
Factors Explaining Adolescent Girls’ Eating Habits in Urban Benin: A Qualitative Study

Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Sampling
2.2. Data Collection
2.3. Data Analysis
3. Results
3.1. Descriptive Findings
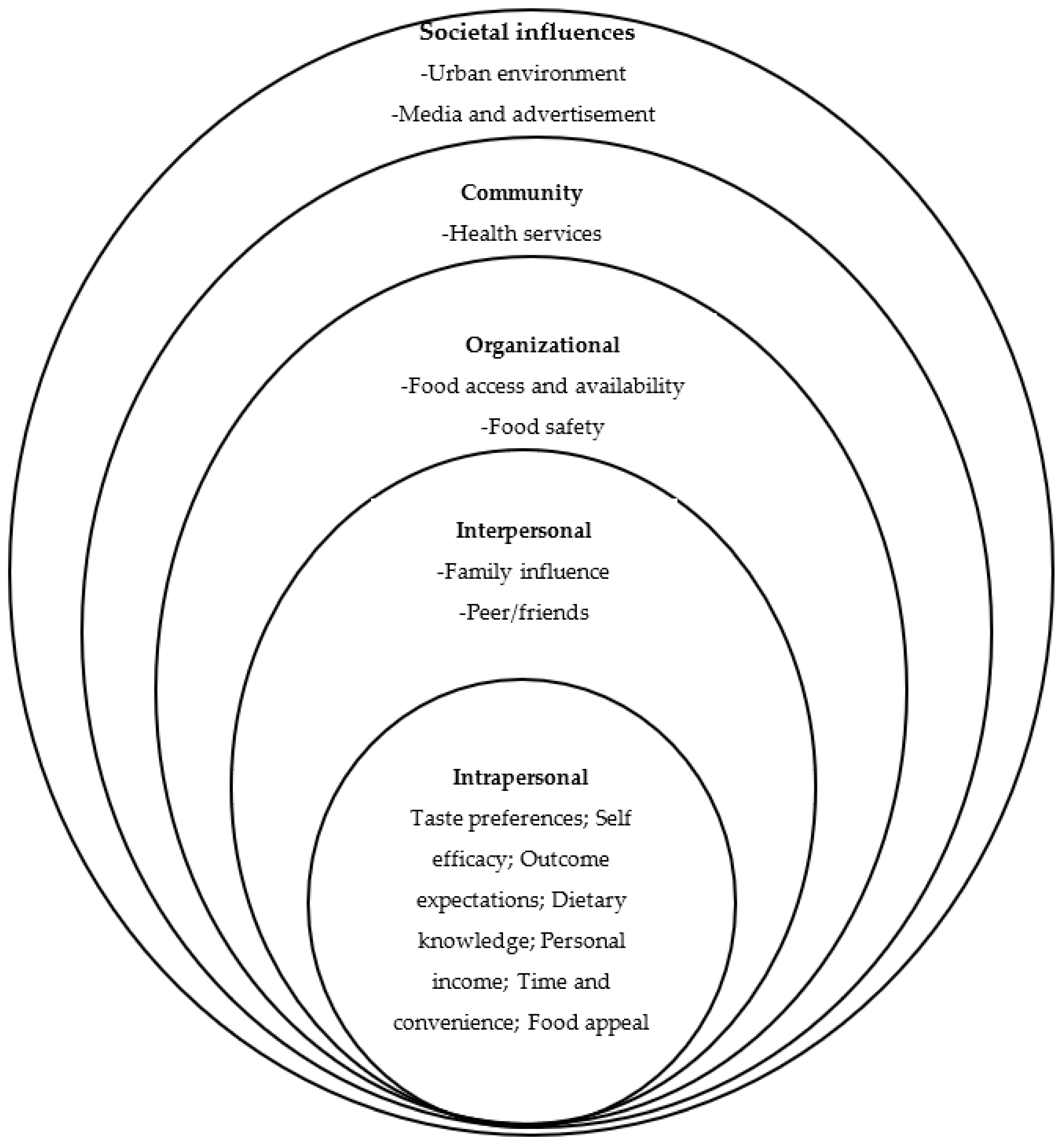
3.2. Factors Influencing Adolescent Girls’ Eating Habits
3.2.1. Individual Factors
- Taste preferences
“Food taste and smell are important to me” (18- to 19-year, Focus group discussions 4, Public school)
“I can’t stop eating sweet foods, I am fond of their taste” (18- to 19-year, Focus group discussions 11, Public school)
“I don’t like vegetable’ taste” (18- to 19-year, Interview 3, Private school)
- Self-efficacy
- Outcome expectations
“I don’t eat fast-food like shawarma because it gives me allergies” (15- to 17-year, Interview 2, Private school)
“A day without sweets can get me feel sick” (18- to 19-year, Focus group discussions 1, Public school).
- Dietary knowledge
“I know that overconsumption of chocolate and biscuits is unhealthy…()…I’m just unaware of the recommended daily intake” (18- to 19-year, Focus group discussions 2, Public school)
“Healthy eating also depends on one’s blood type. My own doesn’t allow me to take orange” (18- to 19-year, Focus group discussions 8, Private school)
- Personal income
- Time and convenience
- Food appeal
3.2.2. Interpersonal Factors
- Family influence
“If mom decides to cook maize dough, that’s what we are all going to eat at home. It makes me like dough finally” (15- to 17-years, Focus group discussions 1)
“Only when overindulging sweet food, my father yells at me to stop eating that” (18- to 19-year, Interview 6)
- Peers/Friends
“I have a friend who always feels snacking to stay awake in class. I don’t know how but now I’m tempted to snack not to sleep” (18- to 19-year, Focus group discussions 11, Public school)
“On a friends’ birthday in a restaurant, I have been presented hamburger as the main menu and I couldn’t refuse. Since that day, I start consuming that.” (15- to 17-years, Focus group discussions 10, Private school)
3.2.3. Institutional or Organizational Factors
- Food access and availability
“There are no fruits to buy in the canteen. During the break we eat biscuits, chips, candies or toffies.” (18- to 19-year, Interview3, Public school)
- Food safety
3.2.4. Community Factors
- Health services
3.2.5. Societal Influences
- Urban environment
- Media and advertisement
“Advertisement about any kind of food motivates me to eat it.” (15- to 17-years, Interview2, Private school)
“I tried the food called pancake after seeing it on TV. It was good” (18- to 19-year, Focus group discussions 8, Private school).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Question Guide | |
|---|---|
| Questions | |
| Introduction | Please introduce yourself Describe a bit what you ate yesterday |
| Key questions | What factors influence the type of food you usually consume? For each factor, probe the participants with stimulating questions such as “could you tell us more? Please give an example; Please describe what you mean; ” Is there anything else? What are the most important factors influencing your eating behaviours? |
| Ending question | Is there anything else you would like to add? Or forgot to mention? |
| Closing session | All your answers will help us understand what explains your eating behaviours. Your answers and discussions have been very helpful and informative. We thank you for the information you provided us. Do you have any questions or suggestions? |
References
- Gebremariam, H. Assessment of Nutritional Status and Associated Factors among School Going Adolescents of Mekelle City, Northern Ethiopia. Int. J. Nutr. Food Sci. 2015, 4, 118. [Google Scholar] [CrossRef]
- United Nations Population Fund. World Population Dashboard. 2018. Available online: https://www.unfpa.org/data/world-population-dashboard (accessed on 3 March 2019).
- Caleyachetty, R.; Thomas, G.N.; Kengne, A.P.; Echouffo-Tcheugui, J.B.; Schilsky, S.; Khodabocus, J.; Uauy, R. The Double Burden of Malnutrition among Adolescents: Analysis of Data from the Global School-Based Student Health and Health Behavior in School-Aged Children Surveys in 57 Low- and Middle-Income Countries. Am. J. Clin. Nutr. 2018, 108, 414–424. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Guideline: Implementing Effective Actions for Improving Adolescent Nutrition; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Elizondo-Montemayor, L.; Hernández-Escobar, C.; Lara-Torre, E.; Nieblas, B.; Gómez-Carmona, M. Gynecologic and Obstetric Consequences of Obesity in Adolescent Girls. J. Pediatr. Adolesc. Gynecol. 2017, 30, 156–168. [Google Scholar] [CrossRef] [PubMed]
- Hoteyi, S.M.I.; Gnimadi, C.C.; Adjadji, G.V.; Igue, A.M.; Mensah, G.A. Alimentation de Rue Des Populations: Une Santé En Péril à Cotonou Au Sud-Bénin? BRAB 2014, 21–34. Available online: https://publications-chercheurs.inrab.org/uploads/fichiers/lots2/BRAB_2014%20%C3%A0%202018/BRAB_2014/BRAB_N%C2%B0%20Sp%C3%A9cial%20ABSP%202014/Article%203_BRAB%20N%C2%B0%20sp%C3%A9cial%20ABSP_septembre%202014_Hoteyi%20et%20al_Alimentation%20de%20rue%20des%20populations.pdf (accessed on 1 April 2022).
- Houinato, O.A.; Kpozehouen, A.; Hounkpatin, B.; Gbédji, K.Y.; Robin, H.; Mizéhoun-Adissoda, C.; Guédou, F.; Houinato, D.S.; Perrin, R.X. Prevalence and Factors Associated with Overweight and Obesity among Adolescents in Schools in Benin in 2016. Open J. Epidemiol. 2019, 9, 213. [Google Scholar] [CrossRef]
- Badr, H.E.; Lakha, S.F.; Pennefather, P. Differences in physical activity, eating habits and risk of obesity among Kuwaiti adolescent boys and girls: A population-based study. Int. J. Adolesc. Med. Health 2017, 31. [Google Scholar] [CrossRef]
- Okeyo, A.P.; Seekoe, E.; de Villiers, A.; Faber, M.; Nel, J.H.; Steyn, N.P. Dietary Practices and Adolescent Obesity in Secondary School Learners at Disadvantaged Schools in South Africa: Urban-Rural and Gender Differences. Int. J. Environ. Res. Public Health 2020, 17, 5864. [Google Scholar] [CrossRef]
- Feeley, A.B.; Norris, S.A. Added sugar and dietary sodium intake from purchased fast food, confectionery, sweetened beverages and snacks among Sowetan adolescents. S. Afr. J. Child Health 2014, 8, 88–91. [Google Scholar] [CrossRef]
- National Department of Health (NDoH); Statistics South Africa (Stats SA); South African Medical Research Council (SAMRC); ICF. South Africa Demographic and Health Survey Pretoria, South Africa, and Rockville, Maryland, USA: NDoH, Stats SA, SAMRC, and ICF. Available online: http://dhsprogram.com/pubs/pdf/PR84/PR84.pdf (accessed on 18 March 2022).
- 2021 Global Nutrition Report: The State of Global Nutrition; Development Initiatives: Bristol, UK, 2022; Available online: https://globalnutritionreport.org/resources/nutrition-profiles/africa/western-africa/benin/ (accessed on 5 March 2022).
- Bhutta, Z.A.; Lassi, Z.S.; Bergeron, G.; Koletzko, B.; Salam, R.; Diaz, A.; McLean, M.; Black, R.E.; De-Regil, L.M.; Christian, P.; et al. Delivering an Action Agenda for Nutrition Interventions Addressing Adolescent Girls and Young Women: Priorities for Implementation and Research. Ann. N. Y. Acad. Sci. 2017, 1393, 61–71. [Google Scholar] [CrossRef]
- Stephenson, J.; Heslehurst, N.; Hall, J.; Schoenaker, D.A.J.M.; Hutchinson, J.; Cade, J.E.; Poston, L.; Barrett, G.; Crozier, S.R.; Barker, M.; et al. Before the Beginning: Nutrition and Lifestyle in the Preconception Period and Its Importance for Future Health. Lancet 2018, 391, 1830–1841. [Google Scholar] [CrossRef]
- Keats, E.C.; Rappaport, A.I.; Shah, S.; Oh, C.; Jain, R.; Bhutta, Z.A. The Dietary Intake and Practices of Adolescent Girls in Low-and Middle-Income Countries: A Systematic Review. Nutrients 2018, 10, 1978. [Google Scholar] [CrossRef]
- Akseer, N.; Al-Gashm, S.; Mehta, S.; Mokdad, A.; Bhutta, Z.A. Global and Regional Trends in the Nutritional Status of Young People: A Critical and Neglected Age Group. Ann. N. Y. Acad. Sci. 2017, 1393, 3–20. [Google Scholar] [CrossRef]
- Loaiza, E.; Liang, M. Adolescent Pregnancy: A Review of the Evidence. Unfpa. 2013. Available online: https://www.unfpa.org/sites/default/files/pub-pdf/ADOLESCENT%20PREGNANCY_UNFPA.pdf (accessed on 5 March 2022).
- Khara, T.; Mates, E.; Mason, F. Adolescent Nutrition: Policy and Programming in SUN+ Countries; Save the Children: London, UK, 2015; Available online: https://resourcecentre.savethechildren.net/pdf/adolescent_nutrition.pdf/ (accessed on 5 March 2022).
- Dodd, J.M.; Grivell, R.M.; Nguyen, A.M.; Chan, A.; Robinson, J.S. Maternal and perinatal health outcomes by body mass index category. Aust. N. Z. J. Obstet. Gynaecol. 2011, 51, 136. [Google Scholar] [CrossRef]
- International Food Policy Research Institute. Global Nutrition Report 2014: Actions and Accountability to Accelerate the World’s Progress on Nutrition; International Food Policy Research Institute (IFPRI): Washington, DC, USA; Available online: https://www.ifpri.org/publication/global-nutrition-report-2014-actions-and-accountability-accelerate-worlds-progress (accessed on 5 March 2022).
- Nago, E.S.; Lachat, C.K.; Huybregts, L.; Roberfroid, D.; Dossa, R.A.; Kolsteren, P.W. Food, Energy and Macronutrient Contribution of out-of-Home Foods in School-Going Adolescents in Cotonou, Benin. Br. J. Nutr. 2010, 103, 281–288. [Google Scholar] [CrossRef]
- Darboux, A.J.; Sossa, J.C.; Falola, L.G. Study of the Food Offer and Eating Behavior of Adolescents in Private and Public Secondary Schools in Benin: Case of Three Schools in Cotonou. Int. J. Innov. Appl. Stud. 2019, 27, 410–416. [Google Scholar]
- Benedict, R.; Schmale, A.; Namaste, S. Adolescent Nutrition 2000–2017: DHS Data on Adolescents Age 15–19; ICF International: Rockville, MD, USA, 2018; pp. 15–19. [Google Scholar]
- Tucunduva Philippi, S.; Guerra, P.H.; Barco Leme, A.C. Health Behavioral Theories Used to Explain Dietary Behaviors in Adolescents: A Systematic Review. Nutrire 2016, 41, 22. [Google Scholar] [CrossRef]
- Birru, S.M.; Tariku, A.; Belew, A.K. Improved Dietary Diversity of School Adolescent Girls in the Context of Urban Northwest Ethiopia: 2017. Ital. J. Pediatr. 2018, 44, 48. [Google Scholar] [CrossRef]
- Yirga, B.; Assefa Gelaw, Y.; Derso, T.; Wassie, M.M. Disordered Eating Attitude and Associated Factors among High School Adolescents Aged 12–19 Years in Addis Ababa, Ethiopia: A Cross-Sectional Study. BMC Res. Notes 2016, 9, 503. [Google Scholar] [CrossRef]
- Moreno-Maldonado, C.; Ramos, P.; Moreno, C.; Rivera, F. How Family Socioeconomic Status, Peer Behaviors, and School-Based Intervention on Healthy Habits Influence Adolescent Eating Behaviors. Sch. Psychol. Int. 2018, 39, 92–118. [Google Scholar] [CrossRef]
- Vilela, S.; Muresan, I.; Correia, D.; Severo, M.; Lopes, C. The Role of Socioeconomic Factors in Food Consumption of Portuguese Children and Adolescents: Results from the National Food, Nutrition and Physical Activity Survey 2015. Br. J. Nutr. 2020, 124, 591–601. [Google Scholar] [CrossRef]
- Delfino, L.D.; Tebar, W.R.; Silva, D.A.S.; Gil, F.C.S.; Mota, J.; Christofaro, D.G.D. Food Advertisements on Television and Eating Habits in Adolescents: A School-Based Study. Rev. Saude. Publica. 2020, 54, 55. [Google Scholar] [CrossRef] [PubMed]
- ALFaris, N.A.; Al-Tamimi, J.Z.; Al-Jobair, M.O.; Al-Shwaiyat, N.M. Trends of Fast Food Consumption among Adolescent and Young Adult Saudi Girls Living in Riyadh. Food Nutr. Res. 2015, 59, 26488. [Google Scholar] [CrossRef] [PubMed]
- Said, L.; Gubbels, J.S.; Kremers, S.P.J. Dietary Knowledge, Dietary Adherence, and BMI of Lebanese Adolescents and Their Parents. Nutrients 2020, 12, 2398. [Google Scholar] [CrossRef] [PubMed]
- McLeroy, K.R.; Bibeau, D.; Steckler, A.; Glanz, K. An Ecological Perspective on Health Promotion Programs. Health Educ. Q. 1988, 15, 351–377. [Google Scholar] [CrossRef] [PubMed]
- Keeley, B.; Little, C.; Zuehlke, E. The State of the World’s Children Children, Food and Nutrition: Growing Well in a Changing World; United Nations Children’s Fund: New York, NY, USA, 2019; Available online: https://www.unicef.org/reports/state-of-worlds-children-2019 (accessed on 5 March 2022).
- Institut National de la Statistique et de l’Analyse Économique (INSAE); ICF. Enquête Démographique et de Santé 2017–2018; Cotonou: Bénin et Rockville, MD, USA, 2019. [Google Scholar]
- Delisle, H.; Chandra-Mouli, V.; Benoist, B. Should Adolescents Be Specifically Targeted for Nutrition in Developing Countries? To Address Which Problems, and How? WHO: Geneva, Switzerland, 2005. [Google Scholar]
- Katz, D.L.; O’Connell, M.; Njike, V.Y.; Yeh, M.-C.; Nawaz, H. Strategies for the Prevention and Control of Obesity in the School Setting: Systematic Review and Meta-Analysis. Int. J. Obes. 2008, 32, 1780–1789. [Google Scholar] [CrossRef] [PubMed]
- Morgan, D.L.; Krueger, R.A.; Scannell, A.U. Planning Focus Groups; Sage: Newcastle upon Tyne, UK, 1998. [Google Scholar]
- Davey Smith, G.; Hart, C.; Hole, D.; MacKinnon, P.; Gillis, C.; Watt, G.; Blane, D.; Hawthorne, V. Education and occupational social class: Which is the more important indicator of mortality risk? J. Epidemiol. Community Health 1998, 52, 153–160. [Google Scholar] [CrossRef]
- Sherar, L.B.; Griffin, T.P.; Ekelund, U.; Cooper, A.R.; Esliger, D.W.; van Sluijs, E.M.; Bo Andersen, L.; Cardon, G.; Davey, R.; Froberg, K.; et al. Association between maternal education and objectively measured physical activity and sedentary time in adolescents. J. Epidemiol. Community Health 2016, 70, 541–548. [Google Scholar] [CrossRef]
- Wamani, H.; Tylleskär, T.; Astrøm, A.N.; Tumwine, J.K.; Peterson, S. Mothers’ education but not fathers’ education, household assets or land ownership is the best predictor of child health inequalities in rural Uganda. Int. J. Equity Health 2004, 3, 9. [Google Scholar] [CrossRef]
- Bandura, A. Health Promotion from the Perspective of Social Cognitive Theory. Psychol. Health 1998, 13, 623–649. [Google Scholar] [CrossRef]
- Fitzgerald, A.; Heary, C.; Kelly, C.; Nixon, E.; Shevlin, M. Self-Efficacy for Healthy Eating and Peer Support for Unhealthy Eating Are Associated with Adolescents’ Food Intake Patterns. Appetite 2013, 63, 48–58. [Google Scholar] [CrossRef]
- Pedersen, S.; Grønhøj, A.; Thøgersen, J. Following Family or Friends. Social Norms in Adolescent Healthy Eating. Appetite 2015, 86, 54–60. [Google Scholar] [CrossRef] [PubMed]
- Liem, D.G.; Russell, C.G. The Influence of Taste Liking on the Consumption of Nutrient Rich and Nutrient Poor Foods. Front. Nutr. 2019, 15. [Google Scholar] [CrossRef] [PubMed]
- Dazeley, P.; Houston-Price, C. Exposure to foods’ non-taste sensory properties. A nursery intervention to increase children’s willingness to try fruit and vegetables. Appetite 2015, 84, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 1977, 84, 191–215. [Google Scholar] [CrossRef]
- Bagherniya, M.; Sharma, M.; Mostafavi Darani, F.; Maracy, M.R.; Safarian, M.; Allipour Birgani, R.; Bitarafan, V.; Keshavarz, S.A. School-Based Nutrition Education Intervention Using Social Cognitive Theory for Overweight and Obese Iranian Adolescent Girls: A Cluster Randomized Controlled Trial. Int. Q. Community Health Education. 2017, 38, 37–45. [Google Scholar] [CrossRef]
- Kuroko, S.; Black, K.; Chryssidis, T.; Finigan, R.; Hann, C.; Haszard, J.; Jackson, R.; Mahn, K.; Robinson, C.; Thomson, C. Create Our Own Kai: A Randomised Control Trial of a Cooking Intervention with Group Interview Insights into Adolescent Cooking Behaviours. Nutrients 2020, 12, 796. [Google Scholar] [CrossRef]
- El-Ammari, A.; El Kazdouh, H.; Bouftini, S.; El Fakir, S.; El Achhab, Y. Social-Ecological Influences on Unhealthy Dietary Behaviours among Moroccan Adolescents: A Mixed-Methods Study. Public Health Nutr. 2020, 23, 996–1008. [Google Scholar] [CrossRef]
- Banna, J.C.; Buchthal, O.V.; Delormier, T.; Creed-Kanashiro, H.M.; Penny, M.E. Influences on Eating: A Qualitative Study of Adolescents in a Periurban Area in Lima, Peru. BMC Public Health 2016, 16, 40. [Google Scholar] [CrossRef]
- Bandura, A. Health Promotion by Social Cognitive Means. Health Educ. Behav. 2004, 31, 143–164. [Google Scholar] [CrossRef]
- DiClemente, R.J.; Salazar, L.F.; Crosby, R.A. Health Behavior Theory for Public Health: Principles, Foundations, and Applications; Jones & Bartlett Learning: Burlington, MA, USA, 2013. [Google Scholar]
- Brown, C.; Shaibu, S.; Maruapula, S.; Malete, L.; Compher, C. Perceptions and Attitudes towards Food Choice in Adolescents in Gaborone, Botswana. Appetite 2015, 95, 29–35. [Google Scholar] [CrossRef]
- Shaw, S.; Correia Simao, S.; Jenner, S.; Lawrence, W.T.; Woods-Townsend, K.; Vogel, C.A.; Farrell, D.; Inskip, H.; Baird, J.; Morrison, L.; et al. Parental Perspectives on Negotiations over Diet and Physical Activity: How Do We Involve Parents in Adolescent Health Interventions? Public Health Nutr. 2021, 24, 2727–2736. [Google Scholar] [CrossRef] [PubMed]
- Boatemaa, S.; Badasu, D.M.; de-Graft Aikins, A. Food Beliefs and Practices in Urban Poor Communities in Accra: Implications for Health Interventions. BMC Public Health 2018, 18, 434. [Google Scholar] [CrossRef] [PubMed]
- Rathi, N.; Riddell, L.; Worsley, A. What Influences Urban Indian Secondary School Students’ Food Consumption?—A Qualitative Study. Appetite 2016, 105, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Voorend, C.G.N.; Norris, S.A.; Griffiths, P.L.; Sedibe, M.H.; Westerman, M.J.; Doak, C.M. “We Eat Together; Today She Buys, Tomorrow I Will Buy the Food”: Adolescent Best Friends’ Food Choices and Dietary Practices in Soweto, South Africa. Public Health Nutr. 2013, 16, 559–567. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.C. Social Comparison and Body Image: Attractiveness Comparisons to Models and Peers Among Adolescent Girls and Boys. Sex. Roles 2001, 45, 645–664. [Google Scholar] [CrossRef]
- Mellanby, A.R.; Rees, J.B.; Tripp, J.H. Peer-Led and Adult-Led School Health Education: A Critical Review of Available Comparative Research. Health Educ. Res. 2000, 15, 533–545. [Google Scholar] [CrossRef]
- Campbell, R.; Starkey, F.; Holliday, J.; Audrey, S.; Bloor, M.; Parry-Langdon, N.; Hughes, R.; Moore, L. An Informal School-Based Peer-Led Intervention for Smoking Prevention in Adolescence (ASSIST): A Cluster Randomised Trial. Lancet 2008, 371, 1595–1602. [Google Scholar] [CrossRef]
- Ghaffar, S.A.; Talib, R.A.; Karim, N.A. Food Choices and Diet Quality in the School Food Environment: A Qualitative Insight from the Perspective of Adolescents. Malays. J. Med. Health Sci. 2019, 15. Available online: https://medic.upm.edu.my/upload/dokumen/2019041008170103_MJMHS_Vol_15_SP1.pdf (accessed on 18 March 2022).
- Sondari, M.; Brouwer, I.; Februhartanty, J. Eating Behaviour of Adolescent Schoolgirls in Malang, East Java: A Qualitative Study. Malays. J. Nutr. 2019, 25, 87–96. [Google Scholar]
- Sedibe, H.M.; Kahn, K.; Edin, K.; Gitau, T.; Ivarsson, A.; Norris, S.A. Qualitative Study Exploring Healthy Eating Practices and Physical Activity among Adolescent Girls in Rural South Africa. BMC Pediatr. 2014, 14, 211. [Google Scholar] [CrossRef]
- Stephens, L.D.A.; McNaughton, S.A.; Crawford, D.; MacFarlane, A.; Ball, K. Correlates of Dietary Resilience among Socioeconomically Disadvantaged Adolescents. Eur. J. Clin. Nutr. 2011, 65, 1219–1232. [Google Scholar] [CrossRef]
- Holtom-Viesel, A.; Allan, S. A systematic review of the literature on family functioning across all eating disorder diagnoses in comparison to control families. Clin. Psychol. Rev. 2014, 34, 29–43. [Google Scholar] [CrossRef] [PubMed]
- George, M.W.; Fairchild, A.J.; Mark Cummings, E.; Davies, P.T. Marital conflict in early childhood and adolescent disordered eating: Emotional insecurity about the marital relationship as an explanatory mechanism. Eat Behav. 2014, 15, 532–539. [Google Scholar] [CrossRef] [PubMed]
- Berge, J.M.; MacLehose, R.F.; Meyer, C.; Didericksen, K.; Loth, K.A.; Neumark-Sztainer, D. He Said, She Said: Examining Parental Concordance on Home Environment Factors and Adolescent Health Behaviors and Weight Status. J. Acad. Nutr. Diet 2016, 116, 46–60. [Google Scholar] [CrossRef] [PubMed]
- Doku, D.; Koivusilta, L.; Raisamo, S.; Rimpelä, A. Socio-economic differences in adolescents’ breakfast eating, fruit and vegetable consumption and physical activity in Ghana. Public Health Nutr. 2013, 16, 864–872. [Google Scholar] [CrossRef]
- Razzak, A.; Juliana, F.M.; Hossain, S.; Asaduzzaman, S.U. Socio-demography characteristics of parents of the adolescent girls in a nutrition education based intervention study in rural Bangladesh. J. Nutr. Health Food Eng. 2017, 7, 281. [Google Scholar] [CrossRef]
- Jesson, J.; Kouakou, E.K.V.; Hardy-Johnson, P.; Ngoran-Theckly, P.; Kehoe, S.H.; Adonis, L.; Fall, C.; Leroy, V.; Barker, M.; Weller, S. Adolescent Nutrition and Physical Activity in Low-Income Suburbs of Abidjan, Côte d’Ivoire: The Gap between Knowledge, Aspirations and Possibilities. Public Health Nutr. 2021, 24, 5227–5237. [Google Scholar] [CrossRef]

| Focus Groups (n = 77) | Individual Interviews (n = 7) | ||
|---|---|---|---|
| Age in years (mean ± SD) | 16.53 ± 1.1 | 17 ± 1.1 | |
| Participant education level n (%) | Grade 5 | 39 | 42.8 |
| Grade 6 | 20.8 | 28.6 | |
| Grade 7 | 40.2 | 28.6 | |
| School character n (%) | Public schools | 63.6 | 57.1 |
| Private schools | 36.4 | 42.9 | |
| Living with n (%) | Mother | 75.3 | 71.4 |
| Others (grand-parents, uncle/aunt, sister/brother) | 24.7 | 2.6 | |
| Mothers’ educational level n (%) | Primary and below | 27.3 | 57.1 |
| Secondary | 22.1 | 28.6 | |
| Higher (Bachelor, Master, Doctorate) | 5.1 | 14.3 | |
| Mothers’ main occupation n (%) | Employee | 18.2 | 28.6 |
| Handicraft | 16.9 | 0 | |
| Tradeswoman | 55.8 | 57.1 | |
| Housekeeper | 9.1 | 14.3 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mama Chabi, S.; Fanou-Fogny, N.; Nago Koukoubou, E.; Deforche, B.; Van Lippevelde, W. Factors Explaining Adolescent Girls’ Eating Habits in Urban Benin: A Qualitative Study. Adolescents 2022, 2, 205-219. https://doi.org/10.3390/adolescents2020017
Mama Chabi S, Fanou-Fogny N, Nago Koukoubou E, Deforche B, Van Lippevelde W. Factors Explaining Adolescent Girls’ Eating Habits in Urban Benin: A Qualitative Study. Adolescents. 2022; 2(2):205-219. https://doi.org/10.3390/adolescents2020017
Chicago/Turabian StyleMama Chabi, Sherifath, Nadia Fanou-Fogny, Eunice Nago Koukoubou, Benedicte Deforche, and Wendy Van Lippevelde. 2022. "Factors Explaining Adolescent Girls’ Eating Habits in Urban Benin: A Qualitative Study" Adolescents 2, no. 2: 205-219. https://doi.org/10.3390/adolescents2020017
APA StyleMama Chabi, S., Fanou-Fogny, N., Nago Koukoubou, E., Deforche, B., & Van Lippevelde, W. (2022). Factors Explaining Adolescent Girls’ Eating Habits in Urban Benin: A Qualitative Study. Adolescents, 2(2), 205-219. https://doi.org/10.3390/adolescents2020017