
Calanus Oil and Lifestyle Interventions Improve Glucose Homeostasis in Obese Subjects with Insulin Resistance

 , ,
, ,  and
and
Abstract
1. Introduction
2. Results
2.1. Study Cohort Characteristics at Baseline
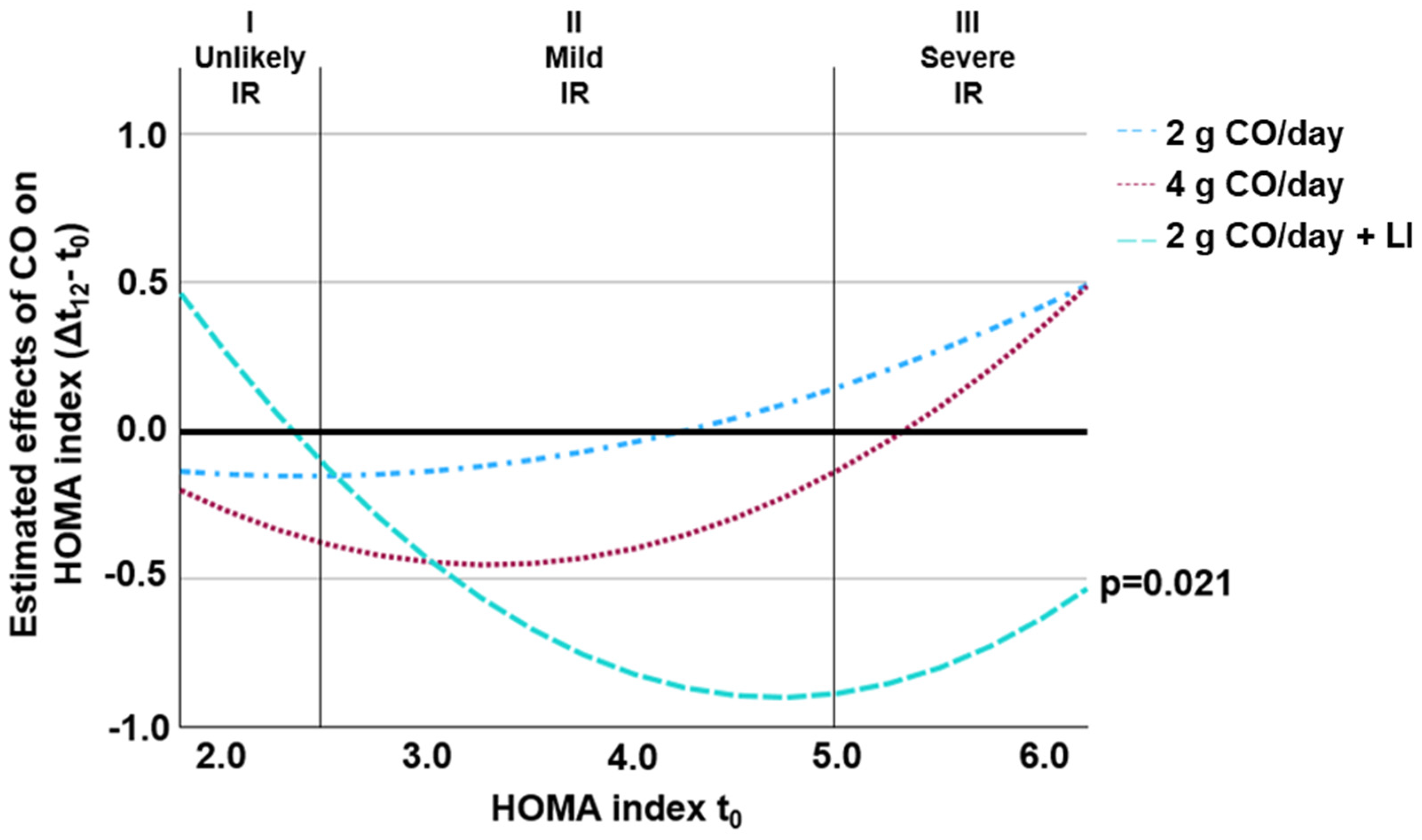
2.2. Effects of Intervention on HOMA Index (Primary Outcome)
2.3. Secondary Outcomes
3. Discussion
Limitations
4. Materials and Methods
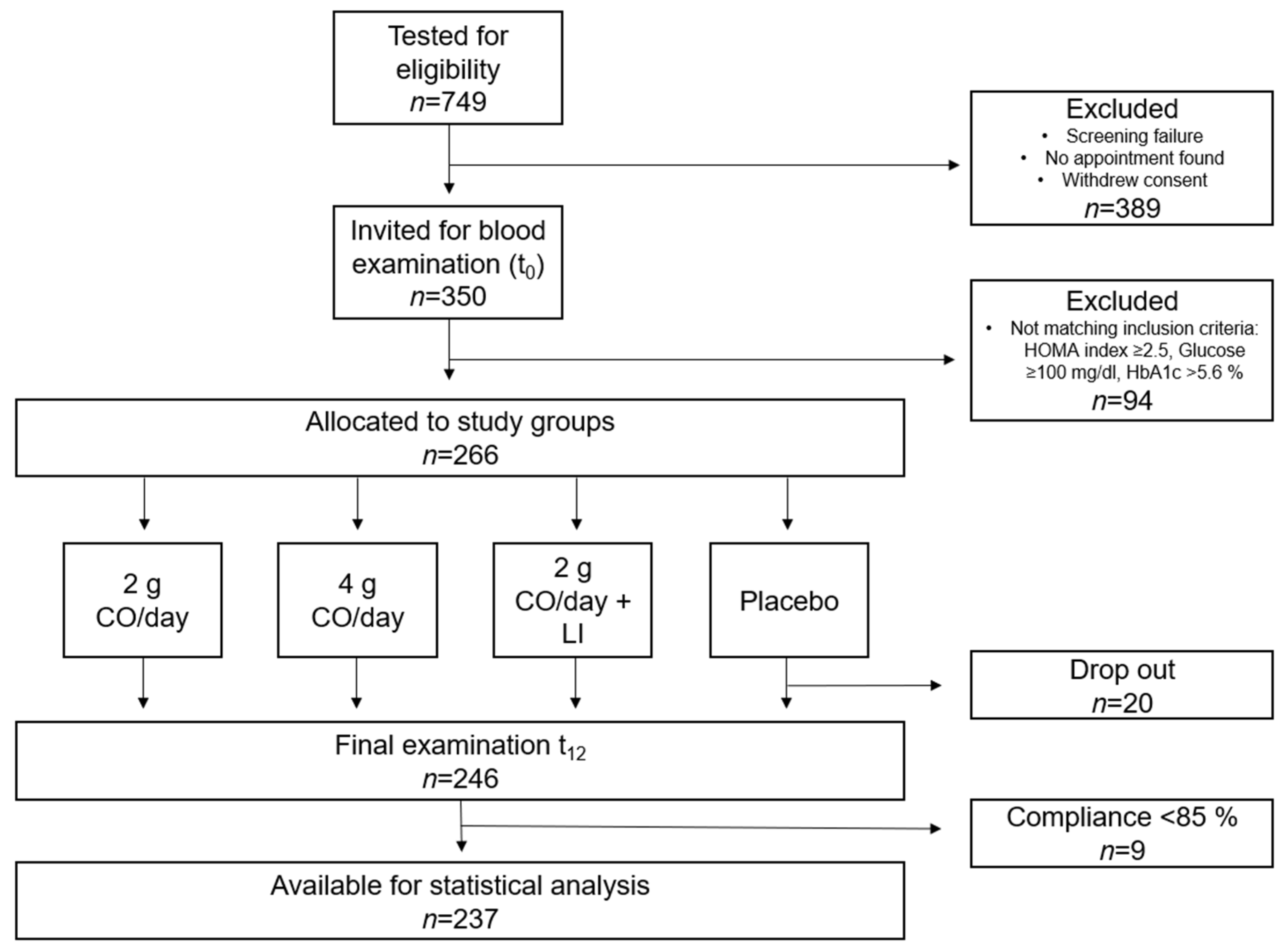
4.1. Study Design and Study Subjects
- A total of 2 g CO/day spread over 4 capsules;
- A total of 4 g CO/day spread over 8 capsules;
- A total of 2 g CO/day in combination with LI (diet counselling + moderate exercise, approximately 2.5 h per week;
- Placebo, 4 capsules of paraffin oil per day.
4.2. Test Products
4.3. Anthropometric and Body Composition Measurements
4.4. Monitoring of Lifestyle Intervention and Physical Activity
4.5. Blood Sampling and Biochemical Analysis
4.6. Sample Size Calculation and Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CO | Calanus Oil |
| DHA | Docosahexaenoic Acid |
| EMM | Estimated Marginal Means |
| EPA | Eicosapentaenoic Acid |
| HOMA | Homeostatic Model Assessment |
| IR | Insulin Resistance |
| LI | Lifestyle Intervention |
| MetS | Metabolic Syndrome Severity Score |
| n3 PUFA | Long-chain Polyunsaturated Fatty Acid |
| VAT | Visceral Adipose Tissue |
| WC | Waist Circumference |
References
- Mirabelli, M.; Chiefari, E.; Arcidiacono, B.; Corigliano, D.M.; Brunetti, F.S.; Maggisano, V.; Russo, D.; Foti, D.P.; Brunetti, A. Mediterranean Diet Nutrients to Turn the Tide against Insulin Resistance and Related Diseases. Nutrients 2020, 12, 1066. [Google Scholar] [CrossRef] [PubMed]
- Blüher, M.; Aras, M.; Aronne, L.J.; Batterham, R.L.; Giorgino, F.; Ji, L.; Pietilänien, K.; Schnell, O.; Tonschevska, E.; Wilding, J. New insights into the treatment of obesity. Diabetes Obes. Metab. 2023, 25, 2058–2072. [Google Scholar] [CrossRef] [PubMed]
- Kawai, T.; Autieri, M.V.; Scalia, R. Adipose tissue inflammation and metabolic dysfunction in obesity. Am. J. Physiol. Cell Physiol. 2021, 320, C375–C391. [Google Scholar] [CrossRef]
- Hardy, O.T.; Czech, M.P.; Corvera, S. What causes the insulin resistance underlying obesity? Curr. Opin. Endocrinol. Diabetes Obes. 2012, 19, 81–87. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Wallace, T.M.; Levy, J.C.; Matthews, D.R. Use and abuse of HOMA modeling. Diabetes Care 2004, 27, 1487–1495. [Google Scholar] [CrossRef]
- Cho, S.K.; Huh, J.H.; Yoo, J.S.; Kim, J.W.; Lee, K.J. HOMA-estimated insulin resistance as an independent prognostic factor in patients with acute pancreatitis. Sci. Rep. 2019, 9, 14894. [Google Scholar] [CrossRef]
- Singh, Y.; Garg, M.K.; Tandon, N.; Marwaha, R.K. A Study of Insulin Resistance by HOMA-IR and its Cut-off Value to Identify Metabolic Syndrome in Urban Indian Adolescents. J. Clin. Res. Pediatr. Endocrinol. 2013, 5, 245–251. [Google Scholar]
- Lee, S.; Lacy, M.E.; Jankowich, M.; Correa, A.; Wu, W.-C. Association between obesity phenotypes of insulin resistance and risk of type 2 diabetes in African Americans: The Jackson Heart Study. J. Clin. Transl. Endocrinol. 2020, 19, 100210. [Google Scholar] [CrossRef]
- Magkos, F.; Hjorth, M.F.; Astrup, A. Diet and exercise in the prevention and treatment of type 2 diabetes mellitus. Nat. Rev. Endocrinol. 2020, 16, 545–555. [Google Scholar] [CrossRef]
- Lean, M.E.; Leslie, W.S.; Barnes, A.C.; Brosnahan, N.; Thom, G.; McCombie, L.; Peters, C.; Zhyzhneuskaya, S.; Al-Mrabeh, A.; Hollingsworth, K.; et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT): An open-label, cluster-randomised trial. Lancet 2018, 391, 541–551. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.F.; Hagen, W.; Kattner, G. Lipid storage in marine zooplankton. Mar. Ecol. Prog. Ser. 2006, 307, 273–306. [Google Scholar] [CrossRef]
- Marazzi, G.; Cacciotti, L.; Pelliccia, F.; Iaia, L.; Volterrani, M.; Caminiti, G.; Sposata, B.; Massaro, R.; Grieco, F.; Rosano, G. Long-term effects of nutraceuticals (berberine, red yeast rice, policosanol) in elderly hypercholesterolemic patients. Adv. Ther. 2011, 28, 1105–1113. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Luo, F.; Lin, Q. Policosanol: Extraction and biological functions. J. Funct. Foods 2019, 57, 351–360. [Google Scholar] [CrossRef]
- Höper, A.C.; Salma, W.; Khalid, A.M.; Hafstad, A.D.; Sollie, S.J.; Raa, J.; Larsen, T.; Aasum, E. Oil from the marine zooplankton Calanus finmarchicus improves the cardiometabolic phenotype of diet-induced obese mice. Br. J. Nutr. 2013, 110, 2186–2193. [Google Scholar] [CrossRef]
- Burhop, M.; Schuchardt, J.P.; Nebl, J.; Müller, M.; Lichtinghagen, R.; Hahn, A. Marine Oil from C. finmarchicus Enhances Glucose Homeostasis and Liver Insulin Resistance in Obese Prediabetic Individuals. Nutrients 2022, 14, 396. [Google Scholar] [CrossRef]
- Kjøbsted, R.; Hingst, J.R.; Fentz, J.; Foretz, M.; Sanz, M.-N.; Pehmøller, C.; Shum, M.; Marette, A.; Mounier, R.; Treebak, J.; et al. AMPK in skeletal muscle function and metabolism. FASEB J. 2018, 32, 1741–1777. [Google Scholar] [CrossRef]
- Oharomari, L.K.; Ikemoto, M.J.; Hwang, D.J.; Koizumi, H.; Soya, H. Benefits of Exercise and Astaxanthin Supplementation: Are There Additive or Synergistic Effects? Antioxidants 2021, 10, 870. [Google Scholar] [CrossRef]
- Basu, R.; Barosa, C.; Jones, J.; Dube, S.; Carter, R.; Basu, A.; Rizza, R. Pathogenesis of prediabetes: Role of the liver in isolated fasting hyperglycemia and combined fasting and postprandial hyperglycemia. J. Clin. Endocrinol. Metab. 2013, 98, E409–E417. [Google Scholar] [CrossRef]
- Engin, B.; Willis, S.A.; Malaikah, S.; Sargeant, J.A.; Yates, T.; Gray, L.J.; Aithal, J.; Stensel G., P.; King D., J.A. The effect of exercise training on adipose tissue insulin sensitivity: A systematic review and meta-analysis. Obes. Rev. 2022, 23, e13445. [Google Scholar] [CrossRef]
- Neeland, I.J.; Ayers, C.R.; Rohatgi, A.K.; Turer, A.T.; Berry, J.D.; Das, S.R.; Vega, G.; Khera, L.; McGuire, D.; Gundi, S.M.; et al. Associations of visceral and abdominal subcutaneous adipose tissue with markers of cardiac and metabolic risk in obese adults. Obesity 2013, 21, E439–E447. [Google Scholar] [CrossRef] [PubMed]
- Schots, P.C.; Pedersen, A.M.; Eilertsen, K.-E.; Olsen, R.L.; Larsen, T.S. Possible Health Effects of a Wax Ester Rich Marine Oil. Front. Pharmacol. 2020, 11, 961. [Google Scholar] [CrossRef] [PubMed]
- Wasserfurth, P.; Nebl, J.; Schuchardt, J.P.; Müller, M.; Boßlau, T.K.; Krüger, K.; Hahn, A. Effects of Exercise Combined with a Healthy Diet or Calanus finmarchicus Oil Supplementation on Body Composition and Metabolic Markers—A Pilot Study. Nutrients 2020, 12, 2139. [Google Scholar] [CrossRef] [PubMed]
- Čížková, T.; Štěpán, M.; Daďová, K.; Ondrůjová, B.; Sontáková, L.; Krauzová, E.; Matouš, M.; Koc, M.; Gojda, J.; Kračmerová, J.; et al. Exercise Training Reduces Inflammation of Adipose Tissue in the Elderly: Cross-Sectional and Randomized Interventional Trial. J. Clin. Endocrinol. Metab. 2020, 105, dgaa630. [Google Scholar] [CrossRef]
- Burgess, E.; Hassmén, P.; Pumpa, K.L. Determinants of adherence to lifestyle intervention in adults with obesity: A systematic review. Clin. Obes. 2017, 7, 123–135. [Google Scholar] [CrossRef]
- Sandforth, A.; von Schwartzenberg, R.J.; Arreola, E.V.; Hanson, R.L.; Sancar, G.; Katzenstein, S.; Lange, K.; Preißl, H.; Dreher, S.; Weigert, C.; et al. Mechanisms of weight loss-induced remission in people with prediabetes: A post-hoc analysis of the randomised, controlled, multicentre Prediabetes Lifestyle Intervention Study (PLIS). Lancet Diabetes Endocrinol. 2023, 11, 798–810. [Google Scholar] [CrossRef]
- Barbu, E.; Popescu, M.-R.; Popescu, A.-C.; Balanescu, S.-M. Phenotyping the Prediabetic Population—A Closer Look at Intermediate Glucose Status and Cardiovascular Disease. Int. J. Mol. Sci. 2021, 22, 6864. [Google Scholar] [CrossRef]
- Abbott, K.A.; Burrows, T.L.; Acharya, S.; Thota, R.N.; Garg, M.L. DHA-enriched fish oil reduces insulin resistance in overweight and obese adults. Prostaglandins Leukot. Essent. Fat. Acids 2020, 159, 102154. [Google Scholar] [CrossRef]
- Wagner, R.; Heni, M.; Tabák, A.G.; Machann, J.; Schick, F.; Randrianarisoa, E.; Hrabe de Angelis, M.; Birkenfeld, A.L.; Stefan, N.; Peter, A.; et al. Pathophysiology-based subphenotyping of individuals at elevated risk for type 2 diabetes. Nat. Med. 2021, 27, 49–57. [Google Scholar] [CrossRef]
- Derosa, G.; Cicero, A.F.G.; D’Angelo, A.; Borghi, C.; Maffioli, P. Effects of n-3 pufas on fasting plasma glucose and insulin resistance in patients with impaired fasting glucose or impaired glucose tolerance. BioFactors 2016, 42, 316–322. [Google Scholar] [CrossRef]
- Mounien, L.; Tourniaire, F.; Landrier, J.-F. Anti-Obesity Effect of Carotenoids: Direct Impact on Adipose Tissue and Adipose Tissue-Driven Indirect Effects. Nutrients 2019, 11, 1562. [Google Scholar] [CrossRef] [PubMed]
- Ciaraldi, T.P.; Boeder, S.C.; Mudaliar, S.R.; Giovannetti, E.R.; Henry, R.R.; Pettus, J.H. Astaxanthin, a natural antioxidant, lowers cholesterol and markers of cardiovascular risk in individuals with prediabetes and dyslipidaemia. Diabetes Obes. Metab. 2023, 25, 1985–1994. [Google Scholar] [CrossRef] [PubMed]
- Xia, W.; Tang, N.; Kord-Varkaneh, H.; Low, T.Y.; Tan, S.C.; Wu, X.; Zhu, Y. The effects of astaxanthin supplementation on obesity, blood pressure, CRP, glycemic biomarkers, and lipid profile: A meta-analysis of randomized controlled trials. Pharmacological research 2020, 161, 105113. [Google Scholar] [CrossRef]
- Wang, J.-F.; Zhang, H.-M.; Li, Y.-Y.; Xia, S.; Wei, Y.; Yang, L.; Wang, D.; Ye, J.-J.; Li, H.-X.; Yuan, J.; et al. A combination of omega-3 and plant sterols regulate glucose and lipid metabolism in individuals with impaired glucose regulation: A randomized and controlled clinical trial. Lipids Health Dis. 2019, 18, 106. [Google Scholar] [CrossRef]
- Schuchardt, J.P.; Hahn, A. Bioavailability of long-chain omega-3 fatty acids. Prostaglandins Leukot. Essent. Fat. Acids 2013, 89, 1–8. [Google Scholar] [CrossRef]
- WHO. WHO Guidelines on Physical Activity and Sedentary Behaviour, 1st ed.; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Frey, I.; Berg, A.; Grathwohl, D.; Keul, J. Freiburger Fragebogen zur körperlichen Aktivität--Entwicklung, Prüfung und Anwendung. Soz.-Und Praventivmedizin 1999, 44, 55–64. [Google Scholar] [CrossRef]
- Metz, L.; Thivel, D.; Peirrera, B.; Richard, R.; Julian, V.; Duclos, M. A new equation based on the 6-min walking test to predict VO2peak in women with obesity. Disabil. Rehabil. 2018, 40, 1702–1707. [Google Scholar] [CrossRef]
- DeBoer, M.D.; Filipp, S.L.; Gurka, M.J. Use of a Metabolic Syndrome Severity Z Score to Track Risk During Treatment of Prediabetes: An Analysis of the Diabetes Prevention Program. Diabetes Care 2018, 41, 2421–2430. [Google Scholar] [CrossRef]
- Keskin, M.; Kurtoglu, S.; Kendirci, M.; Atabek, M.E.; Yazici, C. Homeostasis model assessment is more reliable than the fasting glucose/insulin ratio and quantitative insulin sensitivity check index for assessing insulin resistance among obese children and adolescents. Pediatrics 2005, 115, e500–e503. [Google Scholar] [CrossRef]
- Wang, Q.; Wang, J.; Lin, H.; Huo, X.; Zhu, Q.; Zhang, M. Relationship between fat mass and obesity-associated gene expression and type 2 diabetes mellitus severity. Exp. Ther. Med. 2018, 15, 2917–2921. [Google Scholar] [CrossRef]
- Lee, J.; Kim, M.-H.; Jang, J.-Y.; Oh, C.-M. Assessment HOMA as a predictor for new onset diabetes mellitus and diabetic complications in non-diabetic adults: A KoGES prospective cohort study. Clin. Diabetes Endocrinol. 2023, 9, 7. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| 2 g CO/Day n = 61 | 4 g CO/Day n = 61 | 2 g CO/Day + LI n = 57 | Placebo n = 58 | p-Value | |
|---|---|---|---|---|---|
| Variables | n (%) | n (%) | n (%) | n (%) | |
| Gender | |||||
| Female | 41 (68) | 42 (69) | 39 (68) | 38 (66) | 0.981 a |
| Male | 20 (32) | 18 (31) | 18 (32) | 20 (34) | |
| Anthropometric | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |
| Age [year] | 54.2 ± 9.6 | 57.3 ± 11.3 | 56.0 ± 9.0 | 54.4 ± 9.4 | 0.265 b |
| BMI [kg/m2] | 34.2 ± 5.4 | 34.4 ± 4.1 | 34.2 ± 6.1 | 34.1 ± 4.3 | 0.990 b |
| WC [cm] | 109 ± 12.6 | 111 ± 10.6 | 110 ± 13.4 | 111 ± 11.2 | 0.815 b |
| Body composition | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |
| Phase angle [°] | 6.0 ± 0.8 | 5.8 ± 0.8 | 6.0 ± 0.7 | 5.8 ± 0.7 | 0.282 b |
| Body fat [%] | 42.4 ± 7.3 | 42.8 ± 7.5 | 41.6 ± 8.0 | 43.0 ± 7.6 | 0.782 b |
| Visceral fat mass [L] | 4.2 ± 2.5 | 4.2 ± 212 | 4.2 ± 2.7 | 4.1 ± 2.2 | 0.994 b |
| Metabolic Syndrome Severity (MetS) Score | |||||
| MetS score (based on BMI) | 0.6 ± 0.6 | 0.6 ± 0.5 | 0.6 ± 0.6 | 0.5 ± 0.5 | 0.931 b |
| MetS score (based on WC) | 0.7 ± 0.8 | 0.6 ± 0.5 | 0.6 ± 0.6 | 0.6 ± 0.5 | 0.845 b |
| 2 g CO/Day | 4 g CO/Day | 2 g CO/Day + LI | Placebo | p-Value Effect Size | |||
|---|---|---|---|---|---|---|---|
| n = 61 | n = 61 | n = 57 | n = 58 | ||||
| Variables | Mean ± SD | At t0 a | Interaction b | ηp2 | |||
| HOMA index [AU] | |||||||
| t0 | 3.9 ± 2.0 | 4.0 ± 2.1 | 4.0 ± 2.0 | 3.8 ± 1.7 | 0.900 | ||
| t12 | 4.0 ± 2.2 | 4.0 ± 2.7 | 3.8 ± 2.2 | 3.9 ± 2.3 | 0.011 * | 0.043 | |
| HbA1c [%] | |||||||
| t0 | 5.6 ± 0.3 | 5.6 ± 0.3 | 5.6 ± 0.3 | 5.7 ± 0.3 | 0.619 | ||
| t12 | 5.6 ± 0.3 | 5.6 ± 0.3 | 5.6 ± 0.3 | 5.7 ± 0.3 | 0.014 * | 0.004 | |
| 2 g CO/Day | 4 g CO/Day | 2 g CO/Day + LI | Placebo | p-Value Effect Size | |||
|---|---|---|---|---|---|---|---|
| n = 61 | n = 61 | n = 57 | n = 58 | ||||
| Variables | Mean ± SD | At t0 a | Interaction b | ηp2 | |||
| Inflammation | |||||||
| CRP [mg/dL] | |||||||
| t0 | 3.1 ± 3.6 | 3.4 ± 7.4 | 3.7 ± 4.6 | 4.4 ± 6.9 | 0.626 | ||
| t12 | 2.8 ± 2.9 | 2.9 ± 3.0 | 3.5 ± 3.3 | 3.6 ± 3.5 | 0.318 | 0.016 | |
| Lipid metabolism | |||||||
| TG [mg/dL] | |||||||
| t0 | 151 ± 70.7 | 146 ± 68.2 | 140 ± 57.9 | 128 ± 64.9 | 0.176 | ||
| t12 | 139 ± 65.0 | 141 ± 61.8 | 133 ± 57.2 | 136 ± 61.2 | 0.092 | 0.027 | |
| TC [mg/dL] | |||||||
| t0 | 232 ± 43.0 | 227 ± 37.2 | 238 ± 48.7 | 226 ± 43.5 | 0.470 | ||
| t12 | 232 ± 43.4 | 229 ± 43.2 | 231 ± 42.7 | 227 ± 46.1 | 0.147 | 0.023 | |
| HDL-C [mg/dL] | |||||||
| t0 | 57.5 ± 11.9 | 58.7 ± 13.9 | 61.5 ± 11.6 | 59.8 ± 12.3 | 0.154 | ||
| t12 | 56.2 ± 11.6 | 57.7 ± 14.6 | 58.8 ± 11.5 | 57.8 ± 12.0 | 0.425 | 0.012 | |
| LDL-C [mg/dL] | |||||||
| t0 | 148 ± 30.2 | 142 ± 27.1 | 151 ± 36.1 | 142 ± 31.6 | 0.426 | ||
| t12 | 148 ± 32.7 | 140 ± 30.9 | 145 ± 31.0 | 142 ± 34.1 | 0.256 | 0.017 | |
| Components | g/ 100 g CO | mg/ 2 g CO | mg/ 4 g CO |
|---|---|---|---|
| MUFA | 9.7 | 194 | 388 |
| PUFA | 26.2 | 524 | 1048 |
| n3 PUFAs | 25.0 | 500 | 1000 |
| ALA | 1.4 | 28 | 56 |
| SDA | 8.4 | 168 | 336 |
| EPA | 6.9 | 138 | 276 |
| DHA | 6.4 | 128 | 256 |
| n6 PUFAs | 1.1 | 22 | 44 |
| LA | 0.7 | 14 | 28 |
| ARA | 0.2 | 4 | 8 |
| Fatty alcohols | 28.8 | 576 | 1152 |
| Sterols | 0.35 | 7 | 14 |
| Astaxanthin | 0.1 | 2 | 4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kerlikowsky, F.; Bartsch, M.; Jonas, W.; Hahn, A.; Schuchardt, J.P. Calanus Oil and Lifestyle Interventions Improve Glucose Homeostasis in Obese Subjects with Insulin Resistance. Mar. Drugs 2025, 23, 139. https://doi.org/10.3390/md23040139
Kerlikowsky F, Bartsch M, Jonas W, Hahn A, Schuchardt JP. Calanus Oil and Lifestyle Interventions Improve Glucose Homeostasis in Obese Subjects with Insulin Resistance. Marine Drugs. 2025; 23(4):139. https://doi.org/10.3390/md23040139
Chicago/Turabian StyleKerlikowsky, Felix, Madeline Bartsch, Wiebke Jonas, Andreas Hahn, and Jan Philipp Schuchardt. 2025. "Calanus Oil and Lifestyle Interventions Improve Glucose Homeostasis in Obese Subjects with Insulin Resistance" Marine Drugs 23, no. 4: 139. https://doi.org/10.3390/md23040139
APA StyleKerlikowsky, F., Bartsch, M., Jonas, W., Hahn, A., & Schuchardt, J. P. (2025). Calanus Oil and Lifestyle Interventions Improve Glucose Homeostasis in Obese Subjects with Insulin Resistance. Marine Drugs, 23(4), 139. https://doi.org/10.3390/md23040139