70 | 0.66 |
| Difficult terrain | 1.16 | 0.77–1.74 | 0.48 |
| Bad weather | 1.86 | 1.28–2.70 | 0.001 |
4. Discussion and Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Physical Activity Guidelines Advisory Committee. Physical Activity Guidelines Advisory Committee Report, 2008; US Department of Health and Human Services: Washington, DC, USA, 2008. [Google Scholar]
- Brownson, R.C.; Boehmer, T.K.; Luke, D.A. Declining rates of physical activity in the united states: What are the contributors? Annu. Rev. Public Health 2005, 26, 421–443. [Google Scholar] [CrossRef] [PubMed]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the american college of sports medicine and the american heart association. Med. Sci. Sports Exerc. 2007, 39, 1423–1434. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control Prevention. U.S. Physical Activity Statistics: 2007 State Demographic Data Comparison. Available online: http://www.cdc.gov/physicalactivity/data/ (accessed on 15 April 2015).
- Robert Wood Johnson Foundation. F as in Fat: How Obesity Threatens America’s Future; Trust for America’s Health: Washington, DC, USA, 2010. [Google Scholar]
- Centers for Disease Control and Prevention. An Explanation of U.S. Physical Activity Surveys. Available online: http://www.cdc.gov/physicalactivity/professionals/data/explanation.html (accessed on 15 April 2015).
- Pucher, J.; Buehler, R.; Bassett, D.R.; Dannenberg, A.L. Walking and cycling to health: A comparative analysis of city, state, and international data. Am. J. Public Health 2010, 100, 1986–1992. [Google Scholar] [CrossRef] [PubMed]
- Lindstrom, M. Means of transportation to work and overweight and obesity: A population-based study in southern sweden. Prev. Med. 2008, 46, 22–28. [Google Scholar] [CrossRef] [PubMed]
- Sugiyama, T.; Merom, D.; Reeves, M.; Leslie, E.; Owen, N. Habitual active transport moderates the association of TV viewing time with body mass index. J. Phys. Act, Health 2010, 7, 11–16. [Google Scholar]
- Wanner, M.; Gotschi, T.; Martin-Diener, E.; Kahlmeier, S.; Martin, B.W. Active transport, physical activity, and body weight in adults: A systematic review. Am. J. Prev. Med. 2012, 42, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Hamer, M.; Chida, Y. Active commuting and cardiovascular risk: A meta-analytic review. Prev. Med. 2008, 46, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Andersen, L.B.; Schnohr, P.; Schroll, M.; Hein, H.O. All-cause mortality associated with physical activity during leisure time, work, sports, and cycling to work. Arch. Intern. Med. 2000, 160, 1621–1628. [Google Scholar] [CrossRef] [PubMed]
- Shephard, R.J. Is active commuting the answer to population health? Sports Med. 2008, 38, 751–758. [Google Scholar] [CrossRef] [PubMed]
- Humphreys, D.K.; Goodman, A.; Ogilvie, D. Associations between active commuting and physical and mental wellbeing. Prev. Med. 2013, 57, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Hansson, E.; Mattisson, K.; Bjork, J.; Ostergren, P.O.; Jakobsson, K. Relationship between commuting and health outcomes in a cross-sectional population survey in southern sweden. BMC Public Health 2011, 11, 834. [Google Scholar] [CrossRef] [PubMed]
- Westman, J.; Johansson, M.; Olsson, L.E.; Martensson, F.; Friman, M. Children's affective experience of every-day travel. J. Transp. Geogr. 2013, 29, 95–102. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services (USDHHS). Healthy People 2020. Available online: http://www.healthypeople.gov/2020/default.aspx (accessed on 15 April 2015).
- Zheng, Y. The benefit of public transportation: Physical activity to reduce obesity and ecological footprint. Prev. Med. 2008, 46, 4–5. [Google Scholar] [CrossRef] [PubMed]
- Morabia, A.; Mirer, F.E.; Amstislavski, T.M.; Eisl, H.M.; Werbe-Fuentes, J.; Gorczynski, J.; Goranson, C.; Wolff, M.S.; Markowitz, S.B. Potential health impact of switching from car to public transportation when commuting to work. Am. J. Public Health 2010, 100, 2388–2391. [Google Scholar] [CrossRef] [PubMed]
- Maibach, E.; Steg, L.; Anable, J. Promoting physical activity and reducing climate change: Opportunities to replace short car trips with active transportation. Prev. Med. 2009, 49, 326–327. [Google Scholar] [CrossRef] [PubMed]
- U.S. Census Bureau. Commuting in the United States: 2009; US Department of Commerce: Washington, DC, USA, 2011.
- Alliance for Biking & Walking. Bicycling and Walking in the United States 2014 Benchmarking Report; Alliance for Biking & Walking: Washington, DC, USA, 2014; p. 268. [Google Scholar]
- American Public Transportation Association. 2012 Public Transportation Fact Book. Appendix A: Historical Tables; American Public Transportation Association: Washington, DC, USA, 2012. [Google Scholar]
- Besser, L.M.; Dannenberg, A.L. Walking to public transit: Steps to help meet physical activity recommendations. Am. J. Prev. Med. 2005, 29, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Lachapelle, U. Walk, bicycle and transit trips of transit dependent and choice riders in the NHTS 2009. J. Phys. Act. Health 2014, 2014. [Google Scholar] [CrossRef]
- Lachapelle, U.; Frank, L.D. Transit and health: Mode of transport, employer-sponsored public transit pass programs, and physical activity. J. Public Health Policy 2009, 30, S73–S94. [Google Scholar] [CrossRef] [PubMed]
- Chaix, B.; Kestens, Y.; Duncan, S.; Merrien, C.; Thierry, B.; Pannier, B.; Brondeel, R.; Lewin, A.; Karusisi, N.; Perchoux, C.; et al. Active transportation and public transportation use to achieve physical activity recommendations? A combined gps, accelerometer, and mobility survey study. Int. J. Behav. Nutr. Phys. ACT. 2014, 11, 124. [Google Scholar] [CrossRef] [PubMed]
- Rissel, C.; Curac, N.; Greenaway, M.; Bauman, A. Physical activity associated with public transport use—A review and modelling of potential benefits. Int. J. Environ. Res. Public Health 2012, 9, 2454–2478. [Google Scholar] [CrossRef] [PubMed]
- Edwards, R.D. Public transit, obesity, and medical costs: Assessing the magnitudes. Prev. Med. 2008, 46, 14–21. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, J.M.; Stokes, R.J.; Cohen, D.A.; Kofner, A.; Ridgeway, G.K. The effect of light rail transit on body mass index and physical activity. Am. J. Prev. Med. 2010, 39, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Wener, R.E.; Evans, G.W. A morning stroll: Levels of physical activity in car and mass transit commuting. Environ. Behav. 2007, 39, 62–74. [Google Scholar] [CrossRef]
- Litman, T. Short and Sweet. Analysis of Shorter Trips Using National Personal Travel Survey Data; Victoria Transport Policy Institute: Victoria, BC, Canada, 2014. [Google Scholar]
- Litman, T. Transportation and public health. Annu. Rev. Public Health 2013, 34, 217–233. [Google Scholar] [CrossRef] [PubMed]
- Villanueva, K.; Giles-Corti, B.; McCormack, G. Achieving 10,000 steps: A comparison of public transport users and drivers in a university setting. Prev. Med. 2008, 47, 338–341. [Google Scholar] [CrossRef] [PubMed]
- Lachapelle, U.; Frank, L.; Saelens, B.E.; Sallis, J.F.; Conway, T.L. Commuting by public transit and physical activity: Where you live, where you work, and how you get there. J. Phys. Act. Health 2011, 8, S72–S82. [Google Scholar] [PubMed]
- Stokes, R.J.; MacDonald, J.; Ridgeway, G. Estimating the effects of light rail transit on health care costs. Health Place 2008, 14, 45–58. [Google Scholar] [CrossRef] [PubMed]
- Rabi, A.; de Nazelle, A. Benefits of shift from car to active transport. Transp. Policy 2013, 19, 121–131. [Google Scholar]
- Baranowski, T.; Anderson, C.; Carmack, C. Mediating variable framework in physical activity interventions. How are we doing? How might we do better? Am. J. Prev. Med. 1998, 15, 266–297. [Google Scholar] [CrossRef] [PubMed]
- De Bruijn, G.J.; Kremers, S.P.; Singh, A.; van den Putte, B.; van Mechelen, W. Adult active transportation: Adding habit strength to the theory of planned behavior. Am. J. Prev. Med. 2009, 36, 189–194. [Google Scholar]
- Chaney, R.A.; Bernard, A.L.; Wilson, B.R. Characterizing active transportation behavior among college students using the theory of planned behavior. Int. Q. Community Health Educ. 2013, 34, 283–294. [Google Scholar] [CrossRef] [PubMed]
- Murtagh, S.; Rowe, D.A.; Elliott, M.A.; McMinn, D.; Nelson, N.M. Predicting active school travel: The role of planned behavior and habit strength. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 65. [Google Scholar] [CrossRef] [PubMed]
- Troped, P.J.; Saunders, R.P.; Pate, R.R.; Reininger, B.; Addy, C.L. Correlates of recreational and transportation physical activity among adults in a new england community. Prev. Med. 2003, 37, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Panter, J.R.; Jones, A. Attitudes and the environment as determinants of active travel in adults: What do and don’t we know? J. Phys. Act. Health 2010, 7, 551–561. [Google Scholar] [PubMed]
- Panter, J.R.; Jones, A.P.; van Sluijs, E.M.; Griffin, S.J.; Wareham, N.J. Environmental and psychological correlates of older adult’s active commuting. Med. Sci. Sports Exerc. 2011, 43, 1235–1243. [Google Scholar] [CrossRef] [PubMed]
- Ajzen, I. The theory of planned behavior. Organ. Behav. Hum. Decis. Process. 1991, 13, 179–204. [Google Scholar] [CrossRef]
- Bandura, A. Social Foundations of Thought and Action: A Social Cognitive Theory; Prentice-Hall: Englewood Cliffs, NJ, USA, 1986; p. 617. [Google Scholar]
- Conn, V.S.; Tripp-Reimer, T.; Maas, M.L. Older women and exercise: Theory of planned behavior beliefs. Public Health Nurs. 2003, 20, 153–163. [Google Scholar] [CrossRef] [PubMed]
- Davis, S.C.; Diegel, S.W.; Boundy, R.G. Chapter 8. Household vehicles and characteristics. In Transportation Energy Data Book, 33rd ed.Oak Ridge National Laboratory: Oak Ridge, TN, USA, 2014. [Google Scholar]
- Djurhuus, S.; Hansen, H.S.; Aadahl, M.; Glumer, C. The association between access to public transportation and self-reported active commuting. Int. J. Environ. Res. Public Health 2014, 11, 12632–12651. [Google Scholar] [CrossRef] [PubMed]
- Transit Coopertive Research Program. Current Practices in Greenhouse Gas Emissions. Savings from Transit; Transportation Research Board: Washington, DC, USA, 2010. [Google Scholar]
- Vuchic, V.R. Transportation for Livable Cities; Center for Urban Policy Research, University of Michigan: Ann Arbor, MI, USA, 1999. [Google Scholar]
- Yang, L.; Sahlqvist, S.; McMinn, A.; Griffin, S.J.; Ogilvie, D. Interventions to promote cycling: Systematic review. BMJ 2010, 341, c5293. [Google Scholar] [CrossRef] [PubMed]
- van der Kloof, A.; Bastiaanssen, J.; Martens, K. Bicycle lessons, activity participation and empowerment. Case Stud. Transp. Policy 2014, 2, 89–95. [Google Scholar]
- Kaczynski, A.T.; Bopp, M.J.; Wittman, P. Association of workplace supports with active commuting. Prev. Chronic Dis. 2010, 7, A127. [Google Scholar] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bopp, M.; Gayah, V.V.; Campbell, M.E. Examining the Link Between Public Transit Use and Active Commuting. Int. J. Environ. Res. Public Health 2015, 12, 4256-4274. https://doi.org/10.3390/ijerph120404256
Bopp M, Gayah VV, Campbell ME. Examining the Link Between Public Transit Use and Active Commuting. International Journal of Environmental Research and Public Health. 2015; 12(4):4256-4274. https://doi.org/10.3390/ijerph120404256
Chicago/Turabian StyleBopp, Melissa, Vikash V. Gayah, and Matthew E. Campbell. 2015. "Examining the Link Between Public Transit Use and Active Commuting" International Journal of Environmental Research and Public Health 12, no. 4: 4256-4274. https://doi.org/10.3390/ijerph120404256
APA StyleBopp, M., Gayah, V. V., & Campbell, M. E. (2015). Examining the Link Between Public Transit Use and Active Commuting. International Journal of Environmental Research and Public Health, 12(4), 4256-4274. https://doi.org/10.3390/ijerph120404256