
Dezocine and Addiction: Friend or Foe?



Abstract
1. Introduction
2. Medicinal Chemistry of Dezocine
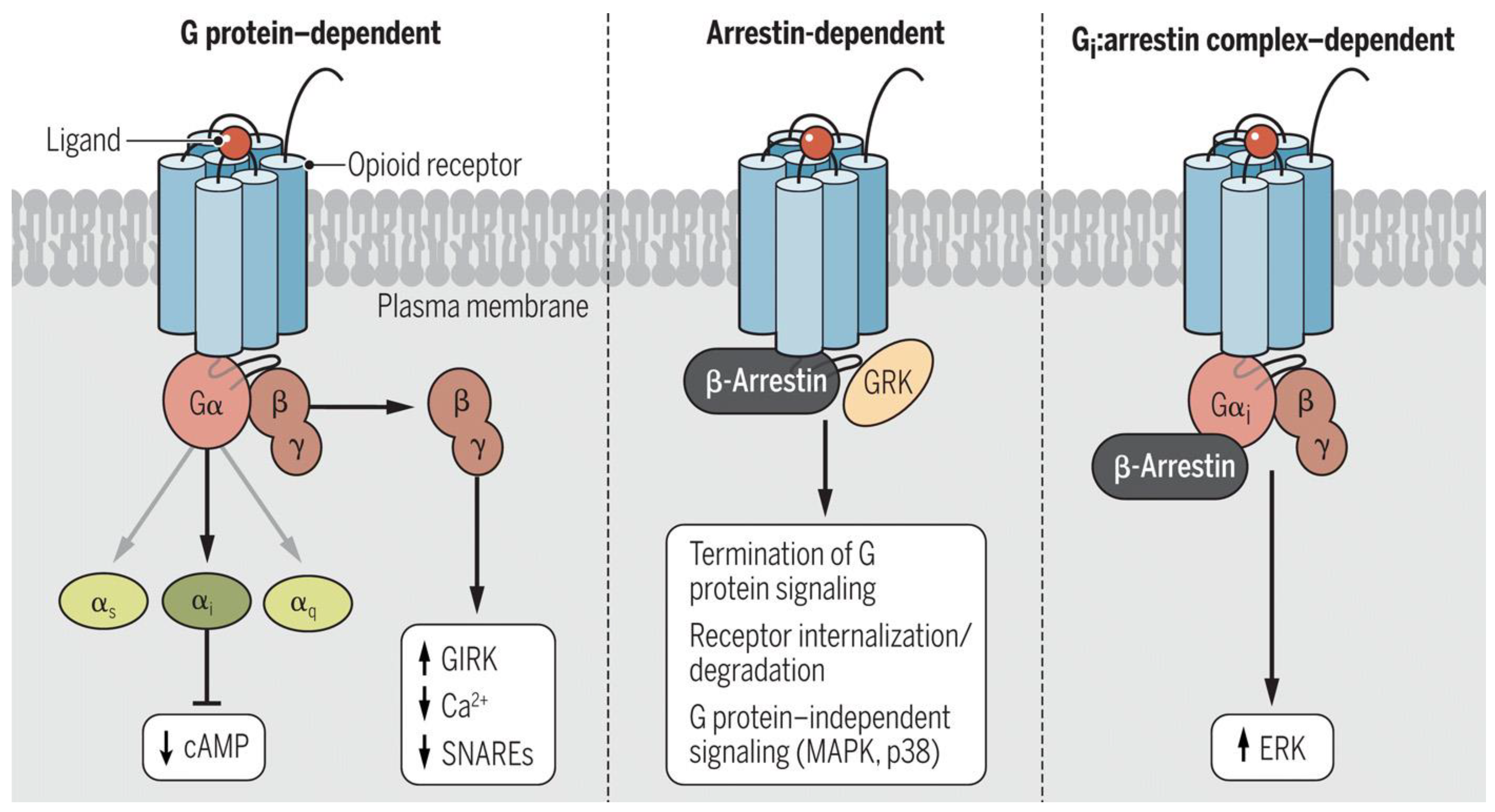
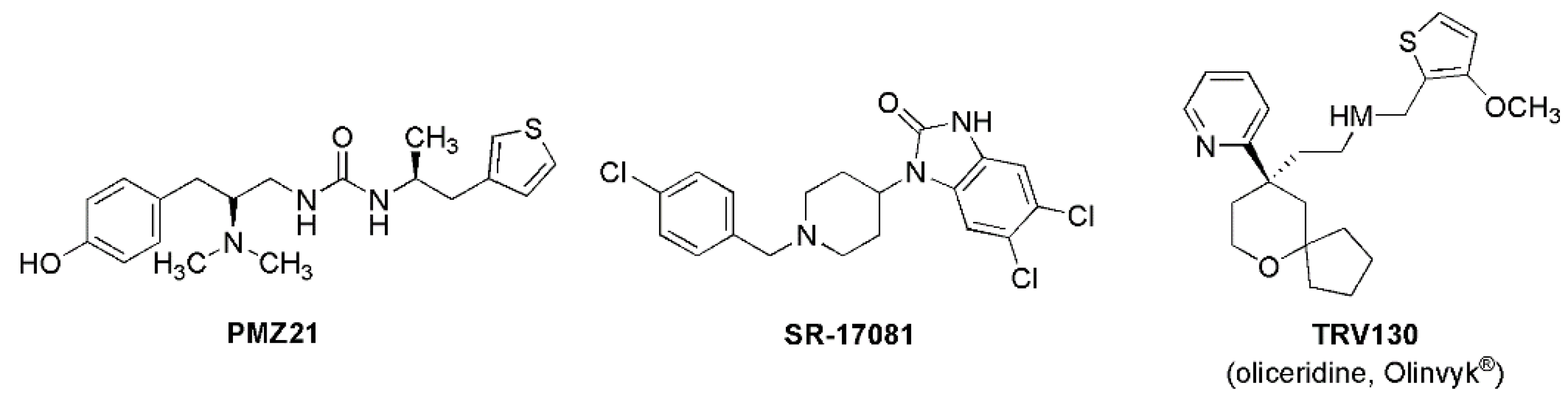
3. Biased Ligand Signaling
4. Dezocine and Biogenic Amine Reuptake
5. Dezocine and Addiction
6. Dezocine and Lack of Withdrawal Symptoms
7. Dezocine and Addressing Physicochemical Properties
8. Opinion: Uses of Dezocine
9. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Schiff, P.L., Jr. Opium and its alkaloids. Am. J. Pharma. Ed. 2002, 66, 186–194. [Google Scholar]
- Bandyopadhyay, S. An 8000-year history of use and abuse of opium and opioids: How that matters for a successful control of the epidemic? Neurology 2019, 92 (Suppl. S15), 49–55. [Google Scholar]
- Klockgether-Radke, A.P. FW Serturner and the discovery of morphine. 200 years of pain therapy with opioids. Anasthesiol. Intensivmed. Notfallmed. Schmerzther. 2002, 37, 244–249. [Google Scholar] [CrossRef]
- Sneader, W. The discovery of heroin. Lancet 1998, 352, 1697–1699. [Google Scholar] [CrossRef]
- Dydyk, A.M.; Jain, N.K. Opioid Use Disorder. StatPearls. 2024. Available online: https://www.statpearls.com/point-of-care/42233#:~:text=Opioid%20Use%20Disorder,dependence%20on%20opi (accessed on 2 January 2025).
- Drug Overdose Deaths: Facts and Figures, National Institute on Drug Abuse. Available online: https://nida.nih.gov/research-topics/trends-statistics/overdose-death-rates#Fig3 (accessed on 2 January 2025).
- Ling, W.; Mooney, L.; Torrington, M. Buprenorphine for opioid addiction. Pain Manag. 2012, 2, 345–350. [Google Scholar] [CrossRef]
- Freed, M.E.; Potoski, J.R.; Freed, E.H.; Conklin, G.L.; Malis, J.M. Bridged aminotetralins as novel potent analgesic substances. J. Med. Chem. 1973, 16, 595–599. [Google Scholar] [CrossRef]
- Haffajee, R.; Mello, M.M. Drug companies’ liability for the opioid epidemic. N. Engl. J. Med. 2017, 377, 2301–2305. [Google Scholar] [CrossRef] [PubMed]
- Ye, R.-R.; Jiang, S.; Xu, X.; Lu, Y.; Wang, Y.-J.; Liu, J.-G. Dezocine as a potent analgesic: Overview of its pharmacological characterization. Acta. Pharmacol. Sin. 2022, 43, 1646–1657. [Google Scholar] [CrossRef]
- Zhang, Y.; Wu, W.; Li, Z.; Yang, G.; Fang, Y.; Zhang, T.; Gu, W.; Chen, S.; Wang, F.; Li, J. Dezocine Analog. WO2017118375A1, 13 July 2017. [Google Scholar]
- Rice, K.C.; Jacobson, A.E.; Li, F.; Gutman, E.S.; Bow, E.W. Biased Potent Opioid-Like Agonists as Improved Medications to Treat Chronic and Acute Pain and Methods of Using the Same. WO2019183950A1, 26 September 2019. [Google Scholar]
- Shao, L.; Hu, T.; Xu, H.; Chen, L.; Zou, Y.; Cai, W.; Yang, X.; Li, H.; Xue, D. Dezocine Derivative and Medical Use Thereof. WO2020165522A1, 6 August 2020. [Google Scholar]
- Yao, S.; Zhang, L.; An, R.; Sun, C.; Lu, S.; Lyu, H.; Li, H.; Li, B.; Luo, H.; Zhu, X. Opioid Compound as Well as Preparation Method and Application Thereof. CN115124435A, 30 September 2022. [Google Scholar]
- Childers, W.E.; Abou-Gharbia, M.A. “I’ll be back”: The resurrection of dezocine. ACS Med. Chem. Lett. 2021, 12, 961–969. [Google Scholar] [CrossRef]
- Grothusen, J. Dezocine: A totally different opioid. Transl. Perioper. Pain Med. 2022, 9, 430–433. [Google Scholar]
- Want, Y.-H.; Chai, J.-R.; Xu, X.-J.; Ye, R.-F.; Zan, G.-Y.; Liu, G.Y.-K.; Long, J.-D.; Ma, Y.; Huang, X.; Xaio, Z.-C.; et al. Pharmacological characterization of dezocine, a potent analgesic acting as a κ partial agonist and μ partial agonist. Sci. Rep. 2018, 8, 14087. [Google Scholar]
- Li, N.N.; Huang, Y.Q.; Huang, L.E.; Guo, S.H.; Shen, M.R.; Guo, C.L.; Zhu, S.M.; Yao, Y.X. Dezocine antagonizes morphine analgesia upon simultaneous administration in rodent models of acute nociception. Pain Physician 2017, 20, E401–E409. [Google Scholar] [PubMed]
- Hoskin, P.J.; Hanks, G.W. Opioid agonist-antagonist drugs in acute and chronic pain states. Drugs 1991, 41, 326–344. [Google Scholar] [CrossRef]
- Stahl, E.L.; Bohn, L.M. Low intrinsic efficacy alone cannot explain the improved side effect profiles of new opioid agonists. Biochem. 2022, 61, 1923–1935. [Google Scholar] [CrossRef] [PubMed]
- Che, T.; Dwivedi-Agnihotri, H.; Shukla, A.K.; Roth, B.L. Biased ligands at opioid receptors: Current status and future directions. Sci. Signal. 2021, 14, eaac0320. [Google Scholar] [CrossRef]
- Jean-Charles, P.Y.; Kaur, S.; Shenoy, S.K. GPCR signaing via β-arrestin-dependent mechanisms. J. Cardiovasc. Pharmacol. 2017, 70, 142–158. [Google Scholar] [CrossRef] [PubMed]
- Auo, A. The role of opioid receptor internalization and β-arrestins in the development of opioid tolerance. Anesth. Analg. 2005, 101, 728–734. [Google Scholar]
- Raehal, K.M.; Bohn, L.M. β-Arrestins: Regulatory role and therapeutic potential in opioid and cannabinoid receptor-mediated analgesia. Handb. Exp. Pharmacol. 2014, 219, 427–443. [Google Scholar]
- Gillis, A.; Kliewer, A.; Kelly, E.; Henderson, G.; Christie, M.J.; Schulz, S.; Canals, M. Critical assessment of G-protein-biased agonism at the μ-opioid receptor. Trends Pharmacol. Sci. 2020, 12, 947–959. [Google Scholar] [CrossRef]
- Madariaga-Mazon, A.; Marmolejo-Valencia, A.F.; Li, Y.; Toll, L.; Houghten, R.A.; Martinez-Mayorga, K. Mu-opioid receptor biased ligands: A safer and painless discovery of analgesics? Drug Disc. Today 2017, 22, 1719–1729. [Google Scholar] [CrossRef]
- Grothusen, J.; Lin, W.; Xi, J.; Zanni, G.; Rarr, G.A.; Liu, R. Dezocine is a biased ligand without significant beta-arrestin activation of the mu opioid receptor. Transl. Perioper. Pain Med. 2022, 9, 424–439. [Google Scholar]
- Malis, J.L.; Rosenthale, M.E.; Gluckman, M.I. Animal pharmacology of WY-16,225, a new analgesic agent. J. Pharmacol. Exp. Ther. 1975, 194, 488–498. [Google Scholar] [CrossRef] [PubMed]
- O’Brian, J.J.; Benfield, P. Dezocine: A preliminary review of its pharmacodynamics and pharmacokinetic properties, and therapeutic efficacy. Drugs 1989, 38, 226–248. [Google Scholar] [CrossRef] [PubMed]
- Gal, T.J.; DiFazio, C.A. Ventilatory and analgesic effects of dezocine in humans. Anesthesiology 1984, 61, 716–722. [Google Scholar] [CrossRef]
- Yang, H.; Shen, R.; Zhan, F.-F.; Shao, J.-L.; Lu, Y.-J.; Wang, L. Effects of dezocine combined with dexmedetomidine on adverse reactions and inflammatory factors in patients undergoing HIPEC after intestinal surgery and its protective effect on the heart in the perioperative period. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 3437–3443. [Google Scholar]
- Faouzi, A.; Varga, B.R.; Majumdar, S. Biased opioid ligands. Molecules 2020, 25, 4257. [Google Scholar] [CrossRef] [PubMed]
- Kise, R.; Inoue, A. GPCR signaling bias: An emerging framework for opioid drug development. J. Biochem. 2024, 175, 367–376. [Google Scholar] [CrossRef]
- Conibear, A.E.; Kelly, E. A biased view of μ-opioid receptors? Mol. Pharmacol. 2019, 96, 542–549. [Google Scholar] [CrossRef]
- Olinvyk Package Insert. Drugs.com. Available online: https://www.drugs.com/pro/olinvyk.html#LINK_21f3751b-1f8d-42ff-94bb-b723545069b7 (accessed on 2 January 2025).
- Liu, R.; Huang, X.P.; Yeliseer, A.; Xi, J. Novel molecular targets of dezocine and their clinical implications. Anesthesiology 2014, 120, 714–723. [Google Scholar] [CrossRef]
- Coleman, J.A.; Gureaux, E. Structural basis for recognition of diverse antidepressants by the human serotonin transporter. Nat. Struct. Mol. Biol. 2018, 25, 170–175. [Google Scholar] [CrossRef]
- Song, A.L.; Wu, X.D. Mechanistic insights of substrate transport and inhibitor binding revealed by high-resolution structures of human epinephrine transporter. Cell Res. 2024, 34, 810–813. [Google Scholar] [CrossRef] [PubMed]
- Pertovaarda, A. Noradrenergic pain modulation. Prog. Neurobiol. 2006, 80, 53–83. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.X.; Mao, X.F.; Li, F.F.; Gong, N.; Zhang, M.A. Dexocine exhibits antihypersensitivity activities in neuropathy through spinal mu-opioid receptor activation and norepinephrine reuptake inhibition. Sci. Rep. 2017, 7, 43137. [Google Scholar]
- Mao, X.F.; Ahsan, M.Z.; Apryani, E.; Tang, X.Q.; Zhao, M.J.; Li, X.Y. Dual mu-opioid receptor and norepinephrine reuptake mechanisms contribute to dezocine- and tapenfadol-induced mechanical antiallodynia in cancer pain. Eur. J. Pharmacol. 2020, 876, 173062. [Google Scholar] [CrossRef]
- Fu, B.; Jiang, J.; Huang, Y. The analgesic effects of dezocine in rats with chronic constriction injuries. Exp. Anim. 2023, 72, 496–504. [Google Scholar] [CrossRef]
- Wu, F.X.; Pan, R.R.; Yu, W.F.; Liu, R. The anti-nociception effect of dezocine in a rat neuropathic pain model. Transl. Perioper. Pain Med. 2014, 1, 5–8. [Google Scholar]
- Ahzan, M.Z.; Zhao, M.J.; Shoaib, R.M.; Zhang, Y.; Wang, Y.X. Comparative study of dezocine, pentazocine and tapentadol on antinociception and physical dependence. Life Sci. 2021, 285, 119996. [Google Scholar] [CrossRef]
- Ding, Y.; White, P.F. Comparative effects of ketodolac, dezocine and fentanyl as adjuvants during outpatient anesthesia. Anesth. Analg. 1992, 75, 566–571. [Google Scholar] [CrossRef]
- Huang, R.; Jiang, L.; Cao, Y.; Liu, H.; Ping, M.; Li, W.; Xu, Y.; Ning, J.; Chen, Y.; Wang, X. Comparative Efficacy of therapeutics for chronic cancer pain: A Bayesian network meta-analysis. J. Clin. Oncol. 2019, 37, 1742–1752. [Google Scholar] [CrossRef]
- Stambaugh, J.E., Jr.; McAdams, J. Comparison in intramuscular dezocine with butorphanol and placebo in chronic cancer pain: A method to evaluate analgesia after both single and repeated doses. Clin. Parmacol. Ther. 1987, 42, 210–219. [Google Scholar] [CrossRef]
- Gong, W.Y.; Xu, B.; Liu, L.; Li, S.T. Dezocine relieves the postoperative hyperalgesia in rats through suppressing the hyper-action of Akt1/GSK-3β pathway. Exp. Brain Res. 2022, 240, 1435–1444. [Google Scholar] [CrossRef] [PubMed]
- Vazquez-Leon, P.; Miranda-Paez, A.; Valencia-Flores, K.; Sanchez-Cstillo, H. Defensive and emotional behavior modulation by serotonin in the eriaqueductal gray. Cell Mol. Neurobiol. 2023, 43, 1453–1468. [Google Scholar] [CrossRef]
- Shang, L.; Duan, C.; Chang, S.; Chang, N.; Jia, S. Antidepressant-like effects of dezocine in mice: Involvement of 5-HT1A and κ-opioid receptors. Behav. Pharmacol. 2021, 32, 472–478. [Google Scholar] [CrossRef]
- Wang, H.; Lyu, N.; Zhao, Q. Case report: Dezocine’s rapid and sustained antidepressant effects. Front. Pharmacol. 2024, 15, 1411119. [Google Scholar] [CrossRef]
- Wong, S.; Le, G.H.; Vasudeva, S.; Teopiz, K.M.; Phan, L.; Meshkat, S.; Kwan, A.T.H.; Rhee, T.G.; Ho, R.; Choi, H.; et al. Preclinical and clinical efficacy of kappa opioid receptor antagonists for depression: A systematic review. J. Affect. Disord. 2024, 362, 816–827. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Lu, Y.; Jia, M.; Bai, Y.; Sun, L.; Dong, Z.; Tian, W.; Yin, F.; Sei, S.; Wang, Y. Kappa opioid receptor in nucleus accumbens regulates depressive-like behaviors following prolonged morphine withdrawal in mice. iScience 2023, 26, 107536. [Google Scholar] [CrossRef]
- Gowing, L.; Farrell, M.; Ali, R.; White, J.M. Alphs2-adrenergic agonists for the management of opioid withdrawal. Cochrane Database Syst. Rev. 2016, 5, CD002024. [Google Scholar]
- Grothusen, J.R.; Blendy, J.A.; Barr, G.A. A brief overview of the neuropharmacology of opioid addiction. Transl. Perioper. Pain Med. 2022, 9, 491–496. [Google Scholar] [PubMed]
- Barr, G.A.; Schmidt, H.D.; Thakrar, A.P.; Kranzler, H.R.; Liu, R. Revisiting dezocine for opioid use disorder: A narrative review of its potential abuse liability. CNS Neurisci. Ther. 2024, 30, e70034. [Google Scholar] [CrossRef]
- Jasinski, D.R.; Preston, K.L. Assessment of dezocine for morphine-like subjective effects and miosis. Clin. Pharmacol. Ther. 1985, 38, 544–548. [Google Scholar] [CrossRef]
- Wu, X.; Zhang, Y.; Zeng, J.; Fei, Y. Clinical analysis of 8 drugs dependence with dezocine. Clin. J. Drug Depend. 2020, 29, 474–475. [Google Scholar]
- Shen, Q.; Zhang, L. Analysis of a case of addiction caused by dezocine injection in a patient with human immunodeficiency virus infection. Chin. Pharmacovigil. 2023, 20, 1181–1183. [Google Scholar]
- Holtzman, S.G. Drug discrimination studies. Drug Alcohol Depend. 1985, 14, 263–282. [Google Scholar] [CrossRef] [PubMed]
- Young, A.M.; Stephens, K.R.; Hein, D.W.; Woods, J.H. Reinforcing and discriminative stimulus properties of mixed agonist-antagonist opioids. J. Pharmacol. Exp. Ther. 1984, 229, 118–126. [Google Scholar] [CrossRef]
- Schaefer, G.J.; Holtzman, S.G. Morphine-like stimulus effects in the monkey: Opioids with antagonist properties. Pharmacol. Biochem. Behav. 1981, 14, 241–245. [Google Scholar] [CrossRef] [PubMed]
- Picker, M.J. Discriminative stimulus effects of the mixed-opioid agonist/antagonist dezocine: Cross-substitution by mu and delta opioid agonists. J. Pharmacol. Exp. Ther. 1997, 283, 1009–1017. [Google Scholar] [CrossRef] [PubMed]
- Banks, M.L. The rise and fall of kappa-opioid receptors in drug abuse research. In Substance Use Disorders, From Etology to Treatment. Handbook of Experimental Pharmacology; Nader, M., Hurd, Y., Eds.; Springer Nature: Bern, Switzerland, 2019; Volume 258, pp. 147–166. [Google Scholar]
- Porter-Stransky, K.A.; Weinshenker, D. Arresting the development of addiction: The role of β-arrestin 2 in drug abuse. J. Pharmacol. Exp. Ther. 2017, 361, 341–348. [Google Scholar] [CrossRef]
- Wise, R.A.; Robbie, M.A. Dopamine and addiction. Ann. Rev. Psychol. 2020, 71, 79–106. [Google Scholar] [CrossRef]
- Liu, R.; Milas, B.; Grothusen, J. Non-scheduled short-acting opioid to taper off opioids? CNS Neurosci. Ther. 2024, 30, e14705. [Google Scholar] [CrossRef]
- Wu, F.X.; Babazada, H.; Gao, H.; Huang, X.P.; Xi, C.H.; Chen, C.H.; Xi, J.; Yu, W.F.; Liu, R. Dezocine alleviates morphine-induced dependence in rats. Anesth. Analg. 2019, 128, 1328–1335. [Google Scholar] [CrossRef]
- Pdergolizzi, J.V., Jr.; Raffa, R.B.; Rosenblatt, M.H. Opioid withdrawal symptoms, a consequence of chronic opioid use and opioid use disorder: Current understanding and approaches to management. J. Clin. Pharm. Ther. 2020, 45, 892–903. [Google Scholar] [CrossRef] [PubMed]
- Zhao, P.; Wu, Z.; Li, C.; Yang, G.; Ding, J.; Wang, K.; Wang, M.; Feng, L.; Duan, G.; Li, H. Postoperative analgesia using dezocine alleviates depressive symptoms after colorectal cancer surgery: A randomized controlled, double-blind trial. PLoS ONE 2020, 15, e0233412. [Google Scholar] [CrossRef] [PubMed]
- Hu, X.D.; Yang, K.; Wen, X. Dezocine can alleviate depression of breast cancer. Int. J. Clin. Stud. Med. Case Rep. 2023, 33, 003. [Google Scholar] [CrossRef]
- Foster, S.L.; Weinshanker, D. The role of norepinephrine in drug addiction: Past, present, and future. In Neural Mechanisms of Addiction; Torregrossa, M., Ed.; Elsevier: Amsterdam, The Netherland, 2018; pp. 221–236. [Google Scholar]
- Schmidt, H.D.; Zhang, Y.; Xi, J.; Zanni, G.; Liu, R.; Barr, G.A. A new formulation of dezocine, Cyc-dezocine, reduces oxycodone self-administration in female and male rats. Neurosci. Lett. 2023, 815, 137479. [Google Scholar] [CrossRef]
- Pandey, S.P.; Shukla, T.; Dhote, V.K.; Mishra, D.K.; Maheshwari, R.; Tekade, R.K. Use of Polymers in Controlled Release of Active Agents. In Basic Fundamentals of Drug Delivery; Tekade, R.K., Ed.; Academic Press: London, UK, 2019; Chapter 4; pp. 113–172. [Google Scholar]
- Liu, R.; Abou-Gharbia, M.; Cao, H.; Chen, X.; Fleisher, L.A.; Hasan, A.; Huang, Y.; Li, J.; Liu, H.; Ma, H.; et al. 2024 US-China round table consensus discussion on perioperative opioid management. Transl. Perioper Pain Med. 2024, 11, 683–686. [Google Scholar]
- Ozdemir, E.; Gursoy, S.; Bagcivan, I. The effects of serotonin/norepinephrine reuptake inhibitors and serotonin receptor agonist on morphine analgesia and tolerance in rats. J. Physio. Sci. 2012, 62, 317–323. [Google Scholar] [CrossRef]
- Smith, B.H.; Higgins, C.; Baldacchino, A.; Kidd, B.; Bannister, J. Substance misuse of gabapentin. Br. J. Gen. Pract. 2012, 62, 406–407. [Google Scholar] [CrossRef]
- Kingwell, K. Nav1.8 inhibitor poised to provide opioid-free pain relief. Nat. Rev. Drug Disc. 2025, 24, 3–5. [Google Scholar] [CrossRef]
- Osteen, J.D.; Immani, S.; Tapley, T.L.; Indersmitten, T.; Hurst, N.W.; Healey, T.; Aertgeerts, K.; Negulescu, P.A.; Lechner, S.M. Pharmacology and mechanism of action of suzetrigine, a potent and selective Nav1.8 pain signal inhibitor for the treatment of moderate to severe pain. Pain Ther. 2025. published online ahead of print. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patent/Application Number | Original Publication Date | Title | Assignee |
|---|---|---|---|
| CN101671269 | 17 March 2010 | Preparation method of substituted methylene benzocyclodecene ketoxime | Yangtze River Pharmaceutical Group Co., Ltd., Shanghai, China |
| CN102503840 | 20 June 2012 | Preparation method of dezocine | Yangtze River Pharmaceutical Group Co., Ltd., Shanghai, China |
| CN104910002 | 16 September 2015 | Dezocine key intermediate preparation method | Wenzhou Medical University |
| CN107337609/ WO2018214877 | 10 November 2017 | A dezocine crystal form and a preparing method thereof | Yangtze River Pharmaceutical Group Co., Ltd., Shanghai, China |
| CN107522625 | 29 December 2017 | Crystal form of dezocine and preparation method therefor | Yangtze River Pharmaceutical Group Co., Ltd., Shanghai, China |
| CN107778187 | 9 March 2018 | Dezocine crystal form A and preparation method thereof | Jiangsu Nhwa Pharmaceutical Co., Ltd., Nanjing, China |
| CN108299173/ WO2018214877 | 20 July 2018 | Asymmetric synthesis method of dezocine key intermediate | Yangtze River Pharmaceutical Group Co., Ltd., Shanghai, China |
| CN110283085 | 27 September 2019 | Dezocine production process | DR Double Crane Limin Pharamceutical Jinan Co., Ltd., Jinan, China |
| CN113896621 | 7 January 2022 | Asymmetric synthesis method of dezocine key intermediate | Ningbo Zejun Pharmaceutical Tech Co., Ltd., Ningbo, China |
| CN113979875/ WO2022022388 | 28 January 2022 | Dexocine derivative crystal form A as well as preparation method and application thereof | Yangtze River Pharmaceutical Group Co., Ltd., Shanghai, China |
| CN114380702 | 22 April 2022 | Separation and purification method of dezocine | Taizhou Danding Biotechnology Co., Ltd., Taizhou, China |
| CN115043742 | 13 September 2022 | Preparation method of dezocine | Nanjing Damei Biological Pharmaceutical Co., Ltd., Nanijng, China |
| Patent/Application Number | Original Publication Date | Title | Assignee |
|---|---|---|---|
| Inventions addressing improved non-intravenous administration | |||
| WO2009032246 | 12 March 2009 | Compositions and methods for the delivery of poorly soluble drugs | Nanotherapeutics Inc., Alachua, FL, USA |
| CN104622791 | 20 May 2015 | Dezocine oral preparation | Yangtze River Pharmaceutical Group Co., Ltd., Shanghai, China |
| WO2016157509 | 15 October 2015 | Compositions and methos for treating opioid receptor associated diseases | University of Pennsylvania, Philadelphia, PA, USA |
| CN108210933/ WO2018113581 | 28 June 2018 | Conjugate of dezocine and polyethylene glycol | Jenkem Technology Co., Ltd., Shanghai, China |
| CN113679659 | 23 November 2021 | Dezocine in-situ gel composition and application thereof | Yangtze River Pharmaceutical Group Co., Ltd., Shanghai, China |
| WO2020008370A1 | 9 January 2020 | Transdermal patch | Clexio Biosciences Ltd., Yokneam, Israel |
| WO2020008366A1 | 9 January 2020 | Transdermal dosage form | Clexio Biosciences Ltd., Yokneam, Israel |
| CN108653446 | 16 October 2018 | Surface anesthesia medicine composition, microemulsion, as well as preparation method and application of microemulsion | West China Hospital, Sichuan University, Sichuan, China |
| CN108285423 | 17 July 2018 | Pain-easing active compound and medical application thereof | Taizhou Huayuan Medicine Technology Co., Ltd., Taizhou, China |
| Inventions addressing short duration of action (e.g., sustained release formulations, prodrugs) | |||
| CN11689549 | |||
| CN115770232 | 10 Marsh 2023 | Dezocine sustained release microsphere and preparation method thereof | Soochow University, Jiangsu, China |
| CN113730340 | 3 December 2021 | Fatty acid sustained-release composition for injection and preparation method and application thereof | China Pharmaceutical University, Jiangsu, China |
| CN110101865 | 9 August 2019 | Dezocine-containing medicine sustained-release preparation and preparation method thereof | Tianjin Third Central Hospital |
| CN110101660 | 9 August 2019 | Compound medicine sustained-release preparation containing dezocine and lidocaine and preparation method thereof | Tianjin Third Central Hospital, China |
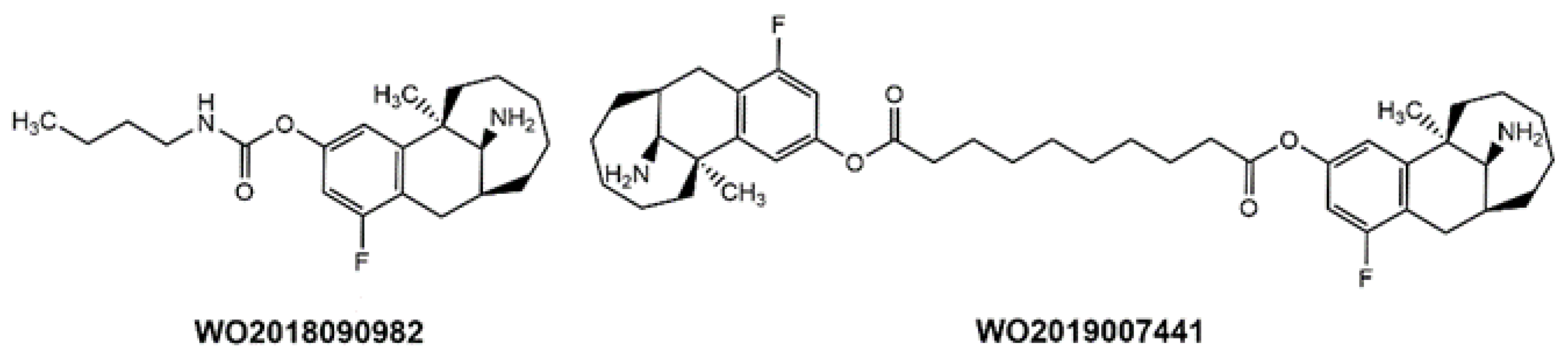
| WO2018090982 | 24 May 2018 | Preparation of benzodicycloalkane derivative as analgesics | Shanghai Haiyan Pharmaceutical Technology Co., Ltd., Shanghai, China |
| WO2019007443 | 10 January 2019 | Dezocine analogue ester-containing sustained-release suspension and preparation method thereof | Shandong Danhong Pharmaceutical Co., Ltd., Heze, China |
| WO2019007441 | 10 January 2019 | Sustained-release suspension containing dezocine analog ester and preparation method thereof | Shandong Danhong Pharmaceutical Co., Ltd., Heze, China |
| CN108704137 | 26 October 2018 | Opioid receptor partial agonist supported sustained release microsphere as well as preparation method and application thereof | Institute of Process Engineering, Chinese Academy of Sciences, China |
| WO2019007285A | 10 January 2019 | Crystal form and amorphous form of dezocine analogue hydrochloride | Shandong Danhong Pharmaceutical Co., Ltd., Heze, China |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Childers, W.; Elokely, K.; Abou-Gharbia, M. Dezocine and Addiction: Friend or Foe? Pharmaceuticals 2025, 18, 386. https://doi.org/10.3390/ph18030386
Childers W, Elokely K, Abou-Gharbia M. Dezocine and Addiction: Friend or Foe? Pharmaceuticals. 2025; 18(3):386. https://doi.org/10.3390/ph18030386
Chicago/Turabian StyleChilders, Wayne, Khaled Elokely, and Magid Abou-Gharbia. 2025. "Dezocine and Addiction: Friend or Foe?" Pharmaceuticals 18, no. 3: 386. https://doi.org/10.3390/ph18030386
APA StyleChilders, W., Elokely, K., & Abou-Gharbia, M. (2025). Dezocine and Addiction: Friend or Foe? Pharmaceuticals, 18(3), 386. https://doi.org/10.3390/ph18030386