1. Introduction
Cerebral palsy is one of the common movement disorders in younger school-age children [
1,
2,
3] It is a neurodevelopmental, non-progressive disorder caused by prenatal, perinatal, or early postnatal brain damage, which affects the child’s motor development [
4,
5]. Although it is a permanent condition, it does not worsen over the years, and as Seidel (2015) mentioned, with rehabilitation the condition of an affected individual can improve. Recent trends generally point to the possibility of early diagnosis of cerebral palsy or an increased risk for it even during pregnancy (6 months). In most cases, it is usually detected between 12 and 42 weeks of age [
6,
7]. However, early diagnosis is crucial due to the timely deployment of intervention [
8].
Cerebral palsy has several forms, and three primary groups can be distinguished: the spastic forms of cerebral palsy, dyskinetic forms of cerebral palsy, and ataxic forms of cerebral palsy [
9]. The most common form of cerebral palsy is diparesis (Yokoshi, 2012), which is classified as spastic (spasmodic) polio. In diparesis, the lower limbs are characteristically affected, and as a result, the individual moves by a so-called scissoring gait [
3]. At the same time, mild upper limb damage may occur (Kolář, 2015). Nevertheless, movement disorder may not always be associated with cerebral palsy. Dyspraxia is an often overlooked and underestimated chronic disorder affecting an individual’s daily life due to a reduction in his/her motor functions [
10].
Dyspraxia is manifested by a very low level of one’s control of movements, coordination, and overall perception of one’s body [
11]. It is a certain inability of an individual to plan, organize, and coordinate movements, which can cause problems associated with the development and control of fine motor skills, gross motor skills, as well as speech [
12]. Further, the individuals have an impaired ability to learn motor skills appropriate to their age [
13]. Children with dyspraxia are often described as clumsy because they have problems tying shoes, writing, or handling certain objects. Imitation problems may also occur [
14].
Dyspraxia prevalence is currently reported in 5–6% of the population [
15]. Although the condition does not deteriorate, individual reeducation of dyspraxia is a long-term process with an ambiguous prognosis, and the individual’s weakened movement performance will limit them throughout their life [
16]. One of the possible approaches to addressing the issues is psychomotor therapy. Activities within the therapeutic process mediated through experience bring much positive impact to an individual and at the same time facilitate the process of relaxation, rehabilitation, and coping with negative states.
1.1. Background
Psychomotor therapy affects the somatic, psychological, and social aspects of the individual, with activities focusing not only on increasing physical fitness but also on reducing stress [
17,
18]. Following up-to-date trends and approaches focused on new technologies potentially capable of supporting the individuals, both motorically and cognitively, are shown to be effective as well, e.g., meaningful use of game consoles and freely available commercial products that can replace testing through classical pencil-and-paper procedures proved its potential as well [
19,
20,
21]. Robotic therapeutic assistance, as one of the contemporary approaches in the rehabilitation of people with cognitive and motor problems, has also been successfully applied in the last decade supporting patients’ motor skills in particular. The robotic therapy assists in an intensive, repetitive, and interactive training within a controlled environment that supports the control over and restoration of motor skills [
22].
Robotic rehabilitation is a modern and advanced rehabilitation technology, which was created as a modification of body weight supported treadmill training for walking. From a neurophysiological point of view, the therapy is based on spinal anatomy, the plasticity of the central nervous system (CNS), and motor learning. The objective of this therapy is to affect the somatic and mental state of the patient [
23,
24,
25].
An illustration of such a device is the Armeo
® spring, which is a system used to rehabilitate upper limbs. This exoskeleton provides a patient with gravitational support for the affected upper limb through spring mechanisms. This increases any residual ranges of active motion [
26,
27] speak of assistive robotics as a technology that is widely used in rehabilitation. Such assistance in rehabilitation is in general well-received by patients and has proven to be a suitable motivational supplement for patients suffering from motor problems. It is the interaction of a man and a robot, which represents new possibilities for application processes in rehabilitation; i.e., a new interest emerges in using social robots as assistance in rehabilitation processes.
In addition to the basic ability to move and play autonomously, social-assisted robotics also focuses on using the physical component of the robot to communicate and interact with a patient. Such devices are then also designed to motivate, train, supervise, educate, or facilitate communication within assisting or rehabilitation processes. Overall, they may thus help to obtain better results within the rehabilitation itself [
28,
29].
1.2. Purpose
The purpose of the presented research was to inform understanding of the motor development of selected patients with regard to the monitored indicators and their management of common daily activities. The selected single-case research design allowed us to get a deeper insight into the research issues that were chosen and reflected in the introduction. This motor development is then reflected not only in the management of school duties but also in the quality of spending free time. A comprehensive view was the goal of the research survey. With regard to the theoretical background and the aim of the research, we were interested in the effects our intervention method might have on the monitored indicators in the selected patients. The research was conducted to find out whether the intensive therapy we had chosen had any effects on the development of motor skills in selected patients.
2. Material and Methods
Two patients (N = 2) participated in our research survey based on intentional sampling. They were selected based on relevant features, i.e., motor deficit, age 7–9 years, and participation in rehabilitation interventions. Based on predetermined criteria, we contacted the two patients, one of whom (N = 1) was diagnosed with cerebral palsy diparesis (according to ICD-10; G80.1: spastic diplegic cerebral palsy, 8.8 years of age) and the other patient (N = 1) with developmental dyspraxia (according to ICD-10; F82: a specific developmental disorder of motor functions, 7.4 years of age). The patients were intentionally selected without prior testing.
The aim of the research was to find out what effect the chosen combination therapy using robotically assisted therapy and the elements of occupational therapy and special education have on the development of the motor skills of the patients together with the support of social adaptability. The intervention (as well as the testing) was carried out by postdoctoral researchers, and the authors only conducted the data statistic analysis. In this way, we achieved the removal of the authors’ ego involvement and overall bias in obtaining the ideal results of the research survey. The patients underwent the intervention that complemented their other rehabilitation activities regularly three times a week. The intervention was conducted in an individual form, initially with the participation of the family (or legal representatives) of the patient, then fully individually with the participation of the patient and a therapist. The individual interventions were divided into four areas of impact:
Fine motor skills development: motor skills development worksheets, object manipulation, model activities;
Gross motor skills development: robot-assisted therapy—motored, therapeutic physical education, psychomotor therapy;
Social adaptability support;
Independence and self-sufficiency support.
The therapy took place mainly in an individual form with the use of combined therapeutic approaches. These approaches are listed below. The therapy took place three times a week for 50 min. There was a total of 20 interventions of which 15 were with the application of therapy and testing and 5 were only for testing purposes (see description below). For data processing, the method of single-case research design (namely reversal or ABA design) was used, characterized by a thorough insight into a specific case followed by the potential discovery of new contexts undetectable within massive research [
30]. The single-case research design method is called N = 1. This designation determines the size of the research sample, i.e., the examination of an individual (single) case. In this case, the research survey is N = 2, the one individual case of a patient with diagnosed cerebral palsy and the other individual case of a patient with diagnosed developmental dyspraxia, which will each help us complement the idea of the effect of the new combination therapy.
The single-case research design works with the data obtained prior to the start of the intervention, forming the so-called baseline (referred to as phase A or a baseline phase) and data that a researcher collects during the therapy or intervention (marked B). The data compiled in this way is then compared, and it is determined how the applied therapeutic approach affected the initially measured values. The format is referred to as the AB format (or a basic reversal design). In this research, the basic reversal design was extended to the ABAB format with the reintroduction of the intervention and, yet, another return to the baseline measurement. A standardized test was applied to measure success. The data for our research study was obtained using a modification of the standardized test focused on functional independence (FIM test—Functional Independence Measure; Data Management Service of the Uniform Data System for Medical Rehabilitation, State University of New York at Buffalo; areas of locomotion and social adaptability). The measurements took place after reaching a steady phase, following periods of adjustment (as the variables had to reach a steady state prior to the measurement); i.e., when the first therapy was completed, the patient was not under the intervention for a certain period. The measurements indicate whether the patient’s condition following the intervention remains at the level affected by the intervention (B) or whether the condition gradually returns to the baseline levels (A). If they tend to return to the initial values after a rest period, we may assume that the tested therapy may have an impact on the patient’s improved condition.
3. Results
During 2020/2021, regular monthly testing took place using a standardized FIM test with the following results. The presented results point to the state prior to and after the chosen intervention of two patients selected for the research survey based on the relevant features.
Table 1 shows the development of the test value in the monitored indicators in patient 1 diagnosed with cerebral palsy. Regular testing without intervention was carried out at the beginning of January and February 2020.
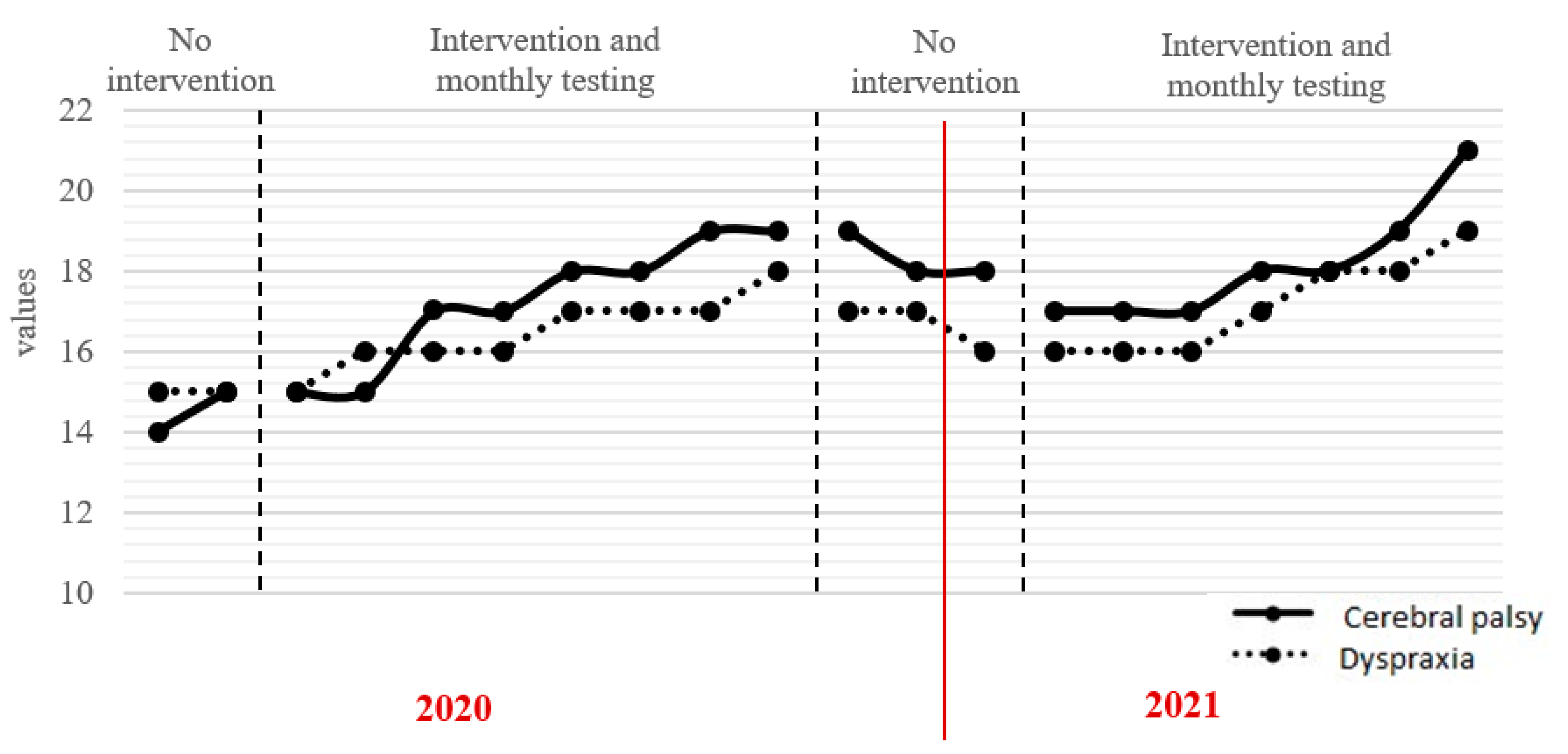
The patient participated only in personal rehabilitation sessions and other supportive therapies. The rehabilitation intervention, along with regular monthly testing, began in March 2020 and was carried on until October 2020. During this period, regarding the monitored indicators of the given standardized test, the condition of the patient improved. The improvement by five points was declared through the comparison of the initial and the last testing in this block. A rehabilitation intervention period was followed by a period of no intervention again at the turn of 2020/2021 from November 2020 to January 2021. In this period, a slight decrease (by one point) was measured. The trend continued even at the beginning of our intervention starting in February 2021 when the score decreased by up to two points. It was not until May 2021 that the increase began climbing to a total of 21 points. Overall, the patient improved by seven points in the monitored indicators (the input = 14 points, the output = 21 points).
Table 2 shows the development of the test value in the monitored indicators in patient 2 diagnosed with developmental dyspraxia. Regular testing without intervention was carried out at the beginning of January and February 2020. The patient participated in no other therapies but in the personal rehabilitation and other supportive therapies (no intervention). The rehabilitation intervention, along with regular monthly testing, began in March 2020 and was carried on until October 2020. In that period, the condition of the patient improved within the monitored indicators of the standardized test. The comparison of the initial testing and the last testing in this block showed an improvement of two points. A no intervention period followed at the turn of 2020/2021 from November 2020 to January 2021 and a slight decrease (by two points) was measured. The decline continued also at the beginning of another intervention (from February 2021) with a two point decline. It was not until May 2021 that the point increase began climbing to a total of 19 points. Overall, the patient improved by four points in the monitored indicators (the input =15 points, the output = 19 points).
Figure 1 shows the graphic layout of the survey results for both patients at the time of the project. The comparison of input, output, and continuous testing is visible. A noticeable improvement in the monitored indicators in both patients is also evident. A drop in the score matches the period of intervention. This decline in both patients lasted for three months until the subsequent improvement in the monitored indicators started. Based on this fact, we can assume that the intervention (through combined therapy) had a certain impact on the improved patient outcomes. Combined therapy means a set of partial rehabilitation approaches directly or indirectly applied to the given diagnoses. These approaches also include the use of not only robotically assisted therapy or modern technologies (e.g., BalanceTutor) but also the use of game consoles or tablets. These are modern technologies that through entertainment motivate clients to develop their fine and gross motor skills along with the development of cognitive functions. However, cognitive rehabilitation was not the main content of the intervention in our case, as we focused on the development of motor skills regarding the support of social adaptability.
The results recorded using the FIM test were obtained by a tester who was not a part of the intervention team. Thus, there was no authors’ self-involvement in the results, with the potential consequent bias of the data in favour of the intervention. The single-case research design method was applied to explore the possibility of a qualitative research investigation with a deeper insight into the researched issues.
4. Discussion
The presented research survey focused on the work with patients (N = 2) who were selected based on relevant features, e.g., motor deficit. One patient suffered from cerebral palsy diparesis, and the other from developmental dyspraxia. The presented results show that the determined intervention method was beneficial for the patients’ development in the monitored indicators. The conclusion was reached following the use of the single-case research design method, allowing thorough insight into the issue and detailed monitoring of the individual subjects. The therapy was specifically focused on the use of robotically assisted therapy. The BalanceTutor device and subsequently other activities leading to the support of impaired motor skills of the patients were used in this research. The effectiveness of robotically assisted therapy is accepted somewhat ambiguously in practice with its supporters and their opponents claiming that robotically assisted therapy is rather a supplement to common rehabilitation procedures.
In practice, robot-assisted gait training is implemented in rehabilitation programs and can be encountered in rehabilitation clinics or wards or wards of pediatric neurorehabilitation centres. Such approaches have been considered innovative for almost 10 years and have been increasingly in the spotlight of both the general and professional public with their development constantly advancing. However, the impact and the effect of the advanced therapies remain unclear, and some authors are inclined to use robotic therapy merely as a complement to classical therapy [
31]. The therapies utilizing computer game programs are, yet, another innovative approach considered here. An example is the development of a robot game consisting of three phases (levels of difficulty). Such games are specifically focused on neuropsychomotor rehabilitation therapy programs. However, based on the presented results, researchers point out that such approaches are more appropriate as complementary to standard therapy than as their full replacement (Lins et al., 2019).
In general, physical interaction with the environment and object manipulation play important roles in the development of children’s cognitive and perceptual skills. It is in physically disabled children that we often encounter the occurrence of fear. The fear is of losing meaningful play. Robotic therapy (assistance robots) can help these individuals to participate in game activities. Robotically assisted walking or another intensity-based therapy (repetition) has beneficial effects on the recovery and improvement of the patient’s postural and motor functions [
32,
33]. The Robotic therapy device use was placed at the forefront in this case, yet the classic rehabilitation procedures remained as well. We thus, support a variability of approaches most beneficial for a given patient. Besides, the use of elements of integrated rehabilitation seems effective in practice, specifically the cooperation between special education and ergotherapy as two relatively fundamental components in the field of integrated rehabilitation. Close cooperation between the professionals is, thus, beneficial for the patients from several aspects. It is primarily the development of given motor skills from the point of view of medical rehabilitation (ergotherapy) contributing to the improvement of movements, grip precision, or overall stability and a correct walking stereotype training. Educational rehabilitation on the other hand deals not only with the support of motor skills using various worksheets but also provides support for the achievement of the highest possible level of education. In practice, cooperation between these fields forms multidisciplinary teams that purposefully and through various approaches develop entrusted individuals and, thus, increase the professionalism of the rehabilitation activities. This leads to an increase in the number of intervention approaches, which is both desirable and beneficial [
34,
35].
5. Conclusions
In the research, we focused on the description of the condition prior to and after our chosen intervention as the presented results cannot be fully generalized due to the low number of patients. The interventions were run by postdoctoral researchers who ensured the regularity of individual interventions. The presented results show a positive impact of the intervention. It was the approach of the single-case research design method that enabled us to gain a deeper insight into the researched issues. We were also able to rule out possible influences in the development of motor skills in the given patients. This took place during the period without the intervention when it was clear that the conditions of the patients slightly worsened. After the interventions started to take place again, theur situations started to slightly improve again in the monitored indicators of managing daily activities. Based on the presented results, the following is evident. By the time the intervention was omitted, the conditions of the patients began to deteriorate slightly again. For this reason, we can point to the positive impact of combination therapy. This therapy aimed to improve the motor skills of two selected patients. This improvement then led to an overall improvement in the management of normal daily activities—clothing, meals, hygiene, mobility, etc. These activities are greatly influenced by the development of motor skills, and they are also important from the point of view of comprehensive rehabilitation. Nonetheless, our study has some limits, which we list below:
Group equivalence (selection): By using a single-case research method, we addressed two different diagnoses with a common indicator, i.e., motor deficit. With regard to the research survey, it was necessary to reflect on these variables. The initial testing with the widely used standardized tests showed very similar initial results in selected groups and individual participants. In our case, we tried to limit the unequal input conditions (adjusting the requirements for the same testing, deliberately selecting participants corresponding to the relevant features) and create a suitable environment for both groups with the same testing conditions.
Maturation and natural development (growth): We focused on two patients, in whom there was a presumption of classic motor development. This development may have affected the results presented after the end of our intervention; thus, we tried to avoid this situation by using the ABAB method within the single-case research design method. This allowed us to omit the intervention, where the deterioration of the patients is evident. Following the start of the intervention, the situation improved again in the monitored indicators.
Measurement effect (device): The testing was carried out by staff with no interest in publishing the results, and the patients could not influence the testing. In doing so, we tried to achieve the greatest possible degree of objectivity.
Measurement tool error: Testing with the help of a standardized test was performed with no interest in publishing the results. In this way, we minimized the risk of self-involvement and bias in influencing results.
Author Contributions
Conceptualization, L.Z. and J.J.; methodology, M.V.; software, B.L.; validation, M.V., B.L. and L.Z.; formal analysis, J.J.; investigation, M.V.; resources, M.V.; data curation, M.V.; writing—original draft preparation, M.V.; writing—review and editing, M.V.; visualization, B.L.; supervision, L.Z.; project administration, J.J.; funding acquisition, M.V. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by [SGS Jan Evangelista Purkyně University in Ústí nad Labem, Faculty of Education] grant number [UJEP-SGS-2021-43-007-2].
Institutional Review Board Statement
The study was approved by the Ethical Committee Jan Evangelista Purkyně University in Ústí nad Labem, the Czech Republic.
Informed Consent Statement
Informed consent was obtained from all participants included in the study.
Data Availability Statement
The data is available upon reasonable request.
Acknowledgments
Our thanks for the proofreading of our text goes to our colleague, Anthony Laue, M.A.
Conflicts of Interest
The authors declared no potential conflict of interest concerning the research, authorship, and/or publication of this article.
References
- Bradley, C. Definition of childhood in psychiatric literature. Am. J. Psychiatry 1937, 94, 33–36. [Google Scholar] [CrossRef]
- Psychologie Celoživotního Vývoje; Blatný, M. (Ed.) Univerzita Karlova: Prague, Czech Republic; Karolinum Press: Prague, Czech Republic, 2017. [Google Scholar]
- Kraus, J. Dětská Mozková Obrna; Galén: Praha, Czech Republic, 2005. [Google Scholar]
- Kolář, P. Dětská Mozková Obrna. Rehabilitace v Klinické Praxi; Galén: Praha, Czech Republic, 2009. [Google Scholar]
- Graham, H.K.; Rosenbaum, P.; Paneth, N.; Dan, B.; Lin, J.; Damiano, D.L.; Becher, J.G.; Gaebler-Spira, D.; Colver, A.; Reddihough, D.S.; et al. Cerebral palsy. Nat. Rev. Dis Primers 2016, 2, 15082. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, S.; Morgan, C.; Walker, K.; Novak, I. Cerebral Palsy-Don’t Delay. Delay. Dev. Disabil. Res. Rev. 2011, 17, 114–129. [Google Scholar] [CrossRef] [PubMed]
- Spittle, A.J.; Morgan, C.; Olsen, J.E.; Novak, I.; Cheong, J.L. Early diagnosis and treatment of cerebral palsy in children with a history of preterm birth. Clin. Perinatol. 2018, 45, 409–420. [Google Scholar] [CrossRef]
- Sankar, C.; Mundkur, N. Cerebral palsy-definition, classification, etiology and early diagnosis. Indian J. Pediatr. 2005, 72, 865–868. [Google Scholar] [CrossRef] [PubMed]
- Gulati, S.; Sondhi, V. Cerebral palsy: An overview. Indian J. Pediatrics 2018, 85, 1006–1016. [Google Scholar] [CrossRef] [PubMed]
- Lammel, P.; Schulte-Markwort, M. Dyspraxie. Mon. Kinderheilkd. 2017, 165, 490–494. [Google Scholar] [CrossRef]
- Zelinková, O. Dyspraxie. Pedagogika 2007, 57, 58–67. [Google Scholar]
- Gibbs, J.; Appleton, J.; Appleton, R. Dyspraxia or developmental coordination disorder? Unravelling the enigma. Arch. Dis. Child. 2007, 92, 534–539. [Google Scholar] [CrossRef] [PubMed]
- Biotteau, M.; Chais, Y.; Albaret, J. What do we really know about motor learning in children with Developmental Coordination Disorder? Curr. Dev. Disord. Rep. 2016, 3, 152–160. [Google Scholar] [CrossRef] [Green Version]
- Werner, J.; Cermak, M.; Sharon, A.; Aziz-Zadeh, L. Neural Correlates of Developmental Coordination Disorder: The Mirror Neuron System Hypothesis. J. Behav. Brain Sci. 2012, 2, 258–268. [Google Scholar] [CrossRef] [Green Version]
- Blank, R.; Barnett, A.L.; Cairney, J.; Green, D.; Kirby, A.; Polatajko, H.; Rosenblum, S.; Smits-Engelsman, B.; Sugden, D.; Wilson, P. International clinical practice recommendations on the definition, diagnosis, assessment, intervention, and psychosocial aspects of developmental coordination disorder. Dev. Med. Child. Neurol. 2019, 61, 242–285. [Google Scholar] [CrossRef] [PubMed]
- Kolář, P.; Smržová, J.; Kobesová, A. Vývojová porucha koordinace–vývojová dyspraxie. Cesk Slov. Neurol. N 2011, 74, 5. [Google Scholar]
- Blahutková, M.; Brůžková, L.; Matějková, E.; Trávníková, D. Psychomotorická Terapie; Masarykova Univerzita: Brno, Czech Republic, 2009. [Google Scholar]
- Adámková-Ségard, M.; Hátlová, B. Psychomotor Therapy: In the Treatment of Schizofrenia; Univerzita J. E. Purkyně: Ústí nad Labem, Czech Republic, 2012. [Google Scholar]
- Vostrý, M.; Škoda, J.; Doulík, P.; Pančocha, K.; Kynštová, H. Efektivita Edukační Intervence u Osob Trpících Alzheimerovou Chorobou; Jan Evangelista Purkyně University in Ústí nad Labem: Ústí nad Labem, Czech Republic, 2018. [Google Scholar]
- Vostrý, M. Selected Opportunities for access to geriatric clients from the perspective of assisting professions. J. Educ. Cult. Soc. 2018, 8, 89–95. [Google Scholar] [CrossRef]
- Anguera, J.A.; Boccanfuso, J.; Rintoul, J.L.; Al-Hashimi, O.; Faraji, F.; Janowich, J.; Kong, E.; Larraburo, Y.; Rolle, C.; Johnston, E.; et al. Video game training enhances cognitive kontrol in older adults. Nature 2013, 501, 97–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hsieh, Y.; Lin, K.; Wu, C.; Shih, T.; Li, M.; Chen, C. Comparison of proximal versus distal upper-limb robotic rehabilitation on motor performance after stroke: A cluster controlled trial. Sci. Rep. 2018, 8, 2091. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ficher, S.; Ptáček, R.; Žukov, I.; Sláma, K. Účinky robotické rehabilitace chůze na psychosomatické indikátory u osob s různou etiologií lehké mentální retardace. Cesk Slov. Neurol. N 2017, 80, 695–699. [Google Scholar] [CrossRef]
- Wiart, L.; Rosychuk, R.J.; Wright, F.V. Evaluation of the effectiveness of robotic gaint training and gait-focused physical therapy programs for children and youth with cerebral palsy: A mixed methods. BMC Neurol. 2016, 16, 86. [Google Scholar] [CrossRef] [Green Version]
- Druzbicki, M.; Rusek, V.; Snela, S.; Dudek, J.; Szczepanik, M.; Zak, E.; Durmala, J.; Czernuszenko, A.; Bonikowski, M.; Sobota, G. Functional efects of robotic-assistend locomotor treadmill therapy in children with cerebral palsy. J. Rehabil. Med. 2013, 45, 358–363. [Google Scholar] [CrossRef] [Green Version]
- El-Shamy, S.M. Efficacy of Armeo® Robotic Therapy Versus Conventional Therapy on Upper Limb Function in Children with Hemiplegic Cerebral Palsy. Am. J. Phys. Med. Rehabil. 2018, 97, 164–169. [Google Scholar] [CrossRef]
- Buitrago, J.A.; Bolaños, A.M.; Caicedo Bravo, E. A motor learning therapeutic intervention for a child with cerebral palsy through a social assistive robot. Disabil. Rehabil. Assist. Technol. 2020, 15, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Feil-seifer, D.; Matari, M.J. Defining socially assistive robotics. In Proceedings of the 9th International Conference on Rehabilitation Robotics, Chicago, IL, USA, 28 June–1 July 2005; pp. 465–468. [Google Scholar]
- Tapus, A.; Maja, M.; Scassellatti, B. The grand challenges in socially assistive robotics. IEEE Robot. Autom. Mag. 2013, 14, 35–42. [Google Scholar] [CrossRef]
- Gavora, M. Metody Pedagogického Výzkumu: Základy Kvantitativního Výzkumu, 2, Aktualizované Vydání; Galén: Praha, Czech Republic, 2016. [Google Scholar]
- Ammann-Reiffer, C.; Bastiaenen, C.H.G.; Meyer-Heim, A.D.; van Hedel, H.J.A. Effectiveness of robot-assisted gait training in children with cerebral palsy: A bicenter, pragmatic, randomized, cross-over trial. BMC Pediatr. 2017, 17, 64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Najafi, M.; Sharifi, M.; Adams, K.; Tavakoli, M. Robotic assistance for children with cerebral palsy based on learning from tele-cooperative demonstration. Int. J. Intell Robot. Appl. 2017, 1, 43–54. [Google Scholar] [CrossRef]
- Wallard, L.; Dietrich, G.; Kerlirzin, Y.; Bredin, J. Robotic-assisted gait training improves walking abilities in diplegic children with cerebral palsy. Eur. J. Paediatr. Neurol. 2017, 21, 557–564. [Google Scholar] [CrossRef] [PubMed]
- Lins, A.A.; de Oliveira, J.M.; Rodriques, J.J.; Albuquerque, V.H. (Robot-assisted therapy for rehabilitation of children with cerebral palsy—A complementary and alternative approach. Comput. Hum. Beahavior 2019, 100, 152–167. [Google Scholar] [CrossRef]
- Yokoshi, K. Gait patterns in spastic diplegia and periventricular leukomalacia. Brain Dev. 2012, 23, 34–37. [Google Scholar] [CrossRef]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).





{kind=link}