
Association of Exposure to Particular Matter and Carotid Intima-Media Thickness: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Eligibility Criteria
2.2. Study Selection
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
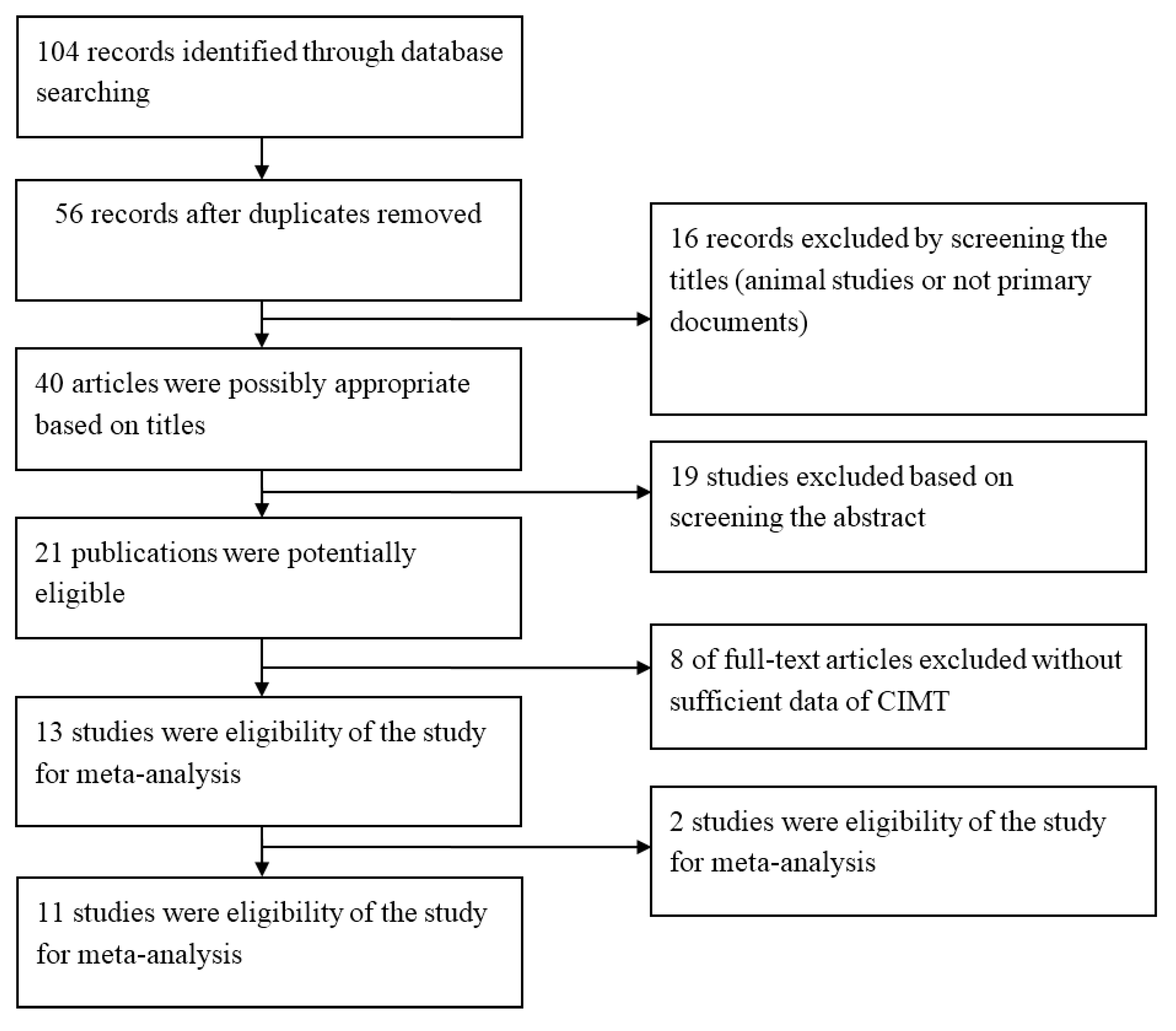
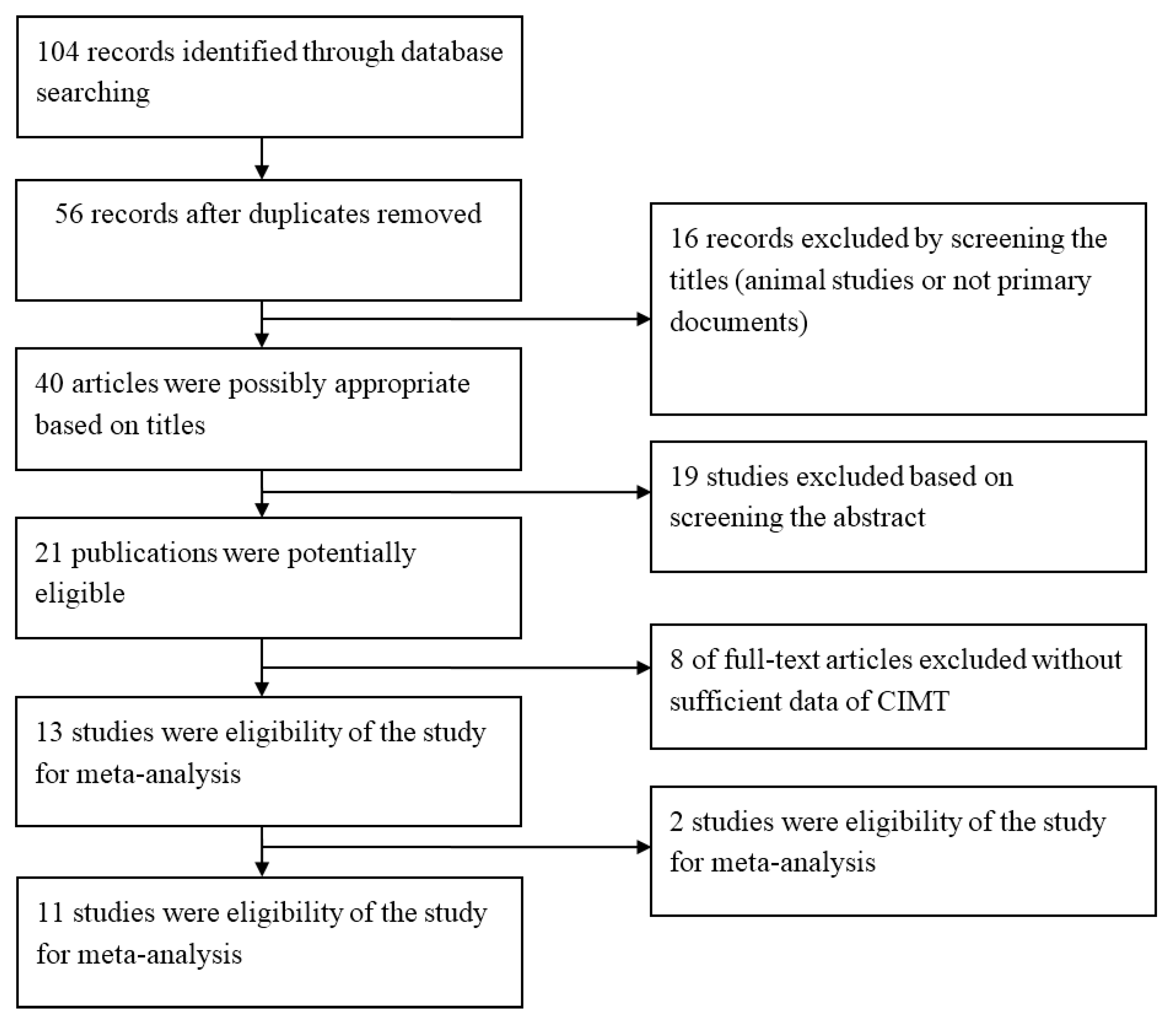
3.1. Literature Search
3.2. Study Characteristics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author,Year [Reference No.] | Location | Period | Study design | Samplesize | Age (Years) | Exposure Measurement | Statistical Analysis |
|---|---|---|---|---|---|---|---|
| Su, 2015 [16] | Taiwan | 2009–2011 | cross-sectional | 689 | 35–65 | Individual | multiple linearregression model |
| Perez, 2015 [17] | Europe | 1997–2009 | cross-sectional | 9183 | 42–68 | Individual | linear regression model |
| Kim, 2014 [18] | USA | 2000–2002 | cross-sectional | 5488 | 45–84 | individual | multiple linearregression model |
| Gan, 2014 [19] | Canada | 2004–2011 | longitudinal | 509 | 30–65 | individual | general linear regression model |
| Sun, 2013 [20] | USA | 2000–2002 | cross-sectional | 6256 | 45–84 | ambient | multiple linearregression model |
| Adar, 2013 [21] | USA | 2000–2005 | cross-sectional | 5660 | 45–84 | individual | longitudinal mixed model |
| Breton, 2012 [22] | USA | 2007–2009 | cross-sectional | 768 | 18–27 | ambient | linear regression model |
| Tonne, 2012 [23] | Britain | 2002–2006 | cross-sectional | 2348 | 55–67 | individual | generalized linear regression models |
| Künali, 2010 [24] | USA | 1994–2006 | cross-sectional, longitudinal | 1483 | >30 | ambient | linear regression model |
| Lenters, 2010 [25] | The Netherlands | 1999–2000 | cross-sectional | 745 | 45–84 | individual | multiple linearregression model |
| Künali, 2005 [26] | USA | 1998–2003 | cross-sectional | 798 | >40 | ambient | linear regression model |
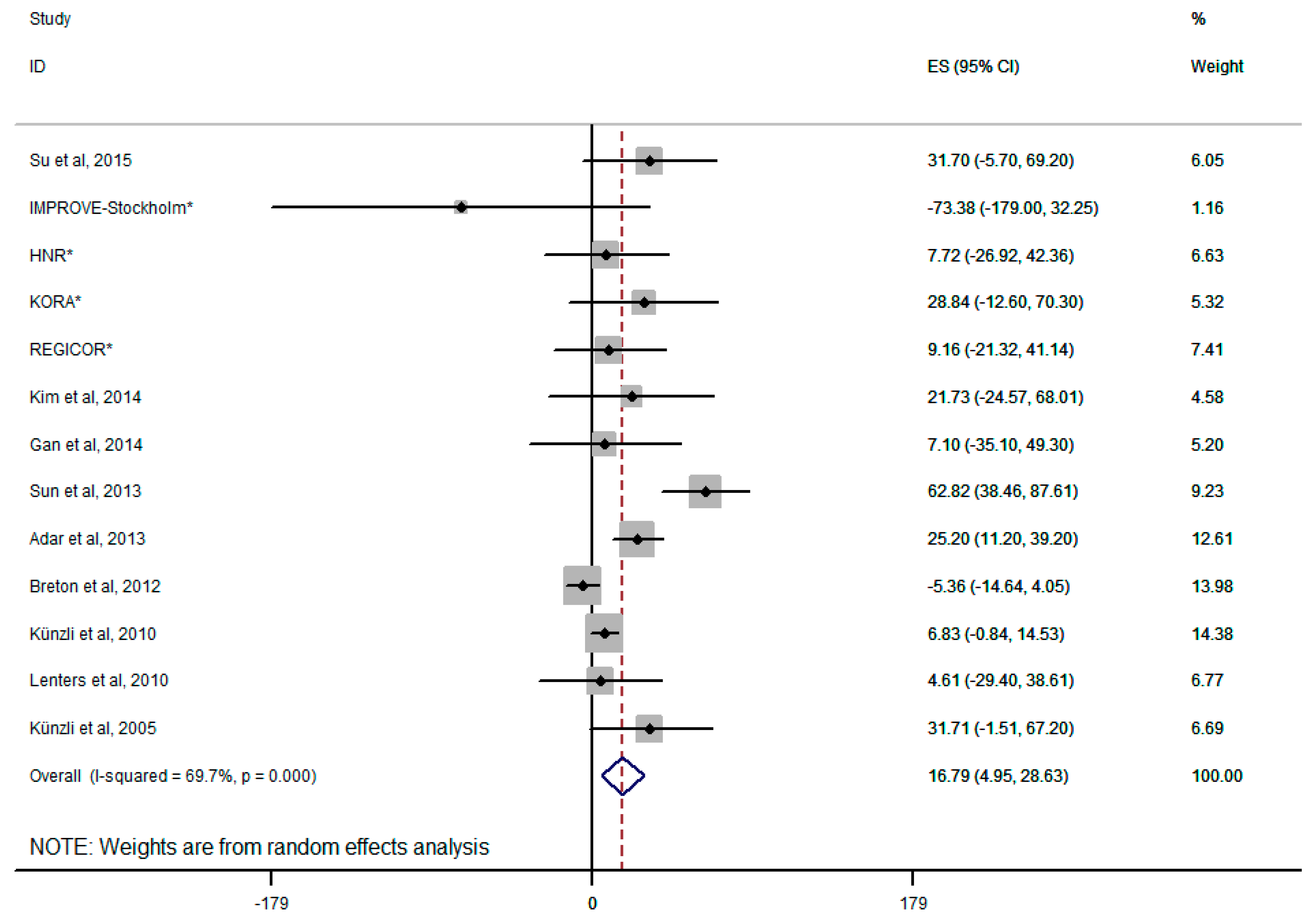
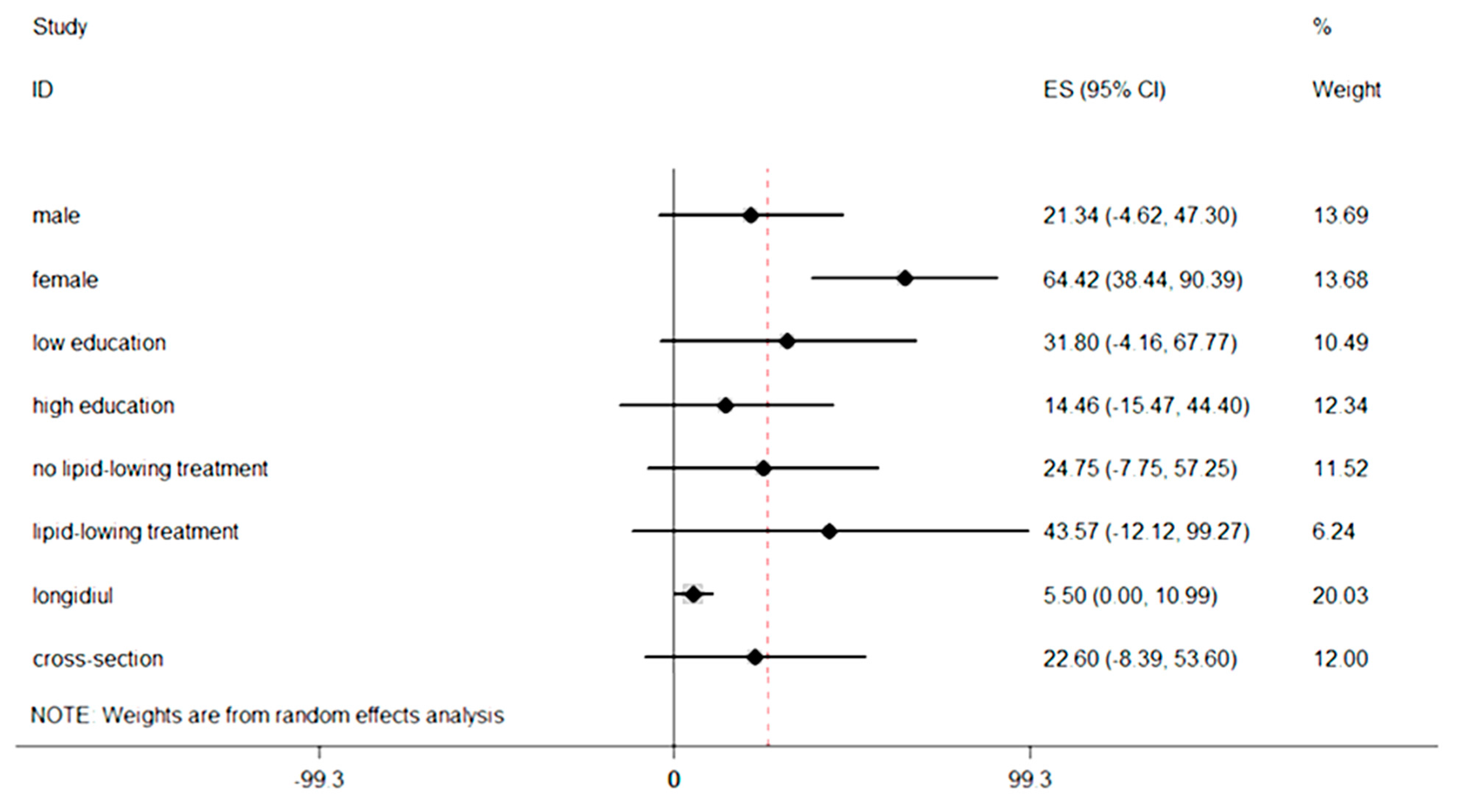
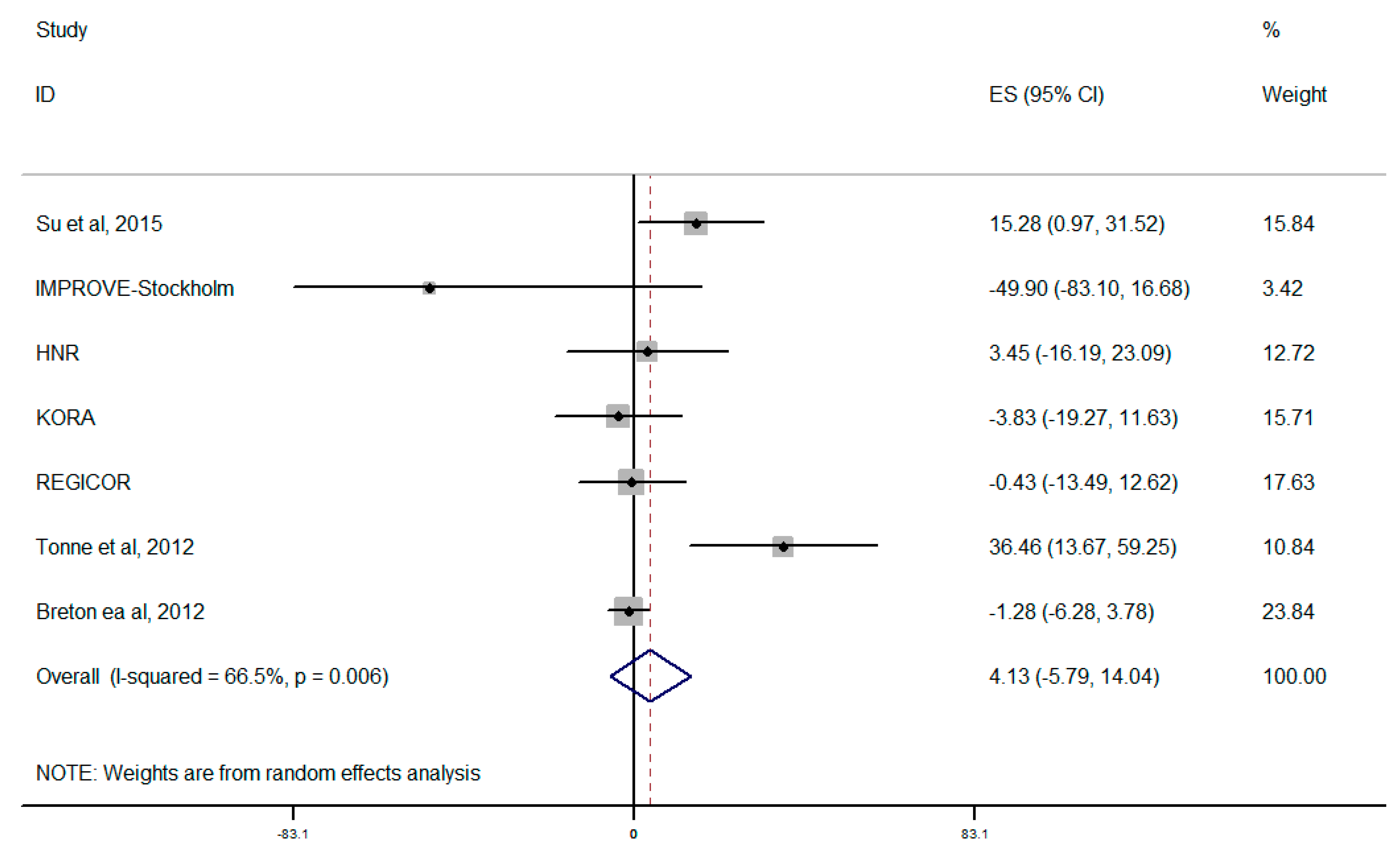
3.3. Analysis
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Miller, K.A.; Siscovick, D.S.; Sheppard, L.; Shepherd, K.; Sullivan, J.H.; Anderson, G.L.; Kaufman, J.D. Long-term exposure to air pollution and incidence of cardiovascular events in women. N. Engl. J. Med. 2007, 356, 447–458. [Google Scholar] [CrossRef] [PubMed]
- Pope, C.R.; Burnett, R.T.; Thurston, G.D.; Thun, M.J.; Calle, E.E.; Krewski, D.; Godleski, J.J. Cardiovascular mortality and long-term exposure to particulate air pollution: Epidemiological evidence of general pathophysiological pathways of disease. Circulation 2004, 109, 71–77. [Google Scholar] [CrossRef] [PubMed]
- Hoek, G.; Brunekreef, B.; Goldbohm, S.; Fischer, P.; van den Brandt, P.A. Association between mortality and indicators of traffic-related air pollution in the Netherlands: A cohort study. Lancet 2002, 360, 1203–1209. [Google Scholar] [CrossRef]
- Dockery, D.W.; Pope, C.A., III; Xu, X.; Spengler, J.D.; Ware, J.H.; Fay, M.E.; Ferris, B.G., Jr.; Speizer, F.E. An association between air pollution and mortality in six U.S. cities. N. Engl. J. Med. 1993, 329, 1753–1759. [Google Scholar] [CrossRef] [PubMed]
- Liang, R.; Zhang, B.; Zhao, X.; Ruan, Y.; Lian, H.; Fan, Z. Effect of exposure to PM2.5 on blood pressure: A systematic review and meta-analysis. J. Hypertens 2014, 32, 2130–2140. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.; Sun, Z.; Ruan, Y.; Yan, J.; Mukherjee, B.; Yang, F.; Duan, F.; Sun, L.; Liang, R.; Lian, H.; et al. Personal black carbon exposure influences ambulatory blood pressure: Air pollution and cardiometabolic disease (AIRCMD-China) study. Hypertension 2014, 63, 871–877. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Rajagopalan, S.; Pope, C.A., III; Brook, J.R.; Bhatnagar, A.; Diez-Roux, A.V.; Holguin, F.; Hong, Y.; Luepker, R.V.; Mittleman, M.A.; et al. Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the American Heart Association. Circulation 2010, 121, 2331–2378. [Google Scholar] [CrossRef] [PubMed]
- Libby, P.; Theroux, P. Pathophysiology of coronary artery disease. Circulation 2005, 111, 3481–3488. [Google Scholar] [CrossRef] [PubMed]
- Lusis, A.J. Atherosclerosis. Nature 2000, 407, 233–241. [Google Scholar] [CrossRef] [PubMed]
- Ross, R. The pathogenesis of atherosclerosis: A perspective for the 1990s. Nature 1993, 362, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Stein, J.H.; Korcarz, C.E.; Hurst, R.T.; Lonn, E.; Kendall, C.B.; Mohler, E.R.; Najjar, S.S.; Rembold, C.M.; Post, W.S. American Society of Echocardiography Carotid Intima-Media Thickness Task Force.Use of carotid ultrasound to identify subclinical vascular disease and evaluate cardiovascular disease risk: A consensus statement from the American Society of Echocardiography Carotid Intima-Media Thickness Task Force. Endorsed by the Society for Vascular Medicine. J. Am. Soc. Echocardiogr. 2008, 21, 93–111. [Google Scholar] [PubMed]
- Chambless, L.E.; Folsom, A.R.; Clegg, L.X.; Sharrett, A.R.; Shahar, E.; Nieto, F.J.; Rosamond, W.D.; Evans, G. Carotid wall thickness is predictive of incident clinical stroke: The Atherosclerosis Risk in Communities (ARIC) Study. Am. J. Epidemiol. 2000, 151, 478–487. [Google Scholar] [CrossRef] [PubMed]
- Chambless, L.E.; Heiss, G.; Folsom, A.R.; Rosamond, W.; Szklo, M.; Sharrett, A.R.; Clegg, L.X. Association of coronary heart disease incidence with carotid arterial wall thickness and major risk factors: The Atherosclerosis Risk in Communities (ARIC)study, 1987–1993. Am. J. Epidemiol. 1997, 146, 483–494. [Google Scholar] [CrossRef] [PubMed]
- Bauer, M.; Moebus, S.; Möhlenkamp, S.; Dragano, N.; Nonnemacher, M.; Fuchsluger, M.; Kessler, C.; Jakobs, H.; Memmesheimer, M.; Erbel, R.; et al. Urban particulate matter air pollution is associated with subclinical atherosclerosis: Results from the HNR (Heinz Nixdorf Recall) study. J. Am. Coll. Cardiol. 2010, 56, 1803–1808. [Google Scholar] [CrossRef] [PubMed]
- Diez, R.A.; Auchincloss, A.H.; Franklin, T.G.; Raghunathan, T.; Barr, R.G.; Kaufman, J.; Astor, B.; Keeler, J. Long-term exposure to ambient particulate matter and prevalence of subclinical atherosclerosis in the Multi-Ethnic Study of Atherosclerosis. Am. J. Epidemiol. 2008, 167, 667–675. [Google Scholar] [CrossRef] [PubMed]
- Su, T.C.; Hwang, J.J.; Shen, Y.C.; Chan, C.C. Carotid Intima-media thickness and long-term exposure to traffic-related air pollution in middle-aged residents of taiwan: A cross-sectional study. Environ. Health Perspect. 2015, 123, 773–778. [Google Scholar] [CrossRef] [PubMed]
- Perez, L.; Wolf, K.; Hennig, F.; Penell, J.; Basagaña, X.; Foraster, M.; Aguilera, I.; Agis, D.; Beelen, R.; Brunekreef, B.; et al. Air pollution and atherosclerosis: A cross-sectional analysis of four european cohort studies in the ESCAPE study. Environ. Health Perspect. 2015, 123, 795–605. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y.; Sheppard, L.; Kaufman, J.D.; Bergen, S.; Szpiro, A.A.; Larson, T.V.; Adar, S.D.; Diez Roux, A.V.; Polak, J.F.; Vedal, S.; et al. Individual-level concentrations of fine particulate matter chemical components and subclinical atherosclerosis: A cross-sectional analysis based on 2 advanced exposure prediction models in the multi-ethnic study of atherosclerosis. Am. J. Epidemiol. 2014, 180, 718–728. [Google Scholar] [PubMed]
- Gan, W.Q.; Allen, R.W.; Brauer, M.; Davies, H.W.; Mancini, G.B.; Lear, S.A. Long-term exposure to traffic-related air pollution and progression of carotid artery atherosclerosis: A prospective cohort study. BMJ Open 2014, 4. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.; Kaufman, J.D.; Kim, S.Y.; Larson, T.V.; Gould, T.R.; Polak, J.F.; Budoff, M.J.; Diez Roux, A.V.; Vedal, S. Particulate matter components and subclinical atherosclerosis: Common approaches to estimating exposure in a multi-ethnic study of atherosclerosis cross-sectional study. Environ. Health Glob. Access Sci. Source 2013, 12. [Google Scholar] [CrossRef] [PubMed]
- Adar, S.D.; Sheppard, L.; Vedal, S.; Polak, J.F.; Sampson, P.D.; Diez Roux, A.V.; Budoff, M.; Jacobs, D.R., Jr.; Barr, R.G.; Watson, K.; et al. Fine particulate air pollution and the progression of carotid intima-medial thickness: A prospective cohort study from the multi-ethnic study of atherosclerosis and air pollution. PLoS Med. 2013, 10. [Google Scholar] [CrossRef] [PubMed]
- Breton, C.V.; Wang, X.; Mack, W.J.; Berhane, K.; Lopez, M.; Islam, T.S.; Feng, M.; Lurmann, F.; McConnell, R.; Hodis, H.N.; et al. Childhood air pollutant exposure and carotid artery intima-media thickness in young adults. Circulation 2012, 126, 1614–1620. [Google Scholar] [CrossRef] [PubMed]
- Tonne, C.; Yanosky, J.D.; Beevers, S.; Wilkinson, P.; Kelly, F.J. PM mass concentration and PM oxidative potential in relation to carotid intima-media thickness. Epidemiology 2012, 23, 486–494. [Google Scholar] [CrossRef] [PubMed]
- Kunzli, N.; Jerrett, M.; Garcia-Esteban, R.; Basagaña, X.; Beckermann, B.; Gilliland, F.; Medina, M.; Peters, J.; Hodis, H.N.; Mack, W.J.; et al. Ambient air pollution and the progression of atherosclerosis in adults. PLoS ONE 2010, 5. [Google Scholar] [CrossRef]
- Lenters, V.; Uiterwaal, C.S.; Beelen, R.; Bots, M.L.; Fischer, P.; Brunekreef, B.; Hoek, G. Long-term exposure to air pollution and vascular damage in young adults. Epidemiology 2010, 21, 512–520. [Google Scholar] [CrossRef] [PubMed]
- Kunzli, N.; Jerrett, M.; Mack, W.J.; Beckerman, B.; LaBree, L.; Gilliland, F.; Thomas, D.; Peters, J.; Hodis, H.N. Ambient air pollution and atherosclerosis in Los Angeles. Environ. Health Perspect. 2005, 113, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Hodis, H.N.; Mack, W.J.; LaBree, L.; Selzer, R.H.; Liu, C.R.; Liu, C.H.; Azen, S.P. The role of carotid arterial intima-media thickness in predicting clinical coronary events. Ann. Intern. Med. 1998, 128, 262–269. [Google Scholar] [CrossRef] [PubMed]
- Blankenhorn, D.H.; Hodis, N.H. George Lyman Duff Memorial Lecture. Arterial imaging and atherosclerosis reversal. Arterioscler. Thromb. 1994, 14, 177–192. [Google Scholar] [CrossRef] [PubMed]
- Kunzli, N.; Perez, L.; von Klot, S.; Baldassarre, D.; Bauer, M.; Basagana, X.; Breton, C.; Dratva, J.; Elosua, R.; de Faire, U.; et al. Investigating air pollution and atherosclerosis in humans: Concepts and outlook. Prog. Cardiovasc. Dis. 2011, 53, 334–343. [Google Scholar] [CrossRef] [PubMed]
- Johnson, H.M.; Douglas, P.S.; Srinivasan, S.R.; Bond, M.G.; Tang, R.; Li, S.; Chen, W.; Berenson, G.S.; Stein, J.H. Predictors of carotid intima-media thickness progression in young adults: The Bogalusa Heart Study. Stroke 2007, 38, 900–905. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, D.H.; Polak, J.F.; Kronmal, R.A.; Manolio, T.A.; Burke, G.L.; Wolfson, S.K., Jr. Carotid-artery intima and media thickness as a risk factor for myocardial infarction and stroke in older adults. Cardiovascular Health Study CollaborativeResearch Group. N. Engl. J. Med. 1999, 340, 14–22. [Google Scholar] [CrossRef]
- Hoffmann, B.; Moebus, S.; Dragano, N.; Stang, A.; Möhlenkamp, S.; Schmermund, A.; Memmesheimer, M.; Bröcker-Preuss, M.; Mann, K.; Erbel, R.; et al. Chronic residential exposure to particulate matter air pollution and systemic inflammatory markers. Environ. Health Perspect. 2009, 117, 1302–1308. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, R.M.; Adar, S.D.; Szpiro, A.A.; Jorgensen, N.W.; van Hee, V.C.; Barr, R.G.; O’Neill, M.S.; Herrington, D.M.; Polak, J.F.; Kaufman, J.D.; et al. Vascular responses to longandshort-term exposure to fine particulate matter: MESA Air (Multi-Ethnic Study of Atherosclerosis and AirPollution). J. Am. Coll. Cardiol. 2012, 60, 2158–2166. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Urch, B.; Dvonch, J.T.; Bard, R.L.; Speck, M.; Keeler, G.; Morishita, M.; Marsik, F.J.; Kamal, A.S.; Kaciroti, N.; et al. Insights into the mechanisms and mediatorsof the effects of air pollution exposure on blood pressure and vascular function in healthy humans. Hypertension 2009, 54, 659–667. [Google Scholar] [CrossRef] [PubMed]
- Briet, M.; Collin, C.; Laurent, S.; Tan, A.; Azizi, M.; Agharazii, M.; Jeunemaitre, X.; Alhenc-Gelas, F.; Boutouyrie, P. Endothelial function and chronic exposure to airpollution in normal male subjects. Hypertension 2007, 50, 970–976. [Google Scholar] [CrossRef] [PubMed]
- Santoro, L.; D’Onofrio, F.; Campo, S.; Ferraro, P.M.; Tondi, P.; Campo, V.; Flex, A.; Gasbarrini, A.; Santoliquido, A. Endothelial dysfunction but not increased carotid intima-media thickness in young European women with endometriosis. Hum. Reprod. 2012, 27, 1320–1326. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, B.; Moebus, S.; Möhlenkamp, S.; Stang, A.; Lehmann, N.; Dragano, N.; Schmermund, A.; Memmesheimer, M.; Mann, K.; Erbel, R.; et al. Residential exposure to traffic is associated with coronary atherosclerosis. Circulation 2007, 116, 489–496. [Google Scholar] [CrossRef] [PubMed]
- Wilker, E.H.; Mittleman, M.A.; Coull, B.A.; Gryparis, A.; Bots, M.L.; Schwartz, J.; Sparrow, D. Long-term exposure to black carbon and carotid intima-media thickness: The normative aging study. Environ. Health Perspect. 2013, 121, 1061–1067. [Google Scholar] [CrossRef] [PubMed]
- Sun, Q.; Wang, A.; Jin, X.; Natanzon, A.; Duquaine, D.; Brook, R.D.; Aguinaldo, J.G.; Fayad, Z.A.; Fuster, V.; Lippmann, M.; et al. Long-term air pollution exposure and acceleration of atherosclerosis and vascular inflammation in an animal model. JAMA 2005, 294, 3003–3010. [Google Scholar] [CrossRef] [PubMed]
- Suwa, T.; Hogg, J.C.; Quinlan, K.B.; Ohgami, A.; Vincent, R.; van Eeden, S.F. Particulate air pollution induces progression of atherosclerosis. J. Am. Coll. Cardiol. 2002, 39, 935–942. [Google Scholar] [CrossRef]
- Fujii, T.; Hayashi, S.; Hogg, J.C.; Mukae, H.; Suwa, T.; Goto, Y.; Vincent, R.; van Eeden, S.F. Interaction of alveolar macrophages and airway epithelial cells following exposure to particulate matter produces mediators that stimulate the bone marrow. Am. J. Respir. Cell Mol. Biol. 2002, 27, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D. You are what you breathe: Evidence linking air pollution and blood pressure. Curr. Hypertens. Rep. 2005, 7, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Brook, R.D.; Franklin, B.; Cascio, W.; Hong, Y.; Howard, G.; Lipsett, M.; Luepker, R.; Mittleman, M.; Samet, J.; Smith, S.C.; et al. Air pollution and cardiovascular disease: A statement for healthcare professionals from the Expert Panel on Population and Prevention Science of the American Heart Association. Circulation 2004, 109, 2655–2671. [Google Scholar] [CrossRef] [PubMed]
- Sharman, J.E.; Coombes, J.S.; Geraghty, D.P.; Fraser, D.I. Exposure to automotive pollution increases plasma susceptibility to oxidation. Arch. Environ. Health 2002, 57, 536–540. [Google Scholar] [CrossRef] [PubMed]
- Donaldson, K.; Stone, V.; Seaton, A.; MacNee, W. Ambient particle inhalation and the cardiovascular system: Potential mechanisms. Environ. Health Perspect. 2001, 109, 523–527. [Google Scholar] [CrossRef] [PubMed]
- Creason, J.; Neas, L.; Walsh, D.; Williams, R.; Sheldon, L.; Liao, D.; Shy, C. Particulate matter and heart rate variability among elderly retirees: The Baltimore 1998 PM study. J. Expo. Anal. Environ. Epidemiol. 2001, 11, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Kan, H.; London, S.J.; Chen, G.; Zhang, Y.; Song, G.; Zhao, N.; Jiang, L.; Chen, B. Season, sex, age, and education as modifiers of the effects of outdoor air pollution on daily mortality in Shanghai, China: The Public Health and Air Pollution in Asia (PAPA) Study. Environ. Health Perspect. 2008, 116, 1183–1188. [Google Scholar] [CrossRef] [PubMed]
- Zanobetti, A.; Schwartz, J.; Gold, D. Are there sensitive subgroups for the effects of airborne particles? Environ. Health Perspect. 2000, 108, 841–845. [Google Scholar] [CrossRef] [PubMed]
- Clougherty, J.E. A growing role for gender analysis in air pollution epidemiology. Environ. Health Perspect. 2010, 118, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Ciccone, M.M.; Bilianou, E.; Balbarini, A.; Gesualdo, M.; Ghiadoni, L.; Metra, M.; Palmiero, P.; Pedrinelli, R.; Salvetti, M.; Scicchitano, P.; et al. Task force on: “Early markers of atherosclerosis: Influence of age and sex”. J. Cardiovasc. Med. 2013, 14, 757–766. [Google Scholar] [CrossRef] [PubMed]
- Sexton, K.; Gong, H., Jr.; Bailar, J.C., III; Ford, J.G.; Gold, D.R.; Lambert, W.E.; Utell, M.J. Air pollution health risks: Do class and race matter? Toxicol. Ind. Health 1993, 9, 843–878. [Google Scholar] [PubMed]
- Rotko, T.; Kousa, A.; Alm, S.; Jantunen, M. Exposures to nitrogen dioxide in EXPOLIS-Helsinki: Microenvironment, behavioral and sociodemographic factors. J. Expo. Anal. Environ. Epidemiol. 2001, 11, 216–223. [Google Scholar] [CrossRef] [PubMed]
- Rotko, T.; Koistinen, K.; Hänninen, O.; Jantunen, M. Sociodemographic descriptors of personal exposure to fine particles (PM2.5) in EXPOLIS Helsinki. J. Expo. Anal. Environ. Epidemiol. 2000, 10, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Romieu, I.; Téllez-Rojo, M.M.; Lazo, M.; Manzano-Patiño, A.; Cortez-Lugo, M.; Julien, P.; Bélanger, M.C.; Hernandez-Avila, M.; Holguin, F. Omega-3 fatty acid prevents heart rate variability reductions associated with particulate matter. Am. J. Respir. Crit. Care Med. 2005, 172, 1534–1540. [Google Scholar] [CrossRef] [PubMed]
- Goto, Y.; Hogg, J.C.; Shih, C.H.; Ishii, H.; Vincent, R.; van Eeden, S.F. Exposure to ambient particles accelerates monocyte release from bone marrow in atherosclerotic rabbits. Am. J. Physiol. Lung Cell. Mol. Physiol. 2004, 287, L79–L85. [Google Scholar] [CrossRef] [PubMed]
- Wiegman, A. Efficacy and safety of statin therapy in children with familial hypercholesterolemia: A randomized controlled trial. JAMA 2004, 292, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Wittekoek, M.E.; de Groot, E.; Prins, M.H.; Trip, M.D.; Büller, H.R.; Kastelein, J.J. Differences in intima-media thickness in the carotid and femoral arteries in familial hypercholesterolemic heterozygotes with and without clinical manifestations of cardiovascular disease. Atherosclerosis 1999, 146, 271–279. [Google Scholar] [CrossRef]
- Zhu, Y.; Hinds, W.C.; Kim, S.; Sioutas, C. Concentration and size distribution of ultrafine particles near a major highway. J. Air Waste Manag. Assoc. 2002, 52, 1032–1042. [Google Scholar] [CrossRef] [PubMed]
- Painschab, M.S.; Davila-Roman, V.G.; Gilman, R.H.; Vasquez-Villar, A.D.; Pollard, S.L.; Wise, R.A.; Miranda, J.J.; Checkley, W.; CRONICAS Cohort Study Group. Chronic exposure to biomass fuel is associated with increased carotid artery intima-media thickness and a higher prevalence of atherosclerotic plaque. Heart 2013, 99, 984–991. [Google Scholar] [CrossRef] [PubMed]
- Rivera, M.; Basagaña, X.; Aguilera, I.; Foraster, M.; Agis, D.; de Groot, E.; Perez, L.; Mendez, M.A.; Bouso, L.; Targa, J.; et al. Association between long-term exposure to traffic-related air pollution and subclinical atherosclerosis: The REGICOR study. Environ. Health Perspect. 2013, 121, 223–230. [Google Scholar] [PubMed]
- Armijos, R.X.; Weigel, M.M.; Myers, O.B.; Li, W.W.; Racines, M.; Berwick, M. Residential exposure to urban traffic is associated with increased carotid intima-media thickness in children. J. Environ. Public Health 2015. [Google Scholar] [CrossRef] [PubMed]
- Bassett, C.M.; McCullough, R.S.; Edel, A.L.; Maddaford, T.G.; Dibrov, E.; Blackwood, D.P.; Austria, J.A.; Pierce, G.N. Trans-fatty acids in the diet stimulate atherosclerosis. Metabolism 2009, 58, 1802–1808. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, X.; Lian, H.; Ruan, Y.; Liang, R.; Zhao, X.; Routledge, M.; Fan, Z. Association of Exposure to Particular Matter and Carotid Intima-Media Thickness: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2015, 12, 12924-12940. https://doi.org/10.3390/ijerph121012924
Liu X, Lian H, Ruan Y, Liang R, Zhao X, Routledge M, Fan Z. Association of Exposure to Particular Matter and Carotid Intima-Media Thickness: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2015; 12(10):12924-12940. https://doi.org/10.3390/ijerph121012924
Chicago/Turabian StyleLiu, Xiaole, Hui Lian, Yanping Ruan, Ruijuan Liang, Xiaoyi Zhao, Michael Routledge, and Zhongjie Fan. 2015. "Association of Exposure to Particular Matter and Carotid Intima-Media Thickness: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 12, no. 10: 12924-12940. https://doi.org/10.3390/ijerph121012924
APA StyleLiu, X., Lian, H., Ruan, Y., Liang, R., Zhao, X., Routledge, M., & Fan, Z. (2015). Association of Exposure to Particular Matter and Carotid Intima-Media Thickness: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health, 12(10), 12924-12940. https://doi.org/10.3390/ijerph121012924