
Development of a Medication-Related Osteonecrosis of the Jaw Prediction Model Using the FDA Adverse Event Reporting System Database and Machine Learning



Abstract
1. Introduction
2. Results
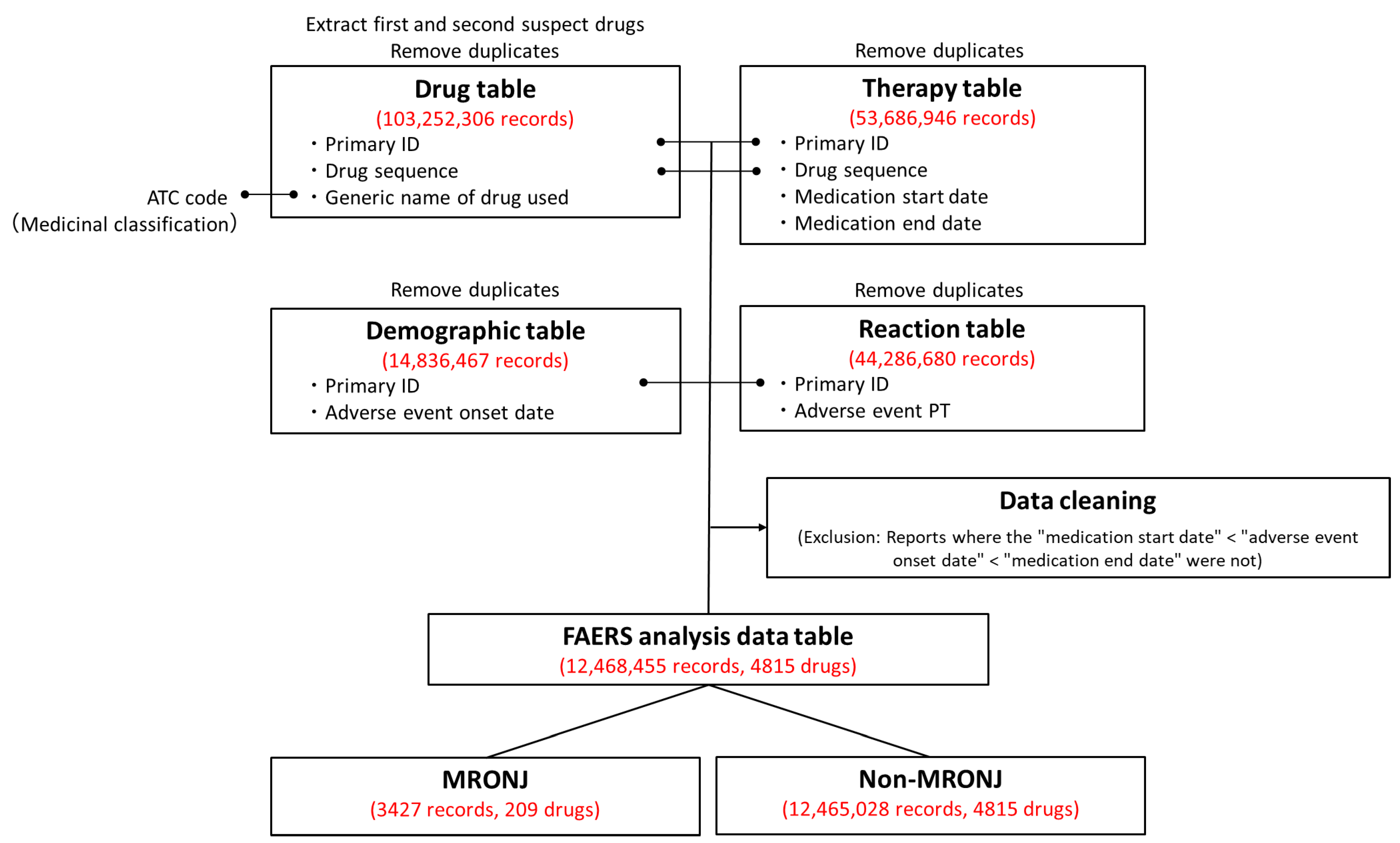
2.1. The FAERS Analysis Data Table
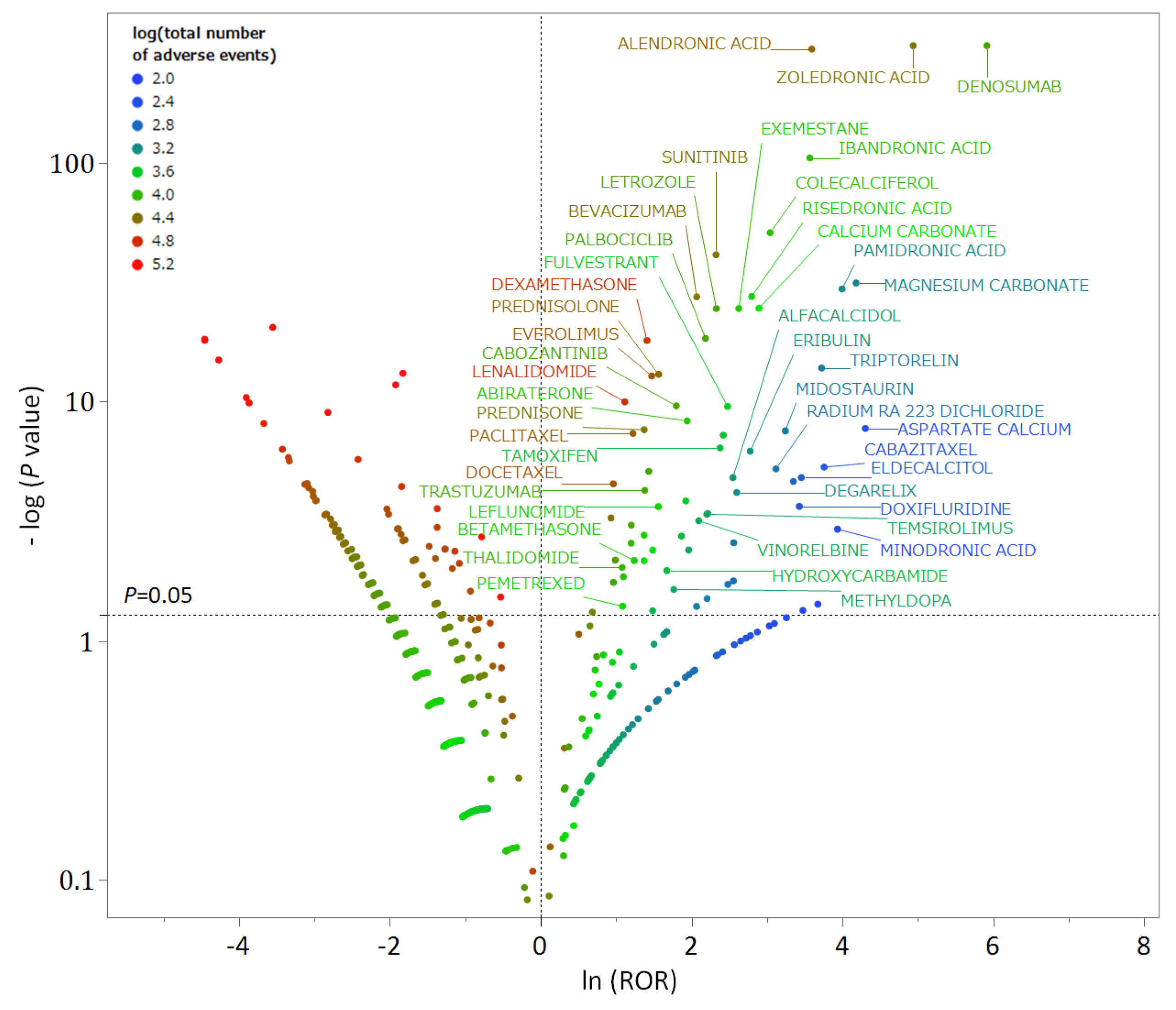
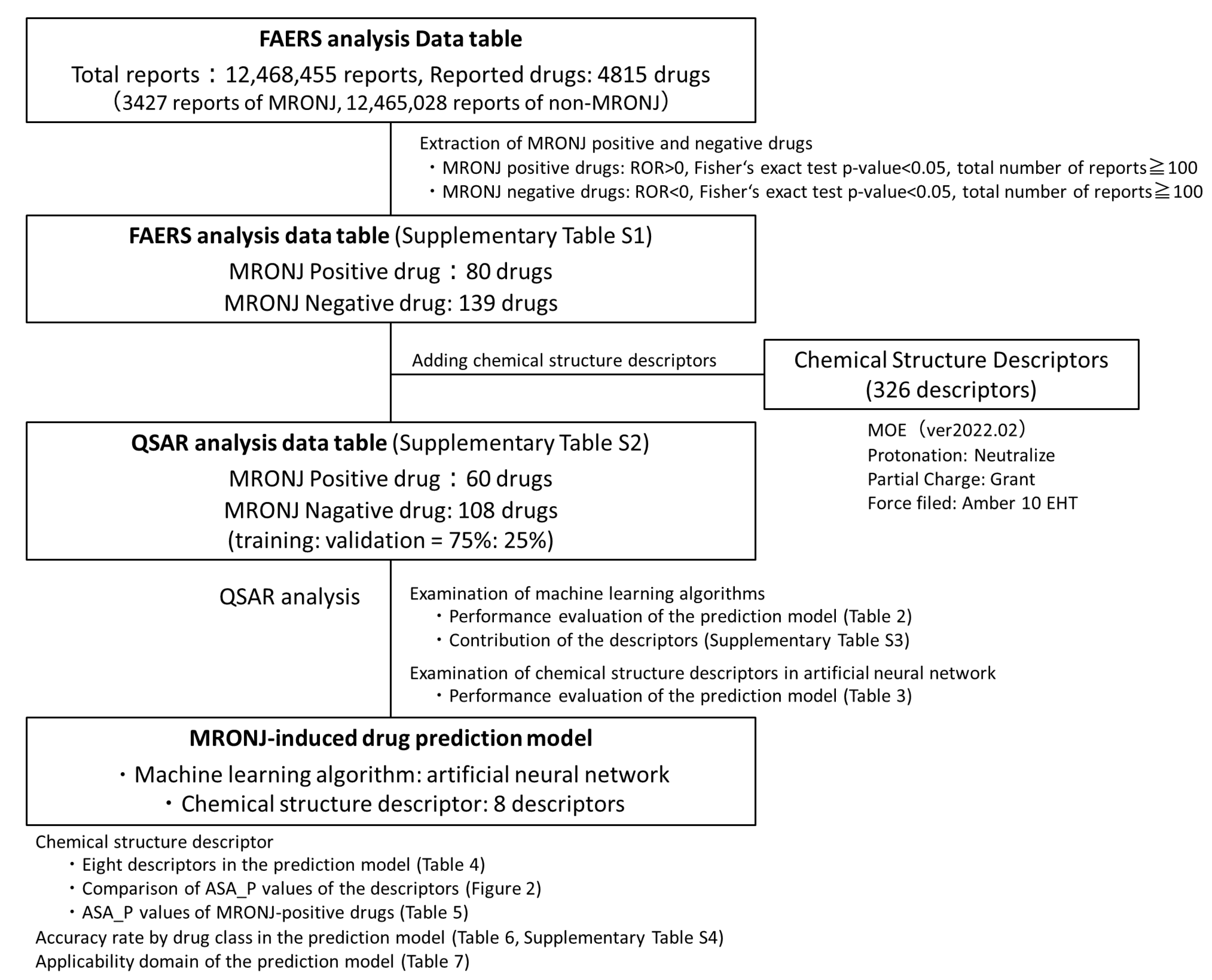
2.2. Positive and Negative Drugs for MRONJ
2.3. QSAR Analysis Data Table
2.4. QSAR Analysis Using Machine Learning (Construction of MRONJ-Induced Drug Prediction Model)
3. Discussion
3.1. Analysis of the Adverse Drug Reaction Database FAERS
3.2. Construction of the MRONJ-Induced Drug Prediction Model
3.3. Limitations
4. Materials and Methods
4.1. Creation of the FAERS Analysis Data Table
4.2. Examination of the FAERS Analysis Data Tables (Extraction of Positive and Negative MRONJ Drugs)
4.3. Creation of QSAR Analysis Data Tables (Addition of Chemical Structure Descriptors)
4.4. QSAR Analysis Using Machine Learning Algorithms (Construction of MRONJ-Induced Drug Prediction Model)
4.5. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| AUROC | Area under the receiver operating characteristic curve |
| FDA | Food and Drug Administration |
| MRONJ | Medication-related osteonecrosis of the jaw |
| QSAR | Quantitative structure–activity relationship |
| RANKL | Receptor activator of nuclear factor kappa B ligand |
| ROR | Reporting odds ratio |
| SMILES | The Simplified Molecular Input Line-Entry System |
References
- Khan, A.A.; Morrison, A.; Hanley, D.A.; Felsenberg, D.; McCauley, L.K.; O’Ryan, F.; Reid, I.R.; Ruggiero, S.L.; Taguchi, A.; Tetradis, S.; et al. Diagnosis and management of osteonecrosis of the jaw: A systematic review and international consensus. J. Bone Miner. Res. 2015, 30, 3–23. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.L.; Dodson, T.B.; Aghaloo, T.; Carlson, E.R.; Ward, B.B.; Kademani, D. American Association of Oral and Maxillofacial Surgeons’ Position Paper on Medication-Related Osteonecrosis of the Jaws-2022 Update. J. Oral Maxillofac. Surg. 2022, 80, 920–943. [Google Scholar] [CrossRef] [PubMed]
- Ishimaru, M.; Ono, S.; Morita, K.; Matsui, H.; Hagiwara, Y.; Yasunaga, H. Prevalence, Incidence Rate, and Risk Factors of Medication-Related Osteonecrosis of the Jaw in Patients with Osteoporosis and Cancer: A Nationwide Population-Based Study in Japan. J. Oral Maxillofac. Surg. 2022, 80, 714–727. [Google Scholar] [CrossRef]
- King, R.; Tanna, N.; Patel, V. Medication-related osteonecrosis of the jaw unrelated to bisphosphonates and denosumab—A review. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 127, 289–299. [Google Scholar] [CrossRef]
- Anastasilakis, A.D.; Pepe, J.; Napoli, N.; Palermo, A.; Magopoulos, C.; Khan, A.A.; Zillikens, M.C.; Body, J.J. Osteonecrosis of the Jaw and Antiresorptive Agents in Benign and Malignant Diseases: A Critical Review Organized by the ECTS. J. Clin. Endocrinol. Metab. 2022, 107, 1441–1460. [Google Scholar] [CrossRef]
- Japanese Allied Committee on Osteonecrosis of the Jaw; Yoneda, T.; Hagino, H.; Sugimoto, T.; Ohta, H.; Takahashi, S.; Soen, S.; Taguchi, A.; Nagata, T.; Urade, M.; et al. Antiresorptive agent-related osteonecrosis of the jaw: Position Paper 2017 of the Japanese Allied Committee on Osteonecrosis of the Jaw. J. Bone Miner. Metab. 2017, 35, 6–19. [Google Scholar] [CrossRef]
- Schiodt, M.; Otto, S.; Fedele, S.; Bedogni, A.; Nicolatou-Galitis, O.; Guggenberger, R.; Herlofson, B.B.; Ristow, O.; Kofod, T. Workshop of European task force on medication-related osteonecrosis of the jaw-Current challenges. Oral Dis. 2019, 25, 1815–1821. [Google Scholar] [CrossRef]
- Campisi, G.; Mauceri, R.; Bertoldo, F.; Bettini, G.; Biasotto, M.; Colella, G.; Consolo, U.; Di Fede, O.; Favia, G.; Fusco, V.; et al. Medication-Related Osteonecrosis of Jaws (MRONJ) Prevention and Diagnosis: Italian Consensus Update 2020. Int. J. Environ. Res. Public Health 2020, 17, 5998. [Google Scholar] [CrossRef]
- Edwards, I.R.; Lindquist, M.; Wiholm, B.E.; Napke, E. Quality criteria for early signals of possible adverse drug reactions. Lancet 1990, 336, 156–158. [Google Scholar] [CrossRef]
- Kimura, K.; Kikegawa, M.; Kan, Y.; Uesawa, Y. Identifying Crude Drugs in Kampo Medicines Associated with Drug-Induced Liver Injury Using the Japanese Adverse Drug Event Report Database: A Comprehensive Survey. Pharmaceuticals 2023, 16, 678. [Google Scholar] [CrossRef]
- Toriumi, S.; Mimori, R.; Sakamoto, H.; Sueki, H.; Yamamoto, M.; Uesawa, Y. Examination of Risk Factors and Expression Patterns of Atypical Femoral Fractures Using the Japanese Adverse Drug Event Report Database: A Retrospective Pharmacovigilance Study. Pharmaceuticals 2023, 16, 626. [Google Scholar] [CrossRef] [PubMed]
- Fang, H.; Su, Z.; Wang, Y.; Miller, A.; Liu, Z.; Howard, P.C.; Tong, W.; Lin, S.M. Exploring the FDA Adverse Event Reporting System to generate hypotheses for monitoring of disease characteristics. Clin. Pharmacol. Ther. 2014, 95, 496–498. [Google Scholar] [CrossRef] [PubMed]
- Hosoya, R.; Ishii-Nozawa, R.; Terajima, T.; Kagaya, H.; Uesawa, Y. The Association between Molecular Initiating Events and Drug-Induced Hiccups. Pharmaceuticals 2024, 17, 379. [Google Scholar] [CrossRef] [PubMed]
- Ahdi, H.S.; Wichelmann, T.A.; Pandravada, S.; Ehrenpreis, E.D. Medication-induced osteonecrosis of the jaw: A review of cases from the Food and Drug Administration Adverse Event Reporting System (FAERS). BMC Pharmacol. Toxicol. 2023, 24, 15. [Google Scholar] [CrossRef]
- Nathan, K.T.; Conn, K.M.; van Manen, R.P.; Brown, J.E. Signal detection for bleeding associated with the use of direct oral anticoagulants. Am. J. Health Syst. Pharm. 2018, 75, 973–977. [Google Scholar] [CrossRef]
- Sanagawa, A.; Hotta, Y.; Kondo, M.; Nishikawa, R.; Tohkin, M.; Kimura, K. Tumor lysis syndrome associated with bortezomib: A post-hoc analysis after signal detection using the US Food and Drug Administration Adverse Event Reporting System. Anticancer Drugs 2020, 2, 183–189. [Google Scholar] [CrossRef]
- Evans, S.J.; Waller, P.C.; Davis, S. Use of proportional reporting ratios (PRRs) for signal generation from spontaneous adverse drug reaction reports. Pharmacoepidemiol. Drug Saf. 2001, 6, 483–486. [Google Scholar] [CrossRef]
- Sakaeda, T.; Tamon, A.; Kadoyama, K.; Okuno, Y. Data mining of the public version of the FDA Adverse Event Reporting System. Int. J. Med. Sci. 2013, 7, 796–803. [Google Scholar] [CrossRef]
- van Puijenbroek, E.P.; Bate, A.; Leufkens, H.G.; Lindquist, M.; Orre, R.; Egberts, A.C. A comparison of measures of disproportionality for signal detection in spontaneous reporting systems for adverse drug reactions. Pharmacoepidemiol. Drug Saf. 2002, 11, 3–10. [Google Scholar] [CrossRef]
- Toriumi, S.; Kobayashi, A.; Sueki, H.; Yamamoto, M.; Uesawa, Y. Exploring the Mechanisms Underlying Drug-Induced Fractures Using the Japanese Adverse Drug Event Reporting Database. Pharmaceuticals 2021, 14, 1299. [Google Scholar] [CrossRef]
- FDA Adverse Event Reporting System (FAERS). Available online: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-adverse-event-reporting-system-faers (accessed on 5 June 2022).
- Zhang, S. Computer-aided drug discovery and development. Methods Mol. Biol. 2011, 716, 23–38. [Google Scholar] [CrossRef] [PubMed]
- Kunimoto, R.; Bajorath, J.; Aoki, K. From traditional to data-driven medicinal chemistry: A case study. Drug Discov. Today 2022, 8, 2065–2070. [Google Scholar] [CrossRef] [PubMed]
- Hansch, C.; Maloney, P.; Fujita, T.; Muir, R.M. Correlation of Biological Activity of Phenoxyacetic Acids with Hammett Substituent Constants and Partition Coefficients. Nature 1962, 194, 178–180. [Google Scholar] [CrossRef]
- Hansch, C.; Fujita, T. p-σ-π Analysis. A Method for the Correlation of Biological Activity and Chemical Structure. J. Am. Chem. Soc. 1964, 86, 1616–1626. [Google Scholar] [CrossRef]
- Hansen, K.; Mika, S.; Schroeter, T.; Sutter, A.; ter Laak, A.; Steger-Hartmann, T.; Heinrich, N.; Müller, K.R. Benchmark data set for in silico prediction of Ames mutagenicity. J. Chem. Inf. Model. 2009, 49, 2077–2081. [Google Scholar] [CrossRef]
- Uesawa, Y. Quantitative structure-activity relationship analysis using deep learning based on a novel molecular image input technique. Bioorg. Med. Chem. Lett. 2018, 28, 3400–3403. [Google Scholar] [CrossRef]
- Zhang, J.; Mucs, D.; Norinder, U.; Svensson, F. LightGBM: An Effective and Scalable Algorithm for Prediction of Chemical Toxicity-Application to the Tox21 and Mutagenicity Data Sets. J. Chem. Inf. Model. 2019, 59, 4150–4158. [Google Scholar] [CrossRef]
- Song, X.; Liu, X.; Liu, F.; Wang, C. Comparison of machine learning and logistic regression models in predicting acute kidney injury: A systematic review and meta-analysis. Int. J. Med. Inform. 2021, 151, 104484. [Google Scholar] [CrossRef]
- Liew, B.X.W.; Kovacs, F.M.; Rügamer, D.; Royuela, A. Machine learning versus logistic regression for prognostic modelling in individuals with non-specific neck pain. Eur. Spine J. 2022, 8, 2082–2091. [Google Scholar] [CrossRef]
- Song, Y.X.; Yang, X.D.; Luo, Y.G.; Ouyang, C.L.; Yu, Y.; Ma, Y.L.; Li, H.; Lou, J.S.; Liu, Y.H.; Chen, Y.Q.; et al. Comparison of logistic regression and machine learning methods for predicting postoperative delirium in elderly patients: A retrospective study. CNS Neurosci. Ther. 2023, 1, 158–167. [Google Scholar] [CrossRef]
- Ranganathan, P.; Pramesh, C.S.; Aggarwal, R. Common pitfalls in statistical analysis: Logistic regression. Perspect. Clin. Res. 2017, 3, 148–151. [Google Scholar] [CrossRef] [PubMed]
- Ambe, K.; Ohya, K.; Takada, W.; Suzuki, M.; Tohkin, M. In Silico Approach to Predict Severe Cutaneous Adverse Reactions Using the Japanese Adverse Drug Event Report Database. Clin. Transl. Sci. 2021, 2, 756–763. [Google Scholar] [CrossRef] [PubMed]
- Levy, J.J.; O’Malley, A.J. Don’t dismiss logistic regression: The case for sensible extraction of interactions in the era of machine learning. BMC Med. Res. Methodol. 2020, 20, 171. [Google Scholar] [CrossRef]
- Polo, T.C.F.; Miot, H.A. Use of ROC curves in clinical and experimental studies. J. Vasc. Bras. 2020, 19, e20200186. [Google Scholar] [CrossRef]
- Graharm, R.; Russell, G. Bisphosphonates: The first 40 years. Bone 2011, 49, 2–19. [Google Scholar] [CrossRef]
- Saad, F.; Brown, S.F.; Poznak, C.V.; Ibrahim, T.; Stemmer, S.M.; Stopeck, A.T.; Diel, I.J.; Takahashi, S.; Shore, N.; Henry, D.H.; et al. Incidence, risk factors, and outcomes of osteonecrosis of the jaw: Integrated analysis from three blinded active-controlled phase III trials in cancer patients with bone metastases. Ann. Oncol. 2012, 23, 1341–1347. [Google Scholar] [CrossRef]
- Hasegawa, S.; Ikesue, H.; Satake, R.; Inoue, M.; Yoshida, Y.; Tanaka, M.; Matsumoto, K.; Wakabayashi, W.; Oura, K.; Muroi, N.; et al. Osteonecrosis of the Jaw Caused by Denosumab in Treatment-Naïve and Pre-Treatment with Zoledronic Acid Groups: A Time-to-Onset Study Using the Japanese Adverse Drug Event Report (JADER) Database. Drugs Real World Outcomes 2022, 9, 659–665. [Google Scholar] [CrossRef]
- Brunello, A.; Saia, G.; Bedogni, A.; Scaglione, D.; Basso, U. Worsening of osteonecrosis of the jaw during treatment with sunitinib in a patient with metastatic renal cell carcinoma. Bone 2009, 44, 173–175. [Google Scholar] [CrossRef]
- Pimolbutr, K.; Porter, S.; Fedele, S. Osteonecrosis of the Jaw Associated with Antiangiogenics in Antiresorptive-Naïve Patient: A Comprehensive Review of the Literature. Biomed. Res. Int. 2018, 2018, 8071579. [Google Scholar] [CrossRef]
- Eguia, A.; Bagán-Debón, L.; Cardona, F. Review and update on drugs related to the development of osteonecrosis of the jaw. Med. Oral Patol. Oral Cir. Bucal. 2020, 25, e71–e83. [Google Scholar] [CrossRef]
- Di Fede, O.; Bedogni, A.; Giancola, F.; Saia, G.; Bettini, G.; Toia, F.; D’Alessandro, N.; Firenze, A.; Matranga, D.; Fedele, S.; et al. BRONJ in patients with rheumatoid arthritis: A multicenter case series. Oral Dis. 2016, 22, 543–548. [Google Scholar] [CrossRef] [PubMed]
- Tsao, C.; Darby, I.; Ebeling, P.R.; Walsh, K.; O’Brien-Simpson, N.; Reynolds, E.; Borromeo, G. Oral health risk factors for bisphosphonate-associated jaw osteonecrosis. J. Oral Maxillofac. Surg. 2013, 71, 1360–1366. [Google Scholar] [CrossRef] [PubMed]
- Khosla, S.K.; Oursler, M.J.; Monroe, D.G. Estrogen and the skeleton. Trends Endocrinol. Metab. 2012, 23, 576–581. [Google Scholar] [CrossRef] [PubMed]
- Toriumi, S.; Kobayashi, A.; Uesawa, Y. Comprehensive Study of the Risk Factors for Medication-Related Osteonecrosis of the Jaw Based on the Japanese Adverse Drug Event Report Database. Pharmaceuticals 2020, 13, 467. [Google Scholar] [CrossRef]
- Puljula, E.; Turhanen, P.; Vepsäläinen, J.; Monteil, M.; Lecouvey, M.; Weisell, J. Structural requirements for bisphosphonate binding on hydroxyapatite: NMR study of bisphosphonate partial esters. ACS Med. Chem. Lett. 2015, 6, 397–401. [Google Scholar] [CrossRef]
- Russell, R.G.; Xia, Z.; Dunford, J.E.; Oppermann, U.; Kwaasi, A.; Hulley, P.A.; Kavanagh, K.L.; Triffitt, J.T.; Lundy, M.W.; Phipps, R.J.; et al. Bisphosphonates: An update on mechanisms of action and how these relate to clinical efficacy. Ann. N. Y. Acad. Sci. 2007, 1117, 209–257. [Google Scholar] [CrossRef]
- Hughes, D.E.; MacDonald, B.R.; Russell, R.G.; Gowen, M. Inhibition of osteoclast-like cell formation by bisphosphonates in long-term cultures of human bone marrow. J. Clin. Investig. 1989, 83, 1930–1935. [Google Scholar] [CrossRef]
- Chavassieux, P.M.; Arlot, M.E.; Reda, C.; Wei, L.; Yates, A.J.; Meunier, P.J. Histomorphometric assessment of the long-term effects of alendronate on bone quality and remodeling in patients with osteoporosis. J. Clin. Investig. 1997, 100, 1475–1480. [Google Scholar] [CrossRef]
- Wood, J.; Bonjean, K.; Ruetz, S.; Bellahcène, A.; Devy, L.; Foidart, J.M.; Castronovo, V.; Green, J.R. Novel antiangiogenic effects of the bisphosphonate compound zoledronic acid. J. Pharmacol. Exp. Ther. 2002, 302, 1055–1061. [Google Scholar] [CrossRef]
- Tseng, H.C.; Kanayama, K.; Kaur, K.; Park, S.H.; Park, S.; Kozlowska, A.; Sun, S.; McKenna, C.E.; Nishimura, I.; Jewett, A. Bisphosphonate-induced differential modulation of immune cell function in gingiva and bone marrow in vivo: Role in osteoclast-mediated NK cell activation. Oncotarget 2015, 24, 20002–20025. [Google Scholar] [CrossRef]
- Lombard, T.; Neirinckx, V.; Rogister, B.; Gilon, Y.; Wislet, S. Medication-Related Osteonecrosis of the Jaw: New Insights into Molecular Mechanisms and Cellular Therapeutic Approaches. Stem Cells Int. 2016, 8768162. [Google Scholar] [CrossRef] [PubMed]
- Roskoski, R., Jr. Properties of FDA-approved small molecule protein kinase inhibitors: A 2024 update. Pharmacol. Res. 2024, 200, 107059. [Google Scholar] [CrossRef]
- Aldridge, S.E.; Lennard, T.W.; Williams, J.R.; Birch, M.A. Vascular endothelial growth factor receptors in osteoclast differentiation and function. Biochem. Biophys. Res. Commun. 2005, 335, 793–798. [Google Scholar] [CrossRef]
- Pazianas, M. Osteonecrosis of the jaw and the role of macrophages. J. Natl. Cancer Inst. 2011, 103, 232–240. [Google Scholar] [CrossRef] [PubMed]
- Madaj, R.; Pawlowska, R.; Chworos, A. In silico exploration of binding of selected bisphosphonate derivatives to placental alkaline phosphatase via docking and molecular dynamics. J. Mol. Graph. Model. 2021, 103, 107801. [Google Scholar] [CrossRef]
- Zhuravleva, I.Y.; Dokuchaeva, A.A.; Karpova, E.V.; Timchenko, T.P.; Titov, A.T.; Shatskaya, S.S.; Polienko, Y.F. Immobilized Bisphosphonates as Potential Inhibitors of Bioprosthetic Calcification: Effects on Various Xenogeneic Cardiovascular Tissues. Biomedicines 2021, 10, 65. [Google Scholar] [CrossRef]
- Weiss-Smith, S.; Deshpande, G.; Chung, S.; Gogolak, V. The FDA drug safety surveillance program: Adverse event reporting trends. Arch. Intern. Med. 2011, 171, 591–593. [Google Scholar] [CrossRef]
- Neha, R.; Beulah, E.; Anusha, B.; Vasista, S.; Stephy, C.; Subeesh, V. Aromatase inhibitors associated osteonecrosis of jaw: Signal refining to identify pseudo safety signals. Int. J. Clin. Pharm. 2020, 42, 721–727. [Google Scholar] [CrossRef]
- Gudivada, V.N.; Apon, A.; Ding, J. Data Quality Considerations for Big Data and Machine Learning: Going Beyond Data Cleaning and Transformations. Int. J. Adv. Softw. 2017, 10, 1–20. [Google Scholar]
- Joonho, G.; Hyunjoong, K. RHSBoost: Improving classification performance in imbalance data. Comput. Stat. Data Anal. 2017, 111, 1–13. [Google Scholar] [CrossRef]
- Ezzat, A.; Wu, M.; Li, X.L.; Kwoh, C.K. Drug-target interaction prediction via class imbalance-aware ensemble learning. BMC Bioinform. 2016, 17, 509. [Google Scholar] [CrossRef] [PubMed]
- ATC/DDD Index. Available online: https://atcddd.fhi.no/atc_ddd_index/ (accessed on 3 July 2022).
- Lumini, A.; Nanni, L. Convolutional Neural Networks for ATC Classification. Curr. Pharm. Des. 2018, 34, 4007–4012. [Google Scholar] [CrossRef] [PubMed]
- ICH Harmonisation for Berrer Health. Available online: https://www.ich.org/ (accessed on 1 July 2022).
- MedDRA; Medical Dictionary for Regulatory Activities. Available online: https://www.meddra.org/how-to-use/support-documentation/japanese/welcome (accessed on 3 July 2022).
- Kan, Y.; Nagai, J.; Uesawa, Y. Evaluation of antibiotic-induced taste and smell disorders using the FDA Adverse Event Reporting System database. Sci. Rep. 2021, 11, 9625. [Google Scholar] [CrossRef] [PubMed]
- Okunaka, M.; Kano, D.; Uesawa, Y. Nuclear receptor and stress response pathways associated with antineoplastic agent-induced diarrhea. Int. J. Mol. Sci. 2022, 23, 12407. [Google Scholar] [CrossRef]
- Oshima, Y.; Tanimoto, T.; Yuji, K.; Tojo, A. Association between GvHD and nivolumab in the FDA Adverse Event Reporting System. Bone Marrow Transplant. 2017, 52, 1463–1464. [Google Scholar] [CrossRef]
- Rothman, K.J.; Lanes, S.; Sacks, S.T. The reporting odds ratio and its advantages over the proportional reporting ratio. Pharmacoepidemiol. Drug Saf. 2004, 13, 519–523. [Google Scholar] [CrossRef]
- Harpaz, R.; DuMouchel, W.; LePendu, P.; Bauer-Mehren, A.; Ryan, P.; Shah, N.H. Performance of pharmacovigilance signal-detection algorithms for the FDA Adverse Event Reporting System. Clin. Pharmacol. Ther. 2013, 93, 539–546. [Google Scholar] [CrossRef]
- European Medicines Agency. “Guideline on the Use of Statistical Signal Detection Methods in the Eudravigilance Data Analysis System”. Available online: https://www.ema.europa.eu/en/documents/regulatory-procedural-guideline/draft-guideline-use-statistical-signal-detection-methods-eudravigilance-data-analysis-system_en.pdf (accessed on 5 July 2022).
- Kurosaki, K.; Uesawa, Y. Molecular Initiating Events Associated with Drug-Induced Liver Malignant Tumors: An Integrated Study of the FDA Adverse Event Reporting System and Toxicity Predictions. Biomolecules 2021, 11, 944. [Google Scholar] [CrossRef]
- Chen, J.J.; Wang, S.J.; Tsai, C.A.; Lin, C.J. Selection of differentially expressed genes in microarray data analysis. Pharmacogenomics J. 2007, 7, 212–220. [Google Scholar] [CrossRef]
- Cui, X.; Churchill, G.A. Statistical tests for differential expression in cDNA microarray experiments. Genome Biol. 2003, 4, 210. [Google Scholar] [CrossRef]
- PubChem. Available online: https://pubchem.ncbi.nlm.nih.gov/ (accessed on 1 July 2022).
- MOE. Available online: https://www.chemcomp.com/Products.htm (accessed on 18 July 2022).
- Breiman, L. Random Forests. Mach. Learn. 2001, 45, 5–32. [Google Scholar] [CrossRef]
- Friedman, J.H. Greedy function approximation: A gradient boosting machine. Ann. Statist. 2001, 29, 1189–1232. [Google Scholar] [CrossRef]
- Hornik, K.; Stinchcombe, M.; White, H. Multilayer feedforward networks are universal approximators. Neural Netw. 1989, 2, 359–366. [Google Scholar] [CrossRef]
- Mamada, H.; Iwamoto, K.; Nomura, Y.; Uesawa, Y. Predicting blood-to-plasma concentration ratios of drugs from chemical structures and volumes of distribution in humans. Mol. Divers. 2021, 3, 1261–1270. [Google Scholar] [CrossRef]
- Nishikiori, K.; Tanaka, K.; Uesawa, Y. Construction of a prediction model for drug removal rate in hemodialysis based on chemical structures. Mol. Divers. 2022, 5, 2647–2657. [Google Scholar] [CrossRef]
- Sahigara, F.; Mansouri, K.; Ballabio, D.; Mauri, A.; Consonni, V.; Todeschini, R. Comparison of different approaches to define the applicability domain of QSAR models. Molecules 2012, 17, 4791–4810. [Google Scholar] [CrossRef]
- Akobeng, A.K. Understanding diagnostic tests 3: Receiver operating characteristic curves. Acta Paediatr. 2007, 96, 644–647. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Drug Name | Drug Group | Number of MRONJ Reports | ROR | p-Value | φ Coefficient |
|---|---|---|---|---|---|
| Denosumab | Anti-RANKL antibody | 907 | 373.78 | <0.0001 | 0.136 |
| Zoledronic acid | Bisphosphonates | 702 | 140.70 | <0.0001 | 0.078 |
| Alendronic acid | Bisphosphonate | 264 | 36.69 | <0.0001 | 0.026 |
| Ibandronic acid | Bisphosphonate | 92 | 35.77 | <0.0001 | 0.015 |
| Sunitinib | Anticancer drugs | 65 | 10.30 | <0.0001 | 0.007 |
| Dexamethasone | Corticosteroids | 60 | 4.12 | <0.0001 | 0.003 |
| Cholecalciferol | Vitamin D | 55 | 21.13 | <0.0001 | 0.009 |
| Bevacizumab | Anticancer drugs | 51 | 7.96 | <0.0001 | 0.005 |
| Lenalidomide | Anticancer drugs | 47 | 3.07 | <0.0001 | 0.002 |
| Everolimus | Anticancer drugs | 39 | 4.39 | <0.0001 | 0.003 |
| Letrozole | Anticancer drugs | 38 | 10.34 | <0.0001 | 0.005 |
| Prednisolone | Corticosteroids | 36 | 4.81 | <0.0001 | 0.003 |
| Risedronic acid | Bisphosphonates | 33 | 16.50 | <0.0001 | 0.006 |
| Exemestane | Anticancer drugs | 32 | 13.92 | <0.0001 | 0.005 |
| Palbociclib | Anticancer drugs | 31 | 8.96 | <0.0001 | 0.004 |
| Paclitaxel | Anticancer drugs | 29 | 3.42 | <0.0001 | 0.002 |
| Calcium carbonate | Calcium | 28 | 18.19 | <0.0001 | 0.006 |
| Docetaxel | Anticancer drugs | 25 | 2.64 | <0.0001 | 0.001 |
| Prednisone | Corticosteroids | 25 | 3.97 | <0.0001 | 0.002 |
| Pamidronic acid | Bisphosphonates | 22 | 54.81 | <0.0001 | 0.009 |
| Machine Learning Algorithms | AUROC of the Training Data | AUROC of the Validation Data | Cutoff Value | Accuracy | Precision/Positive Predictive Value | Negative Predictive Value | Recall/ Sensitivity | Specificity | Balanced Accuracy | F1-Score | Matthews Correlation Coefficient |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Random Forest | 0.996 | 0.726 | 0.533 | 0.714 | 0.600 | 0.778 | 0.600 | 0.778 | 0.689 | 0.600 | 0.378 |
| Gradient Boosting | 0.956 | 0.714 | 0.484 | 0.714 | 0.636 | 0.742 | 0.467 | 0.852 | 0.659 | 0.538 | 0.347 |
| Artificial Neural Networks | 0.849 | 0.741 | 0.526 | 0.714 | 0.579 | 0.826 | 0.733 | 0.704 | 0.719 | 0.647 | 0.421 |
| Number of Chemical Structure Descriptors * | AUROC of the Training Data | AUROC of the Validation Data | Cutoff Value | Accuracy | Precision/Positive Predictive Value | Negative Predictive Value | Recall/ Sensitivity | Specificity | Balanced Accuracy | F1-Score | Matthews Correlation Coefficient |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 5 Descriptors | 0.713 | 0.699 | 0.363 | 0.667 | 0.600 | 0.676 | 0.200 | 0.926 | 0.563 | 0.300 | 0.186 |
| 6 Descriptors | 0.837 | 0.724 | 0.479 | 0.714 | 0.600 | 0.778 | 0.600 | 0.778 | 0.689 | 0.600 | 0.378 |
| 7 Descriptors | 0.703 | 0.719 | 0.554 | 0.714 | 0.615 | 0.759 | 0.533 | 0.815 | 0.674 | 0.571 | 0.361 |
| 8 Descriptors | 0.871 | 0.778 | 0.291 | 0.738 | 0.667 | 0.767 | 0.533 | 0.852 | 0.693 | 0.593 | 0.409 |
| 9 Descriptors | 0.871 | 0.761 | 0.383 | 0.714 | 0.600 | 0.778 | 0.600 | 0.778 | 0.689 | 0.600 | 0.378 |
| 10 Descriptors | 0.877 | 0.748 | 0.265 | 0.667 | 0.533 | 0.741 | 0.533 | 0.741 | 0.637 | 0.533 | 0.274 |
| 20 Descriptors | 0.786 | 0.724 | 0.463 | 0.762 | 0.778 | 0.758 | 0.467 | 0.926 | 0.696 | 0.583 | 0.458 |
| 30 Descriptors | 0.777 | 0.716 | 0.274 | 0.738 | 0.667 | 0.767 | 0.533 | 0.852 | 0.693 | 0.593 | 0.409 |
| Descriptor | Definition | Number of Branches * |
|---|---|---|
| ASA_P | Total polar surface area | 7 |
| PEOE_VSA_FHYD | Fractional hydrophobic dw surface area | 3 |
| PEOE_VSA-5 | Total negative 5 dw surface area | 3 |
| h_pavgQ | Total average charge (pH = 7) | 3 |
| lip_acc | Lipinski acceptor count | 3 |
| vsa_acc | VDW acceptor surface area (A**2) | 2 |
| vsa_pol | VDW polar surface area (A**2) | 2 |
| CASA- | Charge-weighted negative surface area | 2 |
| Drug Name | ATC Code | Drug Group | ASA_P * |
|---|---|---|---|
| Detirelix | L02BX02 | Anticancer drug (hormone-related drugs) | 533.2 |
| Triptorelin | L02AE04 | Anticancer drug (hormone-related drugs) | 509.8 |
| Leuprorelin | L02AE02 | Anticancer drug (hormone-related drugs) | 412.1 |
| Cefcapene | J01DD17 | Antibiotics | 322.2 |
| Pamidronic acid | M05BA03 | Bisphosphonates | 305.2 |
| Alendronic acid | M05BA04 | Bisphosphonates | 302.7 |
| Pemetrexed | L01BA04 | Anticancer drug (metabolic antagonists) | 294.9 |
| Docetaxel | L01CD02 | Anticancer drug (taxanes) | 284.6 |
| Melphalan | L01AA03 | Anticancer drug (alkylating agents) | 283.3 |
| Bicalutamide | L02BB03 | Anticancer drug (hormone-related drugs) | 267.5 |
| Epacadostat | L01XX58 | Anticancer drug (others) | 267.1 |
| Paclitaxel | L01CD01 | Anticancer drug (taxanes) | 265.3 |
| Zoledronic acid | M05BA08 | Bisphosphonates | 263.6 |
| Temsirolimus | L01EG01 | Anticancer drug (protein kinase inhibitors) | 260.5 |
| Allelism | L01EM03 | Anticancer drug (protein kinase inhibitors) | 259.5 |
| Anastrozole | L02BG03 | Anticancer drug (hormone-related drugs) | 256.4 |
| Fulvestrant | L02BA03 | Anticancer drug (hormone-related drugs) | 254.4 |
| Ibandronic acid | M05BA06 | Bisphosphonates | 252.1 |
| Risedronic acid | M05BA07 | Bisphosphonates | 244.2 |
| Capecitabine | L01BC06 | Anticancer drug (metabolic antagonists) | 240.3 |
| Drug Classes in the ATC Classification | FAERS Analysis Data Table | Classification Results for the MRONJ Prediction Model | ||
|---|---|---|---|---|
| Number of Drugs (Positive/Negative) | Positive | Negative | Accuracy | |
| L01E Protein kinase inhibitors | 14 (11/3) | 13 | 1 | 0.75 |
| L02B Hormone antagonists and related agents | 7 (7/0) | 6 | 1 | 0.75 |
| L01X Other antineoplastic agents | 6 (6/0) | 5 | 1 | 0.71 |
| M05B Drugs affect bone structure and mineralization | 6 (6/0) | 6 | 0 | 1.00 |
| L04A Immunosuppressants | 9 (5/4) | 4 | 5 | 0.80 |
| A11C Vitamin a and d, incl. combinations of the two | 4 (4/0) | 4 | 0 | 1.00 |
| H02A Corticosteroids for systemic use, plain | 4 (4/0) | 4 | 0 | 1.00 |
| L01C Plant alkaloids and other natural products | 4 (4/0) | 4 | 0 | 1.00 |
| R01A Decongestants and other nasal preparations for topical use | 7 (3/4) | 5 | 2 | 0.56 |
| D07A Corticosteroids, plain | 5 (3/2) | 5 | 0 | 0.43 |
| A07E Intestinal antiinflammatory agents | 4 (3/1) | 4 | 0 | 0.60 |
| C05A Agents for treatment of hemorrhoids and anal fissures for topical use | 4 (3/1) | 3 | 1 | 1.00 |
| S01B Antiinflammatory agents | 4 (3/1) | 3 | 1 | 1.00 |
| Applicability Domain | Number of Drugs in Applicability Domain | Accuracy | Precision/Positive Predictive Value | Negative Predictive Value | Recall/Sensitivity | Specificity | Balanced Accuracy | F1-Score | Matthews Correlation Coefficient |
|---|---|---|---|---|---|---|---|---|---|
| Exclusion: Cutoff value 0.5 ± 0 (No exclusion) | 42 | 0.738 | 0.667 | 0.767 | 0.533 | 0.852 | 0.693 | 0.593 | 0.409 |
| Exclusion: Cutoff value 0.5 ± 0.1 (Applicability: 40–60% exclusion) | 32 | 0.656 | 0.476 | 1.000 | 1.000 | 0.500 | 0.750 | 0.645 | 0.488 |
| Exclusion: Cutoff value 0.5 ± 0.2 (Applicability: 30–70% exclusion) | 17 | 0.765 | 0.636 | 1.000 | 1.000 | 0.600 | 0.800 | 0.778 | 0.618 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toriumi, S.; Shimokawa, K.; Yamamoto, M.; Uesawa, Y. Development of a Medication-Related Osteonecrosis of the Jaw Prediction Model Using the FDA Adverse Event Reporting System Database and Machine Learning. Pharmaceuticals 2025, 18, 423. https://doi.org/10.3390/ph18030423
Toriumi S, Shimokawa K, Yamamoto M, Uesawa Y. Development of a Medication-Related Osteonecrosis of the Jaw Prediction Model Using the FDA Adverse Event Reporting System Database and Machine Learning. Pharmaceuticals. 2025; 18(3):423. https://doi.org/10.3390/ph18030423
Chicago/Turabian StyleToriumi, Shinya, Komei Shimokawa, Munehiro Yamamoto, and Yoshihiro Uesawa. 2025. "Development of a Medication-Related Osteonecrosis of the Jaw Prediction Model Using the FDA Adverse Event Reporting System Database and Machine Learning" Pharmaceuticals 18, no. 3: 423. https://doi.org/10.3390/ph18030423
APA StyleToriumi, S., Shimokawa, K., Yamamoto, M., & Uesawa, Y. (2025). Development of a Medication-Related Osteonecrosis of the Jaw Prediction Model Using the FDA Adverse Event Reporting System Database and Machine Learning. Pharmaceuticals, 18(3), 423. https://doi.org/10.3390/ph18030423