
ERBB2-Mutant Gastrointestinal Tumors Represent Heterogeneous Molecular Biology, Particularly in Microsatellite Instability, Tumor Mutation Burden, and Co-Mutated Genes: An In Silico Study
Abstract

1. Introduction
2. Materials and Methods
2.1. Data Collection of EAC, GC, and CRC Cases
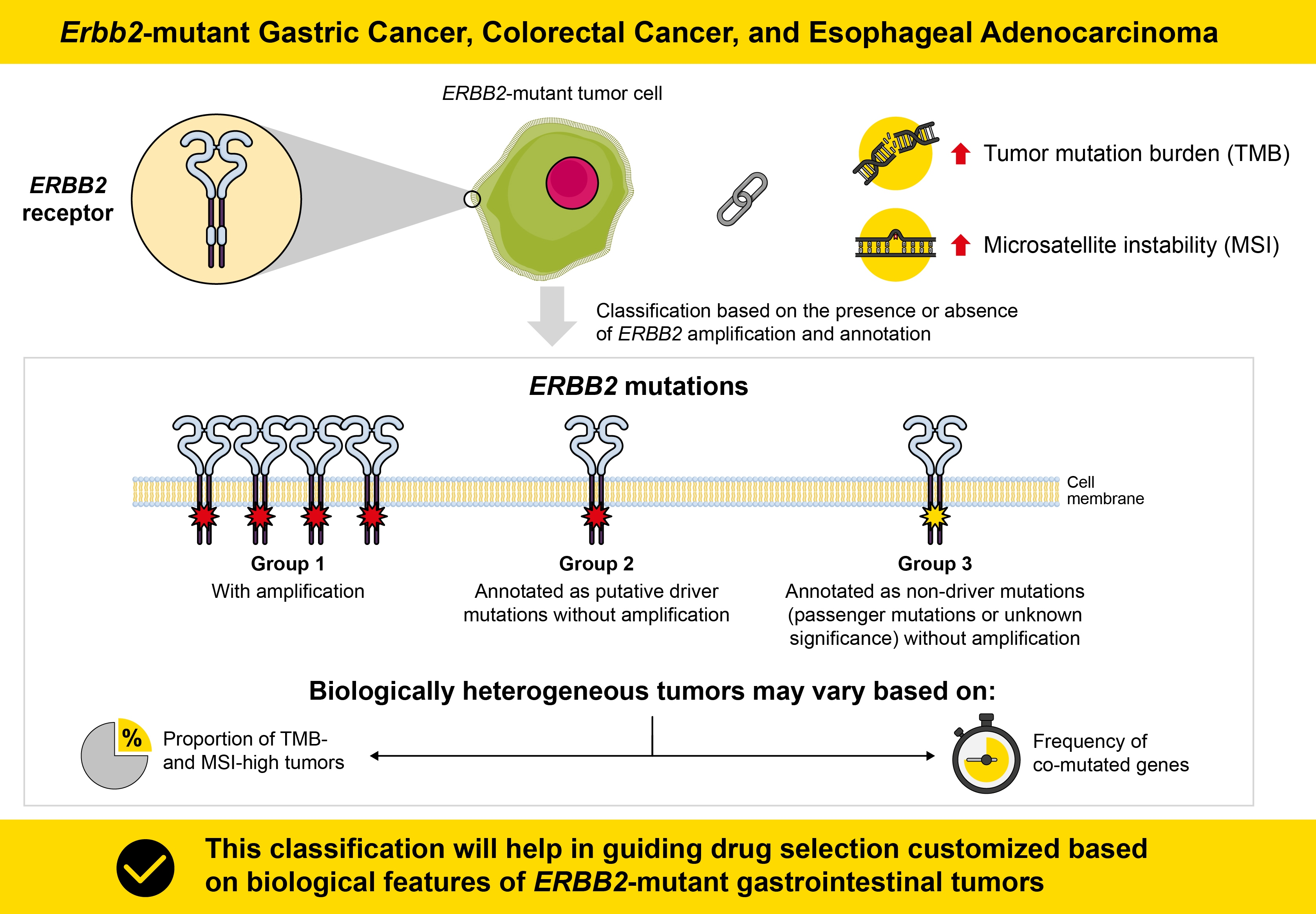
2.2. Molecular Subtype Classification
2.3. MSI Analysis
2.4. TMB Estimation
2.5. Comparison of MS Status and TMB between ERBB2-Mutant and ERBB2-Wild-Type EAC, GC, and CRC
2.6. Comparison of Clinicopathological and Molecular Features among the Three Groups Each of EAC, GC, and CRC
2.7. Analysis of ERBB2 Amplifications and Mutations in Signaling Pathways in EAC, GC, and CRC Samples and Comparison of the Frequencies of Genetic Variants in Each Group
2.8. Statistical Analysis
3. Results
3.1. Comparison of MS Status and TMB between ERBB2-Mutant and ERBB2-Wild-Type EAC, GC, and CRC
3.2. Classification of ERBB2-Mutant EAC, GC, and CRC and Clinicopathological Features of the Groups
3.3. Genomic Landscape of Somatic Mutations and Comparison of Somatic Mutations among the EAC, GC, and CRC Groups
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hyman, D.M.; Piha-Paul, S.A.; Won, H.; Rodon, J.; Saura, C.; Shapiro, G.I.; Juric, D.; Quinn, D.I.; Moreno, V.; Doger, B.; et al. HER kinase inhibition in patients with HER2- and HER3-mutant cancers. Nature 2018, 554, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Miao, J.; Wen, Y.; Xia, X.; Chen, Y.; Huang, M.; Chen, S.; Zhao, Z.; Zhang, Y.; Chen, C.; et al. Molecular landscape of ERBB2 alterations in 14,956 solid tumors. Pathol. Oncol. Res. 2022, 28, 1610360. [Google Scholar] [CrossRef] [PubMed]
- Connell, C.M.; Doherty, G.J. Activating HER2 mutations as emerging targets in multiple solid cancers. ESMO Open 2017, 2, e000279. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; Ahn, S.; Kim, D.G.; Kim, H.; Kang, S.Y.; Kim, K.M. High frequency of juxtamembrane domain ERBB2 mutation in gastric cancer. Cancer Genom. Proteom. 2022, 19, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Ross, J.S.; Fakih, M.; Ali, S.M.; Elvin, J.A.; Schrock, A.B.; Suh, J.; Vergilio, J.A.; Ramkissoon, S.; Severson, E.; Daniel, S.; et al. Targeting HER2 in colorectal cancer: The landscape of amplification and short variant mutations in ERBB2 and ERBB3. Cancer 2018, 124, 1358–1373. [Google Scholar] [CrossRef]
- Janjigian, Y.Y.; Sanchez-Vega, F.; Jonsson, P.; Chatila, W.K.; Hechtman, J.F.; Ku, G.Y.; Riches, J.C.; Tuvy, Y.; Kundra, R.; Bouvier, N.; et al. Genetic predictors of response to systemic therapy in esophagogastric cancer. Cancer Discov. 2018, 8, 49–58. [Google Scholar] [CrossRef]
- Bang, Y.J.; Van Cutsem, E.; Feyereislova, A.; Chung, H.C.; Shen, L.; Sawaki, A.; Lordick, F.; Ohtsu, A.; Omuro, Y.; Satoh, T.; et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): A phase 3, open-label, randomised controlled trial. Lancet 2010, 376, 687–697. [Google Scholar] [CrossRef]
- Nakamura, Y.; Okamoto, W.; Kato, T.; Esaki, T.; Kato, K.; Komatsu, Y.; Yuki, S.; Masuishi, T.; Nishina, T.; Ebi, H.; et al. Circulating tumor DNA-guided treatment with pertuzumab plus trastuzumab for HER2-amplified metastatic colorectal cancer: A phase 2 trial. Nat. Med. 2021, 27, 1899–1903. [Google Scholar] [CrossRef]
- Sartore-Bianchi, A.; Trusolino, L.; Martino, C.; Bencardino, K.; Lonardi, S.; Bergamo, F.; Zagonel, V.; Leone, F.; Depetris, I.; Martinelli, E.; et al. Dual-targeted therapy with trastuzumab and lapatinib in treatment-refractory, KRAS codon 12/13 wild-type, HER2-positive metastatic colorectal cancer (HERACLES): A proof-of-concept, multicentre, open-label, phase 2 trial. Lancet Oncol. 2016, 17, 738–746. [Google Scholar] [CrossRef]
- Li, B.T.; Smit, E.F.; Goto, Y.; Nakagawa, K.; Udagawa, H.; Mazières, J.; Nagasaka, M.; Bazhenova, L.; Saltos, A.N.; Felip, E.; et al. Trastuzumab deruxtecan in HER2-mutant non-small-cell lung cancer. N. Engl. J. Med. 2022, 386, 241–251. [Google Scholar] [CrossRef]
- Subramanian, J.; Katta, A.; Masood, A.; Vudem, D.R.; Kancha, R.K. Emergence of ERBB2 mutation as a biomarker and an actionable target in solid cancers. Oncologist 2019, 24, e1303–e1314. [Google Scholar] [CrossRef] [PubMed]
- Nagano, M.; Kohsaka, S.; Ueno, T.; Kojima, S.; Saka, K.; Iwase, H.; Kawazu, M.; Mano, H. High-throughput functional evaluation of variants of unknown significance in ERBB2. Clin. Cancer Res. 2018, 24, 5112–5122. [Google Scholar] [CrossRef]
- Loree, J.M.; Bailey, A.M.; Johnson, A.M.; Yu, Y.; Wu, W.; Bristow, C.A.; Davis, J.S.; Shaw, K.R.; Broaddus, R.; Banks, K.C.; et al. Molecular landscape of ERBB2/ERBB3 mutated colorectal cancer. J. Natl. Cancer Inst. 2018, 110, 1409–1417. [Google Scholar] [CrossRef]
- Uchida, S.; Kojima, T.; Sugino, T. Clinicopathological features, tumor mutational burden and tumour-infiltrating lymphocyte interplay in erbb2-mutated breast cancer: In silico analysis. Pathol. Oncol. Res. 2021, 27, 633243. [Google Scholar] [CrossRef] [PubMed]
- Hoadley, K.A.; Yau, C.; Hinoue, T.; Wolf, D.M.; Lazar, A.J.; Drill, E.; Shen, R.; Taylor, A.M.; Cherniack, A.D.; Thorsson, V.; et al. Cell-of-origin patterns dominate the molecular classification of 10,000 tumors from 33 types of cancer. Cell 2018, 173, 291–304.e6. [Google Scholar] [CrossRef] [PubMed]
- Sihag, S.; Nussenzweig, S.C.; Walch, H.S.; Hsu, M.; Tan, K.S.; De La Torre, S.; Janjigian, Y.Y.; Maron, S.B.; Ku, G.Y.; Tang, L.H.; et al. The role of the TP53 pathway in predicting response to neoadjuvant therapy in esophageal adenocarcinoma. Clin. Cancer Res. 2022, 28, 2669–2678. [Google Scholar] [CrossRef]
- Guo, Y.A.; Chang, M.M.; Huang, W.; Ooi, W.F.; Xing, M.; Tan, P.; Skanderup, A.J. Mutation hotspots at CTCF binding sites coupled to chromosomal instability in gastrointestinal cancers. Nat. Commun. 2018, 9, 1520. [Google Scholar] [CrossRef]
- Mondaca, S.; Walch, H.; Nandakumar, S.; Chatila, W.K.; Schultz, N.; Yaeger, R. Specific mutations in APC, but not alterations in DNA damage response, associate with outcomes of patients with metastatic colorectal cancer. Gastroenterology 2020, 159, 1975–1978.e4. [Google Scholar] [CrossRef]
- Chakravarty, D.; Gao, J.; Phillips, S.M.; Kundra, R.; Zhang, H.; Wang, J.; Rudolph, J.E.; Yaeger, R.; Soumerai, T.; Nissan, M.H.; et al. OncoKB: A precision oncology knowledge base. JCO Precis. Oncol. 2017, 2017, PO.17.00011. [Google Scholar] [CrossRef]
- Liu, Y.; Sethi, N.S.; Hinoue, T.; Schneider, B.G.; Cherniack, A.D.; Sanchez-Vega, F.; Seoane, J.A.; Farshidfar, F.; Bowlby, R.; Islam, M.; et al. Comparative molecular analysis of gastrointestinal adenocarcinomas. Cancer Cell 2018, 33, 721–735.e8. [Google Scholar] [CrossRef]
- Niu, B.; Ye, K.; Zhang, Q.; Lu, C.; Xie, M.; McLellan, M.D.; Wendl, M.C.; Ding, L. MSIsensor: Microsatellite instability detection using paired tumor-normal sequence data. Bioinformatics 2014, 30, 1015–1016. [Google Scholar] [CrossRef] [PubMed]
- Latham, A.; Srinivasan, P.; Kemel, Y.; Shia, J.; Bandlamudi, C.; Mandelker, D.; Middha, S.; Hechtman, J.; Zehir, A.; Dubard-Gault, M.; et al. Microsatellite instability is associated with the presence of Lynch syndrome pan-cancer. J. Clin. Oncol. 2019, 37, 286–295. [Google Scholar] [CrossRef]
- Park, R.; Da Silva, L.L.; Saeed, A. Immunotherapy predictive molecular markers in advanced gastroesophageal cancer: MSI and beyond. Cancers 2021, 13, 1715. [Google Scholar] [CrossRef] [PubMed]
- Hou, W.; Yi, C.; Zhu, H. Predictive biomarkers of colon cancer immunotherapy: Present and future. Front. Immunol. 2022, 13, 1032314. [Google Scholar] [CrossRef] [PubMed]
- Friedman, C.F.; Hainsworth, J.D.; Kurzrock, R.; Spigel, D.R.; Burris, H.A.; Sweeney, C.J.; Meric-Bernstam, F.; Wang, Y.; Levy, J.; Grindheim, J.; et al. Atezolizumab treatment of tumors with high tumor mutational burden from MyPathway, a multicenter, open-label, Phase IIa multiple basket study. Cancer Discov. 2022, 12, 654–669. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the freely available easy-to-use software ‘EZR’ for medical statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Chmielecki, J.; Ross, J.S.; Wang, K.; Frampton, G.M.; Palmer, G.A.; Ali, S.M.; Palma, N.; Morosini, D.; Miller, V.A.; Yelensky, R.; et al. Oncogenic alterations in ERBB2/HER2 represent potential therapeutic targets across tumors from diverse anatomic sites of origin. Oncologist 2015, 20, 7–12. [Google Scholar] [CrossRef]
- Li, B.T.; Ross, D.S.; Aisner, D.L.; Chaft, J.E.; Hsu, M.; Kako, S.L.; Kris, M.G.; Varella-Garcia, M.; Arcila, M.E. HER2 amplification and HER2 mutation are distinct molecular targets in lung cancers. J. Thorac. Oncol. 2016, 11, 414–419. [Google Scholar] [CrossRef]
- Marcus, L.; Lemery, S.J.; Keegan, P.; Pazdur, R. FDA approval summary: Pembrolizumab for the treatment of microsatellite instability-high solid tumors. Clin. Cancer Res. 2019, 25, 3753–3758. [Google Scholar] [CrossRef] [PubMed]
- Chan, T.A.; Yarchoan, M.; Jaffee, E.; Swanton, C.; Quezada, S.A.; Stenzinger, A.; Peters, S. Development of tumor mutation burden as an immunotherapy biomarker: Utility for the oncology clinic. Ann. Oncol. 2019, 30, 44–56. [Google Scholar] [CrossRef]
- Cappuzzo, F.; Bemis, L.; Varella-Garcia, M. HER2 mutation and response to trastuzumab therapy in non-small-cell lung cancer. N. Engl. J. Med. 2006, 354, 2619–2621. [Google Scholar] [CrossRef]
- Weiler, D.; Diebold, J.; Strobel, K.; Aebi, S.; Gautschi, O. Rapid response to trastuzumab emtansine in a patient with HER2-driven lung cancer. J. Thorac. Oncol. 2015, 10, e16–e17. [Google Scholar] [CrossRef]
- Shih, J.; Bashir, B.; Gustafson, K.S.; Andrake, M.; Dunbrack, R.L.; Goldstein, L.J.; Boumber, Y. Cancer signature investigation: ERBB2 (HER2)-activating mutation and amplification-positive breast carcinoma mimicking lung primary. J. Natl. Compr. Cancer Netw. 2015, 13, 947–952. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cousin, S.; Khalifa, E.; Crombe, A.; Laizet, Y.; Lucchesi, C.; Toulmonde, M.; Le Moulec, S.; Auzanneau, C.; Soubeyran, I.; Italiano, A. Targeting ERBB2 mutations in solid tumors: Biological and clinical implications. J. Hematol. Oncol. 2018, 11, 86. [Google Scholar] [CrossRef] [PubMed]
- Loibl, S.; von Minckwitz, G.; Schneeweiss, A.; Paepke, S.; Lehmann, A.; Rezai, M.; Zahm, D.M.; Sinn, P.; Khandan, F.; Eidtmann, H.; et al. PIK3CA mutations are associated with lower rates of pathologic complete response to anti-human epidermal growth factor receptor 2 (her2) therapy in primary HER2-overexpressing breast cancer. J. Clin. Oncol. 2014, 32, 3212–3220. [Google Scholar] [CrossRef] [PubMed]
- Lopez, S.; Cocco, E.; Black, J.; Bellone, S.; Bonazzoli, E.; Predolini, F.; Ferrari, F.; Schwab, C.L.; English, D.P.; Ratner, E.; et al. Dual HER2/PIK3CA targeting overcomes single-agent acquired resistance in HER2-amplified uterine serous carcinoma cell lines in vitro and in vivo. Mol. Cancer Ther. 2015, 14, 2519–2526. [Google Scholar] [CrossRef]
- Smith, A.E.; Ferraro, E.; Safonov, A.; Morales, C.B.; Lahuerta, E.J.A.; Li, Q.; Kulick, A.; Ross, D.; Solit, D.B.; de Stanchina, E.; et al. HER2 + breast cancers evade anti-HER2 therapy via a switch in driver pathway. Nat. Commun. 2021, 12, 6667. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cancer Type | Characteristic | Category | ERBB2-Mutant | ERBB2-Wild-Type | p |
|---|---|---|---|---|---|
| EAC | MS status (%) | MSS | 17 (77.3) | 272 (95.1) | <0.05 |
| MSI-I | 0 (0) | 3 (1.0) | |||
| MSI-H | 5 (22.7) | 11 (3.8) | |||
| N/A | 0 | 7 | |||
| TMB (mut/Mb) | mean | 22.7 | 7.2 | <0.05 | |
| SD | 33.4 | 9.1 | |||
| Median | 6.9 | 5.4 | |||
| Minimum | 4.1 | 0 | |||
| Maximum | 113.3 | 92.5 | |||
| Low (<10) | 17 (77.3) | 265 (90.4) | 0.11 | ||
| High (≥10) | 5 (22.7) | 28 (9.6) | |||
| GC | MS status (%) | MSS | 14 (56) | 342 (82.8) | <0.05 |
| MSI-I | 2 (8) | 11 (2.7) | |||
| MSI-H | 9 (36) | 60 (14.5) | |||
| N/A | 13 | 136 | |||
| TMB (mut/Mb) | mean | 26.9 | 10.0 | <0.05 | |
| SD | 25.7 | 23.3 | |||
| Median | 22.5 | 3.5 | |||
| Minimum | 0.7 | 0 | |||
| Maximum | 89.6 | 330.8 | |||
| Low (<10) | 17 (44.7) | 453 (83.1) | <0.05 | ||
| High (≥10) | 21 (55.2) | 92 (16.9) | |||
| N/A | 0 | 4 | |||
| CRC | MS status (%) | MSS | 29 (74.4) | 894 (88.7) | <0.05 |
| MSI-I | 1 (2.6) | 19 (1.9) | |||
| MSI-H | 9 (23.1) | 95 (9.4) | |||
| TMB (mut/Mb) | mean | 40.0 | 10.5 | <0.05 | |
| SD | 80.2 | 23.1 | |||
| Median | 9.8 | 4.6 | |||
| Minimum | 2.0 | 0 | |||
| Maximum | 382.6 | 316.8 | |||
| Low (<16) | 26 (66.7) | 870 (90.0) | <0.05 | ||
| High (≥16) | 13 (33.3) | 96 (9.9) |
| Characteristic | Category | Group 1 (n = 8) | Group 2 (n = 9) | Group 3 (n = 5) | p |
|---|---|---|---|---|---|
| Age (years) | Mean | 65.8 | 69.0 | 67.0 | 0.81 |
| N/A | 2 | 6 | 3 | ||
| Sex (%) | Male | 6 (75.0) | 6 (66.7) | 4 (80.0) | 1 |
| Female | 2 (25.0) | 3 (33.3) | 1 (20.0) | ||
| Histological grade (%) | G1 | 1 (12.5) | 2 (22.5) | 0 (0) | 0.28 |
| G2 | 5 (62.5) | 5 (55.6) | 1 (20.0) | ||
| G3 | 2 (25.0) | 2 (22.2) | 4 (80.0) | ||
| Subtype (%) | CIN | 6 (100) | 1 (33.3) | 2 (100) | 0.07 |
| GS | 0 (0) | 0 (0) | 0 (0) | ||
| MSI | 0 (0) | 2 (66.7) | 0 (0) | ||
| POLE | 0 (0) | 0 (0) | 0 (0) | ||
| N/A | 2 | 6 | 3 | ||
| MS status (%) | MSS | 8 (100) | 4 (44.4) | 5 (100) | <0.05 |
| MSI-I | 0 (0) | 0 (0) | 0 (0) | ||
| MSI-H | 0 (0) | 5 (55.6) | 0 (0) | ||
| TMB (mut/Mb) | Mean | 5.2 | 43.5 | 6.0 | 0.05 |
| SD | 1.0 | 42.9 | 3.2 | ||
| Median | 5.0 | 41.5 | 6.1 | ||
| Minimum | 4.1 | 3.5 | 2.4 | ||
| Maximum | 6.9 | 113.2 | 9.5 | ||
| Low (<10) | 8 (100) | 4 (44.4) | 5 (100) | <0.05 | |
| High (<10) | 0 (0) | 5 (55.6) | 0 (0) |
| Characteristic | Category | Group 1 (n = 4) | Group 2 (n = 25) | Group 3 (n = 9) | p |
|---|---|---|---|---|---|
| Age (years) | Mean | 72.3 | 68.1 | 64.3 | 0.32 |
| N/A | 0 | 2 | 2 | ||
| Sex (%) | Male | 2 (50) | 10 (43.5) | 6 (66.7) | 0.78 |
| Female | 2 (50) | 13 (56.5) | 3 (37.5) | ||
| N/A | 0 | 2 | 1 | ||
| Histological grade (%) | G1 | 0 (0) | 0 (0) | 0 (0) | <0.05 |
| G2 | 3 (100) | 4 (26.7) | 5 (71.4) | ||
| G3 | 0 (0) | 11 (73.3) | 2 (28.6) | ||
| Subtype (%) | CIN | 2 (100) | 5 (22.7) | 3 (33.3) | 0.32 |
| EBV | 0 (0) | 1 (4.5) | 0 (0) | ||
| GS | 0 (0) | 1 (4.5) | 1 (11.1) | ||
| MSI | 0 (0) | 15 (68.2) | 5 (56.6) | ||
| N/A | 2 | 3 | 0 | ||
| MS status | MSS | 3 (100) | 7 (46.7) | 4 (57.1) | 0.47 |
| MSI-I | 0 (0) | 1 (6.7) | 1 (14.3) | ||
| MSI-H | 0 (0) | 7 (46.7) | 2 (28.6) | ||
| N/A | 1 | 10 | 2 | ||
| TMB (mut/Mb) | Mean | 4.0 | 26.9 | 36.9 | <0.05 |
| SD | 2.3 | 23.5 | 31.9 | ||
| Median | 4.8 | 28.0 | 38.3 | ||
| Minimum | 0.7 | 2.0 | 5.9 | ||
| Maximum | 5.9 | 88.4 | 89.6 | ||
| Low (<10) | 4 (100) | 10 (40.0) | 3 (33.3) | 0.07 | |
| High (≥10) | 0 (0) | 15 (60.0) | 6 (66.7) |
| Characteristic | Category | Group 1 (n = 6) | Group 2 (n = 16) | Group 3 (n = 17) | p |
|---|---|---|---|---|---|
| Age (years) | Mean | 58.3 | 65.5 | 62.7 | 0.67 |
| Sex (%) | Male | 5 (83.3) | 9 (56.3) | 10 (58.8) | 0.56 |
| Female | 1 (16.7) | 7 (43.8) | 7 (41.2) | ||
| Histological grade | G1 | 0 (0) | 2 (12.5) | 1 (5.9) | 0.73 |
| G2 | 4 (66.7) | 9 (56.3) | 13 (76.5) | ||
| G3 | 2 (33.3) | 5 (31.3) | 3 (17.6) | ||
| Subtype (%) | CIN | 3 (100) | 4 (80.0) | 2 (18.2) | <0.05 |
| GS | 0 (0) | 1 (20.0) | 1 (9.1) | ||
| MSI | 0 (0) | 0 (0) | 6 (54.5) | ||
| POLE | 0 (0) | 0 (0) | 2 (18.2) | ||
| N/A | 3 | 11 | 6 | ||
| MS status | MSS | 6 (100) | 14 (87.5) | 9 (52.9) | <0.05 |
| MSI-I | 0 (0) | 1 (6.3) | 0 (0) | ||
| MSI-H | 0 (0) | 1 (6.3) | 8 (47.1) | ||
| TMB (mut/Mb) | Mean | 5.9 | 11.9 | 78.5 | <0.05 |
| SD | 3.2 | 21.0 | 109.8 | ||
| Median | 4.7 | 7.3 | 37.0 | ||
| Minimum | 2.9 | 2.0 | 2.0 | ||
| Maximum | 9.8 | 89.9 | 382.6 | ||
| Low (<16) | 6 (100) | 16 (100) | 4 (23.5) | <0.05 | |
| High (≥16) | 0 (0) | 0 (0) | 13 (76.5) | <0.05 |
| Cancer Type | Group (Number) | PI3K/MTOR (%) | MAPK (%) |
|---|---|---|---|
| EAC | |||
| Group 1 (n = 8) | 2 (25.0) | 0 (0) | |
| Group 2 (n = 9) | 5 (55.6) | 1 (11.1) | |
| Group 3 (n = 5) | 0 (0) | 1 (20.0) | |
| GC | |||
| Group 1 (n = 4) | 0 (0) | 0 (0) | |
| Group 2 (n = 25) | 10 (40.0) | 9 (36.0) | |
| Group 3 (n = 9) | 4 (44.4) | 2 (22.2) | |
| CRC | |||
| Group 1 (n = 6) | 1 (16.7) | 2 (33.3) | |
| Group 2 (n = 16) | 4 (25.0) | 10 (62.5) | |
| Group 3 (n = 17) | 13 (76.5) | 12 (70.6) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Uchida, S.; Sugino, T. ERBB2-Mutant Gastrointestinal Tumors Represent Heterogeneous Molecular Biology, Particularly in Microsatellite Instability, Tumor Mutation Burden, and Co-Mutated Genes: An In Silico Study. Curr. Issues Mol. Biol. 2023, 45, 7404-7416. https://doi.org/10.3390/cimb45090468
Uchida S, Sugino T. ERBB2-Mutant Gastrointestinal Tumors Represent Heterogeneous Molecular Biology, Particularly in Microsatellite Instability, Tumor Mutation Burden, and Co-Mutated Genes: An In Silico Study. Current Issues in Molecular Biology. 2023; 45(9):7404-7416. https://doi.org/10.3390/cimb45090468
Chicago/Turabian StyleUchida, Shiro, and Takashi Sugino. 2023. "ERBB2-Mutant Gastrointestinal Tumors Represent Heterogeneous Molecular Biology, Particularly in Microsatellite Instability, Tumor Mutation Burden, and Co-Mutated Genes: An In Silico Study" Current Issues in Molecular Biology 45, no. 9: 7404-7416. https://doi.org/10.3390/cimb45090468
APA StyleUchida, S., & Sugino, T. (2023). ERBB2-Mutant Gastrointestinal Tumors Represent Heterogeneous Molecular Biology, Particularly in Microsatellite Instability, Tumor Mutation Burden, and Co-Mutated Genes: An In Silico Study. Current Issues in Molecular Biology, 45(9), 7404-7416. https://doi.org/10.3390/cimb45090468