A Health Impact Assessment of a Proposed Bill to Decrease Speed Limits on Local Roads in Massachusetts (U.S.A.)

Abstract
:1. Introduction
2. Methods
2.1. Decision-Makers and the Decision-Making Process
2.2. Stakeholder Engagement
2.3. Traffic Modeling
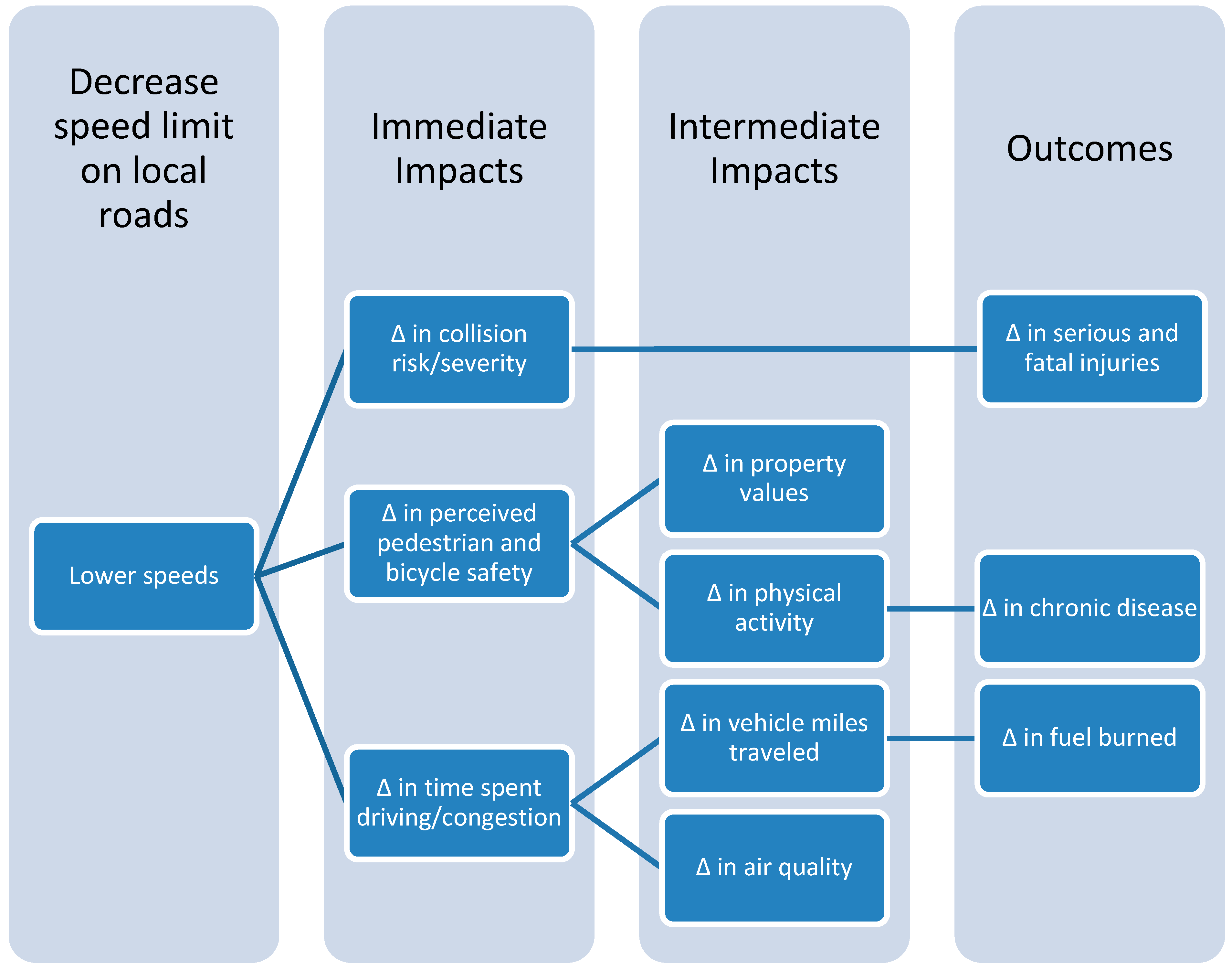
2.4. Pathways Linking Speed Limits and Health
- Collisions, injuries, and fatalities
- Fuel burned and time spent in traffic
- Health effects of air pollution
2.5. Assessment
2.5.1. Collisions, Fatalities, and Injuries
2.5.2. Cost of Collisions
- (1)
- injuries resulting in death, including deaths occurring within and outside a healthcare setting;
- (2)
- injuries resulting in hospitalization with survival to discharge; and (3) injuries requiring an ED visit not resulting in hospitalization.
2.5.3. Time Spent and Fuel Consumed in Traffic
Truck Fuel Economy = 1.4898 × ln(speed) – 0.2554
2.5.4. Air Pollution
2.5.5. Pedestrian and Bicyclist Perceptions of Safety
2.5.6. Parental Safety Perceptions and Children’s Levels of Physical Activity
2.5.7. Property Values
3. Results and Discussion
3.1. Results
3.1.1. Collisions, Fatalities, and Injuries

{kind=link}
{kind=link}
| Crash Type | 2006 | 2007 | 2008 | 2009 | Total | Annual Average |
|---|---|---|---|---|---|---|
| Crashes on All Roads | 124,274 | 120,667 | 120,970 | 111,192 | 477,103 | 119,276 |
| Crashes on Local Roads | 34,832 | 34,953 | 34,319 | 32,158 | 136,262 | 34,066 |
| Fatal Crashes on All Roads | 384 | 400 | 321 | 292 | 1397 | 349 |
| Fatal Crashes on Local Roads | 97 | 93 | 69 | 55 | 314 | 79 |
| Fatalities on All Roads | 410 | 426 | 345 | 316 | 1,497 | 374 |
| Fatalities on Local Roads | 101 | 100 | 71 | 59 | 331 | 83 |
| Injury Crashes on All Roads | 33,038 | 31,289 | 31,017 | 28,933 | 124,277 | 31,069 |
| Injury Crashes on Local Roads | 8543 | 8196 | 7845 | 7560 | 32,144 | 8,036 |
| Injuries on All Roads | 45,934 | 42,947 | 42,321 | 40,077 | 171,279 | 42,820 |
| Injuries on Local Roads | 11,991 | 11,334 | 10,741 | 10,514 | 44,580 | 11,145 |
| Crash Type | 2006 | 2007 | 2008 | 2009 | Total | Annual Average |
|---|---|---|---|---|---|---|
| Crashes on All Roads | 124,274 | 120,667 | 120,970 | 111,192 | 477,103 | 119,276 |
| Crashes on Local Roads | 34,832 | 34,953 | 34,319 | 32,158 | 136,262 | 34,066 |
| Crashes Involving Pedestrians on All Roads | 1577 | 1584 | 1765 | 1671 | 6597 | 1649 |
| Crashes Involving Pedestrians on Local Roads | 576 | 585 | 672 | 615 | 2,448 | 612 |
| Pedestrian Fatalities on All Roads | 58 | 65 | 72 | 46 | 241 | 60 |
| Pedestrian Fatalities on Local Roads | 19 | 15 | 28 | 13 | 75 | 19 |
| Pedestrian Injuries on All Roads | 1116 | 1192 | 1316 | 1331 | 4955 | 1239 |
| Pedestrian Injuries on Local Roads | 408 | 437 | 478 | 479 | 1802 | 451 |
| Crash Type | 2006 | 2007 | 2008 | 2009 | Total | Annual Average |
|---|---|---|---|---|---|---|
| Crashes on All Roads | 124,274 | 120,667 | 120,970 | 111,192 | 477,103 | 119,276 |
| Crashes on Local Roads | 34,832 | 34,953 | 34,319 | 32,158 | 136,262 | 34,066 |
| Crashes Involving Cyclists on All Roads | 1069 | 1069 | 1227 | 1248 | 4613 | 1153 |
| Crashes Involving Cyclists on Local Roads | 398 | 393 | 458 | 455 | 1704 | 426 |
| Cyclist Fatalities on All Roads | 6 | 11 | 10 | 6 | 33 | 8 |
| Cyclist Fatalities on Local Roads | 1 | 8 | 4 | 1 | 14 | 4 |
| Cyclist Injuries on All Roads | 753 | 744 | 866 | 882 | 3245 | 811 |
| Cyclist Injuries on Local Roads | 277 | 281 | 309 | 313 | 1180 | 295 |
| Estimated Annual Decrease in | 1.8 mph Speed Reduction Estimate (95% Confidence Interval) | 0.67 mph Speed Reduction Estimate (95% Confidence Interval) |
|---|---|---|
| Total Crashes | 2219 (286, 4042) | 811 (102, 1505) |
| Fatal Crashes | 15 (2, 27) | 6 (1, 11) |
| Injury Crashes | 772 (460, 1072) | 285 (168, 401) |
| Fatalities | 18 (−4, 35) | 7 (−1, 15) |
| Injured Road Users | 1239 (369, 2039) | 460 (133, 77) |
| Pedestrian Fatalities | 4 (−1, 8) | 2 (0, 3) |
| Cyclist Fatalities | 1 (0, 1) | 0.3 (−0.1, 0.6) |
| Injured Pedestrians | 50 (15, 82) | 19 (5, 31) |
| Injured Cyclists | 33 (10, 54) | 12 (4, 21) |
3.1.2. Cost of Collisions
| Outcome | Fatalities | Pedestrian Fatalities | Cyclist Fatalities |
| Annual Decrease in Deaths | 18 | 4 | 1 |
| Medical Cost Avoided | $346,721 | $76,699 | $18,912 |
| Work Loss Cost Avoided | $29,347,334 | $6,521,513 | $1,630,641 |
| Combined Cost Savings | $29,694,055 | $6,598,212 | $1,649,553 |
| Outcome | Injured Road Users | Injured Pedestrians | Injured Cyclists |
| Annual Decrease in Number Hospitalized | 1239 | 50 | 33 |
| Medical Cost Avoided | $63,872,373 | $2,703,376 | $1,652,705 |
| Work Loss Cost Avoided | $116,610,789 | $5,164,047 | $3,766,654 |
| Combined Cost Savings | $180,483,163 | $7,867,423 | $5,419,359 |
| Outcome | Fatalities | Pedestrian Fatalities | Cyclist Fatalities |
| Annual Decrease in Deaths | 7 | 2 | 0 |
| Medical Cost Avoided | $133,435 | $37,824 | $0 |
| Work Loss Cost Avoided | $10,990,016 | $3,140,455 | $0 |
| Combined Cost Savings | $11,123,451 | $3,178,279 | $0 |
| Outcome | Injured Road Users | Injured Pedestrians | Injured Cyclists |
| Annual Decrease in Number Hospitalized | 460 | 19 | 12 |
| Medical Cost Avoided | $23,713,638 | $1,027,556 | $600,984 |
| Work Loss Cost Avoided | $43,293,937 | $1,962,653 | $1,370,075 |
| Combined Cost Savings | $67,007,575 | $2,990,209 | $1,971,058 |
3.1.3. Time Spent and Fuel Consumed in Traffic
3.1.4. Air Pollution
3.1.5. Pedestrian and Bicyclist Perceptions of Safety
3.1.6. Parental Safety Perceptions and Children’s Levels of Physical Activity
3.1.7. Property Values
3.1.8. Results Summary
3.2. Recommendations
3.2.1. Further reductions in Motor Vehicle Speeds
| Estimated Annual Decrease in: | 1.8 mph Speed Reduction | 5 mph Speed Reduction |
|---|---|---|
| Total Crashes | 2219 (95% CI 286, 4042) | 6265 (95% CI 855, 10,794) |
| Fatalities | 18 (95% CI −4, 35) | 44 (95% CI −11, 67) |
| Injured Road Users | 1239 (95% CI 369, 2039) | 3336 (95% CI 1077, 5088) |
| Medical and Work Lost Cost of Fatalities | $29,694,055 | $72,586,636 |
| Medical and Work Lost Cost of Hospitalizations | $180,483,163 | $485,949,909 |
3.2.2. Implementation—Dissemination
3.2.3. Implementation—Enforcement
3.2.4. Implementation—Traffic Calming
3.3. Dissemination and Impact Evaluation

4. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Centers for Disease Control and Prevention. Injury Prevention & Control: Motor Vehicle Safety. Available online: www.cdc.gov/Motorvehiclesafety/statecosts/ma.html (accessed on 19 August 2014).
- Elvik, R. Speed limits, enforcement, and health consequences. Annu. Rev. Public Health 2012, 33, 225–238. [Google Scholar]
- LIndenmann, H. The effects on road safety of 30 kilometer-per-hour zone signposting in residential districts. ITE J. 2005, 50–54. [Google Scholar]
- Kloeden, C.; Woolley, J.; McLean, J. A follow up evaluation of the 50 km/h default urban speed limit in south Australia. In Proceedings of the Australasian Road Safety Research Policing Education Conference, Melbourne, VIC, Australia, 17–19 October 2007.
- Flexibility in Highway Design; US Department of Transportation, Federal Highway Administration: Washington, DC, USA, 2000.
- Elvik, R.; Christensen, P.; Amundsen, A. Speed and Road Accidents: An Evaluation of the Power Model; TØI Report; Institute of Transport Economics: Oslo, Norway, 2004; Volume 740. [Google Scholar]
- Elvik, R. The Power Model of the Relationship between Speed and Road Safety: Update and New Analyses; Institute of Transport Economics, Norwegian Centre for Transport Research: Oslo, Norway, 2009. [Google Scholar]
- Amoros, E.; Martin, J.L.; Lafont, S.; Laumon, B. Actual incidences of road casualties, and their injury severity, modelled from police and hospital data, France. Eur. J. Public Health 2008, 18, 360–365. [Google Scholar]
- Jeffrey, S.; Stone, D.H.; Blamey, A.; Clark, D.; Cooper, C.; Dickson, K.; Mackenzie, M.; Major, K. An evaluation of police reporting of road casualties. Inj. Prev. 2009, 15, 13–18. [Google Scholar]
- Hu, G.; Baker, T.; Baker, S.P. Comparing road traffic mortality rates from police-reported data and death registration data in China. Bull. World Health Organ. 2011, 89, 41–45. [Google Scholar]
- Centers for Disease Control and Prevention. Costs of Transportation-Related Injuries and Deaths in the United States 2005. Available online: www.cdc.gov/motorvehiclesafety/data/cost-estimates.html (accessed on 12 August 2014).
- Centers for Disease Control and Prevention; National Center for Injury Prevention and Control; Office of Statistics and Programming. Data & statistics (WISQARS™): Cost of Injury Reports. Available online: http://wisqars.cdc.gov:8080/costT/ (accessed on 11 August 2012).
- Central Transportation Planning Staff. Transportation and Emissions Modeling Report; Boston Region Metropolitan Planning Organization: Boston, MA, USA, 2012. [Google Scholar]
- Schrank, D.; Lomax, T.; Eisele, B. Urban Mobility Report; Texas Transportation Institute, The Texas A&M University System: College Station, TX, USA, 2011. [Google Scholar]
- Executive Office of Energy and Environmental Affairs. Massachusetts Gasoline and Diesel Fuel Prices for August 28, 2012; Executive Office of Energy and Environmental Affairs: Boston, MA, USA, 2012. [Google Scholar]
- Peters, A.; Dockery, D.W.; Muller, J.E.; Mittleman, M.A. Increased particulate air pollution and the triggering of myocardial infarction. Circulation 2001, 103, 2810–2815. [Google Scholar]
- Schwartz, J.; Coull, B.; Laden, F.; Ryan, L. The effect of dose and timing of dose on the association between airborne particles and survival. Environ. Health Perspect. 2008, 116, 64–69. [Google Scholar]
- Health Effects Institute. Revised Analyses of Time-Series Studies of Air Pollution and Health; Special Report; Health Effects Institute: Boston, MA, USA, 2003. [Google Scholar]
- Dominici, F.; Peng, R.D.; Bell, M.L.; Pham, L.; McDermott, A.; Zeger, S.L.; Samet, J.M. Fine particulate air pollution and hospital admission for cardiovascular and respiratory diseases. JAMA 2006, 295, 1127–1134. [Google Scholar]
- US Department of Energy. Gas Mileage Tips—Driving More Efficiently. Available online: www.fueleconomy.gov/feg/driveHabits.jsp (accessed on 11 August 2012).
- US Environmental Protection Agency. MOBILE6 Vehicle Emission Modeling Software. Available online: www.epa.gov/oms/m6.htm (accessed on 11 August 2012).
- Levy, J.I.; Buonocore, J.J.; von Stackelberg, K. Evaluation of the public health impacts of traffic congestion: A health risk assessment. Environ. Health 2010, 9, 65. [Google Scholar] [CrossRef]
- Executive Office of Health and Human Services. Massachusetts Community Health Information Profile (Masschip). Available online: www.mass.gov/eohhs/researcher/community-health/masschip/ (accessed on 3 April 2013).
- Centers for Disease Control and Prevention; National Center for Health Statistics. CDC Wonder. Available online: http://wonder.cdc.gov/ (accessed on 3 April 2013).
- Abt Associates Inc. Environmental Benefits Mapping and Analysis Program User’s Manual; Prepared for Office of Air Quality Planning and Standards US Environmental Protection Agency: Research Triangle Park, NC, USA, 2012. [Google Scholar]
- Roman, H.A.; Walker, K.D.; Walsh, T.L.; Conner, L.; Richmond, H.M.; Hubbell, B.J.; Kinney, P.L. Expert judgment assessment of the mortality impact of changes in ambient fine particulate matter in the U.S. Environ. Sci. Technol. 2008, 42, 2268–2274. [Google Scholar]
- Moolgavkar, S.H. Air pollution and hospital admissions for diseases of the circulatory system in three U.S. Metropolitan areas. J. Air Waste Manag. Assoc. 2000, 50, 1199–1206. [Google Scholar]
- Moolgavkar, S.H. Air pollution and hospital admissions for chronic obstructive pulmonary disease in three metropolitan areas in the united states. Inhal. Toxicol. 2000, 12 (Suppl. 4), 75–90. [Google Scholar]
- US Environmental Protection Agency. Regulatory Impact Analysis—Control of Air Pollution from New Motor Vehicles: Tier 2 Motor Vehicle Emissions Standards and Gasoline Sulfur Control Requirements; Engine Programs and Compliance Division, Office of Mobile Sources: Washington, DC, USA, 1999. [Google Scholar]
- Dockins, C.; Maguire, K.; Simon, N.; Sullivan, M. Value of a Statistical Life Analysis and Environmental Policy: A White Paper; US Environmental Protection Agency National Center for Environmental Economics: Washington, DC, USA, 2004. [Google Scholar]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar]
- De Nazelle, A.; Nieuwenhuijsen, M.J.; Anto, J.M.; Brauer, M.; Briggs, D.; Braun-Fahrlander, C.; Cavill, N.; Cooper, A.R.; Desqueyroux, H.; Fruin, S.; et al. Improving health through policies that promote active travel: A review of evidence to support integrated health impact assessment. Environ. Int. 2011, 37, 766–777. [Google Scholar]
- Haskell, W.L.; Blair, S.N.; Hill, J.O. Physical activity: Health outcomes and importance for public health policy. Prev. Med. 2009, 49, 280–282. [Google Scholar]
- Hamer, M.; Chida, Y. Active commuting and cardiovascular risk: A meta-analytic review. Prev. Med. 2008, 46, 9–13. [Google Scholar]
- US Census 2010; US Census Bureau: Washington, DC, USA, 2010.
- Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance System Survey Data; US Department of Health and Human Services, Centers for Disease Control and Prevention: Atlanta, GA, USA, 2010. [Google Scholar]
- White House; Office of Michelle Obama. Let’s Move! Available online: www.letsmove.gov/ (accessed on 4 April 2013).
- Rahman, T.; Cushing, R.A.; Jackson, R.J. Contributions of built environment to childhood obesity. Mt. Sinai J. Med. 2011, 78, 49–57. [Google Scholar]
- Garasky, S.; Stewart, S.D.; Gundersen, C.; Lohman, B.J.; Eisenmann, J.C. Family stressors and child obesity. Soc. Sci. Res. 2009, 38, 755–766. [Google Scholar]
- Grow, H.M.G.; Cook, A.J.; Arterburn, D.E.; Saelens, B.E.; Drewnowski, A.; Lozano, P. Child obesity associated with social disadvantage of children’s neighborhoods. Soc. Sci. Med. (1982) 2010, 71, 584–591. [Google Scholar]
- Morrison, D.S.; Thomson, H.; Petticrew, M. Evaluation of the health effects of a neighbourhood traffic calming scheme. J. Epidemiol. Community Health 2004, 58, 837–840. [Google Scholar]
- Jacobsen, P.L.; Racioppi, F.; Rutter, H. Who owns the roads? How motorised traffic discourages walking and bicycling. Inj. Prev. 2009, 15, 369–373. [Google Scholar]
- Berkman, L.F.; Kawachi, I. Social Epidemiology; Oxford University Press: New York, NY, USA, 2000. [Google Scholar]
- Diez Roux, A.V.; Mair, C. Neighborhoods and health. Ann. N. Y. Acad. Sci. 2010, 1186, 125–145. [Google Scholar]
- National Bicycle and Pedestrian Clearinghouse. The Economic and Social Benefits of Off-Road Bicycle and Pedestrian Facilities; National Bicycle and Pedestrian Clearinghouse: Washington, DC, USA, 1995. [Google Scholar]
- Modra, J. Cost-Benefit Analysis of the Application of Traffic Noise Insulation Measures to Existing Houses; Environment Protection Authority of Victoria: Melbourne, Australia, 1984. [Google Scholar]
- Bagby, D.G. The effects of traffic flow on residential property values. J. Am. Plan. Assoc. 1980, 46, 88–94. [Google Scholar]
- Eppli, M.J.; Tu, C.C. Valuing the New Urbanism: The Impact of the New Urbanism on Prices of Single-Family Homes; Urban Land Institute: Washington, DC, USA, 1999. [Google Scholar]
- Hughes, W.T.; Sirmans, C.F. Traffic externalities and single-family house prices. J. Reg. Sci. 1992, 32, 487–500. [Google Scholar]
- American Community Survey Five-Year Estimates 2006–2010; US Census Bureau: Washington, DC, USA, 2013.
- Massachusetts Department of Environmental Protection. MassDEP Air & Climate Air Quality & Monitoring Massair Version 1.3. Available online: http://public.dep.state.ma.us/MassAir/Pages/ChartByPollutant.aspx?&ht=2&hi=201 (accessed on 4 April 2013).
- World Health Organization. Transport, Environment and Health; WHO Regional Office for Europe: Copenhagen, Denmark, 2000. [Google Scholar]
- Addy, C.L.; Wilson, D.K.; Kirtland, K.A.; Ainsworth, B.E.; Sharpe, P.; Kimsey, D. Associations of perceived social and physical environmental supports with physical activity and walking behavior. Am. J. Public Health 2004, 94, 440–443. [Google Scholar]
- Hoehner, C.M.; Brennan Ramirez, L.K.; Elliott, M.B.; Handy, S.L.; Brownson, R.C. Perceived and objective environmental measures and physical activity among urban adults. Am. J. Prev. Med. 2005, 28, 105–116. [Google Scholar]
- McGinn, A.P.; Evenson, K.R.; Herring, A.H.; Huston, S.L.; Rodriguez, D.A. Exploring associations between physical activity and perceived and objective measures of the built environment. J. Urban Health 2007, 84, 162–184. [Google Scholar]
- Pucher, J.; Garrard, J.; Greaves, S. Cycling down under: A comparative analysis of bicycling trends and policies in Sydney and Melbourne. J. Transp. Geogr. 2011, 19, 332–345. [Google Scholar]
- Wahlgren, L.; Schantz, P. Exploring bikeability in a metropolitan setting: Stimulating and hindering factors in commuting route environments. BMC Public Health 2012, 12, 168. [Google Scholar] [CrossRef]
- Watkins, K.F. Cambridge’s Traffic Calming Program: Pedestrians Are the Focus. In Institute of Transportation Engineers Traffic Calming Library; Institute of Transportation Engineers: Washington, DC, USA, 2000. [Google Scholar]
- Bassett, D.R., Jr.; Pucher, J.; Buehler, R.; Thompson, D.L.; Crouter, S.E. Walking, cycling, and obesity rates in Europe, North America, and Austria. J. Phys. Act. Health 2008, 5, 795–814. [Google Scholar]
- Massachusetts Department of Public Health. Health of Massachusetts: Impact of Overweight and Obesity (1998–2007); Overweight and Obesity Prevention and Control Wellness Division Bureau of Community Health Access and Promotion: Boston, MA, USA, 2009. [Google Scholar]
- Davison, K.K.; Lawson, C.T. Do attributes in the physical environment influence children’s physical activity? A review of the literature. Int. J. Behav. Nutr. Phys. Act. 2006, 3, 19. [Google Scholar]
- Carver, A.; Timperio, A.; Hesketh, K.; Crawford, D. Are safety-related features of the road environment associated with smaller declines in physical activity among youth? J. Urban Health 2010, 87, 29–43. [Google Scholar]
- Wilson, C.; Willis, C.; Hendrikz, J.K.; Le Brocque, R.; Bellamy, N. Speed cameras for the prevention of road traffic injuries and deaths. Cochrane Database Syst Rev. 2010, 11. [Google Scholar] [CrossRef]
- Mountain, L.J.; Hirst, W.M.; Maher, M.J. Are speed enforcement cameras more effective than other speed management measures? The impact of speed management schemes on 30 mph roads. Accid. Anal. Prev. 2005, 37, 742–754. [Google Scholar]
- Pucher, J.; Dijkstra, L. Promoting safe walking and cycling to improve public health: Lessons from The Netherlands and Germany. Am. J. Public Health 2003, 93, 1509–1516. [Google Scholar]
- Elvik, R. Area-wide urban traffic calming schemes: A meta-analysis of safety effects. Accid. Anal. Prev. 2001, 33, 327–336. [Google Scholar]
- Winters, M.; Brauer, M.; Setton, E.M.; Teschke, K. Built environment influences on healthy transportation choices: Bicycling versus driving. J. Urban Health 2010, 87, 969–993. [Google Scholar]
- Johansson, C.; Rosander, P.; Leden, L. Distance between speed humps and pedestrian crossings: Does it matter? Accid. Anal. Prev. 2011, 43, 1846–1851. [Google Scholar]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
James, P.; Ito, K.; Banay, R.F.; Buonocore, J.J.; Wood, B.; Arcaya, M.C. A Health Impact Assessment of a Proposed Bill to Decrease Speed Limits on Local Roads in Massachusetts (U.S.A.). Int. J. Environ. Res. Public Health 2014, 11, 10269-10291. https://doi.org/10.3390/ijerph111010269
James P, Ito K, Banay RF, Buonocore JJ, Wood B, Arcaya MC. A Health Impact Assessment of a Proposed Bill to Decrease Speed Limits on Local Roads in Massachusetts (U.S.A.). International Journal of Environmental Research and Public Health. 2014; 11(10):10269-10291. https://doi.org/10.3390/ijerph111010269
Chicago/Turabian StyleJames, Peter, Kate Ito, Rachel F. Banay, Jonathan J. Buonocore, Benjamin Wood, and Mariana C. Arcaya. 2014. "A Health Impact Assessment of a Proposed Bill to Decrease Speed Limits on Local Roads in Massachusetts (U.S.A.)" International Journal of Environmental Research and Public Health 11, no. 10: 10269-10291. https://doi.org/10.3390/ijerph111010269
APA StyleJames, P., Ito, K., Banay, R. F., Buonocore, J. J., Wood, B., & Arcaya, M. C. (2014). A Health Impact Assessment of a Proposed Bill to Decrease Speed Limits on Local Roads in Massachusetts (U.S.A.). International Journal of Environmental Research and Public Health, 11(10), 10269-10291. https://doi.org/10.3390/ijerph111010269