
Pilot Investigation on p75ICD Expression in Laryngeal Squamous Cell Carcinoma

 ,
,  ,
, 
 , ,
, ,  , , , , , ,
, , , , , ,  ,
, 

Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Method
2.1. Tissue Specimen Collection
2.2. Pathologic Evaluation of the Larynx Surgical Specimens
2.3. Immunofluorescence and Confocal Studies
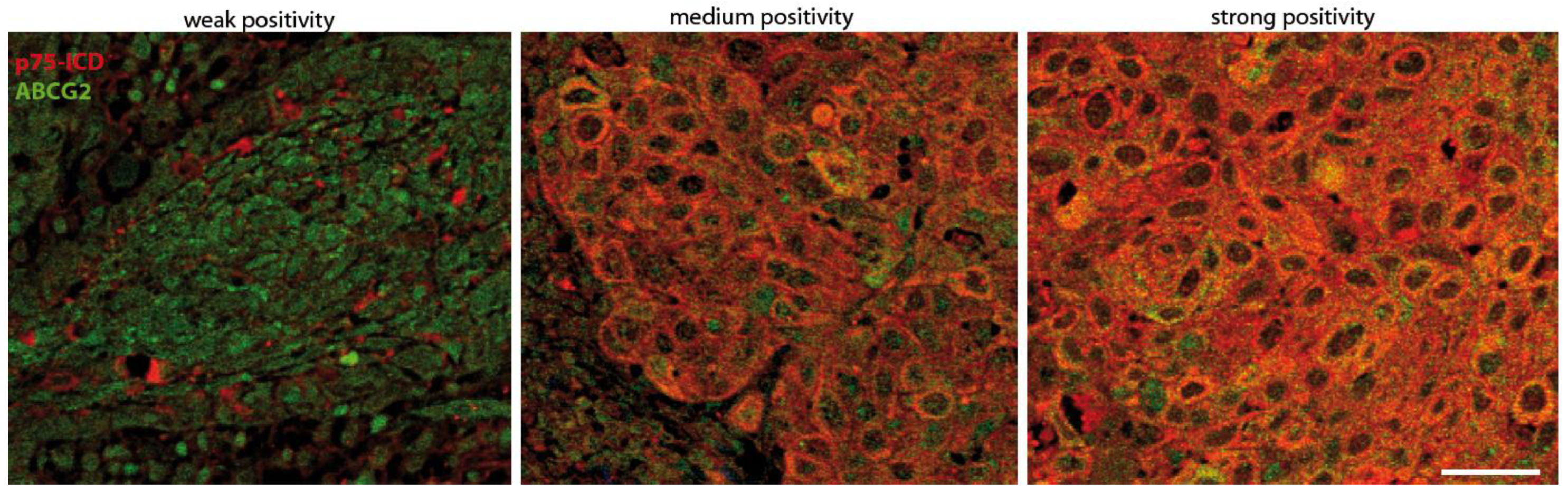
2.4. Pathological Marker Positivity Scoring System
2.5. Western Blotting
3. Results
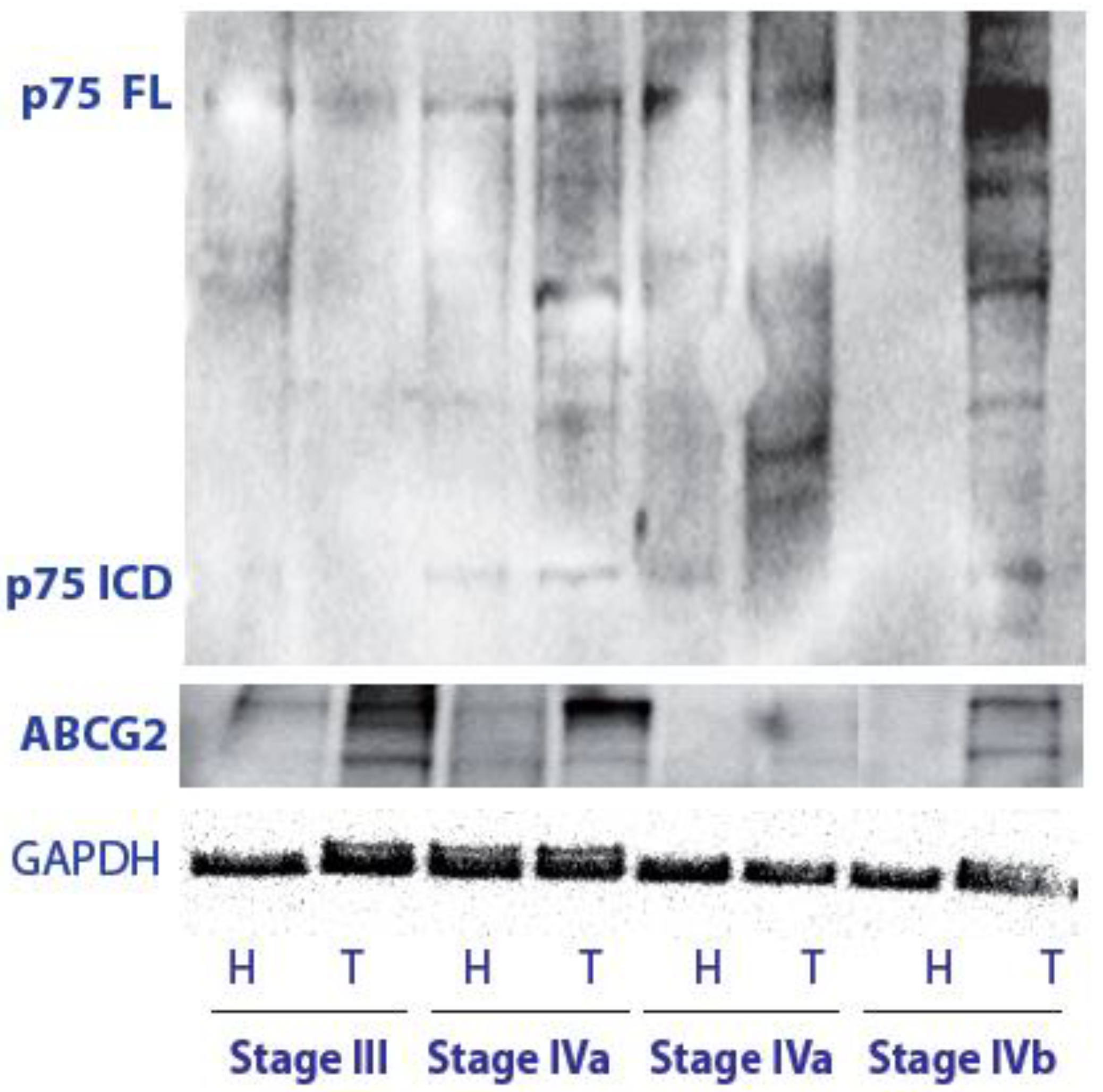
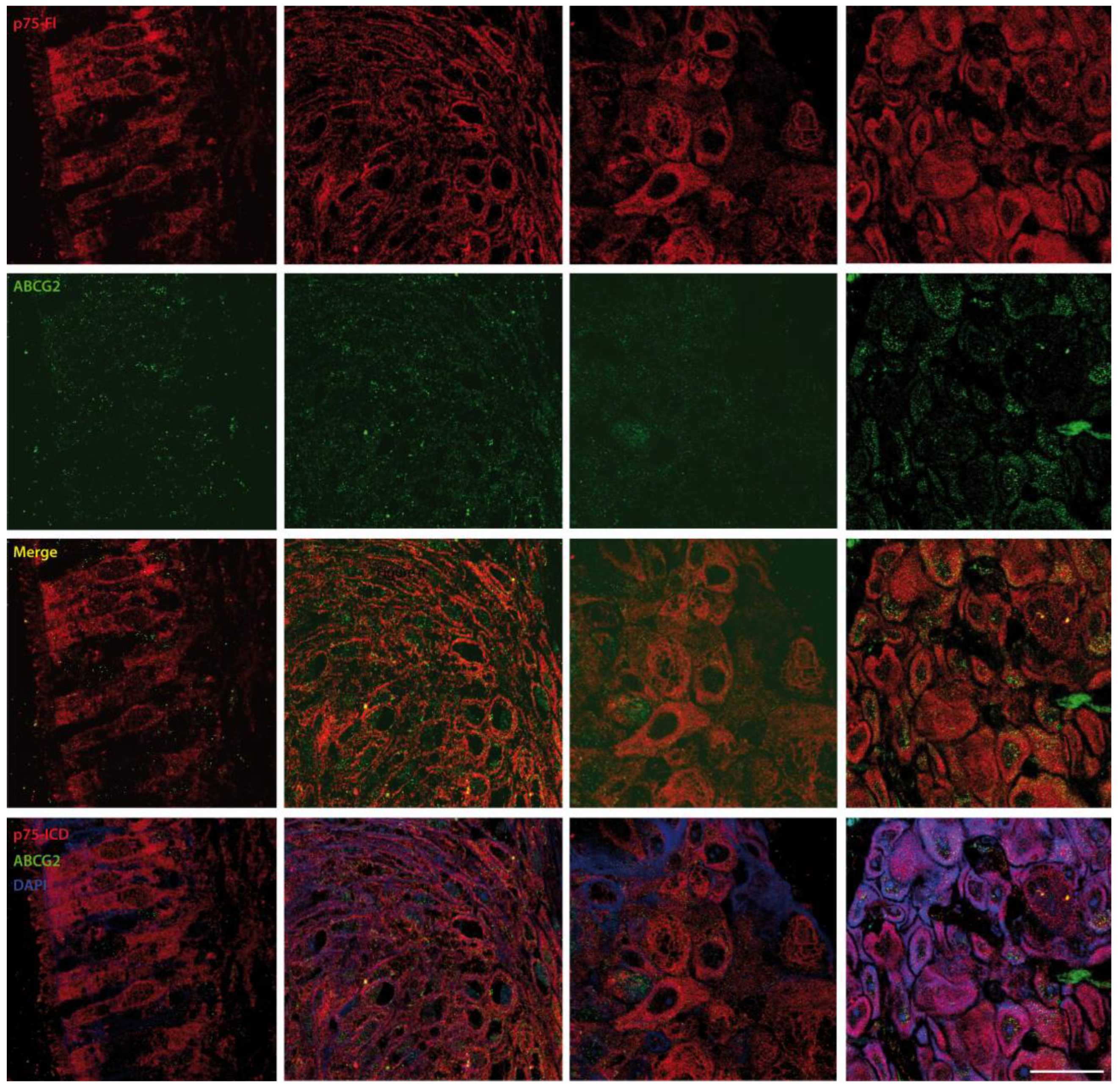
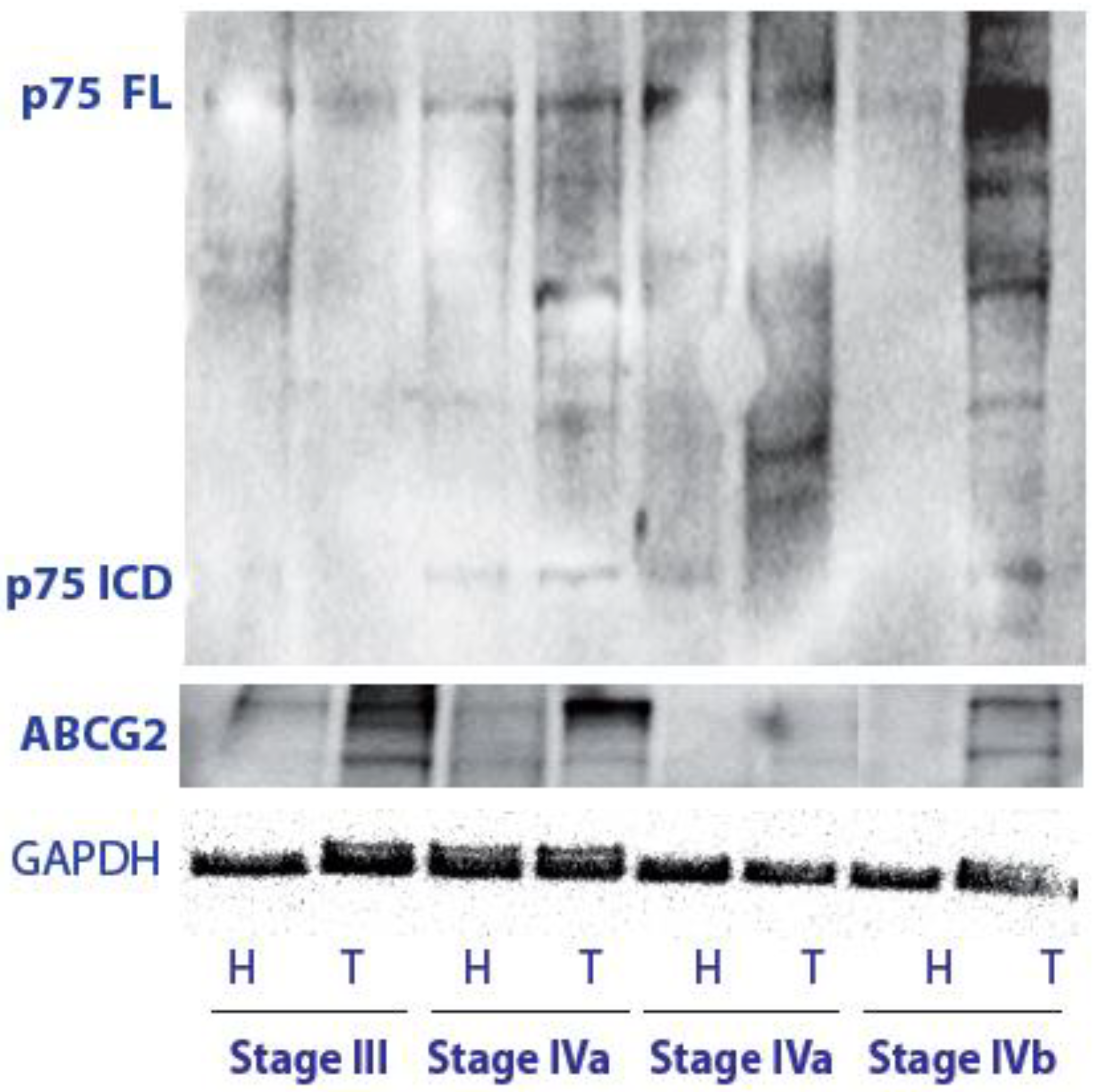
3.1. p75NTR Expression and p75ICD Generation by Regulated Cleavage in LSCC Tissue
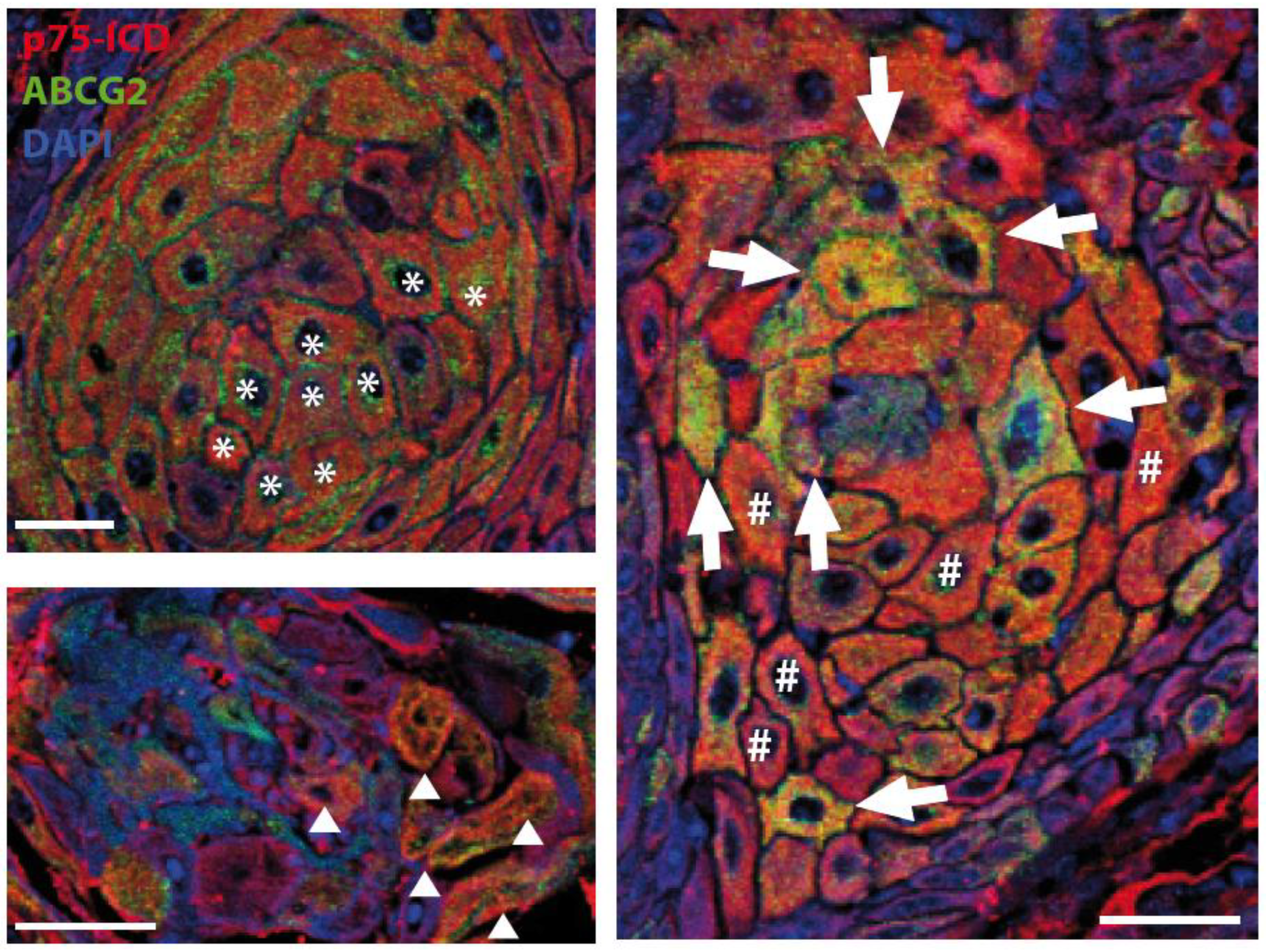
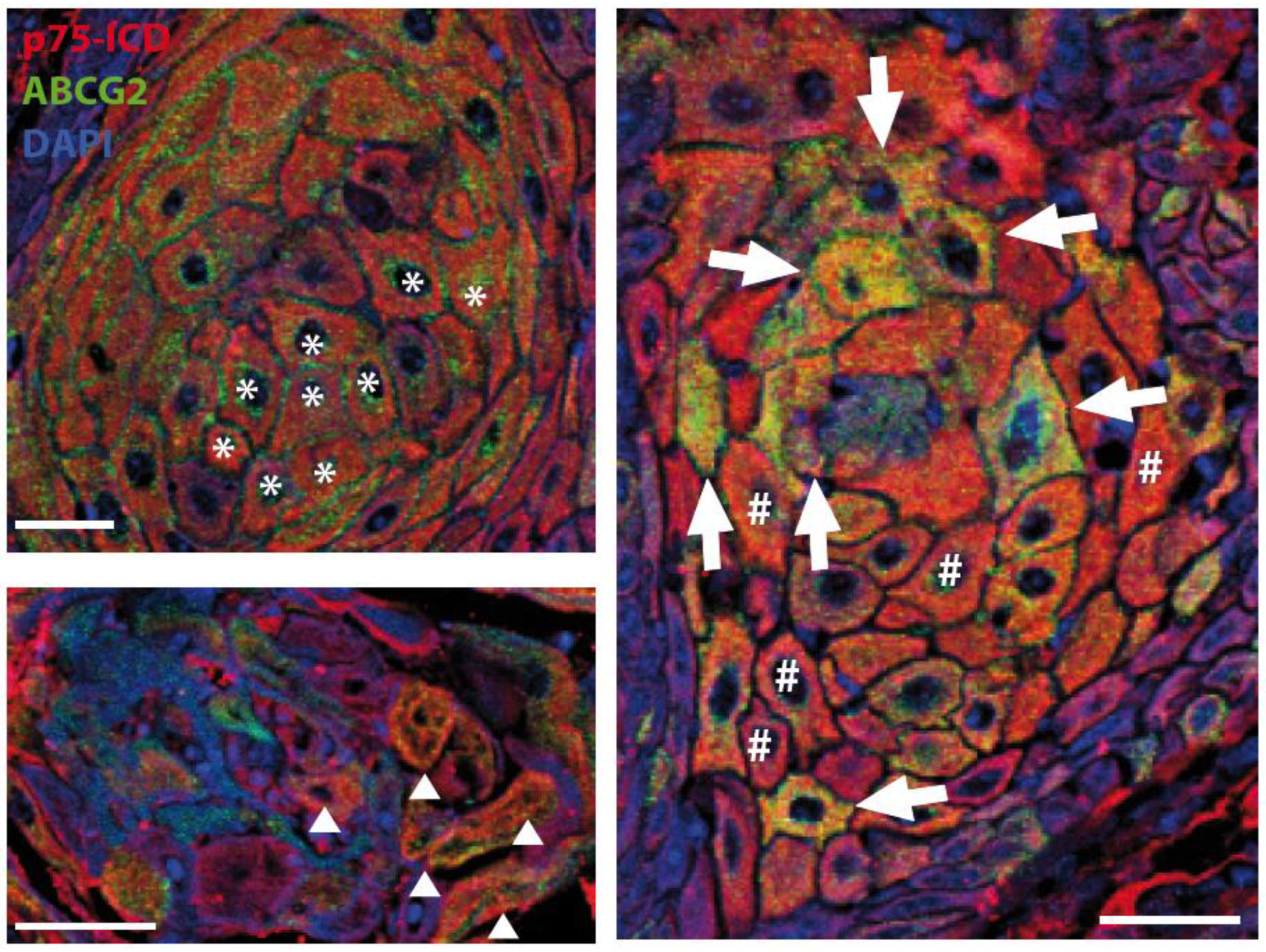
3.2. Preliminary Characterization of the p75ICD and ABCG2 Immunofluorescent Staining Patterns in LSCC Tumor Samples
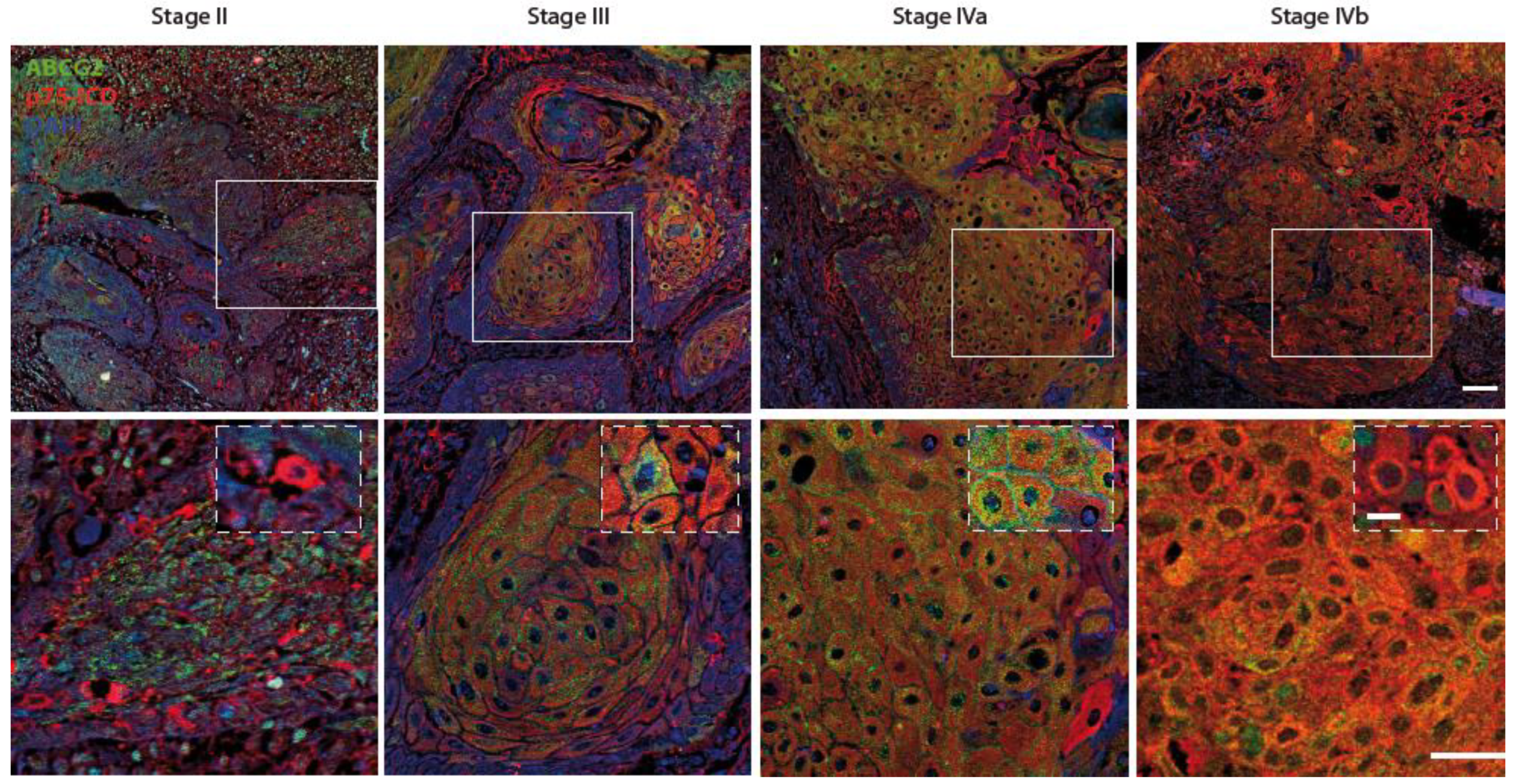
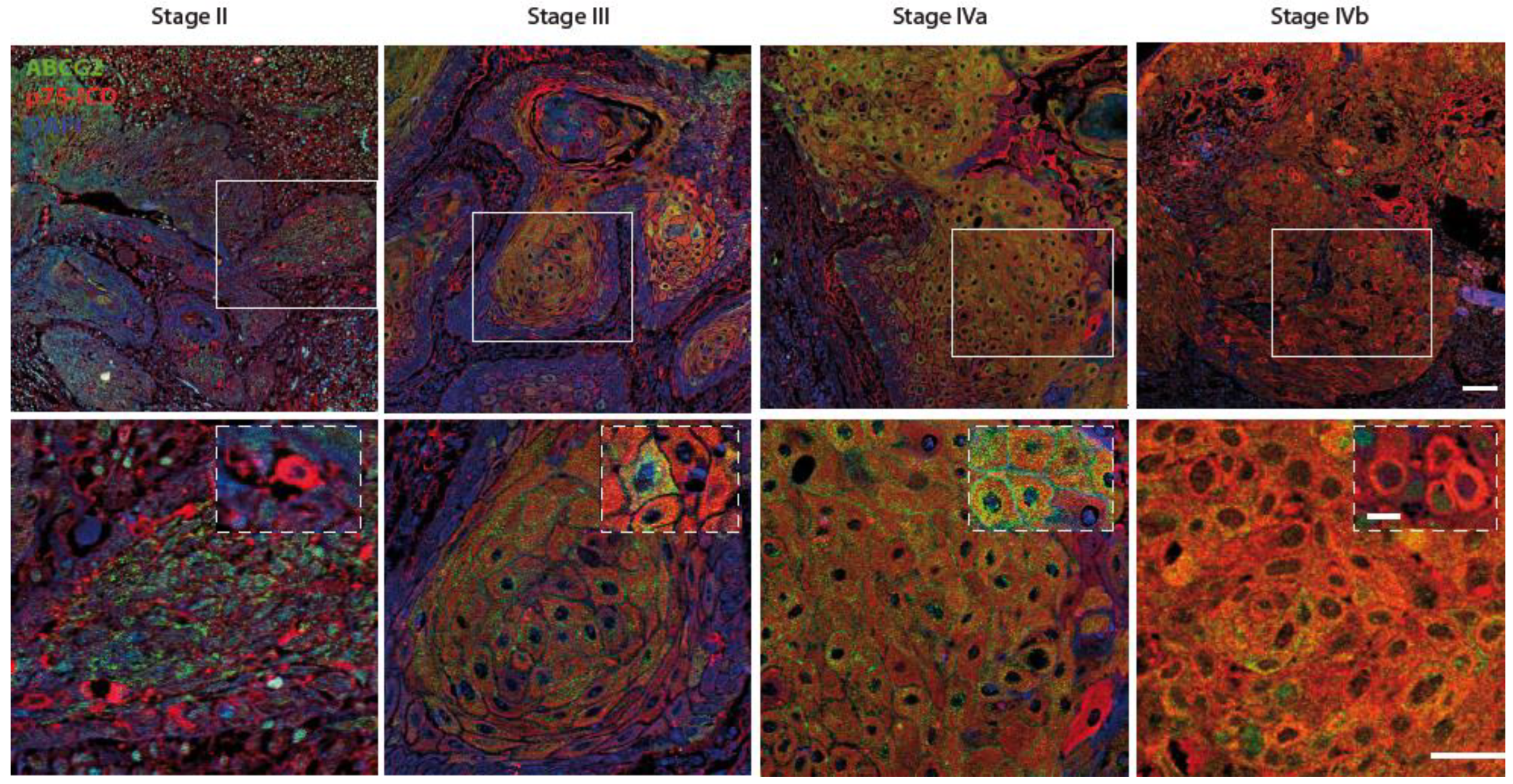
3.3. p75ICD and ABCG2 Distribution in LSCC Tissue at Different Stages
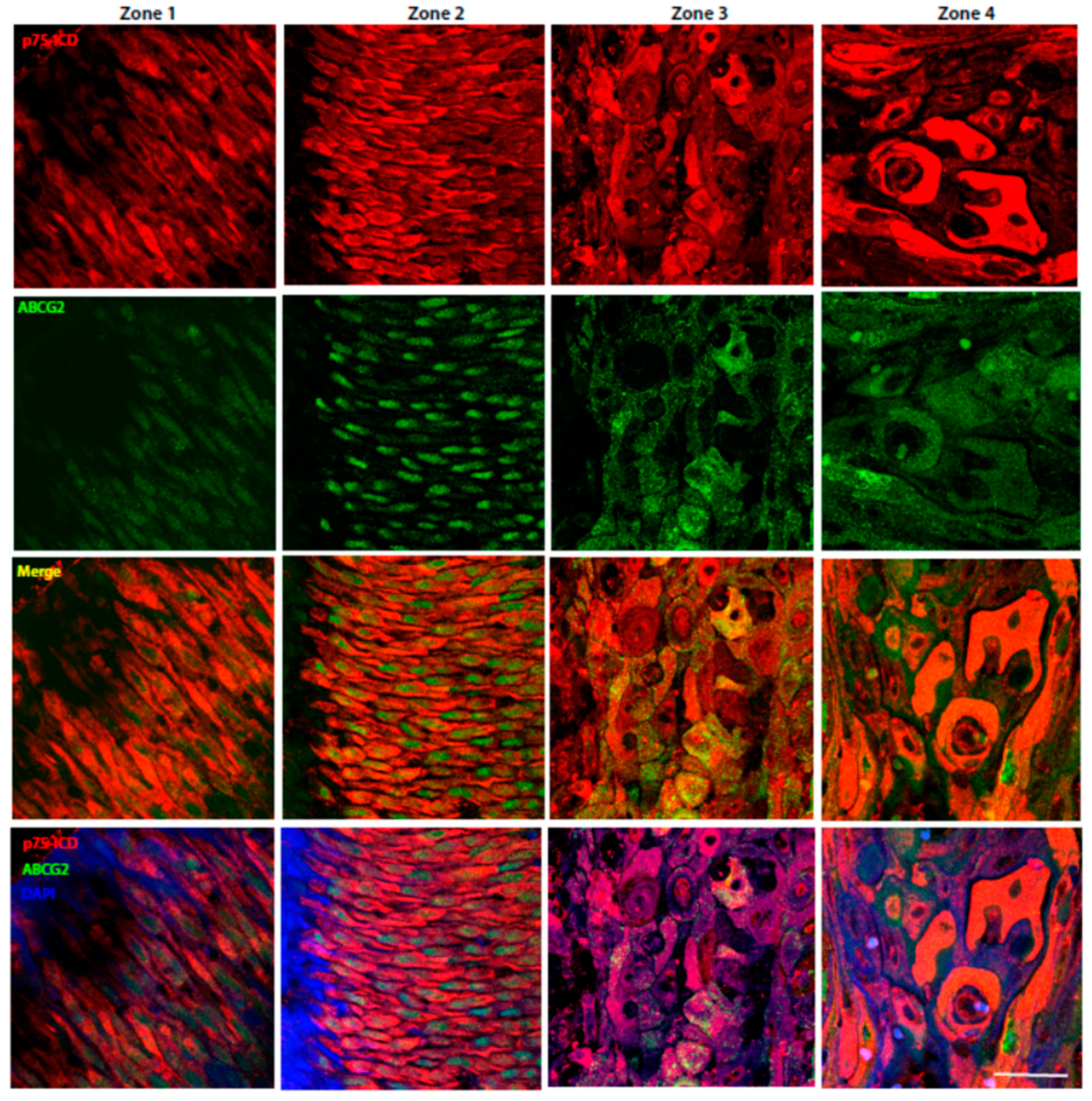
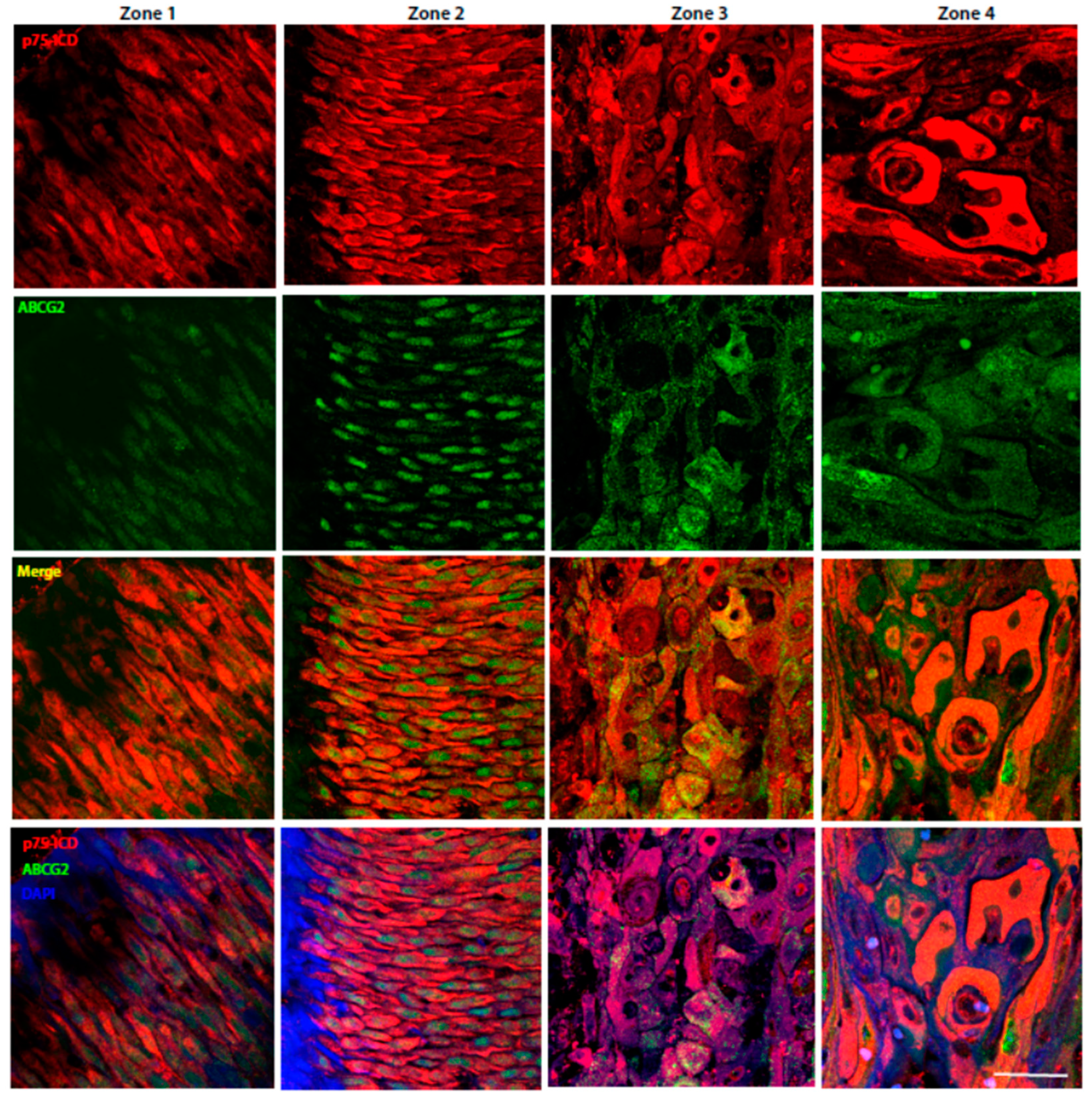
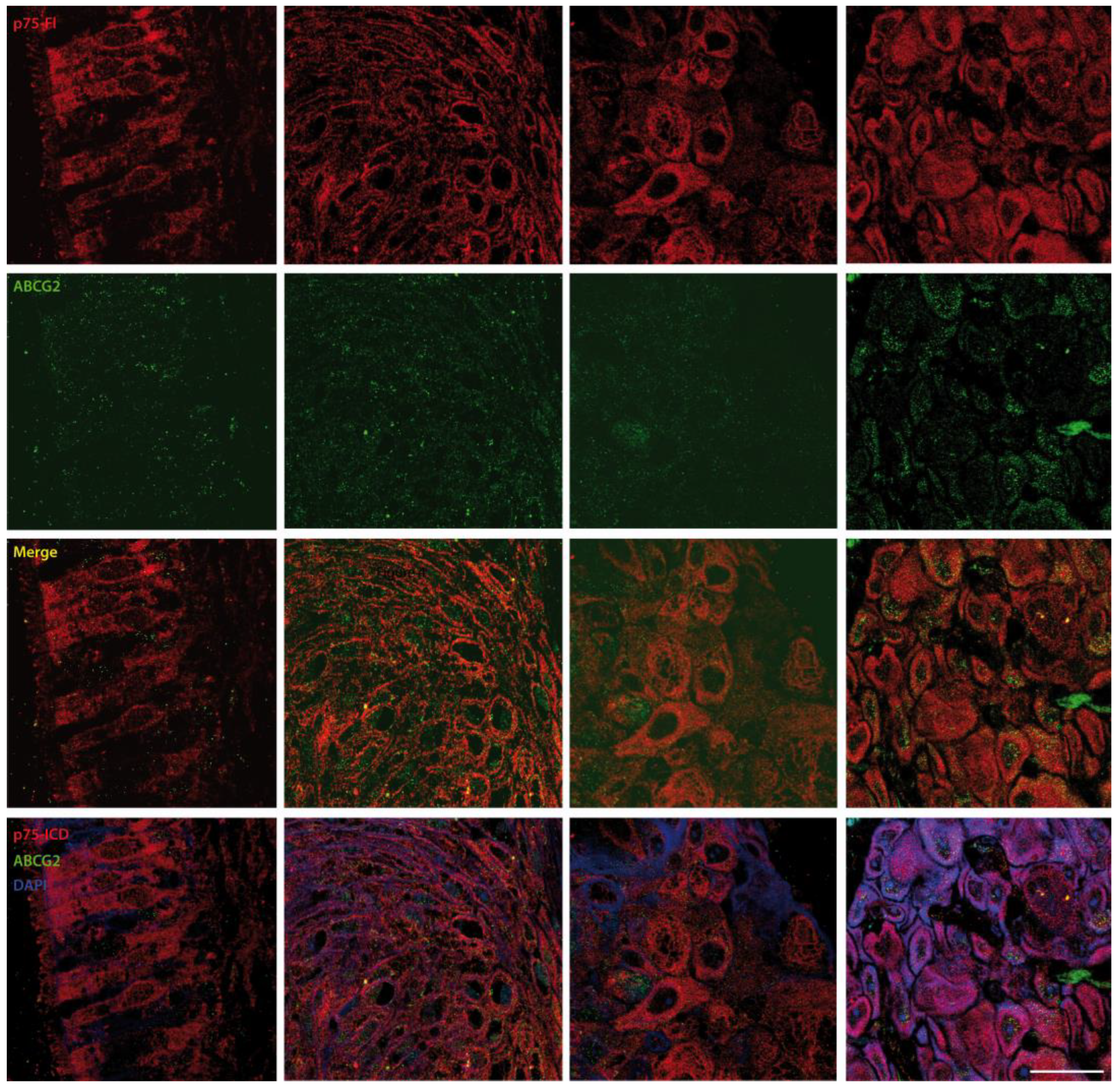
3.4. Characterization of p75NTR and p75ICD Expressions in the Four Different Zones of LSCC Specimens
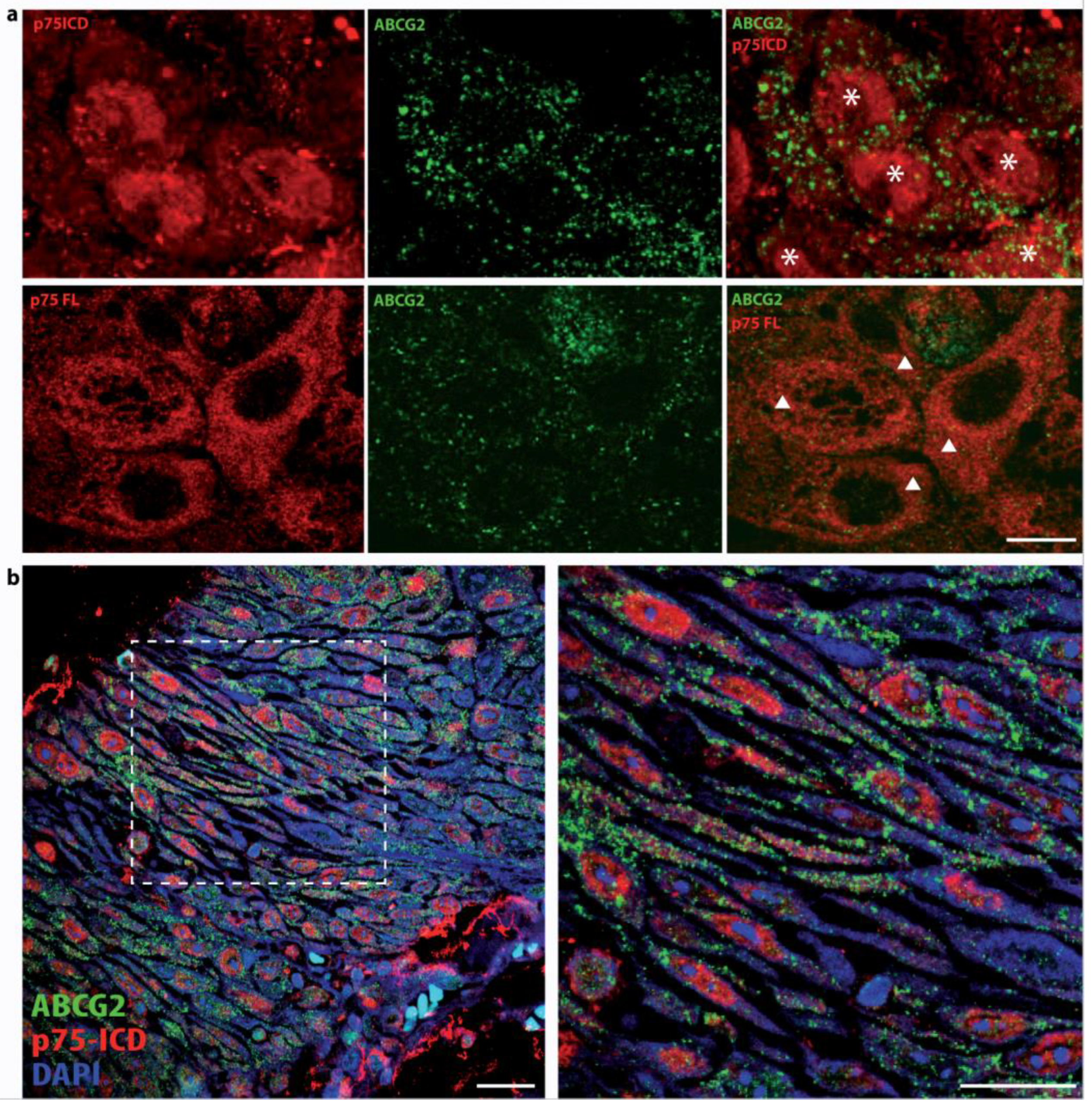
3.5. Differential Intracellular Localization of p75NTR FL and p75ICD in LSCC
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and neck squamous cell carcinoma. Nat. Rev. Dis. Prim. 2020, 6, 92. [Google Scholar] [CrossRef] [PubMed]
- Forastiere, A.A.; Ismaila, N.; Lewin, J.S.; Nathan, C.A.; Adelstein, D.J.; Eisbruch, A.; Fass, G.; Fisher, S.G.; Laurie, S.A.; Le, Q.T.; et al. Use of larynx-preservation strategies in the treatment of laryngeal cancer: American Society of Clinical Oncology clinical practice guideline update. J. Clin. Oncol. 2018, 36, 1143–1169. [Google Scholar] [CrossRef] [PubMed]
- Johnston, A.L.M.; Lun, X.; Rahn, J.J.; Liacini, A.; Wang, L.; Hamilton, M.G.; Parney, I.F.; Hempstead, B.L.; Robbins, S.M.; Forsyth, P.A.; et al. The p75 neurotrophin receptor is a central regulator of glioma invasion. PLoS Biol. 2007, 5, 1723–1737. [Google Scholar] [CrossRef] [PubMed]
- Yamaguchi, T.; Okumura, T.; Hirano, K.; Watanabe, T.; Nagata, T.; Shimada, Y.; Tsukada, K. Detection of circulating tumor cells by p75NTR expression in patients with esophageal cancer. World J. Surg. Oncol. 2016, 14, 40. [Google Scholar] [CrossRef] [Green Version]
- Forsyth, P.A.; Krishna, N.; Lawn, S.; Valadez, J.G.; Qu, X.; Fenstermacher, D.A.; Fournier, M.; Potthast, L.; Chinnaiyan, P.; Gibney, G.T.; et al. p75 neurotrophin receptor cleavage by α- and γ-secretases is required for neurotrophin-mediated proliferation of brain tumor-initiating cells. J. Biol. Chem. 2014, 289, 8067–8085. [Google Scholar] [CrossRef] [Green Version]
- Okumura, T.; Shimada, Y.; Sakurai, T.; Hori, R.; Nagata, T.; Sakai, Y.; Tsukada, K. Abnormal cell proliferation in the p75NTR-positive basal cell compartment of the esophageal epithelium during squamous carcinogenesis. Dis. Esophagus 2015, 28, 634–643. [Google Scholar] [CrossRef]
- Fanburg-Smith, J.C.; Miettinen, M. Low-affinity nerve growth factor receptor (p75) in dermatofibrosarcoma protuberans and other nonneural tumors: A study of 1,150 tumors and fetal and adult normal tissues. Hum. Pathol. 2001, 32, 976–983. [Google Scholar] [CrossRef]
- Zhang, T.; Mi, Z.; Schor, N.F. Role of tyrosine phosphorylation in the antioxidant effects of the p75 neurotrophin receptor. Oxid. Med. Cell. Longev. 2009, 2, 238–246. [Google Scholar] [CrossRef] [Green Version]
- Tong, D.; Sun, J.; Huang, P.; Li, M.; Zhang, F. p75 neurotrophin receptor: A potential surface marker of tongue squamous cell carcinoma stem cells. Mol. Med. Rep. 2017, 15, 2521–2529. [Google Scholar] [CrossRef] [Green Version]
- Murillo-Sauca, O.; Chung, M.K.; Shin, J.H.; Karamboulas, C.; Kwok, S.; Jung, Y.H.; Oakley, R.; Tysome, J.R.; Farnebo, L.O.; Kaplan, M.J.; et al. CD271 is a functional and targetable marker of tumor-initiating cells in head and neck squamous cell carcinoma. Oncotarget 2014, 5, 6854. [Google Scholar] [CrossRef] [Green Version]
- Zhou, X.; Hao, Q.; Liao, P.; Luo, S.; Zhang, M.; Hu, G.; Liu, H.; Zhang, Y.; Cao, B.; Baddoo, M.; et al. Nerve growth factor receptor negates the tumor suppressor p53 as a feedback regulator. eLife 2016, 5, 1–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caponio, V.C.A.; Troiano, G.; Adipietro, I.; Zhurakivska, K.; Arena, C.; Mangieri, D.; Mascitti, M.; Cirillo, N.; Lo Muzio, L. Computational analysis of TP53 mutational landscape unveils key prognostic signatures and distinct pathobiological pathways in head and neck squamous cell cancer. Br. J. Cancer 2020, 123, 1302–1314. [Google Scholar] [CrossRef] [PubMed]
- Shen, D.; Jiang, Y.; Tao, K.; Shen, D.; Jiang, Y.; Tao, K. Expression and clinical significance of p75NTR in esophageal squamous cell carcinoma. Math. Biosci. Eng. 2019, 16, 8060–8068. [Google Scholar] [CrossRef] [PubMed]
- Jin, H.; Pan, Y.; Zhao, L.; Zhai, H.; Li, X.; Sun, L.; He, L.; Chen, Y.; Hong, L.; Du, Y.; et al. p75 neurotrophin receptor suppresses the proliferation of human gastric cancer cells. Neoplasia 2007, 9, 471–478. [Google Scholar] [CrossRef] [Green Version]
- Gravina, G.L.; Mancini, A.; Ranieri, G.; Di Pasquale, B.; Marampon, F.; Di Clemente, L.; Ricevuto, E.; Festuccia, C. Phenotypic characterization of human prostatic stromal cells in primary cultures derived from human tissue samples. Int. J. Oncol. 2013, 42, 2116–2122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, X.; Shen, Y.; Di, B.; Li, J.; Geng, J.; Lu, X.; He, Z. Biological and clinical significance of p75NTR expression in laryngeal squamous epithelia and laryngocarcinoma. Acta Otolaryngol. 2012, 132, 314–324. [Google Scholar] [CrossRef] [PubMed]
- Bankhead, P.; Loughrey, M.B.; Fernández, J.A.; Dombrowski, Y.; McArt, D.G.; Dunne, P.D.; McQuaid, S.; Gray, R.T.; Murray, L.J.; Coleman, H.G.; et al. QuPath: Open source software for digital pathology image analysis. Sci. Rep. 2017, 7, 16878. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Remmele, W.; Stegner, H. Recommendation for uniform definition of an immunoreactive score (IRS) for immunohistochemical estrogen receptor detection (ER-ICA) in breast cancer tissue. Pathologe 1987, 8, 138–140. [Google Scholar]
- Allred, D.; Harvey, J.; Berardo, M.; Clark, G. Prognostic and predictive factors in breast cancer by immunohistochemical analysiso. Mod. Pathol. Off. J. U.S. Can. Acad. Pathol. 1998, 11, 155–168. [Google Scholar]
- Tan, Y.; Cao, K.; Ren, G.; Qin, Z.; Zhao, D.; Li, N.; Chen, X.; Xia, Y.; Lu, Y. Effects of the ABCB1 and ABCG2 polymorphisms on the pharmacokinetics of afatinib in healthy Chinese volunteers. Xenobiotica 2020, 50, 237–243. [Google Scholar] [CrossRef]
- Triaca, V.; Carito, V.; Fico, E.; Rosso, P.; Fiore, M.; Ralli, M.; Lambiase, A.; Greco, A.; Tirassa, P. Cancer stem cells-driven tumor growth and immune escape: The Janus face of neurotrophins. Aging 2019, 11, 11770–11792. [Google Scholar] [CrossRef]
- Triaca, V.; Fico, E.; Sposato, V.; Caioli, S.; Ciotti, M.T.; Zona, C.; Mercanti, D.; La Mendola, D.; Satriano, C.; Rizzarelli, E.; et al. hNGF peptides elicit the NGF-TrkA signalling pathway in cholinergic neurons and retain full neurotrophic activity in the DRG assay. Biomolecules 2020, 10, 216. [Google Scholar] [CrossRef] [Green Version]
- Qi, X.; Yu, D.; Jia, B.; Jin, C.; Liu, X.; Zhao, X.; Zhang, G. Targeting CD133(+) laryngeal carcinoma cells with chemotherapeutic drugs and siRNA against ABCG2 mediated by thermo/pH-sensitive mesoporous silica nanoparticles. Tumor Biol. 2016, 37, 2209–2217. [Google Scholar] [CrossRef] [PubMed]
- Tan, Y.N.; Wu, X.; Li, S.; Wang, X.; Fu, G.; Xie, L.; Wu, Y.; Han, Q.; Tan, Y.N.; Wu, X.; et al. The expression and clinical significance of ABCG2, Oct4 and nanog in laryngeal carcinoma. J. Cancer Ther. 2020, 11, 660–672. [Google Scholar] [CrossRef]
- Chao, M.V. Neurotrophins and their receptors: A convergence point for many signalling pathways. Nat. Rev. Neurosci. 2003, 4, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Pincelli, C. p75 neurotrophin receptor in the skin: Beyond its neurotrophic function. Front. Med. 2017, 4. [Google Scholar] [CrossRef] [Green Version]
- Marconi, A.; Quadri, M.; Farnetani, F.; Ciardo, S.; Palazzo, E.; Lotti, R.; Cesinaro, A.M.; Fabbiani, L.; Vaschieri, C.; Puviani, M.; et al. In vivo melanoma cell morphology reflects molecular signature and tumor aggressiveness. J. Investig. Dermatol. 2022. [Google Scholar] [CrossRef]
- Wang, L.M.; Rahn, J.J.; Lun, X.Q.; Sun, B.; Kelly, J.J.P.; Weiss, S.; Robbins, S.M.; Forsyth, P.A.; Senger, D.L. Gamma-secretase represents a therapeutic target for the treatment of invasive glioma mediated by the p75 neurotrophin receptor. PLoS Biol. 2008, 6, 2496–2511. [Google Scholar] [CrossRef]
- Marchetti, D.; Aucoin, R.; Blust, J.; Murry, B.; Greiter-Wilke, A. p75 neurotrophin receptor functions as a survival receptor in brain-metastatic melanoma cells. J. Cell. Biochem. 2004, 91, 206–215. [Google Scholar] [CrossRef]
- Imai, T.; Tamai, K.; Oizumi, S.; Oyama, K.; Yamaguchi, K.; Sato, I.; Satoh, K.; Matsuura, K.; Saijo, S.; Sugamura, K.; et al. CD271 defines a stem cell-like population in hypopharyngeal cancer. PLoS ONE 2013, 8, e62002. [Google Scholar] [CrossRef] [Green Version]
- Caponio, V.C.A.; Troiano, G.; Togni, L.; Zhurakivska, K.; Santarelli, A.; Laino, L.; Rubini, C.; Lo Muzio, L.; Mascitti, M. Pattern and localization of perineural invasion predict poor survival in oral tongue carcinoma. Oral Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Demir, I.E.; Boldis, A.; Pfitzinger, P.L.; Teller, S.; Brunner, E.; Klose, N.; Kehl, T.; Maak, M.; Lesina, M.; Laschinger, M.; et al. Investigation of schwann cells at neoplastic cell sites before the onset of cancer invasion. J. Natl. Cancer Inst. 2014, 106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salvo, E.; Tu, N.H.; Scheff, N.N.; Dubeykovskaya, Z.A.; Chavan, S.A.; Aouizerat, B.E.; Ye, Y. TNFα promotes oral cancer growth, pain, and Schwann cell activation. Sci. Rep. 2021, 11, 1–14. [Google Scholar] [CrossRef]
- Le Moan, N.; Houslay, D.M.; Christian, F.; Houslay, M.D.; Akassoglou, K. Oxygen-dependent cleavage of the p75 neurotrophin receptor triggers stabilization of HIF-1α. Mol. Cell 2011, 44, 476–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| pTNM Stage | AJCC Stage | G |
|---|---|---|
| pT3N0M0 | III | G2 |
| pT4aN0M0 | IVa | G2 |
| pT3N3bM0 | IVb | G2 |
| pT4aN3bM0 | IVb | G3 |
| pT4aN0M0 | IVa | G2 |
| pT4aN1M0 | IVa | G2 |
| pT2NXM0 | II | G2 |
| pT4aNXM0 | IVa | G2 |
| Stage | p75ICD | ABCG2 |
|---|---|---|
| II | + | ++ |
| III | ++ | ++ |
| IVa | ++ | +++ |
| IVb | +++ | + |
| LSCC | p75ICD | p75NTR FL | ABCG2 |
|---|---|---|---|
| Zone 1 | + | ++ | + |
| Zone 2 | ++ | +++ | ++ |
| Zone 3 | ++ | + | +++ |
| Zone 4 | +++ | ++ | ++ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Triaca, V.; Fico, E.; Rosso, P.; Ralli, M.; Corsi, A.; Severini, C.; Crevenna, A.; Agostinelli, E.; Rullo, E.; Riminucci, M.; et al. Pilot Investigation on p75ICD Expression in Laryngeal Squamous Cell Carcinoma. Cancers 2022, 14, 2622. https://doi.org/10.3390/cancers14112622
Triaca V, Fico E, Rosso P, Ralli M, Corsi A, Severini C, Crevenna A, Agostinelli E, Rullo E, Riminucci M, et al. Pilot Investigation on p75ICD Expression in Laryngeal Squamous Cell Carcinoma. Cancers. 2022; 14(11):2622. https://doi.org/10.3390/cancers14112622
Chicago/Turabian StyleTriaca, Viviana, Elena Fico, Pamela Rosso, Massimo Ralli, Alessandro Corsi, Cinzia Severini, Alvaro Crevenna, Enzo Agostinelli, Emma Rullo, Mara Riminucci, and et al. 2022. "Pilot Investigation on p75ICD Expression in Laryngeal Squamous Cell Carcinoma" Cancers 14, no. 11: 2622. https://doi.org/10.3390/cancers14112622
APA StyleTriaca, V., Fico, E., Rosso, P., Ralli, M., Corsi, A., Severini, C., Crevenna, A., Agostinelli, E., Rullo, E., Riminucci, M., Colizza, A., Polimeni, A., Greco, A., & Tirassa, P. (2022). Pilot Investigation on p75ICD Expression in Laryngeal Squamous Cell Carcinoma. Cancers, 14(11), 2622. https://doi.org/10.3390/cancers14112622