
Dexmedetomidine as Adjunctive Therapy for the Treatment of Alcohol Withdrawal Syndrome: A Systematic Review and Meta-Analysis

 ,
,  ,
,  ,
,  , ,
, ,  , and
, and 
Abstract
1. Introduction
2. Results
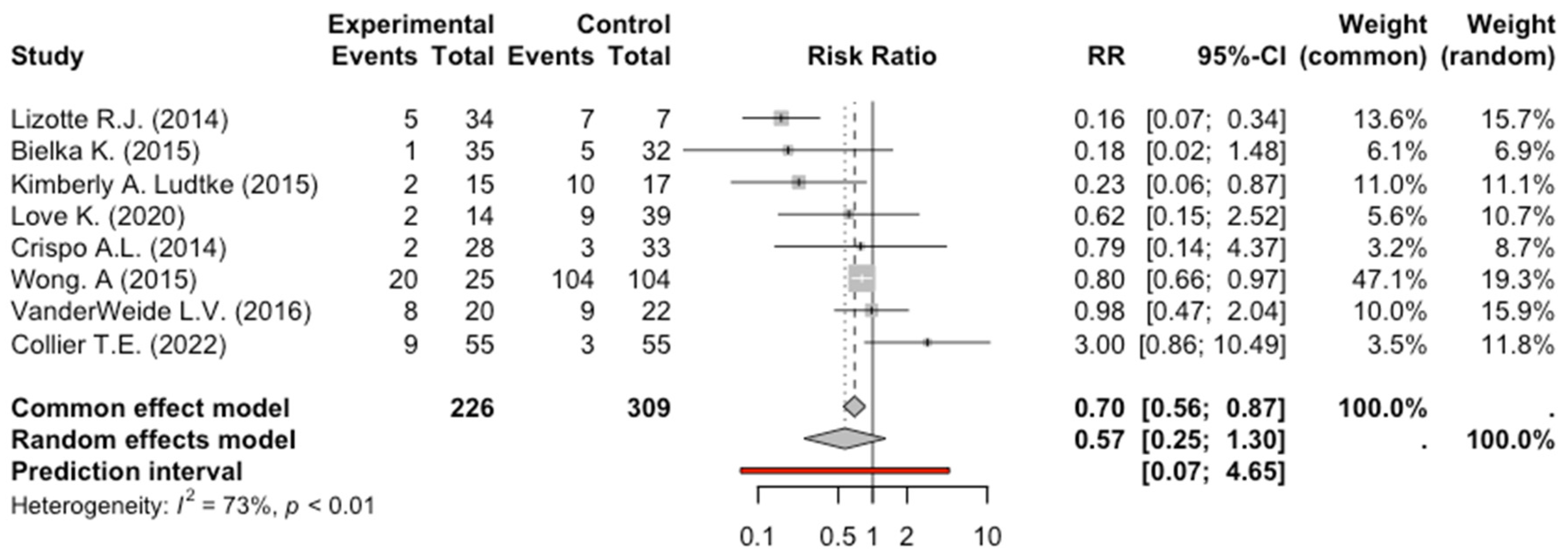
2.1. Primary Outcome (Tracheal Intubation)
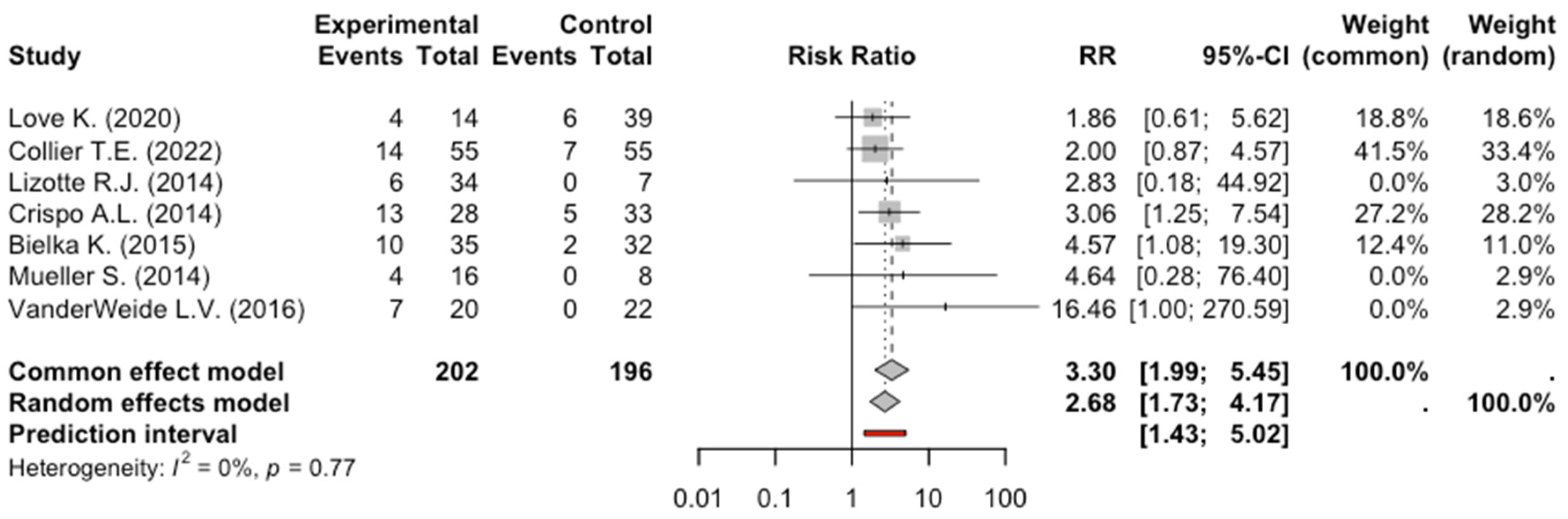
2.2. Secondary Outcome (Bradycardia)
2.3. Secondary Outcome (Hypotension)
3. Discussion
4. Methods
4.1. Study Search
4.2. Study Selection
4.3. Definition and Outcome
4.4. Data Extraction and Quality Assessment
4.5. Data Analysis
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Association, A.P. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2000. [Google Scholar] [CrossRef]
- Ganatra, R.B.; Breu, A.C.; Ronan, M.V. Clinical guideline highlights for the hospitalist: 2020 American Society of Addiction Medicine clinical practice guideline on alcohol withdrawal management. J. Hosp. Med. 2022, 17, 47–49. [Google Scholar] [CrossRef]
- Weerink, M.A.S.; Struys, M.M.R.F.; Hannivoort, L.N.; Barends, C.R.M.; Absalom, A.R.; Colin, P. Clinical Pharmacokinetics and Pharmacodynamics of Dexmedetomidine. Clin. Pharmacokinet. 2017, 56, 893–913. [Google Scholar] [CrossRef] [PubMed]
- Yuki, K. The immunomodulatory mechanism of dexmedetomidine. Int. Immunopharmacol. 2021, 97, 107709. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services (HHS); Substance Abuse and Mental Health Services Administration (SAMHSA); Center for Behavioral Health Statistics and Quality; Treatment Services Branch. Preliminary Findings from Drug-Related Emergency Department Visits. 2021. Available online: https://store.samhsa.gov/sites/default/files/PEP22-07-03-001.pdf (accessed on 16 April 2024).
- Peterson, C.; Li, M.; Xu, L.; Mikosz, C.A.; Luo, F. Assessment of Annual Cost of Substance Use Disorder in US Hospitals. JAMA Netw. Open 2021, 4, e210242. [Google Scholar] [CrossRef]
- Chang, D.W.; Shapiro, M.F. Association between Intensive Care Unit Utilization during Hospitalization and Costs, Use of Invasive Procedures, and Mortality. JAMA Intern. Med. 2016, 176, 1492–1499. [Google Scholar] [CrossRef]
- Harrer, M.; Cuijpers, P.; Furukawa, T.A.; Ebert, D.D. Doing Meta-Analysis with R: A Hands-On Guide, 1st ed.; Chapman & Hall/CRC Press: Boca Raton, FL, USA; London, UK, 2021. [Google Scholar]
- Crispo, A.L.; Daley, M.J.; Pepin, J.L.; Harford, P.H.; Brown, C.V. Comparison of clinical outcomes in nonintubated patients with severe alcohol withdrawal syndrome treated with continuous-infusion sedatives: Dexmedetomidine versus benzodiazepines. Pharmacotherapy 2014, 34, 910–917. [Google Scholar] [CrossRef] [PubMed]
- Bielka, K.; Kuchyn, I.; Glumcher, F. Addition of dexmedetomidine to benzodiazepines for patients with alcohol withdrawal syndrome in the intensive care unit: A randomized controlled study. Ann. Intensive Care 2015, 5, 33. [Google Scholar] [CrossRef] [PubMed]
- VanderWeide, L.A.; Foster, C.J.; MacLaren, R.; Kiser, T.H.; Fish, D.N.; Mueller, S.W. Evaluation of Early Dexmedetomidine Addition to the Standard of Care for Severe Alcohol Withdrawal in the ICU:A Retrospective Controlled Cohort Study. J. Intensive Care Med. 2016, 31, 198–204. [Google Scholar] [CrossRef]
- Lizotte, R.J.; Kappes, J.A.; Bartel, B.J.; Hayes, K.M.; Lesselyoung, V.L. Evaluating the effects of dexmedetomidine compared to propofol as adjunctive therapy in patients with alcohol withdrawal. Clin. Pharmacol. 2014, 6, 171–177. [Google Scholar] [CrossRef]
- Love, K.; Zimmermann, A.E. Use of Propofol Plus Dexmedetomidine in Patients Experiencing Severe Alcohol Withdrawal in the Intensive Care Unit. J. Clin. Pharmacol. 2020, 60, 439–443. [Google Scholar] [CrossRef]
- Collier, T.E.; Farrell, L.B.; Killian, A.D.; Kataria, V.K. Effect of Adjunctive Dexmedetomidine in the Treatment of Alcohol Withdrawal Compared to Benzodiazepine Symptom-Triggered Therapy in Critically Ill Patients: The EvADE Study. J. Pharm. Pract. 2022, 35, 356–362. [Google Scholar] [CrossRef] [PubMed]
- Mueller, S.W.; Preslaski, C.R.; Kiser, T.H.; Fish, D.N.; Lavelle, J.C.; Malkoski, S.P.; MacLaren, R. A randomized, double-blind, placebo-controlled dose range study of dexmedetomidine as adjunctive therapy for alcohol withdrawal. Crit. Care Med. 2014, 42, 1131–1139. [Google Scholar] [CrossRef]
- Ludtke, K.A.; Stanley, K.S.; Yount, N.L.; Gerkin, R.D. Retrospective Review of Critically Ill Patients Experiencing Alcohol Withdrawal: Dexmedetomidine Versus Propofol and/or Lorazepam Continuous Infusions. Hosp. Pharm. 2015, 50, 208–213. [Google Scholar] [CrossRef]
- Wong, A.; Benedict, N.J.; Kane-Gill, S.L. Multicenter evaluation of pharmacologic management and outcomes associated with severe resistant alcohol withdrawal. J. Crit. Care 2015, 30, 405–409. [Google Scholar] [CrossRef]
- Riihioja, P.; Jaatinen, P.; Oksanen, H.; Haapalinna, A.; Heinonen, E.; Hervonen, A. Dexmedetomidine, diazepam, and propranolol in the treatment of ethanol withdrawal symptoms in the rat. Alcohol. Clin. Exp. Res. 1997, 21, 804–808. [Google Scholar] [CrossRef] [PubMed]
- Rovasalo, A.; Tohmo, H.; Aantaa, R.; Kettunen, E.; Palojoki, R. Dexmedetomidine as an adjuvant in the treatment of alcohol withdrawal delirium: A case report. Gen. Hosp. Psychiatry 2006, 28, 362–363. [Google Scholar] [CrossRef]
- DeMuro, J.P.; Botros, D.G.; Wirkowski, E.; Hanna, A.F. Use of dexmedetomidine for the treatment of alcohol withdrawal syndrome in critically ill patients: A retrospective case series. J. Anesth. 2012, 26, 601–605. [Google Scholar] [CrossRef] [PubMed]
- Rayner, S.G.; Weinert, C.R.; Peng, H.; Jepsen, S.; Broccard, A.F. Dexmedetomidine as adjunct treatment for severe alcohol withdrawal in the ICU. Ann. Intensive Care 2012, 2, 12. [Google Scholar] [CrossRef]
- Frazee, E.N.; Personett, H.A.; Leung, J.G.; Nelson, S.; Dierkhising, R.A.; Bauer, P.R. Influence of dexmedetomidine therapy on the management of severe alcohol withdrawal syndrome in critically ill patients. J. Crit. Care 2014, 29, 298–302. [Google Scholar] [CrossRef]
- Polintan, E.T.T.; Danganan, L.M.L.; Cruz, N.S.; Macapagal, S.C.; Catahay, J.A.; Patarroyo-Aponte, G.; Azmaiparashvili, Z.; Lo, K.B. Adjunctive Dexmedetomidine in Alcohol Withdrawal Syndrome: A Systematic Review and Meta-analysis of Retrospective Cohort Studies and Randomized Controlled Trials. Ann. Pharmacother. 2022, 57, 696–705. [Google Scholar] [CrossRef]
- Fiore, M.; Torretta, G.; Passavanti, M.B.; Sansone, P.; Pace, M.C.; Alfieri, A.; Aurilio, C.; Simeon, V.; Chiodini, P.; Pota, V. Dexmedetomidine as adjunctive therapy for the treatment of alcohol withdrawal syndrome: A systematic review protocol. JBI Database Syst. Rev. Implement. Rep. 2019, 17, 2159–2164. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Wells, G.A.; Shea, B.; O’Connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses; Ottawa Hospital Research Institute: Ottawa, ON, USA, 2000. [Google Scholar]
- Mantel, N.; Haenszel, W. Statistical aspects of the analysis of data from retrospective studies of disease. J. Natl. Cancer Inst. 1959, 22, 719–748. [Google Scholar]
- Hedges, L.V.; Vevea, J.L. Estimating Effect Size under Publication Bias: Small Sample Properties and Robustness of a Random Effects Selection Model. J. Educ. Behav. Stat. 1996, 21, 299–332. [Google Scholar] [CrossRef]
- Paule, R.C.; Mandel, J. Consensus Values and Weighting Factors. J. Res. Natl. Bur. Stand. 1982, 87, 377–385. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Published Year) [Ref.] | Setting | Study Design | Control Group | Time Spam | N. Patients | Outcome(s) |
|---|---|---|---|---|---|---|
| Crispo, A.L. (2014) [9] | ED | RC | BZD | 2011–2012 | 122 | TI + B + H |
| Bielka, K. (2015) [10] | ED | RCT | BZD | NS | 134 | TI + B + H |
| VanderWeide, L.A. (2016) [11] | Mixed | RC | BZD | 2008–2012 | 84 | TI + B + H |
| Lizotte, R.J. (2014) [12] | ED | RC | BZD + P | 2010–2013 | 82 | TI + B + H |
| Love, K. (2020) [13] | ICU | RC | BZD + P | 2015–2018 | 53 | TI + B + H |
| Collier, T.E. (2022) [14] | ICU | RC | BZD | 2015–2018 | 110 | TI + B |
| Mueller, S. (2014) [15] | ED | RCT | BZD | 2009–2012 | 48 | B + H |
| Ludtke, K.A. (2015) [16] | ED | RC | BZD + P | 2002–2009 | 64 | TI |
| Wong, A. (2015) [17] | Mixed | RC | BZD + P | 2009–2012 | 258 | TI |
| Study | Ref. | R | D | Mi | Me | S | O |
|---|---|---|---|---|---|---|---|
| Bielka, K. | [10] | + | − | + | + | + | + |
| Mueller, S. | [15] | + | + | − | + | + | + |
| Study | Ref. | Selection | Comparability | Outcome |
|---|---|---|---|---|
| Crispo, A.L. | [9] | *** | * | *** |
| Lizotte, R.J. | [12] | *** | ** | ** |
| VanderWeide, L.A. | [11] | ** | * | ** |
| Ludtke, K.A. | [16] | *** | * | *** |
| Wong, A. | [17] | *** | ** | *** |
| Love, K. | [13] | *** | ** | *** |
| Collier, T.E. | [14] | *** | ** | ** |
| Participants | Intervention | Comparison | Outcomes | Study Design |
|---|---|---|---|---|
| Adult patients in any setting with alcohol withdrawal syndrome | Dexmedetomidine as adjunctive therapy to standard of care | Standard of care | Primary outcomes: Tracheal intubation Secondary outcomes: (a) Hypotension (b) Bradycardia | Randomized controlled trials and observational studies (including cohort and case-control studies) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiore, M.; Alfieri, A.; Torretta, G.; Passavanti, M.B.; Sansone, P.; Pota, V.; Simeon, V.; Chiodini, P.; Corrente, A.; Pace, M.C. Dexmedetomidine as Adjunctive Therapy for the Treatment of Alcohol Withdrawal Syndrome: A Systematic Review and Meta-Analysis. Pharmaceuticals 2024, 17, 1125. https://doi.org/10.3390/ph17091125
Fiore M, Alfieri A, Torretta G, Passavanti MB, Sansone P, Pota V, Simeon V, Chiodini P, Corrente A, Pace MC. Dexmedetomidine as Adjunctive Therapy for the Treatment of Alcohol Withdrawal Syndrome: A Systematic Review and Meta-Analysis. Pharmaceuticals. 2024; 17(9):1125. https://doi.org/10.3390/ph17091125
Chicago/Turabian StyleFiore, Marco, Aniello Alfieri, Giacomo Torretta, Maria Beatrice Passavanti, Pasquale Sansone, Vincenzo Pota, Vittorio Simeon, Paolo Chiodini, Antonio Corrente, and Maria Caterina Pace. 2024. "Dexmedetomidine as Adjunctive Therapy for the Treatment of Alcohol Withdrawal Syndrome: A Systematic Review and Meta-Analysis" Pharmaceuticals 17, no. 9: 1125. https://doi.org/10.3390/ph17091125
APA StyleFiore, M., Alfieri, A., Torretta, G., Passavanti, M. B., Sansone, P., Pota, V., Simeon, V., Chiodini, P., Corrente, A., & Pace, M. C. (2024). Dexmedetomidine as Adjunctive Therapy for the Treatment of Alcohol Withdrawal Syndrome: A Systematic Review and Meta-Analysis. Pharmaceuticals, 17(9), 1125. https://doi.org/10.3390/ph17091125