
Potential Use of 3D CORAGRAF-Loaded PDGF-BB in PLGA Microsphere Seeded Mesenchymal Stromal Cells in Enhancing the Repair of Calvaria Critical-Size Bone Defect in Rat Model

 ,
, {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Results
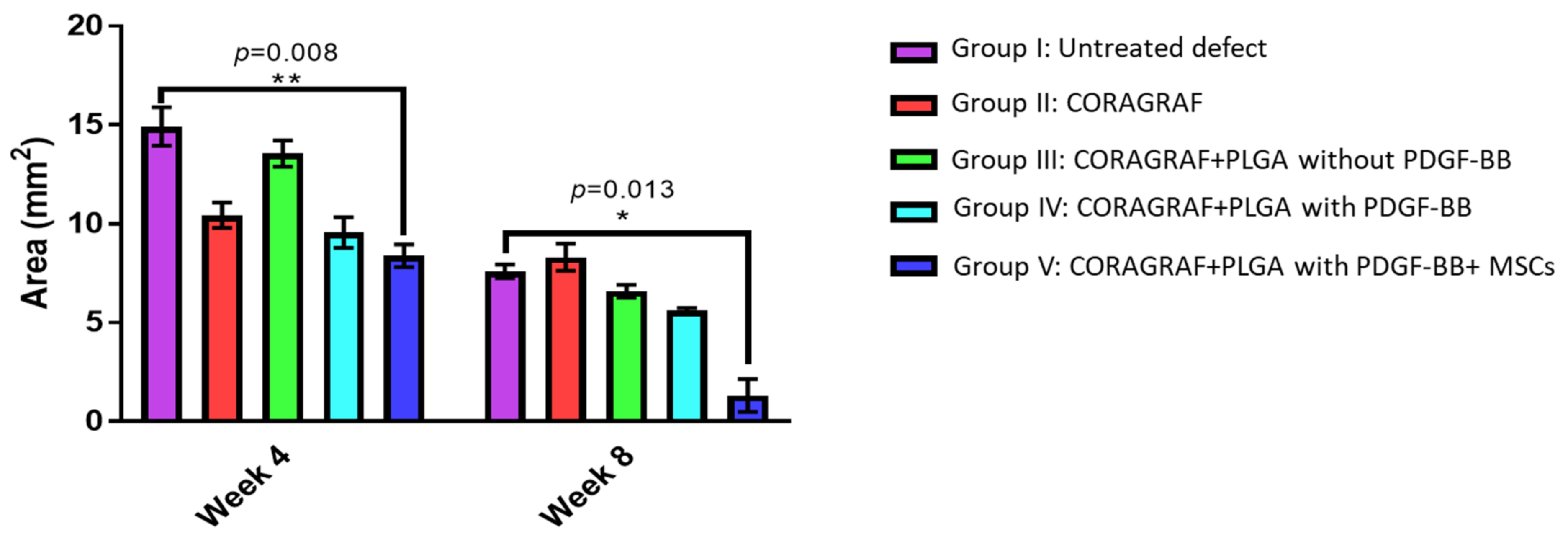
2.1. Micro-CT Analysis
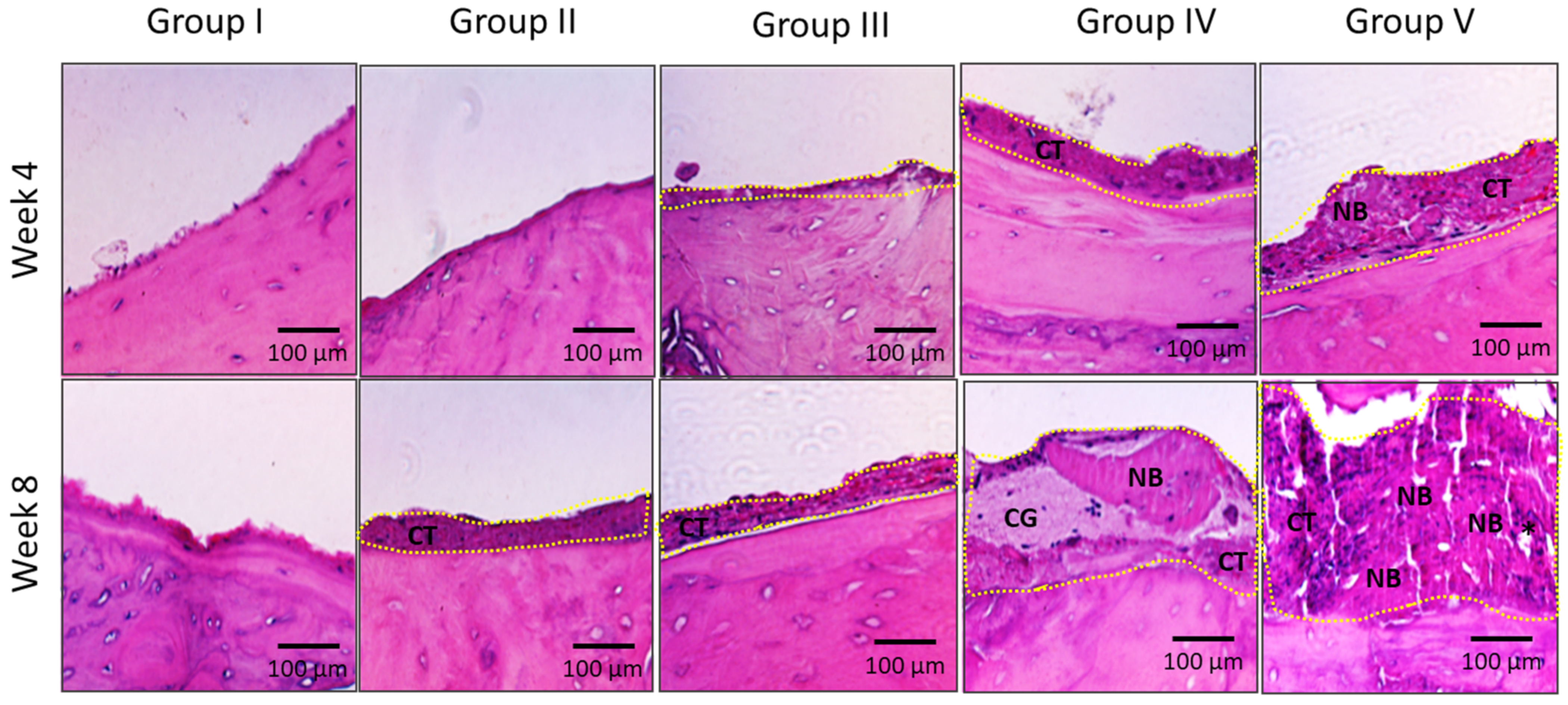
2.2. Histological Analysis of Bone Regeneration
3. Discussion
4. Materials and Methods
4.1. Isolation and Culture of Rat Bone Marrow-Derived Mesenchymal Stromal Cells
4.2. Scaffold Fabrication, Cell Seeding and Culture
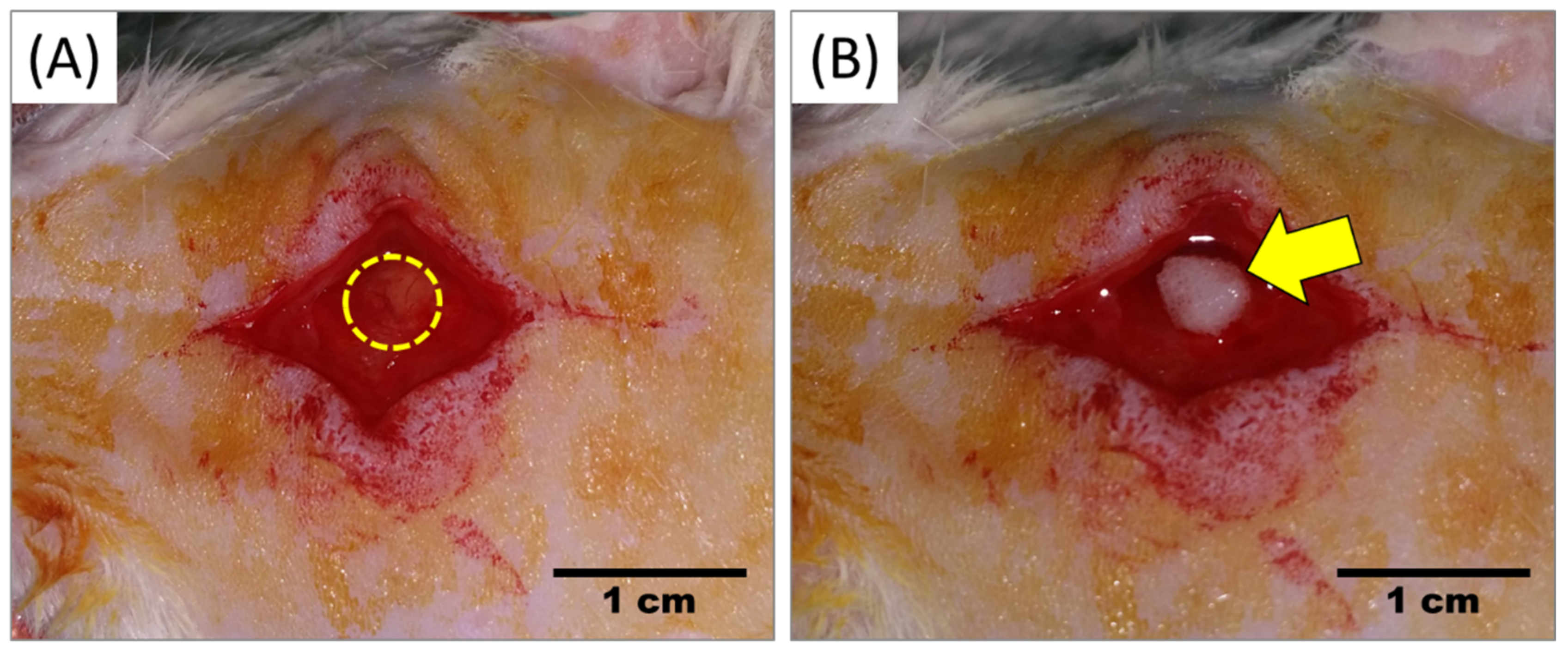
4.3. Creation of Calvaria Critical-Size Defect
4.4. Transplantation of Scaffold
4.5. Microcomputed Tomography (Micro-CT)
4.6. Histological Assessment of Bone Regeneration Using Haematoxylin and Eosin
4.7. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Gaihre, B.; Uswatta, S.; Jayasuriya, A.C. Reconstruction of Craniomaxillofacial Bone Defects Using Tissue-Engineering Strategies with Injectable and Non-Injectable Scaffolds. J. Funct. Biomater. 2017, 8, 49. [Google Scholar] [CrossRef] [PubMed]
- Gomes, M.E.; Holtorf, H.L.; Reis, R.L.; Mikos, A.G. Influence of the porosity of starch-based fiber mesh scaffolds on the proliferation and osteogenic differentiation of bone marrow stromal cells cultured in a flow perfusion bioreactor. Tissue Eng. 2006, 12, 801–809. [Google Scholar] [CrossRef] [PubMed]
- Kübler, N.; Michel, C.; Zöller, J.; Bill, J.; Mühling, J.; Reuther, J. Repair of human skull defects using osteoinductive bone alloimplants. J. Craniomaxillofac. Surg. 1995, 23, 337–346. [Google Scholar] [CrossRef]
- Eppley, B.L.; Pietrzak, W.S.; Blanton, M.W. Allograft and alloplastic bone substitutes: A review of science and technology for the craniomaxillofacial surgeon. J. Craniofac. Surg. 2005, 16, 981–989. [Google Scholar] [CrossRef] [PubMed]
- Ng, V.Y. Risk of disease transmission with bone allograft. Orthopedics 2012, 35, 679–681. [Google Scholar] [CrossRef]
- Pilipchuk, S.P.; Plonka, A.B.; Monje, A.; Taut, A.D.; Lanis, A.; Kang, B.; Giannobile, W.V. Tissue engineering for bone regeneration and osseointegration in the oral cavity. Dent. Mater. 2015, 31, 317–338. [Google Scholar] [CrossRef]
- Bauer, T.W.; Muschler, G.F. Bone graft materials. An overview of the basic science. Clin. Orthop. Relat. Res. 2000, 371, 10–27. [Google Scholar] [CrossRef]
- Tămăşan, M.; Ozyegin, L.S.; Oktar, F.N.; Simon, V. Characterization of calcium phosphate powders originating from Phyllacanthus imperialis and Trochidae Infundibulum concavus marine shells. Mater. Sci. Eng. C Mater. Biol. Appl. 2013, 33, 2569–2577. [Google Scholar] [CrossRef]
- Lee, J.H.; Ryu, M.Y.; Baek, H.R.; Lee, K.M.; Seo, J.H.; Lee, H.K. Fabrication and evaluation of porous beta-tricalcium phosphate/hydroxyapatite (60/40) composite as a bone graft extender using rat calvarial bone defect model. Sci. World J. 2013, 2013, 481789. [Google Scholar] [CrossRef]
- Szpalski, C.; Barr, J.; Wetterau, M.; Saadeh, P.B.; Warren, S.M. Cranial bone defects: Current and future strategies. Neurosurg. Focus 2010, 29, E8. [Google Scholar] [CrossRef] [Green Version]
- Macha, I.J.; Cazalbou, S.; Ben-Nissan, B.; Harvey, K.L.; Milthorpe, B. Marine structure derived calcium phosphate-polymer biocomposites for local antibiotic delivery. Mar. Drugs 2015, 13, 666–680. [Google Scholar] [CrossRef]
- Ben-Nissan, B.; Milev, A.; Vago, R. Morphology of sol-gel derived nano-coated coralline hydroxyapatite. Biomaterials 2004, 25, 4971–4975. [Google Scholar] [CrossRef]
- Mohan, S.; Raghavendran, H.B.; Karunanithi, P.; Murali, M.R.; Naveen, S.V.; Talebian, S.; Mehrali, M.; Mehrali, M.; Natarajan, E.; Chan, C.K.; et al. Incorporation of Human-Platelet-Derived Growth Factor-BB Encapsulated Poly(lactic-co-glycolic acid) Microspheres into 3D CORAGRAF Enhances Osteogenic Differentiation of Mesenchymal Stromal Cells. ACS Appl. Mater. Interfaces 2017, 9, 9291–9303. [Google Scholar] [CrossRef]
- Beck, L., Jr.; D’Amore, P.A. Vascular development: Cellular and molecular regulation. FASEB J. 1997, 11, 365–373. [Google Scholar] [CrossRef]
- Silva de Oliveira, J.C.; Okamoto, R.; Sonoda, C.K.; Poi, W.R.; Garcia, I.R., Jr.; Luvizuto, E.R. Evaluation of the Osteoinductive Effect of PDGF-BB Associated with Different Carriers in Bone Regeneration in Bone Surgical Defects in Rats. Implant Dent. 2017, 26, 559–566. [Google Scholar] [CrossRef]
- Nagai, N.; Kumasaka, N.; Kawashima, T.; Kaji, H.; Nishizawa, M.; Abe, T. Preparation and characterization of collagen microspheres for sustained release of VEGF. J. Mater. Sci. Mater. Med. 2010, 21, 1891–1898. [Google Scholar] [CrossRef]
- Berthold, A.; Cremer, K.; Kreuter, J. Collagen microparticles: Carriers for glucocorticosteroids. Eur. J. Pharm. Biopharm. 1998, 45, 23–29. [Google Scholar] [CrossRef]
- Hwang, S.M.; Kim, D.D.; Chung, S.J.; Shim, C.K. Delivery of ofloxacin to the lung and alveolar macrophages via hyaluronan microspheres for the treatment of tuberculosis. J. Control. Release 2008, 129, 100–106. [Google Scholar] [CrossRef]
- Mathew, S.T.; Devi, S.G.; Kv, S. Formulation and evaluation of ketorolac tromethamine-loaded albumin microspheres for potential intramuscular administration. AAPS PharmSciTech 2007, 8, 14. [Google Scholar] [CrossRef]
- Mirdailami, O.; Khoshayand, M.R.; Soleimani, M.; Dinarvand, R.; Atyabi, F. Release optimization of epidermal growth factor from PLGA microparticles. Pharm. Dev. Technol. 2014, 19, 539–547. [Google Scholar] [CrossRef]
- Allison, S.D. Effect of structural relaxation on the preparation and drug release behavior of poly(lactic-co-glycolic)acid microparticle drug delivery systems. J. Pharm. Sci. 2008, 97, 2022–2035. [Google Scholar] [CrossRef]
- Mohamed, F.; van der Walle, C.F. Engineering biodegradable polyester particles with specific drug targeting and drug release properties. J. Pharm. Sci. 2008, 97, 71–87. [Google Scholar] [CrossRef]
- Chauhan, N.; Singh, Y. Engineered Polymeric Materials/Nanomaterials for Growth Factor/Drug Delivery in Bone Tissue Engineering Applications. In Nanoscale Engineering of Biomaterials: Properties and Applications; Pandey, L.M., Hasan, A., Eds.; Springer Nature: Singapore, 2022; pp. 349–396. [Google Scholar] [CrossRef]
- Souza, F.F.P.; Pérez-Guerrero, J.A.; Gomes, M.J.P.; Cavalcante, F.L.; Souza Filho, M.S.M.; Castro, S., II. Development and characterization of poultry collagen-based hybrid hydrogels for bone regeneration. Acta Cir. Bras. 2022, 37, e370302. [Google Scholar] [CrossRef] [PubMed]
- Nkenke, E.; Radespiel-Tröger, M.; Wiltfang, J.; Schultze-Mosgau, S.; Winkler, G.; Neukam, F.W. Morbidity of harvesting of retromolar bone grafts: A prospective study. Clin. Oral Implants Res. 2002, 13, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Xie, H.; Cui, Z.; Wang, L.; Xia, Z.; Hu, Y.; Xian, L.; Li, C.; Xie, L.; Crane, J.; Wan, M.; et al. PDGF-BB secreted by preosteoclasts induces angiogenesis during coupling with osteogenesis. Nat. Med. 2014, 20, 1270–1278. [Google Scholar] [CrossRef] [PubMed]
- Li, C.; Guo, C.; Fitzpatrick, V.; Ibrahim, A.; Zwierstra, M.J.; Hanna, P.; Lechtig, A.; Nazarian, A.; Lin, S.J.; Kaplan, D.L. Design of biodegradable, implantable devices towards clinical translation. Nat. Rev. Mater. 2020, 5, 61–81. [Google Scholar] [CrossRef]
- Kapoor, D.N.; Bhatia, A.; Kaur, R.; Sharma, R.; Kaur, G.; Dhawan, S. PLGA: A unique polymer for drug delivery. Ther. Deliv. 2015, 6, 41–58. [Google Scholar] [CrossRef] [PubMed]
- Hines, D.J.; Kaplan, D.L. Poly(lactic-co-glycolic) acid-controlled-release systems: Experimental and modeling insights. Crit. Rev. Ther. Drug Carrier Syst. 2013, 30, 257–276. [Google Scholar] [CrossRef]
- Sartoris, D.J.; Holmes, R.E.; Bucholz, R.W.; Mooney, V.; Resnick, D. Coralline hydroxyapatite bone-graft substitutes in a canine diaphyseal defect model. Radiographic-histometric correlation. Investig. Radiol. 1987, 22, 590–596. [Google Scholar] [CrossRef]
- Elsinger, E.C.; Leal, L. Coralline hydroxyapatite bone graft substitutes. J. Foot Ankle Surg. 1996, 35, 396–399. [Google Scholar] [CrossRef]
- Preidler, K.W.; Lemperle, S.M.; Holmes, R.E.; Calhoun, C.J.; Shors, E.C.; Brossmann, J.; Sartoris, D.J. Coralline hydroxyapatite bone graft substitutes. Evaluation of bone density with dual energy X-ray absorptiometry. Investig. Radiol. 1996, 31, 716–723. [Google Scholar] [CrossRef]
- Tsuchiya, A.; Sotome, S.; Asou, Y.; Kikuchi, M.; Koyama, Y.; Ogawa, T.; Tanaka, J.; Shinomiya, K. Effects of pore size and implant volume of porous hydroxyapatite/collagen (HAp/Col) on bone formation in a rabbit bone defect model. J. Med. Dent. Sci. 2008, 55, 91–99. [Google Scholar]
- Simunovic, F.; Finkenzeller, G. Vascularization Strategies in Bone Tissue Engineering. Cells 2021, 10, 1749. [Google Scholar] [CrossRef]
- Feehan, J.; Nurgali, K.; Apostolopoulos, V.; Al Saedi, A.; Duque, G. Circulating osteogenic precursor cells: Building bone from blood. eBioMedicine 2019, 39, 603–611. [Google Scholar] [CrossRef]
- Cenni, E.; Ciapetti, G.; Granchi, D.; Fotia, C.; Perut, F.; Giunti, A.; Baldini, N. Endothelial cells incubated with platelet-rich plasma express PDGF-B and ICAM-1 and induce bone marrow stromal cell migration. J. Orthop. Res. 2009, 27, 1493–1498. [Google Scholar] [CrossRef]
- Murphy, C.M.; O’Brien, F.J.; Little, D.G.; Schindeler, A. Cell-scaffold interactions in the bone tissue engineering triad. Eur. Cells Mater. 2013, 26, 120–132. [Google Scholar] [CrossRef]
- Lima, C.J.d.; Silva, I.I.C.d.; Bittencourt, R.C.; Takamori, E.R.; Lenharo, A.; Granjeiro, J.M. Análise histológica de uma membrana colágena de submucosa intestinal suína. ImplantNews 2010, 7, 515–520. [Google Scholar]
- Lomelino, R.d.O.; Castro, S., II; Linhares, A.B.; Alves, G.G.; Santos, S.R.; Gameiro, V.S.; Rossi, A.M.; Granjeiro, J.M. The association of human primary bone cells with biphasic calcium phosphate (βTCP/HA 70:30) granules increases bone repair. J. Mater. Sci. Mater. Med. 2012, 23, 781–788. [Google Scholar] [CrossRef]
- Shanbhag, S.; Suliman, S.; Mohamed-Ahmed, S.; Kampleitner, C.; Hassan, M.N.; Heimel, P.; Dobsak, T.; Tangl, S.; Bolstad, A.I.; Mustafa, K. Bone regeneration in rat calvarial defects using dissociated or spheroid mesenchymal stromal cells in scaffold-hydrogel constructs. Stem Cell. Res. Ther. 2021, 12, 575. [Google Scholar] [CrossRef]
- Hung, B.P.; Hutton, D.L.; Kozielski, K.L.; Bishop, C.J.; Naved, B.; Green, J.J.; Caplan, A.I.; Gimble, J.M.; Dorafshar, A.H.; Grayson, W.L. Platelet-Derived Growth Factor BB Enhances Osteogenesis of Adipose-Derived but Not Bone Marrow-Derived Mesenchymal Stromal/Stem Cells. Stem Cells 2015, 33, 2773–2784. [Google Scholar] [CrossRef]
- Zhang, M.; Yu, W.; Niibe, K.; Zhang, W.; Egusa, H.; Tang, T.; Jiang, X. The Effects of Platelet-Derived Growth Factor-BB on Bone Marrow Stromal Cell-Mediated Vascularized Bone Regeneration. Stem Cells Int. 2018, 2018, 3272098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Krebsbach, P.H.; Mankani, M.H.; Satomura, K.; Kuznetsov, S.A.; Robey, P.G. Repair of craniotomy defects using bone marrow stromal cells. Transplantation 1998, 66, 1272–1278. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; He, X.T.; Yin, Y.; Wu, R.X.; Tian, B.M.; Chen, F.M. Administration of signalling molecules dictates stem cell homing for in situ regeneration. J. Cell. Mol. Med. 2017, 21, 3162–3177. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mohan, S.; Karunanithi, P.; Raman Murali, M.; Anwar Ayob, K.; Megala, J.; Genasan, K.; Kamarul, T.; Balaji Raghavendran, H.R. Potential Use of 3D CORAGRAF-Loaded PDGF-BB in PLGA Microsphere Seeded Mesenchymal Stromal Cells in Enhancing the Repair of Calvaria Critical-Size Bone Defect in Rat Model. Mar. Drugs 2022, 20, 561. https://doi.org/10.3390/md20090561
Mohan S, Karunanithi P, Raman Murali M, Anwar Ayob K, Megala J, Genasan K, Kamarul T, Balaji Raghavendran HR. Potential Use of 3D CORAGRAF-Loaded PDGF-BB in PLGA Microsphere Seeded Mesenchymal Stromal Cells in Enhancing the Repair of Calvaria Critical-Size Bone Defect in Rat Model. Marine Drugs. 2022; 20(9):561. https://doi.org/10.3390/md20090561
Chicago/Turabian StyleMohan, Saktiswaren, Puvanan Karunanithi, Malliga Raman Murali, Khairul Anwar Ayob, Jayaraman Megala, Krishnamurithy Genasan, Tunku Kamarul, and Hanumantha Rao Balaji Raghavendran. 2022. "Potential Use of 3D CORAGRAF-Loaded PDGF-BB in PLGA Microsphere Seeded Mesenchymal Stromal Cells in Enhancing the Repair of Calvaria Critical-Size Bone Defect in Rat Model" Marine Drugs 20, no. 9: 561. https://doi.org/10.3390/md20090561
APA StyleMohan, S., Karunanithi, P., Raman Murali, M., Anwar Ayob, K., Megala, J., Genasan, K., Kamarul, T., & Balaji Raghavendran, H. R. (2022). Potential Use of 3D CORAGRAF-Loaded PDGF-BB in PLGA Microsphere Seeded Mesenchymal Stromal Cells in Enhancing the Repair of Calvaria Critical-Size Bone Defect in Rat Model. Marine Drugs, 20(9), 561. https://doi.org/10.3390/md20090561