Clinical and Metabolic Parameters in Non-Small Cell Lung Carcinoma and Colorectal Cancer Patients with and without KRAS Mutations

Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Comparison of the clinical and metabolic parameters in patients with and without KRAS mutations
3.2. Comparison of the clinical and metabolic parameters in patients with different types of KRAS mutations
3.3. Comparison of the clinical and metabolic parameters in NSCLC and CRC patients with the same KRAS mutational status
3.4. Comparison of the clinical and metabolic parameters in NSCLC and CRC patients with the same KRAS mutation type
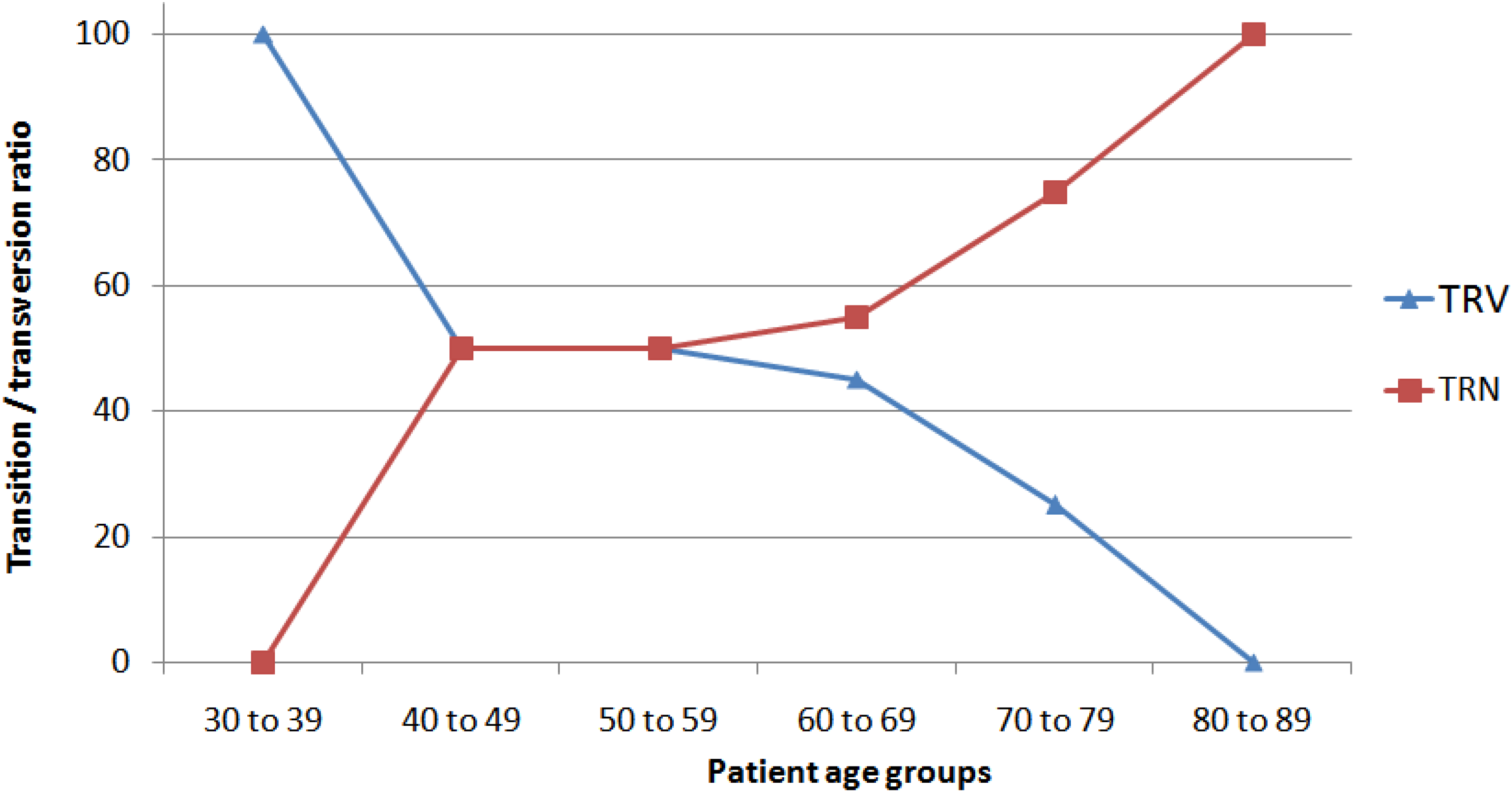
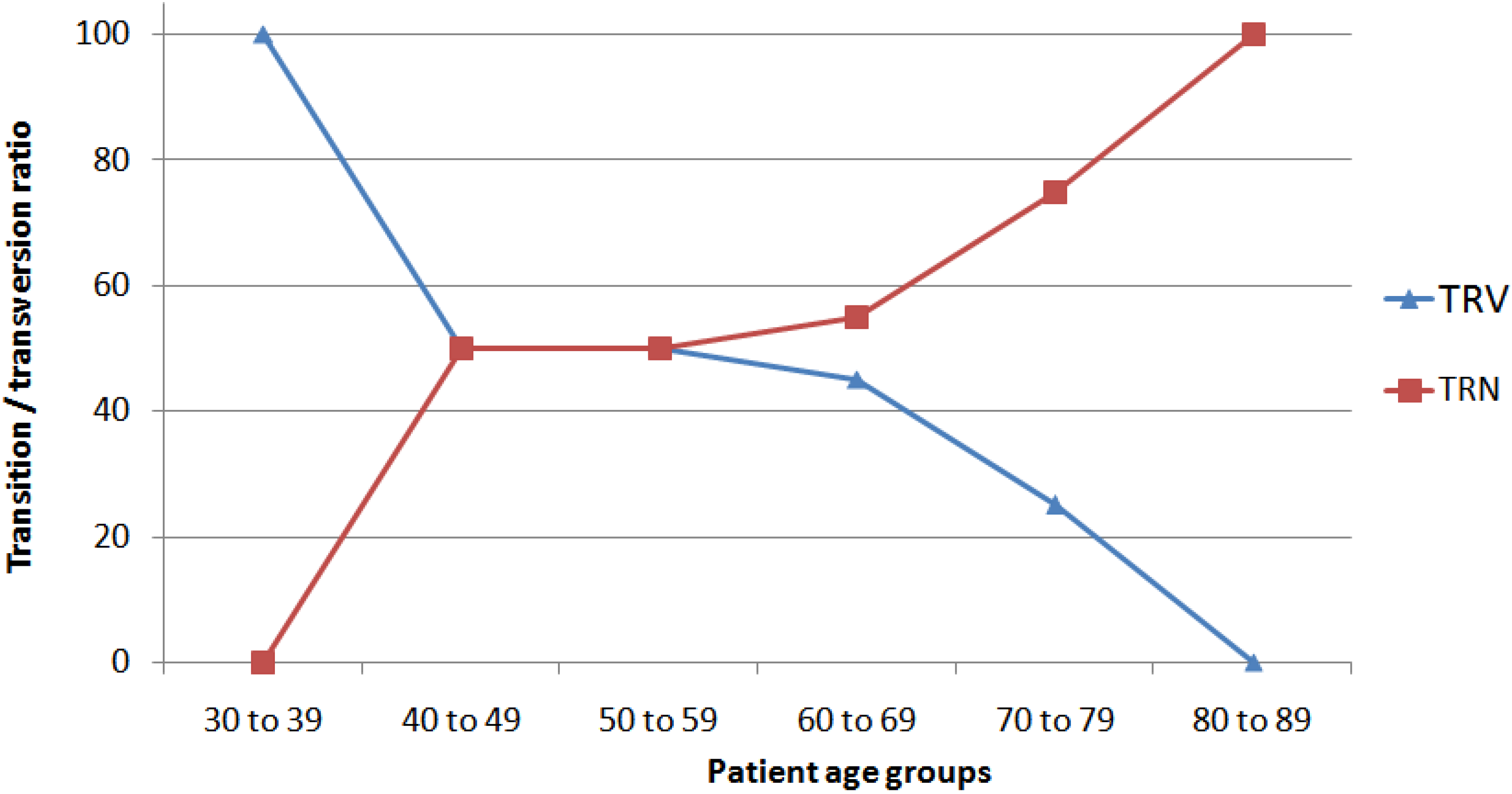
3.5. Nucleotide and amino acid changes in the NSCLC and CRC patients with KRAS mutations

{kind=link}
| Variables | NLSCS | CRC | ||||
|---|---|---|---|---|---|---|
| MUT a | WT a | P | MUT a | WT a | P | |
| Patients | 52 | 56 | 56 | 60 | ||
| Average age (SD), years | 61.0 (8.9) | 62.0 (11.6) | 0.34 | 56.89 (11.7) | 56.1 (12.0) | 0.36 |
| Male gender | 26/51 (51.0) | 29/56 (51.8) | 0.93 | 25/56 (44.6) | 36/60 (60.0) | 0.10 |
| Younger than 60 years of age b | 14/32 (43.8) | 14/42 (33.3) | 0.37 | 30/56(53.6) | 34/60 (56.7) | 0.74 |
| Smoker | 44/48 (91.7) | 36/52 (69.2) | <0.001 * | 25/56 (44.6) | 25/59 (42.4) | 0.81 |
| Consumes alcohol | 12/47 (25.5) | 7/46 (15.2) | 0.23 | 9/56 (16.1) | 12/59 (20.3) | 0.56 |
| Diabetic | 8/47 (17.0) | 7/46 (15.2) | 0.82 | 10/56 (17.9) | 9/60 (15.0) | 0.69 |
| Dyslipidemia present | 20/47 (42.6) | 14/46 (30.4) | 0.23 | 9/56 (16.1) | 13/60 (21.7) | 0.46 |
| Hypertension present | 32/48 (66.7) | 26/47 (55.3) | 0.27 | 26/56 (46.4) | 26/60 (43.3) | 0.75 |
| Individual cancer history present | 6/47 (12.8) | 5/46 (10.9) | 0.79 | 2/56 (3.6) | 5/59 (8.5) | 0.30 |
| Family cancer history present | 33/47 (70.2) | 26/46 (56.5) | 0.18 | 28/56 (50.0) | 32/60 (53.3) | 0.72 |
| Variables | NSCLC | CRC | ||||
|---|---|---|---|---|---|---|
| TRN a | TRV a | P | TRN a | TRV a | P | |
| Patients | 14 | 38 | 29 | 27 | ||
| Average age (SD), years | 62.1 (9.6) | 60.5 (8.6) | 0.32 | 61.03 (11.0) | 52.4 (10.9) | <0.01 * |
| Male gender | 10/14 (71.4) | 16/37 (43.2) | 0.08 | 12/29 (41.4) | 13/27 (48.1) | 0.62 |
| Younger than 60 years of age b | 6/11 (54.5) | 8/21 (38.1) | 0.39 | 13/29 (44.8) | 17/27 (63.0) | 0.19 |
| Smoker | 10/12 (83.3) | 34/36 (94.4) | 0.28 | 17/29 (58.6) | 13/27 (48.1) | 0.45 |
| Consumes alcohol | 5/14 (35.7) | 7/33 (21.2) | 0.32 | 4/29 (13.8) | 5/27 (18.5) | 0.64 |
| Diabetic | 1/14 (7.1) | 7/33 (21.2) | 0.27 | 5/29 (17.2) | 5/27 (18.5) | 0.91 |
| Dyslipidemia present | 7/14 (50.0) | 13/33 (39.4) | 0.51 | 6/29 (20.7) | 3/27 (11.1) | 0.35 |
| Hypertension present | 11/14 (78.8) | 21/34 (61.8) | 0.28 | 16/29 (55.2) | 10/27 (37.0) | 0.18 |
| Individual cancer history present | 1/14 (7.1) | 5/33 (15.1) | 0.49 | 1/29 (3.4) | 1/27 (3.7) | 0.97 |
| Family cancer history present | 11/14 (78.5) | 22/33 (66.7) | 0.43 | 16/29 (55.2) | 12/27 (44.4) | 0.44 |
| Variables | KRAS Mutant | KRAS Wild Type | ||||
|---|---|---|---|---|---|---|
| NSCLC a | CRC a | P | NSCLC a | CRC a | P | |
| Patients | 52 | 56 | 56 | 60 | ||
| Average age (SD), years | 61.0 (8.9) | 56.89 (11.7) | 0.04 * | 62.0 (11.6) | 56.1 (12.0) | <0.001 * |
| Male | 26/51 (51.0) | 25/56 (44.6) | 0.53 | 29/56 (51.8) | 36/60 (60.0) | 0.38 |
| Younger than 60 years of age b | 14/32 (43.8) | 30/56 (53.6) | 0.40 | 14/42 (33.3) | 34/60 (56.7) | 0.02 * |
| Smoker | 44/48 (91.7) | 25/56 (44.6) | <0.01 * | 36/52 (69.2) | 25/59 (42.4) | <0.01 * |
| Consumes alcohol | 12/47 (25.5) | 9/56 (16.1) | 0.25 | 7/46 (15.2) | 12/59 (20.3) | 0.51 |
| Diabetic | 8/47 (17.0) | 10/56 (17.9) | 0.91 | 7/46 (15.2) | 9/60 (15.0) | 0.98 |
| Dyslipidemia present | 20/47 (42.6) | 9/56 (16.1) | <0.01 * | 14/46 (30.4) | 13/60 (21.7) | 0.31 |
| Hypertension present | 32/48 (66.7) | 26/56 (46.4) | 0.04 * | 26/47 (55.3) | 26/60 (43.3) | 0.23 |
| Individual cancer history present | 6/47 (12.8) | 2/56 (3.6) | 0.10 | 5/46 (10.9) | 5/59 (8.5) | 0.69 |
| Family cancer history present | 33/47 (70.2) | 28/56 (50.0) | 0.04 * | 26/46 (56.5) | 32/60 (53.3) | 0.76 |
| Variables | Transition(s) in KRAS Present | Transversion(s) in KRAS Present | ||||
|---|---|---|---|---|---|---|
| NSCLC a | CRC a | P | NSCLC a | CRC a | P | |
| Patients | 14 | 29 | 38 | 27 | ||
| Average age (SD), years | 62.1 (9.6) | 61.03 (11.0) | 0.39 | 60.5 (8.6) | 52.4 (10.9) | <0.001 * |
| Male gender | 10/14 (71.4) | 12/29 (41.4) | 0.07 | 16/37 (43.2) | 13/27 (48.1) | 0.72 |
| Younger than 60 years of age b | 6/11 (54.5) | 13/29 (44.8) | 0.59 | 8/21 (38.1) | 17/27 (63.0) | 0.12 |
| Smoker | 10/12 (83.3) | 17/29 (58.6) | 0.15 | 34/36 (94.4) | 13/27 (48.1) | <0.01 * |
| Consumes alcohol | 5/14 (35.7) | 4/29 (13.8) | 0.13 | 7/33 (21.2) | 5/27 (18.5) | 0.81 |
| Diabetic | 1/14 (7.1) | 5/29 (17.2) | 0.40 | 7/33 (21.2) | 5/27 (18.5) | 0.81 |
| Dyslipidemia present | 7/14 (50.0) | 6/29 (20.7) | 0.06 | 13/33 (39.4) | 3/27 (11.1) | 0.02 * |
| Hypertension present | 11/14 (78.8) | 16/29 (55.2) | 0.15 | 21/34 (61.8) | 10/27 (37.0) | 0.06 |
| Individual cancer history present | 1/14 (7.1) | 1/29 (3.4) | 0.66 | 5/33 (15.1) | 1/27 (3.7) | 0.17 |
| Family cancer history present | 11/14 (78.5) | 16/29 (55.2) | 0.15 | 22/33 (66.7) | 12/27 (44.4) | 0.09 |
| Type of KRAS Mutation a | NSCLC b | CRC b | P |
|---|---|---|---|
| c.34 G>T transversion (G12C) | 22 (57.9) | 7 (25.9) | 0.04 c |
| c.34 G>C transversion (G12R) | 1 (2.6) | 2 (7.4) | |
| c.35 G>T transversion (G12V) | 9 (23.7) | 14 (51.9) | |
| c.35 G>C transversion (G12A) | 3 (7.9) | 3 (11.1) | |
| c.37 G>T transversion (G13C) | 3 (7.9) | 1 (3.7) | |
| c.34 G>A transition (G12S) | 1 (7.1) | 4 (13.8) | 0.44 d |
| c.35 G>A transition (G12D) | 11 (78.6) | 17 (58.6) | |
| c.38 G>A transition (G13D) | 2 (14.3) | 8 (27.6) | |
| Total transversions | 38 (73.1) | 27 (48.2) | <0.01 *,e |
| Total transitions | 14 (26.9) | 29 (51.8) | |
| TOTAL | 52 (100) | 56 (100) |
4. Discussion
4.1. Comparison of the clinical and metabolic parameters in patients with and without KRAS mutations
4.2. Comparison of the clinical and metabolic parameters in patients with different types of KRAS mutations
4.3. Comparison of the clinical and metabolic parameters in NSCLC and CRC patients with the same KRAS mutational status
4.4. Comparison of the clinical and metabolic parameters in NSCLC and CRC patients with the same KRAS mutation type
4.5. Nucleotide and amino acid changes in NSCLC and CRC patients with KRAS mutations
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Parkin, D.M.; Bray, F.; Ferlay, J.; Piasni, P. Estimating the world cancer burden: Globocan 2000. Int J. Cancer 2001, 94, 153–156. [Google Scholar] [CrossRef] [PubMed]
- Einspahr, J.G.; Martinez, M.E.; Jiang, R.; Hsu, C.H.; Rashid, A.; Bhattacharrya, A.K.; Ahnen, D.J.; Jacobs, E.T.; Houlihan, P.S.; Webb, C.R.; et al. Associations of Ki-ras proto-oncogene mutation and p53 gene overexpression in sporadic colorectal adenomas with demographic and clinicopathologic characteristics. Cancer Epidemiol. Biomarkers Prev. 2006, 15, 1443–1450. [Google Scholar] [CrossRef] [PubMed]
- Cheng, Y.D.; Yang, H.; Chen, G.Q.; Zhang, Z.C. Molecularly targeted drugs for metastatic colorectal cancer. Drug Des. Dev. Ther. 2013, 7, 1315–1322. [Google Scholar]
- De Mello, R.A.; Madureira, P.; Carvalho, L.S.; Araújo, A.; O'Brien, M.; Popat, S. EGFR and KRAS mutations, and ALKfusions: Current developments and personalized therapies for patients with advanced non-small-cell lung cancer. Pharmacogenomics 2013, 14, 1765–1777. [Google Scholar]
- Riely, G.J.; Marks, J.; Pao, W. KRAS mutations in non-small cell lung cancer. Proc. Amer. Thorac. Soc. 2009, 6, 201–205. [Google Scholar] [CrossRef]
- Amado, R.G.; Wolf, M.; Peeters, M.; van Cutsem, E.; Siena, S.; Freeman, D.J.; Juan, T.; Sikorski, R.; Suggs, S.; Radinsky, R.; et al. Wild-type KRAS is required for panitumumab efficacy in patients with metastatic colorectal cancer. J. Clin. Oncol. 2008, 26, 1626–1634. [Google Scholar] [CrossRef] [PubMed]
- Cagnol, S.; Rivard, N. Oncogenic KRAS and BRAF activation of the MEK/ERK signaling pathway promotes expression of dual-specificity phosphatase 4 (DUSP4/MKP2) resulting in nuclear ERK1/2 inhibition. Oncogene 2013, 32, 564–576. [Google Scholar] [CrossRef] [PubMed]
- Orecchia, R.; Infusini, E.; Sciutto, A.; Rapallo, A.; di Vinci, A.; Nigro, S.; Geido, E.; Giaretti, W. Ki-ras activation in vitro affects G1 and G2M cell-cycle transit times and apoptosis. J. Pathol. 2000, 190, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Heinemann, V.; Stintzing, S.; Kirchner, T.; Boeck, S.; Jung, A. Clinical relevance of EGFR- and KRAS-status in colorectal cancer patients treated with monoclonal antibodies directed against the EGFR. Cancer Treat. Rev. 2009, 35, 262–271. [Google Scholar] [CrossRef] [PubMed]
- Cushman-Vokoun, A.M.; Stover, D.G.; Zhao, Z.; Koehler, E.A.; Berlin, J.D.; Vnencak-Jones, C.L. Clinical utility of KRAS and BRAF mutations in a cohort of patients with colorectal neoplasms submitted for microsatellite instability testing. Clin. Colorectal Cancer 2013, 12, 168–178. [Google Scholar]
- Westra, W.H.; Slebos, R.J.; Offerhaus, G.J.; Goodman, S.N.; Evers, S.G.; Kensler, T.W.; Askin, F.B.; Rodenhuis, S.; Hruban, R.H. K-ras oncogene activation in lung adenocarcinomas from former smokers. Evidence that K-ras mutations are an early and irreversible event in the development of adenocarcinoma of the lung. Cancer 1993, 72, 432–438. [Google Scholar]
- Gilsing, A.M.; Fransen, F.; de Kok, T.M.; Goldbohm, A.R.; Schouten, L.J.; de Bruïne, A.P.; van Engeland, M.; van den Brandt, P.A.; de Goeij, A.F.; Weijenberg, M.P. Dietary heme iron and the risk of colorectal cancer with specific mutations in KRAS and APC. Carcinogenesis 2013, 34, 2757–2766. [Google Scholar] [CrossRef] [PubMed]
- Slagter, S.N.; Vliet-Ostaptchouk, J.V.; Vonk, J.M.; Boezen, H.M.; Dullaart, R.P.; Kobold, A.C.; Feskens, E.J.; van Beek, A.P.; van der Klauw, M.M.; Wolffenbuttel, B.H. Associations between smoking, components of metabolic syndrome and lipoprotein particle size. BMC Med. 2013, 11. [Google Scholar] [CrossRef]
- Gerber, D.E. Maintenance therapy for advanced lung cancer: Who, what, and when? J. Clin. Oncol. 2013, 31, 2983–2990. [Google Scholar] [CrossRef]
- Doménech, E.; Gómez-López, G.; Gzlez-Peña, D.; López, M.; Herreros, B.; Menezes, J.; Gómez-Lozano, N.; Carro, A.; Graña, O.; Pisano, D.G.; et al. New mutations in chronic lymphocytic leukemia identified by target enrichment and deep sequencing. PLoS One 2012, 7. [Google Scholar] [CrossRef]
- Langer, R.; Becker, K.; Feith, M.; Friess, H.; Höfler, H.; Keller, G. Genetic aberrations in primary esophageal melanomas: Molecular analysis of c-KIT, PDGFR, KRAS, NRAS and BRAF in a series of 10 cases. Mod. Pathol. 2011, 24, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Oki, E.; Zhao, Y.; Yoshida, R.; Egashira, A.; Ohgaki, K.; Morita, M.; Kakeji, Y.; Maehara, Y. The difference in p53 mutations between cancers of the upper and lower gastrointestinal tract. Digestion 2009, 79, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Riely, G.J.; Kris, M.G.; Rosenbaum, D.; Marks, J.; Li, A.; Chitale, D.A.; Nafa, K.; Riedel, E.R.; Hsu, M.; Pao, W. Frequency and distinctive spectrum of KRAS mutations in never smokers with lung adenocarcinoma. Clin. Cancer Res. 2008, 14, 5731–5734. [Google Scholar] [CrossRef] [PubMed]
- Esteller, M.; Risques, R.A.; Toyota, M.; Capella, G.; Moreno, V.; Peinado, M.A.; Baylin, S.B.; Herman, J.G. Promoter hypermethylation of the DNA repair gene O(6)-methylguanine-DNA methyltransferase is associated with the presence of G:C to A:T transition mutations in p53 in human colorectal tumorigenesis. Cancer Res. 2001, 61, 4689–4692. [Google Scholar] [PubMed]
- Shen, L.; Kondo, Y.; Rosner, G.L.; Xiao, L.; Hernandez, N.S.; Vilaythong, J.; Houlihan, P.S.; Krouse, R.S.; Prasad, A.R.; Einspahr, J.G. MGMT promoter methylation and field defect in sporadic colorectal cancer. J. Natl. Cancer. Inst. 2005, 97, 1330–1338. [Google Scholar] [CrossRef] [PubMed]
- Bazan, V.; Migliavacca, M.; Zanna, I.; Tubiolo, C.; Grassi, N.; Latteri, M.A.; La Farina, M.; Albanese, I.; Dardanoni, G.; Salerno, S.; et al. Specific codon 13 K-ras mutations are predictive of clinical outcome in colorectal cancer patients, whereas codon 12 K-ras mutations are associated with mucinous histotype. Ann. Oncol. 2002, 13, 1438–1446. [Google Scholar]
- Minamoto, T.; Mai, M.; Ronai, Z. K-ras mutation: Early detection in molecular diagnosis and risk assessment of colorectal, pancreas, and lung cancers—A review. Cancer Detect. Prev. 2000, 24, 1–12. [Google Scholar] [PubMed]
- Span, M.; Moerkerk, P.T.; De Goeij, A.F.; Arends, J.W. A detailed analysis of K-ras point mutations in relation to tumor progression and survival in colorectal cancer patients. Int. J. Cancer 1996, 69, 241–245. [Google Scholar] [PubMed]
- Poehlmann, A.; Kuester, D.; Meyer, F.; Lippert, H.; Roessner, A.; Schneider-Stock, R. K-ras mutation detection in colorectal cancer using the Pyrosequencing technique. Pathol. Res. Pract. 2007, 203, 489–497. [Google Scholar] [CrossRef] [PubMed]
- Scartozzi, M.; Galizia, E.; Chiorrini, S.; Giampieri, R.; Berardi, R.; Pierantoni, C.; Cascinu, S. Arterial hypertension correlates with clinical outcome in colorectal cancer patients treated with first-line bevacizumab. Ann. Oncol. 2009, 20, 227–230. [Google Scholar] [CrossRef] [PubMed]
- Van Kruijsdijk, R.C.; van der Graaf, Y.; Peeters, P.H.; Visseren, F.L. Second Manifestations of ARTerial Disease (SMART) Study Group. Cancer risk in patients with manifest vascular disease: Effects of smoking, obesity, and metabolic syndrome. Cancer Epidemiol. Biomarkers Prev. 2013, 22, 1267–1277. [Google Scholar]
- Gao, J.; Zhang, J.; Lu, T.; Li, X.Y.; Jia, N.; Liang, Z.Y. Correlation between KRAS mutations and clinicopathologic features in colorectal carcinomas. Zhonghua Bing Li Xue Za Zhi 2012, 41, 595–598. [Google Scholar] [PubMed]
- Roa, I.; Sánchez, T.; Majlis, A.; Schalper, K. KRAS gene mutation in colorectal cancer. Rev. Med. Chil. 2013, 141, 1166–1172. [Google Scholar] [CrossRef] [PubMed]
- Bacchi, C.E.; Ciol, H.; Queiroga, E.M.; Benine, L.C.; Silva, L.H.; Ojopi, E.B. Epidermal growth factor receptor and KRAS mutations in Brazilian lung cancer patients. Clinics 2012, 67, 419–424. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; He, J.; Yang, H.; Luo, X.; Liang, Z.; Chen, J.; Cai, Z.; Xu, J.; Ren-Heidenreich, L. Somatic mutation analysis of EGFR, KRAS, BRAF and PIK3CA in 861 patients with non-small cell lung cancer. Cancer Biomark. 2012, 10, 63–69. [Google Scholar]
- Warth, A.; Penzel, R.; Lindenmaier, H.; Brandt, R.; Stenzinger, A.; Herpel, E.; Goeppert, B.; Thomas, M.; Herth, F.J.; Dienemann, H.; et al. EGFR, KRAS, BRAF and ALK gene alterations in lung adenocarcinomas: Patient outcome, interplay with morphology and immunophenotype. Eur. Respir. J. 2014, 43, 872–883. [Google Scholar] [CrossRef] [PubMed]
- Li, S.; Li, L.; Zhu, Y.; Huang, C.; Qin, Y.; Liu, H.; Ren-Heidenreich, L.; Shi, B.; Ren, H.; Chu, X.; et al. Coexistence of EGFR with KRAS, or BRAF, or PIK3CA somatic mutations in lung cancer: A comprehensive mutation profiling from 5125 Chinese cohorts. Brit. J. Cancer 2014, 110, 2812–2820. [Google Scholar] [CrossRef] [PubMed]
- Takamochi, K.; Oh, S.; Suzuki, K. Differences in EGFR and KRAS mutation spectra in lung adenocarcinoma of never and heavy smokers. Oncol. Lett. 2013, 6, 1207–1212. [Google Scholar] [PubMed]
- Raparia, K.; Villa, C.; Raj, R.; Cagle, P.T. Peripheral lung adenocarcinomas with KRAS mutations are more likely to invade visceral pleura. Arch. Pathol. Lab. Med. 2014, in press. [Google Scholar]
- Saito, N.; Tomita, S.; Ichikawa, K.; Mitomi, H.; Imura, J.; Fujimori, T. Analysis of KRAS mutations in cases of metastatic colorectal cancer at a single institution in Tochigi, Japan. Pathobiology 2014, 81, 133–137. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, C.G.; Aran, V.; Zalcberg-Renault, I.; Victorino, A.P.; Salem, J.H.; Bonamino, M.H.; Vieira, F.M.; Zalis, M. KRAS mutations: Variable incidences in a Brazilian cohort of 8234 metastatic colorectal cancer patients. BMC Gastroenterol. 2014, 14. [Google Scholar] [CrossRef]
- Cserepes, M.; Ostoros, G.; Lohinai, Z.; Raso, E.; Barbai, T.; Timar, J.; Rozsas, A.; Moldvay, J.; Kovalszky, I.; Fabian, K.; et al. Subtype-specific KRAS mutations in advanced lung adenocarcinoma: A retrospective study of patients treated with platinum-based chemotherapy. Eur. J. Cancer 2014, 50, 1819–1828. [Google Scholar] [CrossRef] [PubMed]
- Weijenberg, M.P.; Aardening, P.W.; de Kok, T.M.; de Goeij, A.F.; van den Brandt, P.A. Cigarette smoking and KRAS oncogene mutations in sporadic colorectal cancer: Results from the Netherlands Cohort Study. Mutat. Res. 2008, 652, 54–64. [Google Scholar] [CrossRef] [PubMed]
- Samadder, N.J.; Vierkant, R.A.; Tillmans, L.S.; Wang, A.H.; Lynch, C.F.; Anderson, K.E.; French, A.J.; Haile, R.W.; Harnack, L.J.; Potter, J.D. Cigarette smoking and colorectal cancer risk by KRAS mutation status among older women. Amer. J. Gastroenterol. 2012, 107, 782–789. [Google Scholar] [CrossRef]
- Martinez, F.; Fernández-Martos, C.; Quintana, M.J.; Castells, A.; Llombart, A.; Iniguez, F.; Guillem, V.; Dasí, F. APC and KRAS mutations in distal colorectal polyps are related to smoking habits in men: Results of a cross-sectional study. Clin. Transl. Oncol. 2011, 9, 664–671. [Google Scholar] [CrossRef]
- Sinha, R.; Hussain, S.; Mehrotra, R.; Kumar, R.S.; Kumar, K.; Pande, P.; Doval, D.C.; Basir, S.F.; Bharadwaj, M. Kras gene mutation and RASSF1A, FHIT and MGMT gene promoter hypermethylation: Indicators of tumor staging and metastasis in adenocarcinomatous sporadic colorectal cancer in Indian population. PLoS One 2013. [Google Scholar] [CrossRef]
- Aissi, S.; Buisine, M.P.; Zerimech, F.; Kourda, N.; Moussa, A.; Manai, M.; Porchet, N. Somatic molecular changes and histo-pathological features of colorectal cancer in Tunisia. World J. Gastroenterol. 2013, 19, 5286–5294. [Google Scholar] [CrossRef] [PubMed]
- Okudela, K.; Woo, T.; Yazawa, T.; Ogawa, N.; Tajiri, M.; Masuda, M.; Kitamura, H. Significant association between EGFR-mutated lung adenocarcinoma and past illness from gastric cancer or uterine myoma: Its implication in carcinogenesis. Lung Cancer 2009, 66, 287–291. [Google Scholar] [CrossRef] [PubMed]
- Bello, M.J.; Alonso, M.E.; Amiñoso, C.; Anselmo, N.P.; Arjona, D.; Gonzalez-Gomez, P.; Lopez-Marin, I.; de Campos, J.M.; Gutierrez, M.; Isla, A. Hypermethylation of the DNA repair gene MGMT: Association with TP53 G:C to A:T transitions in a series of 469 nervous system tumors. Mutat. Res. 2004, 554, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Milner, J.A. Dietary modulation of colon cancer risk. J. Nutr. 2007, 137, S2576–S2579. [Google Scholar]
- Maus, M.K.; Grimminger, P.P.; Mack, P.C.; Astrow, S.H.; Stephens, C.; Zeger, G.; Hsiang, J.; Brabender, J.; Friedrich, M.; Alakus, H.; et al. KRAS mutations in non-small-cell lung cancer and colorectal cancer: Implications for EGFR-targeted therapies. Lung Cancer 2014, 83, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.Y.; Lin, K.D.; Hsiao, P.J.; Shin, S.J. The association of diabetes mellitus with liver, colon, lung, and prostate cancer is independent of hypertension, hyperlipidemia, and gout in Taiwanese patients. Metabolism 2012, 61, 242–249. [Google Scholar] [CrossRef] [PubMed]
- Inoue, M.; Noda, M.; Kurahashi, N.; Iwasaki, M.; Sasazuki, S.; Iso, H.; Tsugane, S.; Japan Public Health Center-Based Prospective Study Group. Impact of metabolic factors on subsequent cancer risk: Results from a large-scale population-based cohort study in Japan. Eur. J. Cancer Prev. 2009, 18, 240–247. [Google Scholar]
- Sturmer, T.; Buring, J.E.; Lee, I.M.; Gaziano, J.M.; Glynn, R.J. Metabolic abnormalities and risk for colorectal cancer in the physicians’ health study. Cancer Epidemiol Biomarkers Prev. 2006, 15, 2391–2397. [Google Scholar] [CrossRef] [PubMed]
- Tsilidis, K.K.; Brancati, F.L.; Pollak, M.N.; Rifai, N.; Clipp, S.L.; Hoffman-Bolton, J.; Helzlsouer, K.J.; Platz, E.A. Metabolic syndrome components and colorectal adenoma in the CLUE II cohort. Cancer Causes Control 2010, 21, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Mauldin, P.D.; Ebeling, M.; Hulsey, T.C.; Liu, B.; Thomas, M.B.; Camp, E.R.; Esnaola, N.F. Effect of metabolic syndrome and its components on recurrence and survival in colon cancer patients. Cancer 2013, 119, 1512–1520. [Google Scholar] [CrossRef] [PubMed]
- Porta, M.; Crous-Bou, M.; Wark, P.A.; Vineis, P.; Real, F.X.; Malats, N.; Kampman, E. Cigarette smoking and K-ras mutations in pancreas, lung and colorectal adenocarcinomas: Etiopathogenic similarities, differences and paradoxes. Mutat. Res. 2009, 682, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Dogan, S.; Shen, R.; Ang, D.C.; Johnson, M.L.; D'Angelo, S.P.; Paik, P.K.; Brzostowski, E.B.; Riely, G.J.; Kris, M.G.; Zakowski, M.F. Molecular epidemiology of EGFR and KRAS mutations in 3026 lung adenocarcinomas: Higher susceptibility of women to smoking-related KRAS-mutant cancers. Clin. Cancer Res. 2012, 18, 6169–6177. [Google Scholar] [CrossRef] [PubMed]
- Bruera, G.; Cannita, K.; di Giacomo, D.; Lamy, A.; Frébourg, T.; Sabourin, J.C.; Tosi, M.; Alesse, E.; Ficorella, C.; Ricevuto, E. Worse prognosis of KRAS c.35 G>A mutant metastatic colorectal cancer (MCRC) patients treated with intensive triplet chemotherapy plus bevacizumab (FIr-B/FOx). BMC Med. 2013, 11. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Yilmaz, A.; Mohamed, N.; Patterson, K.A.; Tang, Y.; Shilo, K.; Villalona-Calero, M.A.; Davis, M.E.; Zhou, X.-P.; Frankel, W.; Otterson, G.A.; et al. Clinical and Metabolic Parameters in Non-Small Cell Lung Carcinoma and Colorectal Cancer Patients with and without KRAS Mutations. Int. J. Environ. Res. Public Health 2014, 11, 8645-8660. https://doi.org/10.3390/ijerph110908645
Yilmaz A, Mohamed N, Patterson KA, Tang Y, Shilo K, Villalona-Calero MA, Davis ME, Zhou X-P, Frankel W, Otterson GA, et al. Clinical and Metabolic Parameters in Non-Small Cell Lung Carcinoma and Colorectal Cancer Patients with and without KRAS Mutations. International Journal of Environmental Research and Public Health. 2014; 11(9):8645-8660. https://doi.org/10.3390/ijerph110908645
Chicago/Turabian StyleYilmaz, Ahmet, Nehad Mohamed, Kara A. Patterson, Yan Tang, Konstantin Shilo, Miguel A. Villalona-Calero, Michael E. Davis, Xiao-Ping Zhou, Wendy Frankel, Gregory A. Otterson, and et al. 2014. "Clinical and Metabolic Parameters in Non-Small Cell Lung Carcinoma and Colorectal Cancer Patients with and without KRAS Mutations" International Journal of Environmental Research and Public Health 11, no. 9: 8645-8660. https://doi.org/10.3390/ijerph110908645
APA StyleYilmaz, A., Mohamed, N., Patterson, K. A., Tang, Y., Shilo, K., Villalona-Calero, M. A., Davis, M. E., Zhou, X.-P., Frankel, W., Otterson, G. A., & Zhao, W. (2014). Clinical and Metabolic Parameters in Non-Small Cell Lung Carcinoma and Colorectal Cancer Patients with and without KRAS Mutations. International Journal of Environmental Research and Public Health, 11(9), 8645-8660. https://doi.org/10.3390/ijerph110908645