
Peer Education and Peer Counselling for Health and Well-Being: A Review of Reviews


Abstract
:1. Introduction
Aim of This Paper
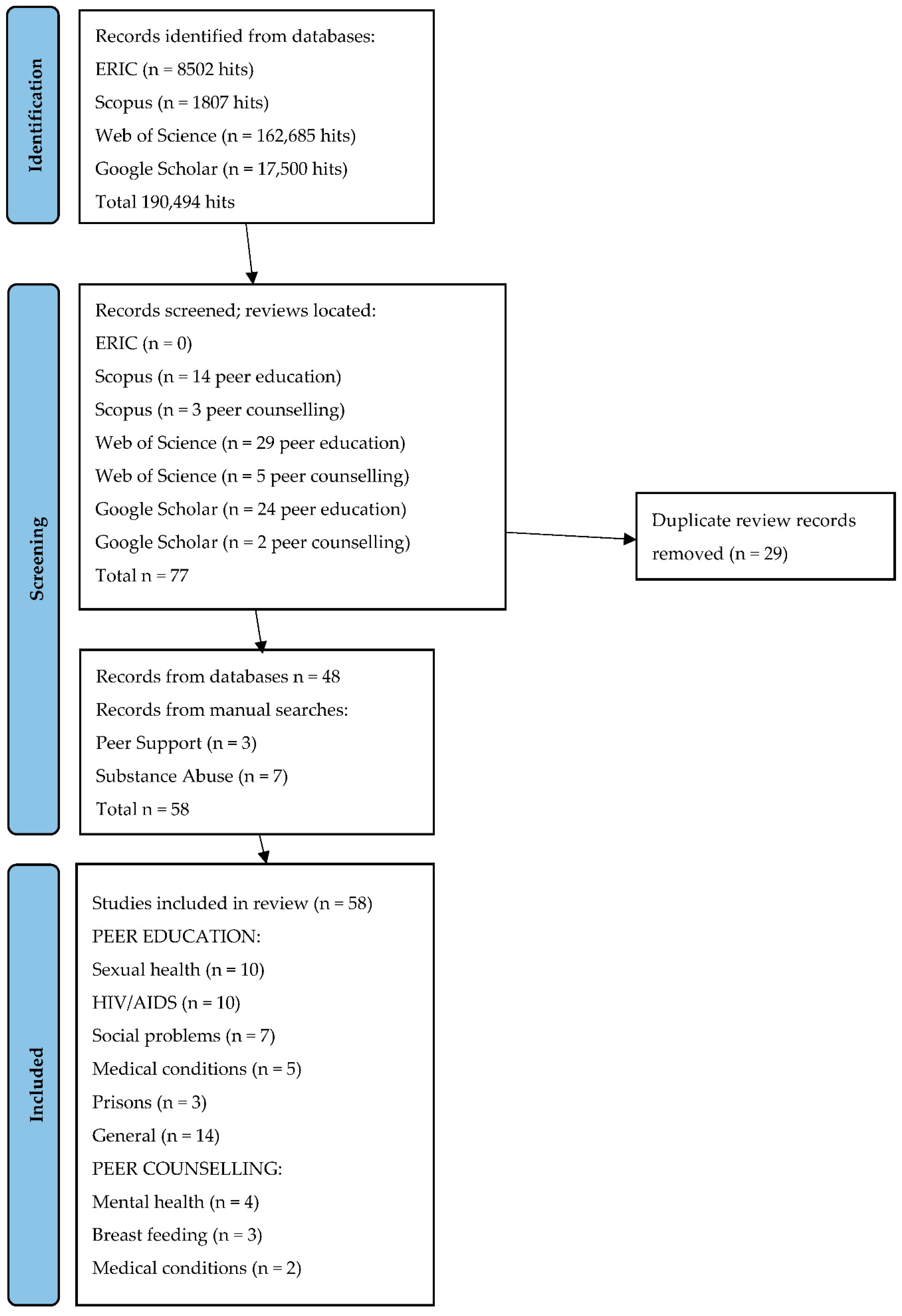
2. Methods
3. Results: Peer Education
3.1. Sexual Health
3.2. Human Immunodeficiency Virus/Acquired Immune Deficiency Syndrome (HIV/AIDS)
3.3. Social Problems
3.3.1. Drug Use
3.3.2. Obesity
3.3.3. Smoking
3.3.4. Alcohol Abuse
3.4. Medical Conditions
3.5. Prisons
3.6. General
4. Results: Peer Counselling and Peer Support
4.1. Mental Health
4.2. Breast-Feeding
4.3. Medical Conditions
5. Discussion
5.1. Summary
5.1.1. Peer Education
5.1.2. Peer Counselling and Support
5.2. Strengths and Limitations
5.3. Implications for Action
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Topping, K.J.; Ehly, S. Peer-Assisted Learning; Lawrence Erlbaum: Mahwah, NJ, USA; London, UK, 1998. [Google Scholar]
- Toseland, R.W.; Smith, G.C. Effectiveness of individual counseling by professional and peer helpers for family caregivers of the elderly. Psychol. Aging 1990, 5, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Zunker, V.; Brown, W. Comparative effectiveness of student and professional counselors. Pers. Guid. J. 1966, 44, 738–743. [Google Scholar] [CrossRef]
- Topping, K.J. Reaching where adults cannot: Peer education and counselling. Educ. Psychol. Pract. 1996, 11, 23–29. [Google Scholar] [CrossRef]
- Pfeiffer, P.N.; Heisler, M.; Piette, J.D.; Rogers, M.A.; Valenstein, M. Efficacy of peer support interventions for depression: A meta-analysis. Gen. Hosp. Psychiatry 2011, 33, 29–36. [Google Scholar] [CrossRef] [Green Version]
- Repper, J.; Carter, T. Using Personal Experience to Support Others with Similar Difficulties: A Review of the Literature on Peer Support in Mental Health Services; Together-UK: London, UK, 2010. [Google Scholar]
- White, S.; Foster, R.; Marks, J.; Morshead, R.; Goldsmith, L.; Barlow, S.; Sin, J.; Gillard, S. The effectiveness of one-to-one peer support in mental health services: A systematic review and meta-analysis. BMC Psychiatry 2020, 20, 534. [Google Scholar] [CrossRef]
- Huriah, T.; Dwi, L.V. School-based smoking prevention in adolescents in developing countries: A literature review. Maced. J. Med. Sci. 2020, 8, 84–89. Available online: https://oamjms.eu/index.php/mjms/article/view/4336 (accessed on 1 March 2022). [CrossRef]
- Cuijpers, P. Effective ingredients of school-based drug prevention programs: A systematic review. Addict. Behav. 2002, 27, 1009–1023. [Google Scholar] [CrossRef]
- Bassuk, E.L.; Hanson, J.; Greene, R.N.; Richard, M.; Laudet, A. Peer-delivered recovery support services for addictions in the United States: A systematic review. J. Subst. Abus. Treat. 2016, 63, 1–9. [Google Scholar] [CrossRef]
- MacArthur, G.J.; Harrison, S.; Caldwell, D.M.; Hickman, M.; Campbell, R. Peer-led interventions to prevent tobacco, alcohol and/or drug use among young people aged 11–21 years: A systematic review and meta-analysis. Addiction 2015, 111, 391–407. [Google Scholar] [CrossRef] [Green Version]
- Chen, Y.; Li, Z.; Yang, Q.; Yang, S.; Dou, C.; Zhang, T.; Guan, B. The effect of peer support on individuals with overweight and obesity: A meta-analysis. Iran. J. Public Health 2021, 50, 2439–2450. [Google Scholar] [CrossRef]
- Lim, S.; Lee, W.K.; Tan, A.; Chen, M.L.; Tay, C.T.; Sood, S.; Pirotta, S.; Moran, L.J.; Daivadanam, M.; Busija, L.; et al. Peer-supported lifestyle interventions on body weight, energy intake, and physical activity in adults: A systematic review and meta-analysis. Obes. Rev. 2021, 22, e13328. [Google Scholar] [CrossRef] [PubMed]
- Yip, C.; Gates, M.; Gates, A.; Hanning, R.M. Peer-led nutrition education programs for school-aged youth: A systematic review of the literature. Health Educ. Res. 2016, 31, 82–97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, R.I. Smoking in children: Developing a social psychological strategy of deterrence. Prev. Med. 1976, 5, 122–127. [Google Scholar] [CrossRef]
- Finn, P. Institutionalizing peer education in the health education classroom. J. Sch. Health 1981, 51, 91–95. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, N. Peer group processes and adolescent health-related behaviour: More than “peer group pressure”? J. Community Appl. Soc. Psychol. 1994, 4, 329–345. [Google Scholar] [CrossRef]
- Steinhausen, G.W. Peer education programs: A look nationally. Health Educ. 1983, 14, 7–8. [Google Scholar] [CrossRef]
- Flay, B.R. Psychosocial approaches to smoking prevention: A review of findings. Health Psychol. 1985, 4, 449–488. [Google Scholar] [CrossRef]
- Moskowitz, J.M. The primary prevention of: A critical review of the research literature. J. Stud. Alcohol 1989, 50, 54–88. [Google Scholar] [CrossRef]
- May, C. Research on alcohol education for young people: A critical review of the literature. Health Educ. J. 1991, 50, 195–199. [Google Scholar] [CrossRef]
- Milburn, K. A critical review of peer education with young people with special reference to sexual health. Health Educ. Res. 1995, 10, 407–420. [Google Scholar] [CrossRef]
- Kim, C.R.; Free, C. Recent evaluations of the peer-led approach in adolescent sexual health education: A systematic review. Perspect. Sex. Reprod. Health 2008, 40, 144–151. [Google Scholar] [CrossRef]
- Price, N.; Knibbs, S. How effective is peer education in addressing young people’s sexual and reproductive health needs in developing countries? Child. Soc. 2009, 23, 291–302. [Google Scholar] [CrossRef]
- Tolli, M.V. Effectiveness of peer education interventions for HIV prevention, adolescent pregnancy prevention and sexual health promotion for young people: A systematic review of European studies. Health Educ. Res. 2012, 27, 904–913. [Google Scholar] [CrossRef] [Green Version]
- Ye, S.; Yin, L.; Amico, K.R.; Simoni, J.; Vermund, S.; Ruan, Y.; Shao, Y.; Qian, H.Z. Efficacy of peer-led interventions to reduce unprotected anal intercourse among men who have sex with men: A meta-analysis. PLoS ONE 2014, 9, e90788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simbar, M.; Alizadeh, S.; Hajifoghaha, M.; Golezar, S. Review of Iranian adolescents’ educational needs for sexual and reproductive health. J. Isfahan Med. Sch. 2017, 34, 1563–1572. [Google Scholar]
- Wong, T.; Pharr, J.R.; Bungum, T.; Coughenour, C.; Lough, N.L. Effects of peer sexual health education on college campuses: A systematic review. Health Promot. Pract. 2019, 20, 652–666. [Google Scholar] [CrossRef] [PubMed]
- Aslan, F. School-based sexual health education for adolescents in Turkey: A systematic review. Int. Q. Community Health Educ. 2020, 42, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Barua, A.; Watson, K.; Plesons, M.; Chandra-Mouli, V.; Sharma, K. Adolescent health programming in India: A rapid review. Reprod. Health 2020, 17, 87. [Google Scholar] [CrossRef]
- Siddiqui, M.; Kataria, I.; Watson, K.; Chandra-Mouli, V. A systematic review of the evidence on peer education programmes for promoting the sexual and reproductive health of young people in India. Sex. Reprod. Health Matters 2020, 28, 1741494. [Google Scholar] [CrossRef] [PubMed]
- Baldwin, J. Using peer education approaches in HIV/AIDS programs for youth: A review of the literature. Peer Facil. Q. 1995, 12, 34–37. [Google Scholar]
- Van Khoat, D.; West, G.R.; Valdiserri, R.O.; Phan, N.T. Peer education for HIV prevention in the socialist republic of Vietnam: A national assessment. J. Community Health 2003, 28, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Maticka-Tyndale, E.; Barnett, J.P. Peer-led interventions to reduce HIV risk of youth: A review. Eval. Program Plan. 2010, 33, 98–112. [Google Scholar] [CrossRef] [PubMed]
- Mwale, M.; Muula, A.S. Systematic review: A review of adolescent behavior change interventions [BCI] and their effectiveness in HIV and AIDS prevention in sub-Saharan Africa. BMC Public Health 2017, 17, 718. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nugroho, A.; Erasmus, V.; Zomer, T.P.; Wu, Q.; Richardus, J.H. Behavioral interventions to reduce HIV risk behavior for MSM and transwomen in Southeast Asia: A systematic review. Aids Care Psychol. Socio-Med. Asp. AIDS/HIV 2017, 29, 98–104. [Google Scholar] [CrossRef] [Green Version]
- Mahat, G.; Scoloveno, M.A. Effectiveness of adolescent peer education programs on reducing HIV/STI Risk: An integrated review. Res. Theory Nurs. Pract. 2018, 32, 168–198. [Google Scholar] [CrossRef]
- Medley, A.; Kennedy, C.; O’Reilly, K.; Sweat, M. Effectiveness of peer education interventions for HIV prevention in developing countries: A systematic review and meta-analysis. AIDS Educ. Prev. 2019, 21, 181–206. [Google Scholar] [CrossRef] [Green Version]
- Chen, D.H.; Luo, G.F.; Meng, X.J.; Wang, Z.X.; Cao, B.L.; Yuan, T.W.; Xie, Y.; Hu, T.; Chen, Y.Q.; Ke, W.J.; et al. Efficacy of HIV interventions among factory workers in low- and middle-income countries: A systematic review. BMC Public Health 2020, 20, 1310. [Google Scholar] [CrossRef]
- He, J.; Wang, Y.; Du, Z.; Liao, J.; He, N.; Hao, Y. Peer education for HIV prevention among high-risk groups: A systematic review and meta-analysis. BMC Infect. Dis. 2020, 20, 338. [Google Scholar] [CrossRef]
- Berg, R.C.; Page, S.; Øgård-Repål, A. The effectiveness of peer-support for people living with HIV: A systematic review and meta-analysis. PLoS ONE 2021, 16, e0252623. [Google Scholar] [CrossRef]
- Gatlin, T.K.; Serafica, R.; Johnson, M. Systematic review of peer education intervention programmes among individuals with type 2 diabetes. J. Clin. Nurs. 2017, 26, 4212–4222. [Google Scholar] [CrossRef]
- Zhong, C.S.; Melendez-Torres, G.J. The effect of peer-led self-management education programmes for adolescents with asthma: A systematic review and meta-analysis. Health Educ. J. 2017, 76, 676–694. [Google Scholar] [CrossRef]
- Chaffey, L.; Bigby, C. Health education by peers with spinal cord injury: A scoping review. J. Dev. Phys. Disabil. 2018, 30, 141–154. [Google Scholar] [CrossRef]
- Madmoli, M.; Khodadadi, M.; Papi Ahmadi, F.; Niksefat, M. A systematic review on the impact of peer education on self-care behaviors of patients. Int. J. Health Biol. Sci. 2019, 2, 1–5. [Google Scholar] [CrossRef]
- Christensen, J.H.; Elsborg, P.; Melby, P.S.; Nielsen, G.; Bentsen, P. A scoping review of peer-led physical activity interventions involving young people: Theoretical approaches, intervention rationales, and effects. Youth Soc. 2021, 53, 811–840. [Google Scholar] [CrossRef]
- Wright, N.; Bleakley, A.; Butt, C.; Chadwick, O.; Mahmood, K.; Patel, K.; Salhi, A. Peer health promotion in prisons: A systematic review. Int. J. Prison. Health 2011, 7, 37–51. [Google Scholar] [CrossRef] [PubMed]
- Bagnall, A.M.; South, J.; Hulme, C.; Woodall, J.; Vinall-Collier, K.; Raine, G.; Kinsella, K.; Dixey, R.; Harris, L.; Wright, N.M. A systematic review of the effectiveness and cost-effectiveness of peer education and peer support in prisons. BMC Public Health 2015, 15, 290. [Google Scholar] [CrossRef] [Green Version]
- Valera, P.; Chang, Y.; Lian, Z. HIV risk inside U.S. prisons: A systematic review of risk reduction interventions conducted in U.S. prisons. AIDS Care 2017, 29, 943–952. [Google Scholar] [CrossRef]
- Fennel, R. A review of evaluations of peer education programs. J. Am. Coll. Health 1993, 41, 251–253. [Google Scholar] [CrossRef]
- Mellanby, A.R.; Rees, J.B.; Tripp, J.H. Peer-led and adult-led school health education: A critical review of available comparative research. Health Educ. Res. 2000, 15, 533–545. [Google Scholar] [CrossRef] [Green Version]
- Bernert, D.J.; Mouzon, L.D. Peer education in the ‘90’s: A literature review of utility and effectiveness. Health Educ. J. Eta Sigma Gamma 2001, 33, 31–37. [Google Scholar]
- Green, J. Peer education. Promot. Educ. 2001, 8, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Harden, A.; Oakley, A.; Olive, S. Peer-delivered health promotion for young people: A systematic review of different study designs. Health Educ. J. 2001, 60, 339–353. [Google Scholar] [CrossRef]
- Webel, A.R.; Okonsky, J.; Trompeta, J.; Holzemer, W.L. A systematic review of the effectiveness of peer-based interventions on health-related behaviors in adults. Am. J. Public Health 2010, 100, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Abdi, F.; Simbar, M. The peer education approach in adolescents—Narrative review article. Iran. J. Public Health 2013, 42, 1200–1206. [Google Scholar] [PubMed]
- Azizi, M.; Hamzehgardeshi, Z.; Shahhosseini, Z. Influential factors for the improvement of peer education in adolescents: A narrative review. J. Pediatr. Rev. 2017, 5, 38–44. Available online: http://jpr.mazums.ac.ir/article-1-135-en.html (accessed on 1 March 2022). [CrossRef]
- Ramchand, R.; Ahluwalia, S.C.; Xenakis, L.; Apaydin, E.; Raaen, L.; Grimm, G. A systematic review of peer-supported interventions for health promotion and disease prevention. Prev. Med. 2017, 101, 156–170. [Google Scholar] [CrossRef]
- Araujo, N. Reviewing the evidence of effective peer education among young people. Perspect. Public Health 2018, 138, 299–300. [Google Scholar] [CrossRef]
- Lorthios-Guilledroit, A.; Lucie, R.; Filiatrault, J. Factors associated with the implementation of community-based peer-led health promotion programs: A scoping review. Eval. Program Plan. 2018, 68, 19–33. [Google Scholar] [CrossRef]
- Vujcich, D.; Thomas, J.; Crawford, K.; Ward, J. Indigenous youth peer-led health promotion in Canada, New Zealand, Australia, and the United States: A systematic review of the approaches, study designs, and effectiveness. Front. Public Health 2018, 6, 31. [Google Scholar] [CrossRef] [Green Version]
- Ghasemi, V.; Simbar, M.; Rashidi Fakari, F.; Saei Ghare Naz, M.; Kiani, Z. The effect of peer education on health promotion of Iranian adolescents: A systematic review. Int. J. Pediatr. 2019, 7, 9139–9157. [Google Scholar] [CrossRef]
- Rose-Clarke, K.; Bentley, A.; Marston, C.; Prost, A. Peer-facilitated community-based interventions for adolescent health in low- and middle-income countries: A systematic review. PLoS ONE 2019, 14, e0210468. [Google Scholar] [CrossRef] [Green Version]
- Warner, R.; Scott, S. Peer counselling. Pers. Guid. J. 1974, 53, 228–231. [Google Scholar]
- Mitchum, N.T. Introducing TIP: The Total Involvement Program for peer facilitators. Sch. Couns. 1983, 31, 146–149. [Google Scholar]
- Bond, J. Knowing You—Knowing Me: A Peer Counselling Project; Department of Education, University of Warwick: Warwick, UK, 1989. [Google Scholar]
- Carr, R. The city-wide peer counselling program. Child. Youth Serv. Rev. 1988, 10, 217–232. [Google Scholar] [CrossRef]
- Hildebrand, A.; Weiss, M.; Stemmler, M. Online peer-to-peer suicide prevention programs in youth and young adults: A systematic review. Z. Psychiatr. Psychol. Psychother. 2019, 67, 221–229. [Google Scholar]
- Chapman, D.J.; Morel, K.; Anderson, A.K.; Damio, G.; Pérez-Escamilla, R. Breastfeeding peer counseling: From efficacy through scale-up. J. Hum. Lact. 2010, 26, 314–326. [Google Scholar] [CrossRef]
- Chola, L.; Fadnes, L.T.; Engebretsen, I.M.S.; Nkonki, L.; Nankabirwa, V.; Sommerfelt, H.; Tumwine, J.K.; Tylleskär, T.; Robberstad, B.; PROMISE-EBF Study Group. Cost-effectiveness of peer counselling for the promotion of exclusive breastfeeding in Uganda. PLoS ONE 2015, 10, e0142718. [Google Scholar] [CrossRef] [Green Version]
- Buckland, C.; Hector, D.; Kolt, G.S.; Fahey, P.; Arora, A. Interventions to promote exclusive breastfeeding among young mothers: A systematic review and meta-analysis. Int. Breastfeed. J. 2020, 15, 102. [Google Scholar] [CrossRef]
- Hu, J.; Wang, X.; Guo, S.; Chen, F.; Wu, Y.-Y.; Ji, F.J.; Fang, X. Peer support interventions for breast cancer patients: A systematic review. Breast Cancer Res. Treat. 2019, 174, 325–341. [Google Scholar] [CrossRef]
- Hu, J.; Wu, Y.; Ji, F.; Fang, X.; Chen, F. Peer support as an ideal solution for racial/ethnic disparities in colorectal cancer screening: Evidence from a systematic review and meta-analysis. Dis. Colon Rectum 2020, 63, 850–858. [Google Scholar] [CrossRef]

{kind=link}
| Type of Problem | Total Number of Reviews | Number of Types of Review: Narrative, Systematic or Meta-Analysis * | Number of Studies with Effect Sizes or Equivalent | Effect Sizes or Equivalent Mean in () |
|---|---|---|---|---|
| PEER EDUCATON | ||||
| Sexual Health | 10 | Narrative 5 Systematic 5 Meta-analysis 1 | 1 | 0.27 |
| HIV/AIDS | 10 | Narrative 4 Systematic 4 Meta-analysis 3 | 3 | 2.28, 0.37, 1.92, 1.22 3.19, 2.66, 0.50, 0.82 1.07, 1.06, 6.24 (mean = 1.94) |
| Social Problems | 7 | Narrative Systematic 5 Meta-analysis 3 | 4 | 0.16, 0.72, 0.24 0.78, 0.12 1.05, 0.24, 0.75, 0.20 0.78, 0.80, 0.70 (mean = 0.55) |
| Medical Conditions | 5 | Narrative 1 Systematic 3 Meta-analysis 1 | 1 | 0.70, 1.36 (mean = 1.03) |
| Prisons | 3 | Narrative Systematic 3 Meta-analysis | 0 | |
| General | 14 | Narrative 8 Systematic 5 Meta-analysis 1 | 1 | −0.50, 2.86 (mean = 1.18) |
| PEER COUNSELING | ||||
| Mental Health | 4 | Narrative 1 Systematic 2 Meta-analysis 1 | 2 | 0.59, 0.10 0.86, 0.19, 0.23 (mean = 0.39) |
| Breast-Feeding | 3 | Narrative 1 Systematic 2 Meta-analysis1 | 0 | |
| Medical Conditions | 2 | Narrative Systematic 2 Meta-analysis1 | 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Topping, K.J. Peer Education and Peer Counselling for Health and Well-Being: A Review of Reviews. Int. J. Environ. Res. Public Health 2022, 19, 6064. https://doi.org/10.3390/ijerph19106064
Topping KJ. Peer Education and Peer Counselling for Health and Well-Being: A Review of Reviews. International Journal of Environmental Research and Public Health. 2022; 19(10):6064. https://doi.org/10.3390/ijerph19106064
Chicago/Turabian StyleTopping, Keith James. 2022. "Peer Education and Peer Counselling for Health and Well-Being: A Review of Reviews" International Journal of Environmental Research and Public Health 19, no. 10: 6064. https://doi.org/10.3390/ijerph19106064
APA StyleTopping, K. J. (2022). Peer Education and Peer Counselling for Health and Well-Being: A Review of Reviews. International Journal of Environmental Research and Public Health, 19(10), 6064. https://doi.org/10.3390/ijerph19106064