Factor Structure of Early Smoking Experiences and Associations with Smoking Behavior: Valence or Sensitivity Model?

Abstract
:1. Introduction
1.1. Perspectives on Initial Subjective Experiences of Tobacco
1.2. Methodological Issues and Measurement of Initial Subjective Experiences of Tobacco
2. Experimental Section
2.1. Participants and Procedures
2.2. Measures
2.2.1. Initial Experience of Tobacco
2.2.2. Smoking Behavior
2.2.3. Socio-Demographic Variables
2.3. Data Analysis
2.3.1. Exploratory Structural Equation Modeling (ESEM)
- -
- The root mean square error of approximation (RMSEA), which is an approximation of the fit in the population. A value of 0.05 or less can be considered a good fit, whereas a RMSEA between 0.05 and 0.08 can be interpreted as an acceptable fit [31];
- -
- The comparative fit index (CFI), which compares the result to the independence model. Values greater than 0.95 are considered a good fit, and those between 0.90 and 0.95 an acceptable fit [32];
- -
- The standardized root mean square residual (SRMR) for EFA and the weighted root mean square residual (WRMR) for ESEM, which calculated the difference between observed and predicted correlations. Values under 0.10 for SRMR and 0.90 for WRMR are interpreted as good fits [33].
2.3.2. Structural Equation Modeling (SEM)
3. Results and Discussion
3.1. Descriptive Results

{kind=link}
{kind=link}
{kind=link}
| Variables | Overall N = 3,368 | Language | Smoking status | ||||
|---|---|---|---|---|---|---|---|
| (N = 3,368) | (N = 3,216) | ||||||
| French-speaking | German-speaking | Current smokers | Former smokers | ||||
| N = 1,745 | N = 1,623 | N = 2,392 | N = 824 | ||||
| Initial experiences of tobacco 1 | |||||||
| Did not feel very well | 38.8 | 41.9 | 35.5 | 41.7 | 30.8 | ||
| Coughed | 44.4 | 50.1 | 38.1 | 47.7 | 35.2 | ||
| Had a headache | 22.4 | 30.7 | 13.6 | 23.2 | 20.1 | ||
| Felt irritation in the eyes and bad taste | 45.8 | 48.9 | 42.4 | 48.2 | 38.2 | ||
| Had an upset stomach | 5.8 | 5.6 | 6.1 | 6.4 | 3.6 | ||
| Felt heart pounding | 14. 9 | 15.7 | 14.1 | 16.4 | 9.7 | ||
| Felt dizzy, lightheaded | 44.4 | 40.1 | 49.0 | 47.2 | 36.8 | ||
| Felt nauseous | 11.8 | 12.6 | 10.9 | 11.9 | 11.0 | ||
| Liked the experience | 45.7 | 45.2 | 46.2 | 48.9 | 39.3 | ||
| Felt relaxed | 44.2 | 38.3 | 50.6 | 48.5 | 32.0 | ||
| Smoking behavior (N = 3,216) | |||||||
| Continued use (past 12 months) 1 | - | 78.0 | 70.5 | 100 | 0 | ||
| Nicotine dependence (FTND, score 0–10) 2 | - | 1.54 (2.04) | 1.35 (1.98) | 1.95 (2.12) | - | ||
| Number of cigarettes smoked weekly 2 | - | 41.47 (54.26) | 37.51 (51.99) | 53.20 (55.52) | - | ||
| Age of onset of tobacco use 2 | - | 14.62 (2.43) | 14.50 (2.40) | 14.43 (2.43) | - | ||
| Socio-demographic covariates | |||||||
| Age 2 | 20.30 (1.29) | 20.36 (1.31) | 19.66 (1.03) | 20.06 (1.23) | 19.91 (1.25) | ||
| Education 1 | |||||||
| Primary (9 years of schooling) | - | 38.5 | 62.6 | 49.8 | 50.7 | ||
| Secondary (12 years of schooling) | - | 29.3 | 24.3 | 27.8 | 24.4 | ||
| Tertiary (13 years of schooling or more) | - | 32.1 | 13.2 | 22.4 | 24.9 | ||
| Perceived financial situation 1 | |||||||
| Below average income | - | 14.8 | 15.8 | 16.0 | 13.1 | ||
| Average income | - | 48.4 | 30.7 | 40.2 | 39.2 | ||
| Above average income | - | 36.8 | 53.4 | 43.8 | 47.7 | ||
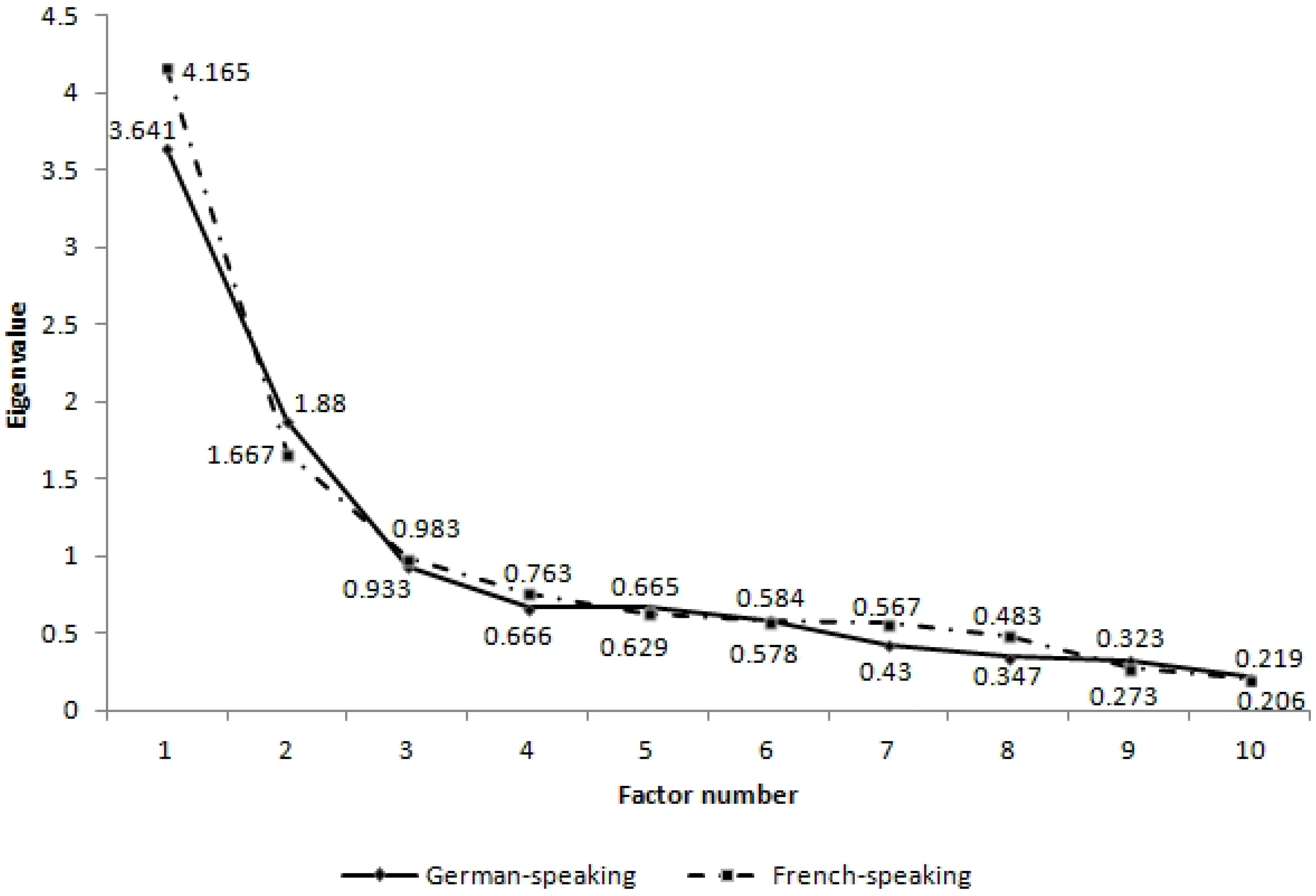
3.2. ESE Factor Structure
| German-speaking | French-speaking | |||||
|---|---|---|---|---|---|---|
| (N = 1,542) | (N = 1,674) | |||||
| 1st factor | 2nd factor | 3nd factor | 1st factor | 2nd factor | 3nd factor | |
| Did not feel very well | 0.258 ** | 0.286 ** | −0.049 | 0.196 * | 0.668 *** | 0.000 |
| Coughed | 0.015 | 0.664 *** | −0.024 | 0.771 *** | 0.005 | −0.081 |
| Had a headache | 0.473 *** | 0.272 * | 0.002 | 0.178 * | 0.625 *** | 0.061 |
| Felt irritation in the eyes and bad taste | −0.018 | 0.654 *** | 0.009 | 0.373 *** | 0.273 *** | −0.018 |
| Had an upset stomach | 1.015 *** | −0.243 *** | 0.001 | 0.001 | 0.779 *** | 0.120 * |
| Felt heart pounding | 0.490 *** | 0.060 | 0.174 ** | -0.047 | 0.610 *** | 0.171 *** |
| Felt dizzy, lightheaded | 0.240 * | 0.401 *** | 0.246 *** | 0.046 | 0.601 *** | 0.250 *** |
| Felt nauseous | 0.805 *** | 0.001 | −0.265 *** | -0.253 | 1.023 *** | −0.017 |
| Liked the experience | −0.188 | 0.000 | 0.975 *** | 0.001 | -0.246 *** | 0.857 *** |
| Felt relaxed | −0.040 | 0.008 | 0.735 *** | -0.040 | 0.008 | 0.735 *** |
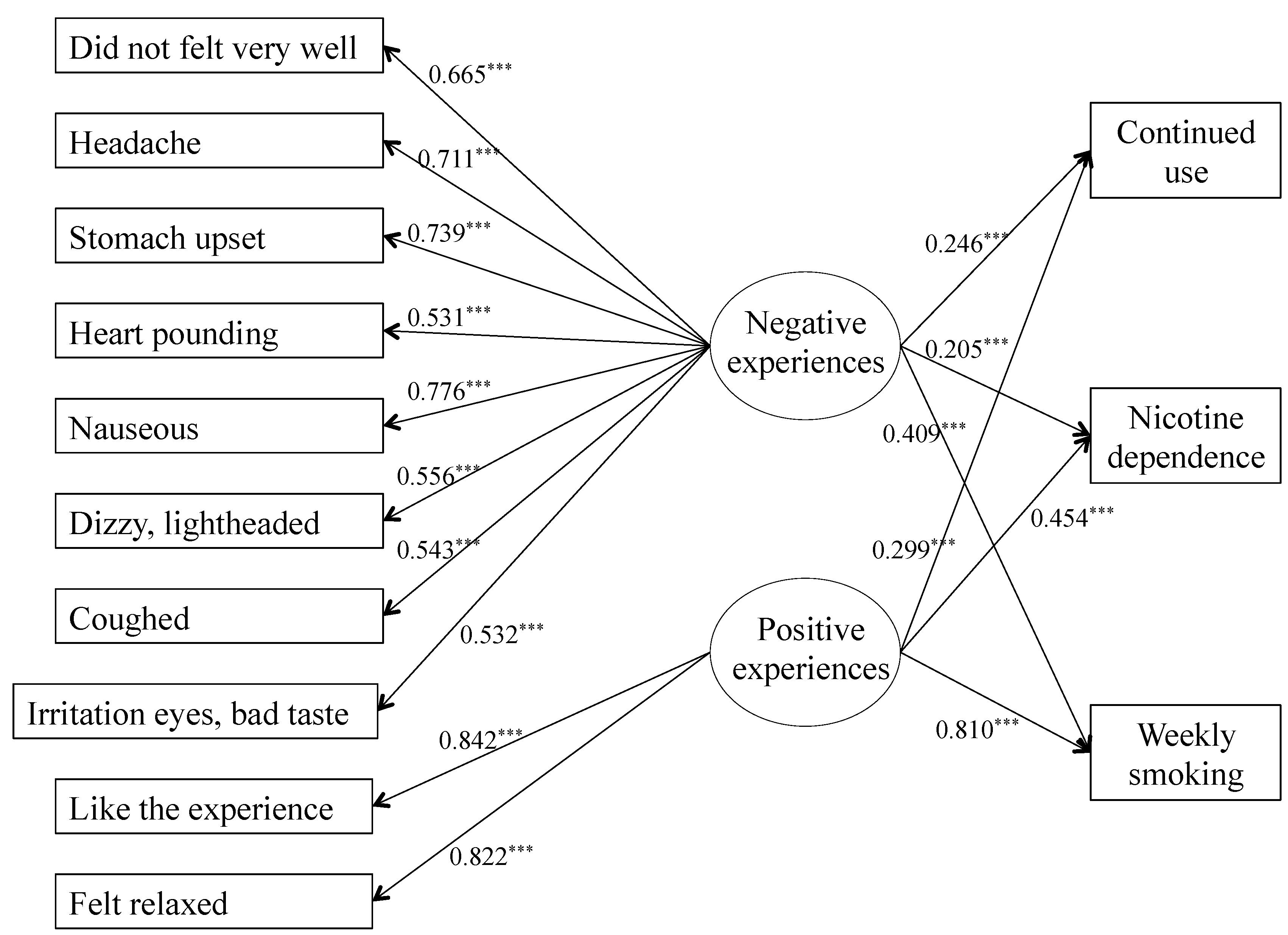
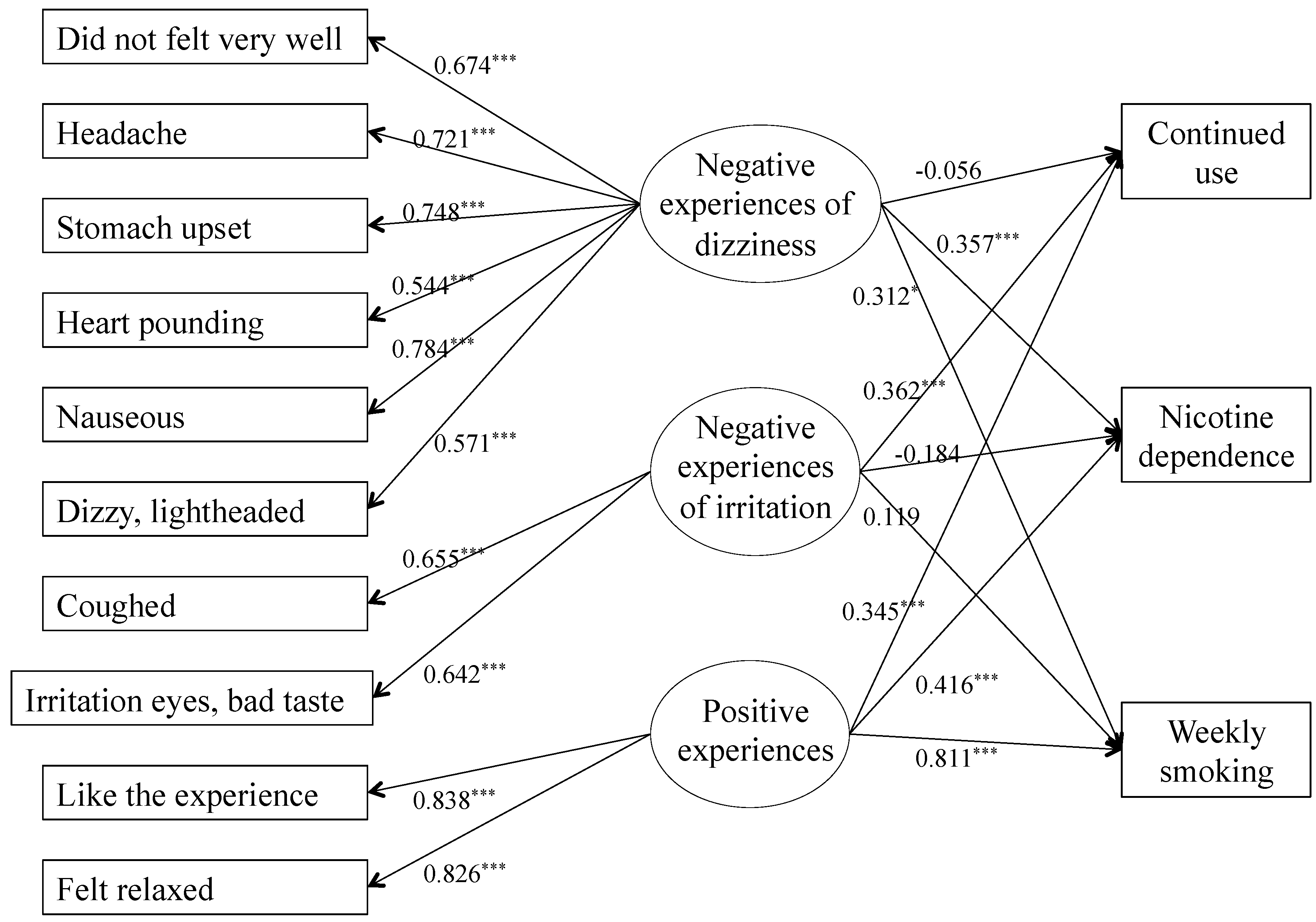
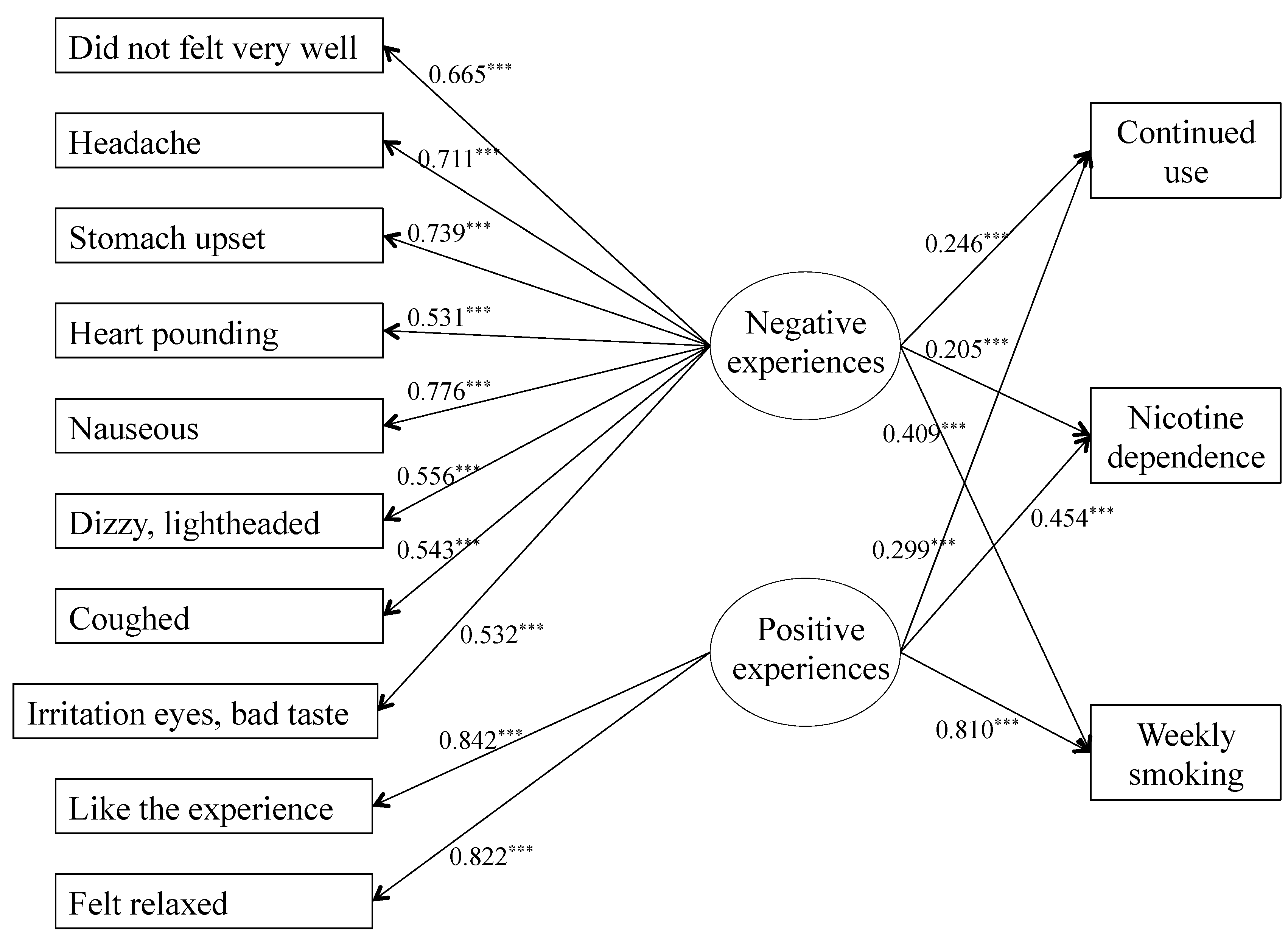
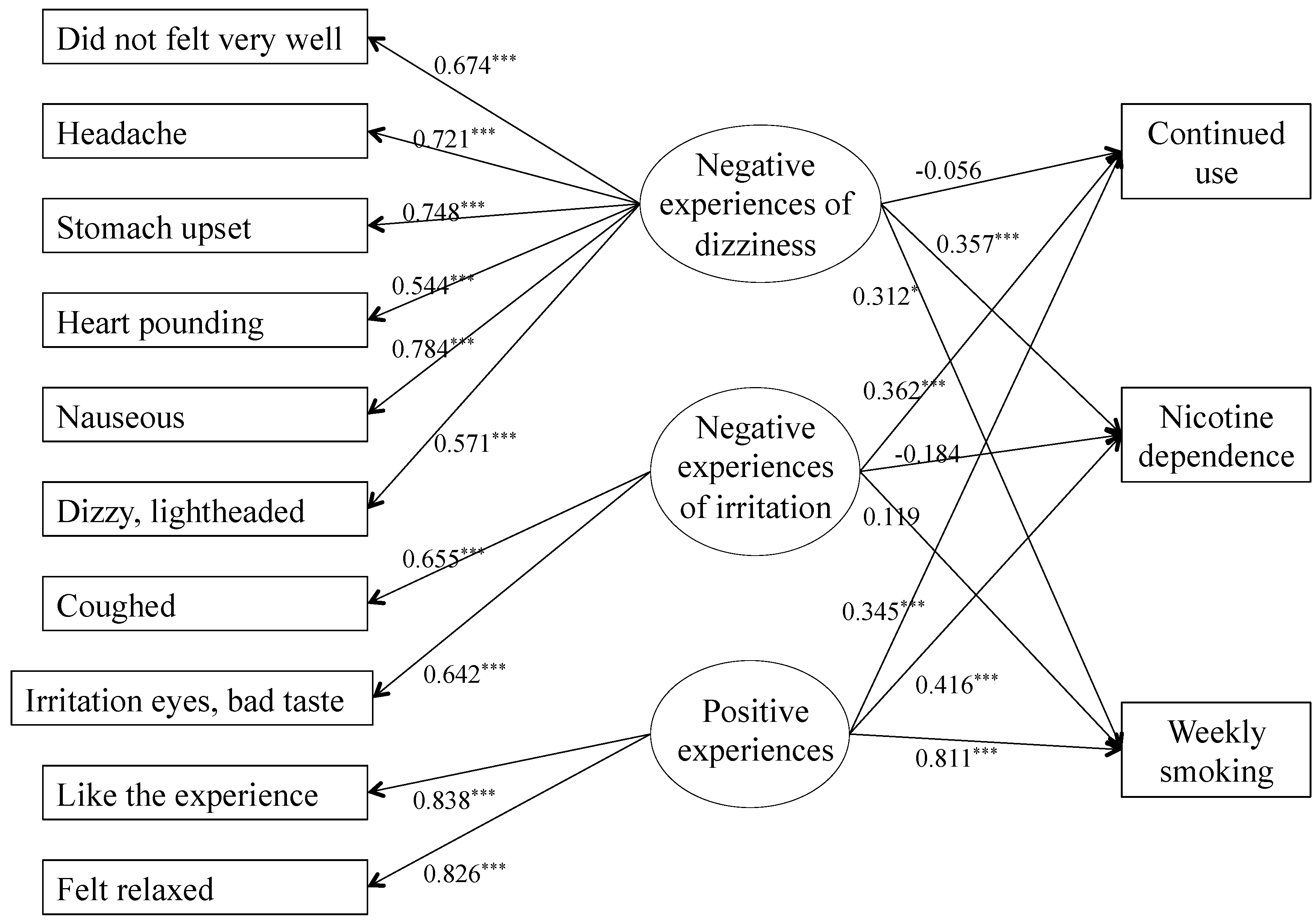
3.3. Predictive Accuracy of Initial Subjective Experiences on Smoking Behavior
3.4. Discussion
4. Conclusions
Conflicts of Interest
References
- Chen, X.; Stacy, A.; Zheng, H.; Shan, J.; Spruijt-Metz, D.; Unger, J.; Gong, J.; Gallaher, P.; Liu, C.; Azen, S.; Shakib, S.; Johnson, C.A. Sensations from initial exposure to nicotine predicting adolescent smoking in China: A potential measure of vulnerability to nicotine. Nicotine Tob. Res. 2003, 5, 455–463. [Google Scholar]
- Eissenberg, T.; Balster, R.L. Initial tobacco use episodes in children and adolescents: Current knowledge, future directions. Drug Alcohol Depend. 2000, 59, S41–S60. [Google Scholar] [CrossRef]
- Pomerleau, O.F.; Collins, A.C.; Shiffman, S.; Pomerleau, C.S. Why some people smoke and others do not: New perspectives. J. Consult. Clin. Psychol. 1993, 61, 723–731. [Google Scholar] [CrossRef]
- DiFranza, J.R.; Savageau, J.A.; Fletcher, K.; Ockene, J.K.; Rigotti, N.A.; McNeill, A.D.; Coleman, M.; Wood, C. Recollections and repercussions of the first inhaled cigarette. Addict. Behav. 2004, 29, 261–272. [Google Scholar] [CrossRef]
- Urbán, R. Early smoking experience in adolescents. Addict. Behav. 2010, 35, 612–615. [Google Scholar] [CrossRef]
- Glautier, S. Measures and models of nicotine dependence: Positive reinforcement. Addiction 2004, 99 (Suppl 1), 30–50. [Google Scholar] [CrossRef]
- Hughes, J.R. Should criteria for drug dependence differ across drugs? Addiction 2006, 101, 134–141. [Google Scholar] [CrossRef]
- de Wit, H.; Phillips, T.J. Do initial responses to drugs predict future use or abuse? Neurosci. Biobehav. Rev. 2012, 36, 1565–1576. [Google Scholar] [CrossRef]
- Hirschman, R.S.; Leventhal, H.; Glynn, K. The Development of smoking behavior: Conceptualization and supportive cross-sectional survey data. J. Appl. Soc. Psychol. 1984, 14, 184–206. [Google Scholar] [CrossRef]
- Shiffman, S. Tobacco “chippers”—Individual differences in tobacco dependence. Psychopharmacology (Berl.) 1989, 97, 539–547. [Google Scholar] [CrossRef]
- Bewley, B.R.; Bland, J.M.; Harris, R. Factors associated with the starting of cigarette smoking by primary school children. Br. J. Prev. Soc. Med. 1974, 28, 37–44. [Google Scholar]
- Friedman, L.S.; Lichtenstein, E.; Biglan, A. Smoking onset among teens: An empirical analysis of initial situations. Addict. Behav. 1985, 10, 1–13. [Google Scholar] [CrossRef]
- Pomerleau, C.S.; Marks, J.L.; Pomerleau, O.F.; Snedecor, S.M. Relationship between early experiences with tobacco and early experiences with alcohol. Addict. Behav. 2004, 29, 1245–1251. [Google Scholar] [CrossRef]
- Pomerleau, C.S.; Pomerleau, O.F.; Namenek, R.J.; Marks, J.L. Initial exposure to nicotine in college-age women smokers and never-smokers: A replication and extension. J. Addict. Dis. 1999, 18, 13–19. [Google Scholar]
- Pomerleau, O.F.; Pomerleau, C.S.; Namenek, R.J. Early experiences with tobacco among women smokers, ex-smokers, and never-smokers. Addiction 1998, 93, 595–599. [Google Scholar] [CrossRef]
- Rodriguez, D.; Audrain-McGovern, J. Construct validity analysis of the early smoking experience questionnaire for adolescents. Addict. Behav. 2004, 29, 1053–1057. [Google Scholar] [CrossRef]
- Urbán, R.; Sutfin, E. Do early smoking experiences count in development of smoking?: Temporal stability and predictive validity of an Early Smoking Experience Questionnaire in adolescents. Nicotine Tob. Res. 2010, 12, 1265–1269. [Google Scholar] [CrossRef]
- Kozlowski, L.T.; Harford, M.R. On the significance of never using a drug: An example from cigarette smoking. J. Abnormal Psychol. 1976, 85, 433–434. [Google Scholar] [CrossRef]
- Ríos-Bedoya, C.F.; Pomerleau, C.S.; Neuman, R.J.; Pomerleau, O.F. Using MIMIC models to examine the relationship between current smoking and early smoking experiences. Nicotine Tob. Res. 2009, 11, 1035–1041. [Google Scholar] [CrossRef]
- Pomerleau, O.F. Individual differences in sensitivity to nicotine: Implications for genetic research on nicotine dependence. Behav. Genet. 1995, 25, 161–177. [Google Scholar] [CrossRef]
- Perkins, K.A.; Lerman, C.; Coddington, S.; Karelitz, J.L. Association of retrospective early smoking experiences with prospective sensitivity to nicotine via nasal spray in nonsmokers. Nicotine Tob. Res. 2008, 10, 1335–1345. [Google Scholar] [CrossRef]
- Riedel, B.W.; Blitstein, J.L.; Robinson, L.A.; Murray, D.M.; Klesges, R.C. The reliability and predictive value of adolescents’ reports of initial reactions to smoking. Nicotine Tob. Res. 2003, 5, 553–559. [Google Scholar] [CrossRef]
- Okoli, C.T.C.; Richardson, C.G.; Johnson, J.L. An examination of the relationship between adolescents’ initial smoking experience and their exposure to peer and family member smoking. Addict. Behav. 2008, 33, 1183–1191. [Google Scholar] [CrossRef]
- Kalman, D. The subjective effects of nicotine: Methodological issues, a review of experimental studies, and recommendations for future research. Nicotine Tob. Res. 2002, 4, 25–70. [Google Scholar] [CrossRef]
- Dar, R.; Kaplan, R.; Shaham, L.; Frenk, H. Euphoriant effects of nicotine in smokers: Fact or artifact? Psychopharmacology (Berl.) 2007, 191, 203–210. [Google Scholar] [CrossRef]
- O’Connor, R.J.; Kozlowski, L.T.; Vandenbergh, D.J.; Strasser, A.A.; Grant, M.D.; Vogler, G.P. An examination of early smoking experiences and smoking status in a national cross-sectional sample. Addiction 2005, 100, 1352–1357. [Google Scholar] [CrossRef]
- Studer, J.; Baggio, S.; Mohler-Kuo, M.; Dermota, P.; Gaume, J.; Bertholet, N.; Daeppen, J.-B.; Gmel, G. Examining non-response bias in substance use research—Are late respondents proxies for non-respondents? Drug Alcohol Depend. 2013, 132, 316–323. [Google Scholar] [CrossRef]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerström, K.O. The Fagerström Test for Nicotine Dependence: A revision of the Fagerström Tolerance Questionnaire. Br. J. Addict. 1991, 86, 1119–1127. [Google Scholar] [CrossRef]
- Asparouhov, T.; Muthén, B. Exploratory structural equation modeling. Struct. Equat. Model. 2009, 16, 397–438. [Google Scholar] [CrossRef]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 6th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2010. [Google Scholar]
- Browne, M.W.; Cudeck, R. Alternative ways of assessing model fit. Sociol. Methods Res. 1992, 21, 230–258. [Google Scholar] [CrossRef]
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equat. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Yu, C.Y.; Muthén, B. Evaluation of Model Fit Indices for Latent Variable Models with Categorical and Continuous Outcome. In Presented in Annual Meeting of the American Educational Research Association, New Orleans, LA, USA, 1–5 April 2002.
- Kaiser, H.F. The application of electronic computers to factor analysis. Educ. Psychol. Measur. 1960, 20, 141–151. [Google Scholar] [CrossRef]
© 2013 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Baggio, S.; Studer, J.; Deline, S.; Mohler-Kuo, M.; Daeppen, J.-B.; Gmel, G. Factor Structure of Early Smoking Experiences and Associations with Smoking Behavior: Valence or Sensitivity Model? Int. J. Environ. Res. Public Health 2013, 10, 6305-6318. https://doi.org/10.3390/ijerph10126305
Baggio S, Studer J, Deline S, Mohler-Kuo M, Daeppen J-B, Gmel G. Factor Structure of Early Smoking Experiences and Associations with Smoking Behavior: Valence or Sensitivity Model? International Journal of Environmental Research and Public Health. 2013; 10(12):6305-6318. https://doi.org/10.3390/ijerph10126305
Chicago/Turabian StyleBaggio, Stéphanie, Joseph Studer, Stéphane Deline, Meichun Mohler-Kuo, Jean-Bernard Daeppen, and Gerhard Gmel. 2013. "Factor Structure of Early Smoking Experiences and Associations with Smoking Behavior: Valence or Sensitivity Model?" International Journal of Environmental Research and Public Health 10, no. 12: 6305-6318. https://doi.org/10.3390/ijerph10126305
APA StyleBaggio, S., Studer, J., Deline, S., Mohler-Kuo, M., Daeppen, J.-B., & Gmel, G. (2013). Factor Structure of Early Smoking Experiences and Associations with Smoking Behavior: Valence or Sensitivity Model? International Journal of Environmental Research and Public Health, 10(12), 6305-6318. https://doi.org/10.3390/ijerph10126305