Comparison of Next-Generation Sequencing and Polymerase Chain Reaction for Personalized Treatment-Related Genomic Status in Patients with Metastatic Colorectal Cancer

 , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
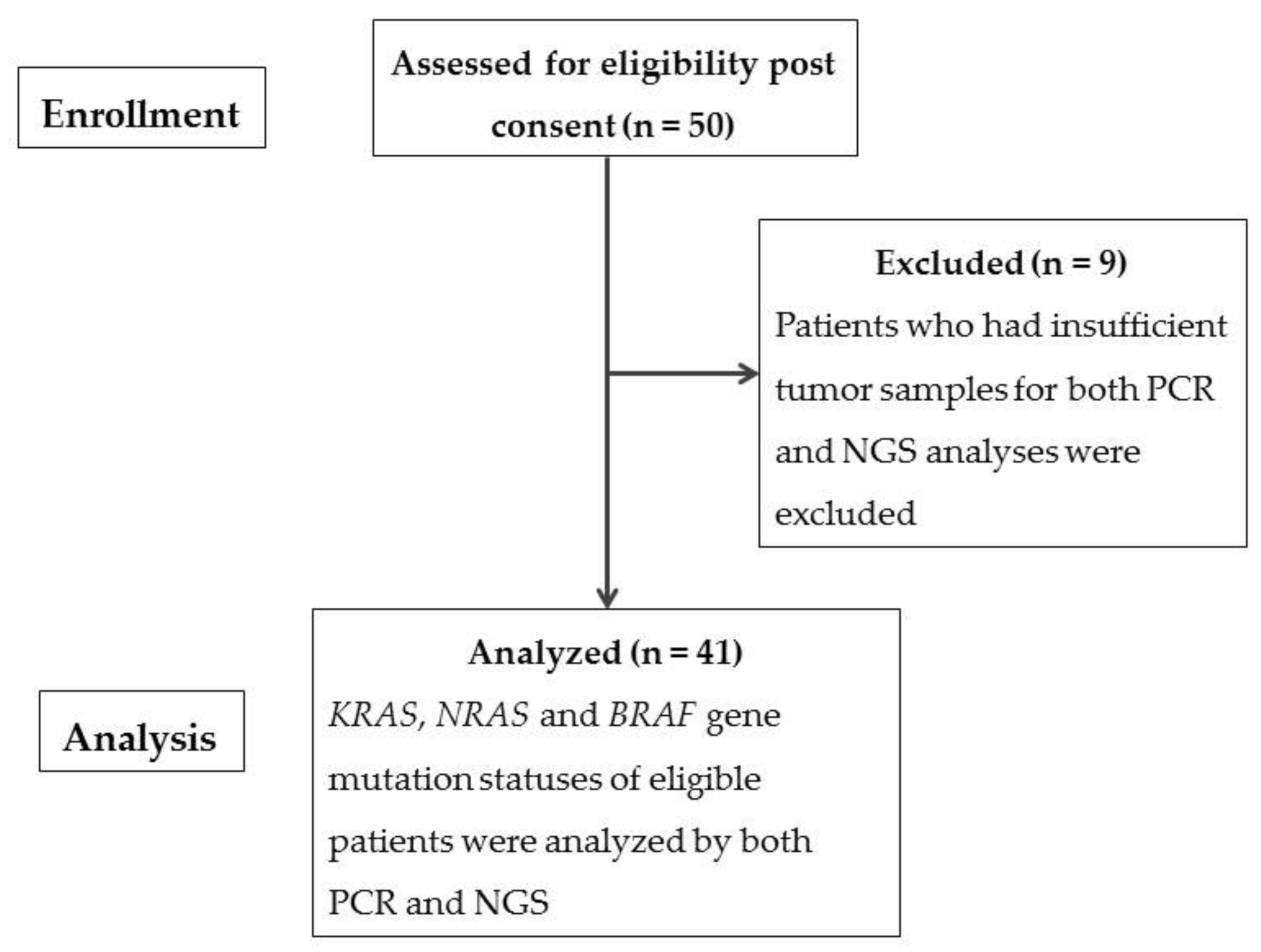
2.1. Patients
2.2. Ethics Approval
2.3. Analyses of KRAS, NRAS, BRAF
2.4. Sample Preparation for Genotyping of KRAS, NRAS, and BRAF Hotspot Mutations through In-House NGS
2.5. Detection of KRAS, NRAS, and BRAF Hotspot Mutations through In-House NGS
2.6. Statistical Analysis
3. Results
3.1. Patient Demographics
Comparison of PCR and NGS for Testing of Targeted Genes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cancer. Available online: http://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 21 May 2018).
- 2019 Causes of Death Statistics. Available online: https://www.mohw.gov.tw/lp-4964-2.html (accessed on 21 May 2021).
- Patil, H.; Saxena, S.G.; Barrow, C.J.; Kanwar, J.R.; Kapat, A.; Kanwar, R.K. Chasing the personalized medicine dream through biomarker validation in colorectal cancer. Drug Discov. Today 2017, 22, 111–119. [Google Scholar] [CrossRef]
- Tsang, A.H.-F.; Cheng, K.H.; Wong, A.S.; Ng, S.S.; Ma, B.B.; Chan, C.M.; Tsui, N.B.; Chan, L.W.; Yung, B.Y.; Wong, S.C. Current and future molecular diagnostics in colorectal cancer and colorectal adenoma. World J. Gastroenterol. 2014, 20, 3847–3857. [Google Scholar] [CrossRef] [PubMed]
- Nong, L.; Zhang, Z.; Xiong, Y.; Zheng, Y.; Li, X.; Li, D.; He, Q.; Li, T. Comparison of next-generation sequencing and immunohistochemistry analysis for targeted therapy-related genomic status in lung cancer patients. J. Thorac. Dis. 2019, 11, 4992–5003. [Google Scholar] [CrossRef] [PubMed]
- Taieb, J.; Jung, A.; Sartore-Bianchi, A.; Peeters, M.; Seligmann, J.; Zaanan, A.; Burdon, P.; Montagut, C.; Laurent-Puig, P. The Evolving Biomarker Landscape for Treatment Selection in Metastatic Colorectal Cancer. Drugs 2019, 79, 1375–1394. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Cutsem, E.; Cervantes, A.; Adam, R.; Sobrero, A.; van Krieken, J.H.; Aderka, D.; Aguilar, E.A.; Bardelli, A.; Benson, A.; Bodoky, G.; et al. ESMO consensus guidelines for the management of patients with metastatic colorectal cancer. Ann. Oncol. 2016, 27, 1386–1422. [Google Scholar] [CrossRef]
- Shen, Y.; Wang, J.; Han, X.; Yang, H.; Wang, S.; Lin, N.; Shi, Y. Effectors of Epidermal Growth Factor Receptor Pathway: The Genetic Profiling of KRAS, BRAF, PIK3CA, NRAS Mutations in Colorectal Cancer Characteristics and Personalized Medicine. PLoS ONE 2013, 8, e81628. [Google Scholar] [CrossRef]
- Peeters, M.; Price, T.; Cervantes, A.; Sobrero, A.F.; Ducreux, M.; Hotko, Y.; André, T.; Chan, E.; Lordick, F.; Punt, C.J.; et al. Randomized Phase III Study of Panitumumab With Fluorouracil, Leucovorin, and Irinotecan (FOLFIRI) Compared With FOLFIRI Alone As Second-Line Treatment in Patients With Metastatic Colorectal Cancer. J. Clin. Oncol. 2010, 28, 4706–4713. [Google Scholar] [CrossRef]
- Douillard, J.-Y.; Oliner, K.S.; Siena, S.; Tabernero, J.; Burkes, R.; Barugel, M.; Humblet, Y.; Bodoky, G.; Cunningham, D.; Jassem, J.; et al. Panitumumab–FOLFOX4 Treatment and RAS Mutations in Colorectal Cancer. N. Engl. J. Med. 2013, 369, 1023–1034. [Google Scholar] [CrossRef] [Green Version]
- Amado, R.G.; Wolf, M.; Peeters, M.; Van Cutsem, E.; Siena, S.; Freeman, D.J.; Juan, T.; Sikorski, R.; Suggs, S.; Radinsky, R.; et al. Wild-TypeKRASIs Required for Panitumumab Efficacy in Patients With Metastatic Colorectal Cancer. J. Clin. Oncol. 2008, 26, 1626–1634. [Google Scholar] [CrossRef]
- Karapetis, C.S.; Khambata-Ford, S.; Jonker, D.J.; O’Callaghan, C.J.; Tu, D.; Tebbutt, N.C.; Simes, R.J.; Chalchal, H.; Shapiro, J.D.; Robitaille, S.; et al. K-rasMutations and Benefit from Cetuximab in Advanced Colorectal Cancer. N. Engl. J. Med. 2008, 359, 1757–1765. [Google Scholar] [CrossRef] [Green Version]
- Sorich, M.J.; Wiese, M.; Rowland, A.; Kichenadasse, G.; McKinnon, R.; Karapetis, C. Extended RAS mutations and anti-EGFR monoclonal antibody survival benefit in metastatic colorectal cancer: A meta-analysis of randomized, controlled trials. Ann. Oncol. 2014, 26, 13–21. [Google Scholar] [CrossRef] [PubMed]
- Bokemeyer, C.; Bondarenko, I.; Makhson, A.; Hartmann, J.T.; Aparicio, J.; de Braud, F.; Donea, S.; Ludwig, H.; Schuch, G.; Stroh, C.; et al. Fluorouracil, Leucovorin, and Oxaliplatin With and Without Cetuximab in the First-Line Treatment of Metastatic Colorectal Cancer. J. Clin. Oncol. 2009, 27, 663–671. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laurent-Puig, P.; Cayre, A.; Manceau, G.; Buc, E.; Bachet, J.-B.; LeComte, T.; Rougier, P.; Lievre, A.; Landi, B.; Boige, V.; et al. Analysis of PTEN, BRAF, and EGFR Status in Determining Benefit From Cetuximab Therapy in Wild-Type KRAS Metastatic Colon Cancer. J. Clin. Oncol. 2009, 27, 5924–5930. [Google Scholar] [CrossRef]
- De Roock, W.; Claes, B.; Bernasconi, D.; De Schutter, J.; Biesmans, B.; Fountzilas, G.; Kalogeras, K.T.; Kotoula, V.; Papamichael, D.; Laurent-Puig, P.; et al. Effects of KRAS, BRAF, NRAS, and PIK3CA mutations on the efficacy of cetuximab plus chemotherapy in chemotherapy-refractory metastatic colorectal cancer: A retrospective consortium analysis. Lancet Oncol. 2010, 11, 753–762. [Google Scholar] [CrossRef]
- Di Nicolantonio, F.; Martini, M.; Molinari, F.; Sartore-Bianchi, A.; Arena, S.; Saletti, P.; De Dosso, S.; Mazzucchelli, L.; Frattini, M.; Siena, S.; et al. Wild-Type BRAF Is Required for Response to Panitumumab or Cetuximab in Metastatic Colorectal Cancer. J. Clin. Oncol. 2008, 26, 5705–5712. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.-C.; Chang, T.-K.; Su, W.-C.; Huang, C.-W.; Tsai, H.-L.; Chen, Y.-C.; Li, C.-C.; Chen, P.-J.; Yin, T.-C.; Ma, C.-J.; et al. UGT1A1 Polymorphism for Irinotecan Dose Escalation in Patients with BRAF-Mutated Metastatic Colorectal Cancer Treated with First-Line Bevacizumab and FOLFIRI. J. Oncol. 2021, 2021, 6686517. [Google Scholar] [CrossRef]
- Revythis, A.; Shah, S.; Kutka, M.; Moschetta, M.; Ozturk, M.; Pappas-Gogos, G.; Ioannidou, E.; Sheriff, M.; Rassy, E.; Boussios, S. Unraveling the Wide Spectrum of Melanoma Biomarkers. Diagnostics 2021, 11, 1341. [Google Scholar] [CrossRef]
- Ghose, A.; Moschetta, M.; Pappas-Gogos, G.; Sheriff, M.; Boussios, S. Genetic Aberrations of DNA Repair Pathways in Prostate Cancer: Translation to the Clinic. Int. J. Mol. Sci. 2021, 22, 9783. [Google Scholar] [CrossRef]
- Amin, M.B.; Edge, S.; Greene, F.; Byrd, D.R.; Brookland, R.K.; Washington, M.K.; Gershenwald, J.E.; Compton, C.C.; Hess, K.R.; Sullivan, D.C. (Eds.) AJCC Cancer Staging Manual, 8th ed.; American College of Surgeons, Springer International Publishing: New York, NY, USA, 2017. [Google Scholar]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- Tirkes, T.; Hollar, M.A.; Tann, M.; Kohli, M.D.; Akisik, F.; Sandrasegaran, K. Response Criteria in Oncologic Imaging: Review of Traditional and New Criteria. RadioGraphics 2013, 33, 1323–1341. [Google Scholar] [CrossRef]
- Li, H.; Durbin, R. Fast and accurate short read alignment with Burrows–Wheeler transform. Bioinformatics 2009, 25, 1754–1760. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, H.; Handsaker, B.; Wysoker, A.; Fennell, T.; Ruan, J.; Homer, N.; Marth, G.; Abecasis, G.; Durbin, R. 1000 Genome Project Data Processing Subgroup. The Sequence Alignment/Map format and SAMtools. Bioinformatics 2009, 25, 2078–2079. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koboldt, D.C.; Larson, D.E.; Wilson, R.K. Using VarScan 2 for Germline Variant Calling and Somatic Mutation Detection. Curr. Protoc. Bioinform. 2013, 44, 15.4.1–15.4.17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balchen, V.; Simon, K. Colorectal cancer development and advances in screening. Clin. Interv. Aging 2016, 11, 967–976. [Google Scholar] [CrossRef] [Green Version]
- Engelman, J.A. Targeting PI3K signalling in cancer: Opportunities, challenges and limitations. Nat. Cancer 2009, 9, 550–562. [Google Scholar] [CrossRef]
- Samuels, Y.; Diaz, L.; Schmidt-Kittler, O.; Cummins, J.M.; DeLong, L.; Cheong, I.; Rago, C.; Huso, D.L.; Lengauer, C.; Kinzler, K.W.; et al. Mutant PIK3CA promotes cell growth and invasion of human cancer cells. Cancer Cell 2005, 7, 561–573. [Google Scholar] [CrossRef] [Green Version]
- McCubrey, J.A.; Steelman, L.S.; Abrams, S.L.; Lee, J.T.; Chang, F.; Bertrand, F.E.; Navolanic, P.M.; Terrian, D.M.; Franklin, R.A.; D’Assoro, A.B.; et al. Roles of the RAF/MEK/ERK and PI3K/PTEN/AKT pathways in malignant transformation and drug resistance. Adv. Enzym. Regul. 2006, 46, 249–279. [Google Scholar] [CrossRef]
- Calistri, D.; Rengucci, C.; Seymour, I.; Lattuneddu, A.; Polifemo, A.M.; Monti, F.; Saragoni, L.; Amadori, D. Mutation analysis ofp53,K-ras, andBRAF genes in colorectal cancer progression. J. Cell. Physiol. 2005, 204, 484–488. [Google Scholar] [CrossRef]
- Zhang, J.; Zheng, J.; Yang, Y.; Lu, J.; Gao, J.; Lu, T.; Sun, J.; Jiang, H.; Zhu, Y.; Zheng, Y.; et al. Molecular spectrum of KRAS, NRAS, BRAF and PIK3CA mutations in Chinese colorectal cancer patients: Analysis of 1110 cases. Sci. Rep. 2015, 5, 18678. [Google Scholar] [CrossRef]
- Wilson, P.M.; LaBonte, M.J.; Lenz, H.-J. Molecular Markers in the Treatment of Metastatic Colorectal Cancer. Cancer J. 2010, 16, 262–272. [Google Scholar] [CrossRef]
- Chuang, S.-C.; Huang, C.-W.; Chen, Y.-T.; Ma, C.-J.; Tsai, H.-L.; Chang, T.-K.; Su, W.-C.; Hsu, W.-H.; Kuo, C.-H.; Wang, J.-Y. Effect of KRAS and NRAS mutations on the prognosis of patients with synchronous metastatic colorectal cancer presenting with liver-only and lung-only metastases. Oncol. Lett. 2020, 20, 2119–2130. [Google Scholar] [CrossRef]
- Tan, C.; Du, X. KRAS mutation testing in metastatic colorectal cancer. World J. Gastroenterol. 2012, 18, 5171–5180. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.-H.; Ke, T.-W.; Huang, C.-W.; Jiang, J.-K.; Chen, C.-C.; Hsieh, Y.-Y.; Teng, H.-W.; Lin, B.-W.; Liang, Y.-H.; Su, Y.-L.; et al. Taiwan Society of Colon and Rectal Surgeons Consensus on mCRC Treatment. Front. Oncol. 2021, 11, 764912. [Google Scholar] [CrossRef]
- Ma, C.-J.; Huang, C.-W.; Chang, T.-K.; Tsai, H.-L.; Su, W.-C.; Yeh, Y.-S.; Chen, P.-J.; Wang, J.-Y. Oncologic Outcomes in Metastatic Colorectal Cancer with Regorafenib with FOLFIRI as a Third- or Fourth-Line Setting. Transl. Oncol. 2018, 12, 502–512. [Google Scholar] [CrossRef] [PubMed]
- Yen, L.-C.; Yeh, Y.-S.; Chen, C.-W.; Wang, H.-M.; Tsai, H.-L.; Lu, C.-Y.; Chang, Y.-T.; Chu, K.-S.; Lin, S.-R.; Wang, J.-Y. Detection of KRAS Oncogene in Peripheral Blood as a Predictor of the Response to Cetuximab Plus Chemotherapy in Patients with Metastatic Colorectal Cancer. Clin. Cancer Res. 2009, 15, 4508–4513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Roock, W.; Piessevaux, H.; De Schutter, J.; Janssens, M.; De Hertogh, G.; Personeni, N.; Biesmans, B.; Van Laethem, J.-L.; Peeters, M.; Humblet, Y.; et al. KRAS wild-type state predicts survival and is associated to early radiological response in metastatic colorectal cancer treated with cetuximab. Ann. Oncol. 2008, 19, 508–515. [Google Scholar] [CrossRef] [PubMed]
- Yeh, J.-H.; Tsai, H.-L.; Chen, Y.-C.; Li, C.-C.; Huang, C.-W.; Chang, T.-K.; Su, W.-C.; Chen, P.-J.; Liu, Y.-P.; Wang, J.-Y. BRAF, MEK, and EGFR Triplet Inhibitors as Salvage Therapy in BRAF-Mutated Metastatic Colorectal Cancer—A Case Series Study Target Therapy of BRAF-Mutated mCRC. Medicina 2021, 57, 1339. [Google Scholar] [CrossRef] [PubMed]
- Boussios, S.; Ozturk, M.A.; Moschetta, M.; Karathanasi, A.; Zakynthinakis-Kyriakou, N.; Katsanos, K.H.; Christodoulou, D.K.; Pavlidis, N. The Developing Story of Predictive Biomarkers in Colorectal Cancer. J. Pers. Med. 2019, 9, 12. [Google Scholar] [CrossRef] [Green Version]
- Missiaglia, E.; Jacobs, B.; D’Ario, G.; Di Narzo, A.; Soneson, C.; Budinska, E.; Popovici, V.; Vecchione, L.; Gerster, S.; Yan, P.; et al. Distal and proximal colon cancers differ in terms of molecular, pathological, and clinical features. Ann. Oncol. 2014, 25, 1995–2001. [Google Scholar] [CrossRef]
- Zarkavelis, G.; Boussios, S.; Papadaki, A.; Katsanos, K.H.; Christodoulou, D.K.; Pentheroudakis, G. Current and future biomarkers in colorectal cancer. Ann. Gastroenterol. 2017, 30, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Takane, K.; Akagi, K.; Fukuyo, M.; Yagi, K.; Takayama, T.; Kaneda, A. DNA methylation epigenotype and clinical features ofNRAS-mutation(+) colorectal cancer. Cancer Med. 2017, 6, 1023–1035. [Google Scholar] [CrossRef] [PubMed]
- Downward, J. Targeting RAS signalling pathways in cancer therapy. Nat. Cancer 2003, 3, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Peeters, M.; Kafatos, G.; Taylor, A.; Gastanaga, V.; Oliner, K.; Hechmati, G.; Terwey, J.-H.; van Krieken, J. Prevalence of RAS mutations and individual variation patterns among patients with metastatic colorectal cancer: A pooled analysis of randomised controlled trials. Eur. J. Cancer 2015, 51, 1704–1713. [Google Scholar] [CrossRef] [PubMed]
- Lai, E.; Pretta, A.; Impera, V.; Mariani, S.; Giampieri, R.; Casula, L.; Pusceddu, V.; Coni, P.; Fanni, D.; Puzzoni, M.; et al. BRAF-mutant colorectal cancer, a different breed evolving. Expert Rev. Mol. Diagn. 2018, 18, 499–512. [Google Scholar] [CrossRef]
- Afrăsânie, V.-A.; Marinca, M.V.; Alexa-Stratulat, T.; Gafton, B.; Păduraru, M.; Adavidoaiei, A.M.; Miron, L.; Rusu, C. KRAS, NRAS, BRAF, HER2 and microsatellite instability in metastatic colorectal cancer—Practical implications for the clinician. Radiol. Oncol. 2019, 53, 265–274. [Google Scholar] [CrossRef] [Green Version]
- Sanz-Garcia, E.; Argiles, G.; Elez, E.; Tabernero, J. BRAF mutant colorectal cancer: Prognosis, treatment, and new perspectives. Ann. Oncol. 2017, 28, 2648–2657. [Google Scholar] [CrossRef]
- Tsai, H.-L.; Chen, Y.-C.; Yin, T.-C.; Su, W.-C.; Chen, P.-J.; Chang, T.-K.; Li, C.-C.; Huang, C.-W.; Wang, J.-Y. Comparison of UGT1A1 polymorphism as guidance of irinotecan dose escalation in RAS wild type metastatic colorectal cancer patients treated with cetuximab or bevacizumab plus FOLFIRI as the first-line therapy. Oncol. Res. Featur. Preclin. Clin. Cancer Ther. 2022. [Google Scholar] [CrossRef]
- Bobo, D.; Lipatov, M.; Rodriguez-Flores, J.L.; Auton, A.; Henn, B.M. False Negatives Are a Significant Feature of Next Generation Sequencing Callsets. BiorXiv 2016. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Subjects with Metastatic CRC (n = 41) | |
|---|---|
| Median age (years, range) | 65 (34–88) |
| Male | 64 (34–86) |
| Female | 65 (38–88) |
| Gender | |
| Male | 26 (63.4%) |
| Female | 15 (36.6%) |
| Tumor location | |
| R’t colon/L’t colon | 6 (14.6%)/35 (85.3%) |
| Depth of tumor invasion | |
| T1/T2/T3/T4 | 0/2 (4.9%)/27 (65.8%)/12 (29.3%) |
| Lymph node involvement | |
| N0/N1/N2 | 11 (26.8%)/17 (41.5%)/13 (31.7%) |
| Vascular invasion | |
| Yes/No | 10 (24.4%)/31 (75.6%) |
| Perineural invasion | |
| Yes/No | 12 (29.3%)/29 (70.7%) |
| Somatic Mutation | |||||||
|---|---|---|---|---|---|---|---|
| Case No. | Tumor Content (%) | KRAS Condon 12/13/59/61/146 Tested by PCR | KRAS Condon 12/13/61/146 Tested by NGS | NRAS Condon 12/13 Tested by PCR | NRAS Condon 12/13 Tested by NGS | BRAF Codon 600 Tested by PCR | BRAF Codon 600 Tested by NGS |
| 1 | 30 | wild-type | wild-type | wild-type | wild-type | wild-type | wild-type |
| 2 | <5 | codon 61 mutation | wild-type | wild-type | wild-type | wild-type | wild-type |
| 3 | 90 | codon 12 mutation | codon 12 mutation | no data * | wild-type | wild-type | wild-type |
| 4 | 15 | wild-type | wild-type | wild-type | wild-type | wild-type | wild-type |
| 5 | 70 | wild-type | wild-type | wild-type | wild-type | wild-type | wild-type |
| 6 | 50 | wild-type | wild-type | wild-type | wild-type | wild-type | wild-type |
| 7 | 10 | wild-type | codon 61 mutation | wild-type | wild-type | wild-type | wild-type |
| 8 | 20 | codon 12 mutation | codon 12 mutation | no data * | codon 12 mutation | wild-type | wild-type |
| 9 | 30 | wild-type | wild-type | wild-type | wild-type | wild-type | wild-type |
| 10 | <5 | wild-type | wild-type | wild-type | wild-type | wild-type | wild-type |
| 11 | <5 | wild-type | wild-type | wild-type | wild-type | wild-type | wild-type |
| 12 | 20 | wild-type | wild-type | wild-type | wild-type | codon 597 mutation | codon 600 mutation |
| 13 | 70 | codon 59 mutation | codon 13 mutation | wild-type | wild-type | wild-type | codon 600 mutation |
| 14 | 40 | codon 146 mutation | codon 146 mutation | wild-type | wild-type | wild-type | wild-type |
| 15 | <5 | wild-type | wild-type | wild-type | wild-type | wild-type | wild-type |
| 16 | 10 | wild-type | wild-type | wild-type | codon 12 mutation | wild-type | codon 600 mutation |
| 17 | 60 | wild-type | wild-type | wild-type | codon 12 mutation | wild-type | codon 600 mutation |
| 18 | 20 | codon 61 mutation | codon 61 mutation | wild-type | wild-type | wild-type | wild-type |
| 19 | 60 | wild-type | wild-type | wild-type | codon 12 mutation | codon 600 mutation | codon 600 mutation |
| 20 | 30 | wild-type | wild-type | codon 12 mutation | codon 12 mutation | wild-type | codon 600 mutation |
| 21 | 15 | wild-type | wild-type | wild-type | wild-type | codon 600 mutation | codon 600 mutation |
| 22 | 10 | wild-type | wild-type | wild-type | wild-type | wild-type | codon 600 mutation |
| 23 | 10 | codon 12 mutation | codon 12 mutation | wild-type | wild-type | wild-type | wild-type |
| 24 | 40 | wild-type | wild-type | wild-type | wild-type | wild-type | wild-type |
| 25 | 10 | wild-type | wild-type | wild-type | wild-type | wild-type | wild-type |
| 26 | 30 | codon 12 mutation | codon 12 mutation | wild-type | wild-type | wild-type | wild-type |
| 27 | 20 | wild-type | wild-type | wild-type | wild-type | wild-type | wild-type |
| 28 | 40 | wild-type | wild-type | wild-type | wild-type | wild-type | wild-type |
| 29 | 80 | wild-type | wild-type | wild-type | wild-type | wild-type | wild-type |
| 30 | 10 | codon 13 mutation | wild-type | wild-type | wild-type | wild-type | wild-type |
| 31 | <5 | codon 12 mutation | wild-type | wild-type | wild-type | wild-type | wild-type |
| 32 | 95 | codon 13 mutation | codon 13 mutation | wild-type | wild-type | wild-type | wild-type |
| 33 | <5 | wild-type | wild-type | wild-type | wild-type | wild-type | wild-type |
| 34 | <5 | wild-type | wild-type | wild-type | wild-type | wild-type | wild-type |
| 35 | 20 | codon 61 mutation | wild-type | wild-type | wild-type | wild-type | wild-type |
| 36 | 50 | wild-type | wild-type | wild-type | wild-type | wild-type | wild-type |
| 37 | 80 | codon 146 mutation | codon 146 mutation | wild-type | wild-type | wild-type | wild-type |
| 38 | 30 | wild-type | wild-type | wild-type | wild-type | wild-type | wild-type |
| 39 | 30 | wild-type | wild-type | wild-type | wild-type | wild-type | wild-type |
| 40 | 95 | codon 12 mutation | codon 12 mutation | wild-type | wild-type | wild-type | wild-type |
| 41 | 40 | wild-type | wild-type | wild-type | wild-type | wild-type | wild-type |
| Gene | No. of Cases Compared | Wild-Type Detected by PCR | Wild-Type Detected by NGS | Mutation Detected by PCR | Mutation Detected by NGS | Percentage of Concordance (%) |
|---|---|---|---|---|---|---|
| KRAS | 41 | 27 | 30 | 14 | 11 | 92.7 |
| NRAS * | 39 | 38 | 35 | 1 | 4 | 92.3 |
| BRAF | 41 | 38 | 33 | 3 | 8 | 87.8 |
| No. of Patients with mCRC | ||||
|---|---|---|---|---|
| Gene | Source | Mutation | Real-Time PCR | NGS |
| KRAS | Tissue DNA | Codon 12 | 6 (14.6%) | 5 (12.2%) |
| Codon 13 | 2 (4.9%) | 2 (4.9%) | ||
| Codon 59 | 1 (2.4%) | 0 | ||
| Codon 61 | 3 (7.3%) | 2 (4.9%) | ||
| Codon 146 | 2 (4.9%) | 2 (4.9%) | ||
| Total | 14 (34.1%) | 11 (26.8%) | ||
| NRAS | Tissue DNA | Codon 12 | 1 (2.4%) | 5 (12.2%) |
| Total | 1 (2.4%) | 5 (12.2%) | ||
| BRAF | Tissue DNA | Codon 600 Codon 597 | 2 (4.9%) 1 (2.4%) | 8 (19.5%) 0 |
| Total | 3 (7.3%) | 8 (19.5%) | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Su, W.-C.; Tsai, Y.-C.; Tsai, H.-L.; Chang, T.-K.; Yin, T.-C.; Huang, C.-W.; Chen, Y.-C.; Li, C.-C.; Chen, P.-J.; Liu, Y.-R.; et al. Comparison of Next-Generation Sequencing and Polymerase Chain Reaction for Personalized Treatment-Related Genomic Status in Patients with Metastatic Colorectal Cancer. Curr. Issues Mol. Biol. 2022, 44, 1552-1563. https://doi.org/10.3390/cimb44040106
Su W-C, Tsai Y-C, Tsai H-L, Chang T-K, Yin T-C, Huang C-W, Chen Y-C, Li C-C, Chen P-J, Liu Y-R, et al. Comparison of Next-Generation Sequencing and Polymerase Chain Reaction for Personalized Treatment-Related Genomic Status in Patients with Metastatic Colorectal Cancer. Current Issues in Molecular Biology. 2022; 44(4):1552-1563. https://doi.org/10.3390/cimb44040106
Chicago/Turabian StyleSu, Wei-Chih, Yi-Chen Tsai, Hsiang-Lin Tsai, Tsung-Kun Chang, Tzu-Chieh Yin, Ching-Wen Huang, Yen-Cheng Chen, Ching-Chun Li, Po-Jung Chen, Yun-Ru Liu, and et al. 2022. "Comparison of Next-Generation Sequencing and Polymerase Chain Reaction for Personalized Treatment-Related Genomic Status in Patients with Metastatic Colorectal Cancer" Current Issues in Molecular Biology 44, no. 4: 1552-1563. https://doi.org/10.3390/cimb44040106
APA StyleSu, W.-C., Tsai, Y.-C., Tsai, H.-L., Chang, T.-K., Yin, T.-C., Huang, C.-W., Chen, Y.-C., Li, C.-C., Chen, P.-J., Liu, Y.-R., Hsieh, T.-H., & Wang, J.-Y. (2022). Comparison of Next-Generation Sequencing and Polymerase Chain Reaction for Personalized Treatment-Related Genomic Status in Patients with Metastatic Colorectal Cancer. Current Issues in Molecular Biology, 44(4), 1552-1563. https://doi.org/10.3390/cimb44040106