
Impact of Bivalirudin on Ischemia/Reperfusion Injury in Patients with Reperfused STEMI Assessed by Cardiac Magnetic Resonance

 ,
,
Abstract
1. Introduction
2. Results
2.1. Baseline Clinical Characteristics
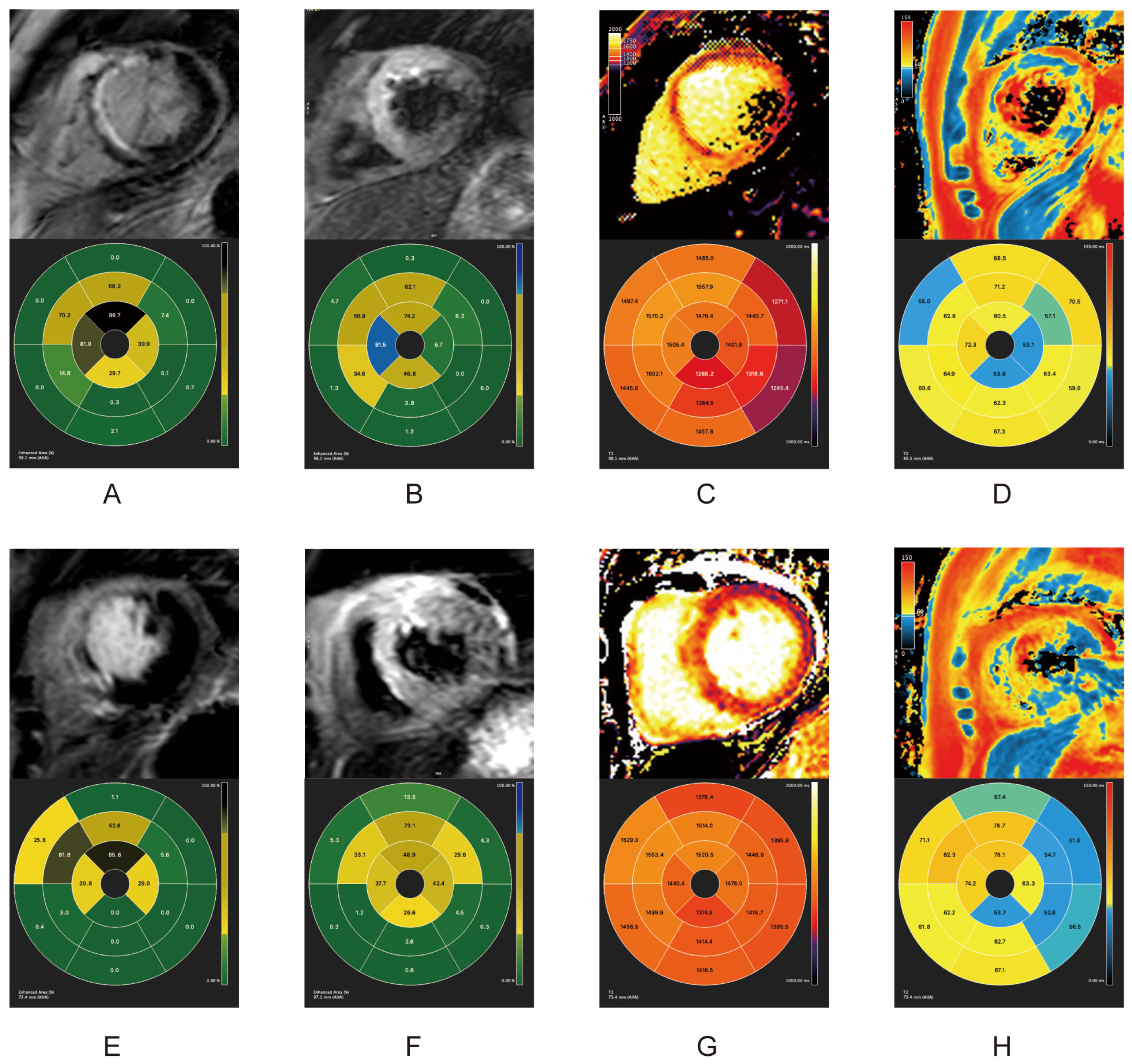
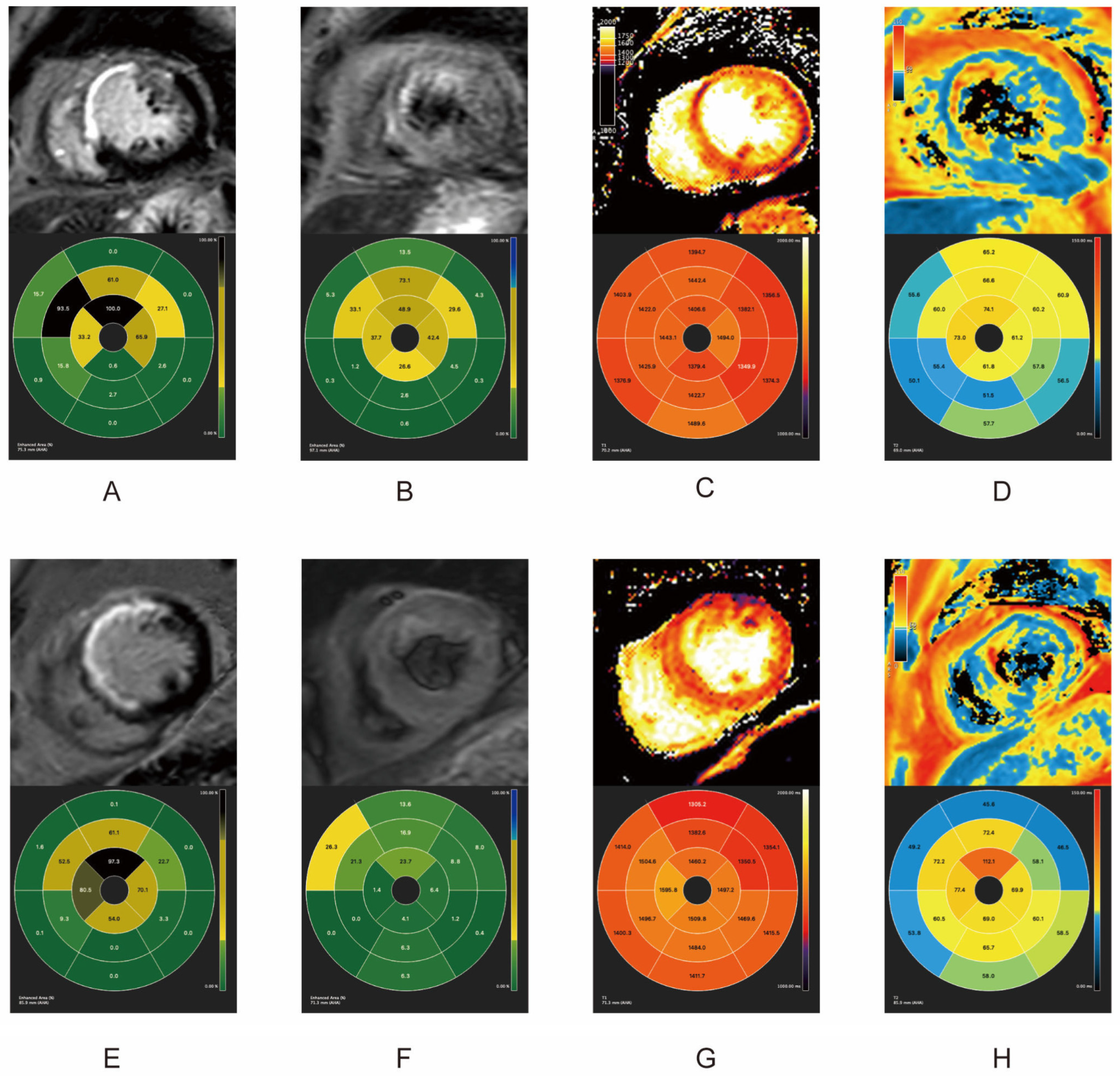
2.2. Quantitative and Qualitative Features of IRI in Acute Phase and Follow-Up
3. Discussion
4. Materials and Methods
4.1. Study Design and Subjects
4.2. Usage of Bivalirudin and UFH
4.3. CMR Protocols
4.4. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef]
- Levine, G.N.; Bates, E.R.; Blankenship, J.C.; Bailey, S.R.; Bittl, J.A.; Cercek, B.; Chambers, C.E.; Ellis, S.G.; Guyton, R.A.; Hollenberg, S.M.; et al. 2015 ACC/AHA/SCAI Focused Update on Primary Percutaneous Coronary Intervention for Patients With ST-Elevation Myocardial Infarction: An Update of the 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention and the 2013 ACCF/AHA Guideline for the Management of ST-Elevation Myocardial Infarction. J. Am. Coll. Cardiol. 2016, 67, 1235–1250. [Google Scholar] [CrossRef]
- Li, Y.; Liang, Z.; Qin, L.; Wang, M.; Wang, X.; Zhang, H.; Liu, Y.; Li, Y.; Jia, Z.; Liu, L.; et al. Bivalirudin plus a high-dose infusion versus heparin monotherapy in patients with ST-segment elevation myocardial infarction undergoing primary percutaneous coronary intervention: A randomised trial. Lancet 2022, 400, 1847–1857. [Google Scholar] [CrossRef]
- Mehran, R.; Lansky, A.J.; Witzenbichler, B.; Guagliumi, G.; Peruga, J.Z.; Brodie, B.R.; Dudek, D.; Kornowski, R.; Hartmann, F.; Gersh, B.J.; et al. Bivalirudin in patients undergoing primary angioplasty for acute myocardial infarction (HORIZONS-AMI): 1-year results of a randomised controlled trial. Lancet 2009, 374, 1149–1159. [Google Scholar] [CrossRef] [PubMed]
- Valgimigli, M.; Calabrò, P.; Cortese, B.; Frigoli, E.; Garducci, S.; Rubartelli, P.; Andò, G.; Santarelli, A.; Galli, M.; Garbo, R.; et al. Scientific foundation and possible implications for practice of the Minimizing Adverse Haemorrhagic Events by Transradial Access Site andSystemic Implementation of AngioX (MATRIX) trial. J. Cardiovasc. Transl. Res. 2014, 7, 101–111. [Google Scholar] [CrossRef] [PubMed]
- Capodanno, D.; Gargiulo, G.; Capranzano, P.; Mehran, R.; Tamburino, C.; Stone, G.W. Bivalirudin versus heparin with or without glycoprotein IIb/IIIa inhibitors in patients with STEMI undergoing primary PCI: An updated meta-analysis of 10,350 patients from five randomized clinical trials. Eur. Heart J. Acute Cardiovasc. Care 2016, 5, 253–262. [Google Scholar] [CrossRef] [PubMed]
- Chong, A.J.; Pohlman, T.H.; Hampton, C.R.; Shimamoto, A.; Mackman, N.; Verrier, E.D. Tissue factor and thrombin mediate myocardial ischemia-reperfusion injury. Ann. Thorac. Surg. 2003, 75, S649–S655. [Google Scholar] [CrossRef] [PubMed]
- Kamel, N.M.; El-Tanbouly, D.M.; Abdallah, D.M.; Sayed, H.M. PAR1, a therapeutic target for remote lung injury associated with hind limb ischemia/reperfusion: ERK5/KLF2-dependent lung capillary barrier preservation. Chem. Biol. Interact. 2022, 354, 109809. [Google Scholar] [CrossRef]
- Tuo, Q.Z.; Liu, Y.; Xiang, Z.; Yan, H.F.; Zou, T.; Shu, Y.; Ding, X.L.; Zou, J.J.; Xu, S.; Tang, F.; et al. Thrombin induces ACSL4-dependent ferroptosis during cerebral ischemia/reperfusion. Signal Transduct. Target. Ther. 2022, 7, 59. [Google Scholar] [CrossRef]
- Raivio, P.; Lassila, R.; Petäjä, J. Thrombin in myocardial ischemia-reperfusion during cardiac surgery. Ann. Thorac. Surg. 2009, 88, 318–325. [Google Scholar] [CrossRef]
- Yano, Y.; Ohmori, T.; Hoshide, S.; Madoiwa, S.; Yamamoto, K.; Katsuki, T.; Mitsuhashi, T.; Mimuro, J.; Shimada, K.; Kario, K.; et al. Determinants of thrombin generation, fibrinolytic activity, and endothelial dysfunction in patients on dual antiplatelet therapy: Involvement of factors other than platelet aggregability in Virchow’s triad. Eur. Heart J. 2008, 29, 1729–1738. [Google Scholar] [CrossRef][Green Version]
- Pan, H.; Lindon, A.; Grabau, R.; Dominguez, W.; Wickline, S. P3100Anti-thrombin nanoparticles limit ischemia-reperfusion injury and no-reflow in myocardial infarction. Eur. Heart J. 2019, 40, ehz745-0176. [Google Scholar] [CrossRef]
- Carswell, C.I.; Plosker, G.L. Bivalirudin: A review of its potential place in the management of acute coronary syndromes. Drugs 2002, 62, 841–870. [Google Scholar] [CrossRef]
- Mirabet, M.; Garcia-Dorado, D.; Ruiz-Meana, M.; Barrabés, J.A.; Soler-Soler, J. Thrombin increases cardiomyocyte acute cell death after ischemia and reperfusion. J. Mol. Cell Cardiol. 2005, 39, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Jormalainen, M.; Vento, A.E.; Lukkarinen, H.; Kääpä, P.; Kytö, V.; Lauronen, J.; Paavonen, T.; Suojaranta-Ylinen, R.; Petäjä, J. Inhibition of thrombin during reperfusion improves immediate postischemic myocardial function and modulates apoptosis in a porcine model of cardiopulmonary bypass. J. Cardiothorac. Vasc. Anesth. 2007, 21, 224–231. [Google Scholar] [CrossRef] [PubMed]
- Ye, H.; Zhang, Y.; Huang, Y.; Li, B.; Cao, R.; Dai, L.; Huang, B.; Tian, P.; Li, L.; Han, Y. Bivalirudin Attenuates Thrombin-Induced Endothelial Hyperpermeability via S1P/S1PR2 Category: Original Articles. Front. Pharmacol. 2021, 12, 721200. [Google Scholar] [CrossRef] [PubMed]
- Carrick, D.; Haig, C.; Rauhalammi, S.; Ahmed, N.; Mordi, I.; McEntegart, M.; Petrie, M.C.; Eteiba, H.; Hood, S.; Watkins, S.; et al. Prognostic significance of infarct core pathology revealed by quantitative non-contrast in comparison with contrast cardiac magnetic resonance imaging in reperfused ST-elevation myocardial infarction survivors. Eur. Heart J. 2016, 37, 1044–1059. [Google Scholar] [CrossRef] [PubMed]
- Erlich, J.H.; Boyle, E.M.; Labriola, J.; Kovacich, J.C.; Santucci, R.A.; Fearns, C.; Morgan, E.N.; Yun, W.; Luther, T.; Kojikawa, O.; et al. Inhibition of the tissue factor-thrombin pathway limits infarct size after myocardial ischemia-reperfusion injury by reducing inflammation. Am. J. Pathol. 2000, 157, 1849–1862. [Google Scholar] [CrossRef] [PubMed]
- Vargas, I.; Stephenson, D.J.; Baldwin, M.; Gaut, J.P.; Chalfant, C.E.; Pan, H.; Wickline, S.A. Sustained local inhibition of thrombin preserves renal microarchitecture and function after onset of acute kidney injury. Nanomedicine 2021, 38, 102449. [Google Scholar] [CrossRef] [PubMed]
- Vargas, I.; Grabau, R.P.; Chen, J.; Weinheimer, C.; Kovacs, A.; Dominguez-Viqueira, W.; Mitchell, A.; Wickline, S.A.; Pan, H. Simultaneous Inhibition of Thrombosis and Inflammation Is Beneficial in Treating Acute Myocardial Infarction. Int. J. Mol. Sci. 2023, 24, 7333. [Google Scholar] [CrossRef]
- Namachivayam, K.; MohanKumar, K.; Shores, D.R.; Jain, S.K.; Fundora, J.; Everett, A.D.; He, L.; Pan, H.; Wickline, S.A.; Maheshwari, A. Targeted inhibition of thrombin attenuates murine neonatal necrotizing enterocolitis. Proc. Natl. Acad. Sci. USA 2020, 117, 10958–10969. [Google Scholar] [CrossRef] [PubMed]
- Ugander, M.; Bagi, P.S.; Oki, A.J.; Chen, B.; Hsu, L.Y.; Aletras, A.H.; Shah, S.; Greiser, A.; Kellman, P.; Arai, A.E. Myocardial edema as detected by pre-contrast T1 and T2 CMR delineates area at risk associated with acute myocardial infarction. JACC Cardiovasc. Imaging 2012, 5, 596–603. [Google Scholar] [CrossRef] [PubMed]
- Beijnink, C.W.H.; van der Hoeven, N.W.; Konijnenberg, L.S.F.; Kim, R.J.; Bekkers, S.; Kloner, R.A.; Everaars, H.; El Messaoudi, S.; van Rossum, A.C.; van Royen, N.; et al. Cardiac MRI to Visualize Myocardial Damage after ST-Segment Elevation Myocardial Infarction: A Review of Its Histologic Validation. Radiology 2021, 301, 4–18. [Google Scholar] [CrossRef]
- Hausenloy, D.J.; Chilian, W.; Crea, F.; Davidson, S.M.; Ferdinandy, P.; Garcia-Dorado, D.; van Royen, N.; Schulz, R.; Heusch, G. The coronary circulation in acute myocardial ischaemia/reperfusion injury: A target for cardioprotection. Cardiovasc. Res. 2019, 115, 1143–1155. [Google Scholar] [CrossRef] [PubMed]
- Sutton, T.A.; Mang, H.E.; Campos, S.B.; Sandoval, R.M.; Yoder, M.C.; Molitoris, B.A. Injury of the renal microvascular endothelium alters barrier function after ischemia. Am. J. Physiol. Renal Physiol. 2003, 285, F191–F198. [Google Scholar] [CrossRef]
- Itagaki, K.; Zhang, Q.; Hauser, C.J. Sphingosine kinase inhibition alleviates endothelial permeability induced by thrombin and activated neutrophils. Shock 2010, 33, 381–386. [Google Scholar] [CrossRef]
- Chen, J.; Shi, W.; Xu, Y.; Zhang, H.; Chen, B. Hirudin prevents vascular endothelial cell apoptosis and permeability enhancement induced by the serum from rat with chronic renal failure through inhibiting RhoA/ROCK signaling pathway. Drug Dev. Res. 2021, 82, 553–561. [Google Scholar] [CrossRef]
- Krug, A.; Du Mesnil de, R.; Korb, G. Blood supply of the myocardium after temporary coronary occlusion. Circ. Res. 1966, 19, 57–62. [Google Scholar] [CrossRef]
- Nijveldt, R.; Beek, A.M.; Hirsch, A.; Stoel, M.G.; Hofman, M.B.; Umans, V.A.; Algra, P.R.; Twisk, J.W.; van Rossum, A.C. Functional recovery after acute myocardial infarction: Comparison between angiography, electrocardiography, and cardiovascular magnetic resonance measures of microvascular injury. J. Am. Coll. Cardiol. 2008, 52, 181–189. [Google Scholar] [CrossRef]
- Wu, K.C.; Zerhouni, E.A.; Judd, R.M.; Lugo-Olivieri, C.H.; Barouch, L.A.; Schulman, S.P.; Blumenthal, R.S.; Lima, J.A. Prognostic significance of microvascular obstruction by magnetic resonance imaging in patients with acute myocardial infarction. Circulation 1998, 97, 765–772. [Google Scholar] [CrossRef]
- Klug, G.; Mayr, A.; Schenk, S.; Esterhammer, R.; Schocke, M.; Nocker, M.; Jaschke, W.; Pachinger, O.; Metzler, B. Prognostic value at 5 years of microvascular obstruction after acute myocardial infarction assessed by cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2012, 14, 46. [Google Scholar] [CrossRef]
- Mayr, A.; Klug, G.; Reindl, M.; Lechner, I.; Tiller, C.; Holzknecht, M.; Pamminger, M.; Troger, F.; Schocke, M.; Bauer, A.; et al. Evolution of Myocardial Tissue Injury: A CMR Study Over a Decade After STEMI. JACC Cardiovasc. Imaging 2022, 15, 1030–1042. [Google Scholar] [CrossRef]
- Bonfig, N.L.; Soukup, C.R.; Shah, A.A.; Olet, S.; Davidson, S.J.; Schmidt, C.W.; Peterson, R.; Henry, T.D.; Traverse, J.H. Increasing myocardial edema is associated with greater microvascular obstruction in ST-segment elevation myocardial infarction. Am. J. Physiol. Heart Circ. Physiol. 2022, 323, H818–H824. [Google Scholar] [CrossRef]
- Guan, X.; Chen, Y.; Yang, H.J.; Zhang, X.; Ren, D.; Sykes, J.; Butler, J.; Han, H.; Zeng, M.; Prato, F.S.; et al. Assessment of intramyocardial hemorrhage with dark-blood T2*-weighted cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2021, 23, 88. [Google Scholar] [CrossRef]
- Kidambi, A.; Biglands, J.D.; Higgins, D.M.; Ripley, D.P.; Zaman, A.; Broadbent, D.A.; McDiarmid, A.K.; Swoboda, P.P.; Al Musa, T.; Erhayiem, B.; et al. Susceptibility-weighted cardiovascular magnetic resonance in comparison to T2 and T2 star imaging for detection of intramyocardial hemorrhage following acute myocardial infarction at 3 Tesla. J. Cardiovasc. Magn. Reson. 2014, 16, 86. [Google Scholar] [CrossRef]
- Hamirani, Y.S.; Wong, A.; Kramer, C.M.; Salerno, M. Effect of microvascular obstruction and intramyocardial hemorrhage by CMR on LV remodeling and outcomes after myocardial infarction: A systematic review and meta-analysis. JACC Cardiovasc. Imaging 2014, 7, 940–952. [Google Scholar] [CrossRef]
- Zhao, Y.N.; Cui, J.N.; Zhang, X.H.; Li, J.F.; Chen, S.M.; Yue, X.Z.; Li, T. Relationship of Microvascular Obstruction with Global and Regional Myocardial Function Determined by Cardiac Magnetic Resonance after ST-Segment Elevation Myocardial Infarction. Chin. Med. Sci. J. 2023, 38, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Kidambi, A.; Mather, A.N.; Motwani, M.; Swoboda, P.; Uddin, A.; Greenwood, J.P.; Plein, S. The effect of microvascular obstruction and intramyocardial hemorrhage on contractile recovery in reperfused myocardial infarction: Insights from cardiovascular magnetic resonance. J. Cardiovasc. Magn. Reson. 2013, 15, 58. [Google Scholar] [CrossRef] [PubMed]
- Masci, P.G.; Pavon, A.G.; Muller, O.; Iglesias, J.F.; Vincenti, G.; Monney, P.; Harbaoui, B.; Eeckhout, E.; Schwitter, J. Relationship between CMR-derived parameters of ischemia/reperfusion injury and the timing of CMR after reperfused ST-segment elevation myocardial infarction. J. Cardiovasc. Magn. Reson. 2018, 20, 50. [Google Scholar] [CrossRef] [PubMed]
- Ibanez, B.; Aletras, A.H.; Arai, A.E.; Arheden, H.; Bax, J.; Berry, C.; Bucciarelli-Ducci, C.; Croisille, P.; Dall’Armellina, E.; Dharmakumar, R.; et al. Cardiac MRI Endpoints in Myocardial Infarction Experimental and Clinical Trials: JACC Scientific Expert Panel. J. Am. Coll. Cardiol. 2019, 74, 238–256. [Google Scholar] [CrossRef] [PubMed]
- Lai, W.; Chen-Xu, Z.; Jian-Xun, D.; Jie, H.; Ling-Cong, K.; Dong-Ao-Lei, A.; Bing-Hua, C.; Song, D.; Zheng, L.; Fan, Y.; et al. Prognostic implications of left ventricular torsion measured by feature-tracking cardiac magnetic resonance in patients with ST-elevation myocardial infarction. Eur. Heart J. Cardiovasc. Imaging 2022, 24, 785–795. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Y.; Lu, X.; Wan, F.; Gao, L.; Lin, N.; He, J.; Wei, L.; Dong, J.; Qin, Z.; Zhong, F.; et al. Disruption of Circadian Rhythms by Shift Work Exacerbates Reperfusion Injury in Myocardial Infarction. J. Am. Coll. Cardiol. 2022, 79, 2097–2115. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Indexes | All (n = 42) | Bivalirudin Group (n = 21) | UFH Group (n = 21) | p Value |
|---|---|---|---|---|
| Age, years (SD) | 67.9 (5.5) | 67.7 (6.5) | 68.1 (4.1) | 0.762 |
| Male, n (%) | 32 (76.2) | 16 (76.2) | 16 (76.2) | 1.000 |
| Smoking, n (%) | 25 (59.5) | 13 (61.9) | 12 (57.1) | 0.753 |
| Hypertension, n (%) | 28 (66.7) | 14 (66.7) | 14 (66.7) | 1.000 |
| Hyperlipidemia, n (%) | 24 (57.1) | 12 (57.1) | 12 (57.1) | 1.000 |
| Diabetes, n (%) | 12 (28.6) | 6 (28.6) | 6 (28.6) | 1.000 |
| BMI, kg/m2 (SD) | 25.3 (1.6) | 25.1 (1.7) | 25.6 (1.6) | 0.366 |
| Killip class, n (%) | 0.948 | |||
| I | 35 (83.3) | 18 (86.7) | 17 (81.0) | |
| II | 3 (7.1) | 1 (4.8) | 2 (9.5) | |
| III | 2 (4.8) | 1 (4.8) | 1 (4.8) | |
| IV | 2 (4.8) | 1 (4.8) | 1 (4.8) | |
| Location of infarction, n (%) | 1.000 | |||
| Anterior | 26 (61.9) | 13 (61.9) | 13 (61.9) | |
| Non-anterior | 16 (38.1) | 8 (38.1) | 8 (38.1) | |
| Multivessel disease, n (%) | 21 (50.0) | 11 (52.4) | 10 (47.6) | 0.758 |
| Number of lesions, n (%) | 1.000 | |||
| 1 | 26 (61.9) | 13 (61.9) | 13 (61.9) | |
| ≥2 | 16 (38.1) | 8 (38.1) | 8 (38.1) | |
| Thrombus aspiration, n (%) | 10 (23.8) | 6 (28.6) | 4 (19.0) | 0.469 |
| TIMI flow post PCI, n (%) | - | |||
| 0 | 0 (0) | 0 (0) | 0 (0) | |
| 1 | 0 (0) | 0 (0) | 0 (0) | |
| 2 | 0 (0) | 0 (0) | 0 (0) | |
| 3 | 42 (100) | 21 (100) | 21 (100) | |
| Aspirin, n (%) | 42 (100) | 21 (100) | 21 (100) | 1.00 |
| P2Y12R inhibitor, n (%) | 0.378 | |||
| Clopidogrel | 6 (14.3) | 2 (9.5) | 4 (19.0) | |
| Ticagrelor | 36 (85.7) | 19 (90.5) | 17 (81.0) | |
| GPIIb/IIIa inhibitor usage | 0 (0) | 0 (0) | 0 (0) | - |
| CMR Index | All (n = 42) | Bivalirudin Group (n = 21) | UFH Group (n = 21) | p Value |
|---|---|---|---|---|
| Within one week after PCI | ||||
| LVEF, % (SD) | 44.4 (7.0) | 44.0 (6.9) | 44.9 (6.8) | 0.67 |
| IS, % (SD) | 29.6 (5.9) | 28.4 (5.9) | 30.9 (5.7) | 0.17 |
| Myocardium edema, n (%) | 42 (100) | 21 (100) | 21 (100) | - |
| Myocardium edema, % (SD) | 34.2 (7.4) | 31.5 (7.4) | 36.9 (6.9) | 0.02 |
| MVO, n (%) | 26 (61.9) | 12 (57.1) | 14 (66.7) | 0.75 |
| MVO, % (SD) | 0.9 (0.5) | 0.5 (0.4) | 1.2 (0.3) | <0.01 |
| IMH *, n (%) | 8 (19.0) | 1 (4.8) | 7 (33.3) | 0.02 |
| T2 mapping, ms (SD) | 48.8 (7.5) | 46.11 (3.2) | 51.5 (9.3) | 0.02 |
| T1 mapping | ||||
| Infarct core, ms (SD) | 1247.9 (96.1) | 1284.0 (49.8) | 1211.8 (115.6) | 0.01 |
| Peri-infarct zone, ms (SD) | 1319.1 (107.4) | 1296.1 (110.8) | 1342.0 (98.7) | 0.17 |
| Remote myocardium, ms (SD) | 1339.1 (147.2) | 1306.8 (119.9) | 1371.9 (163.7) | 0.16 |
| One month after PCI | ||||
| LVEF, % (SD) | 48.2 (10.6) | 49.2 (11.6) | 47.3 (9.3) | 0.57 |
| dLVEF, % (SD) | 3.8 (6.6) | 4.3 (6.8) | 3.3 (6.3) | 0.63 |
| IS, % (SD) | 23.4 (6.4) | 22.7 (5.8) | 24.1 (6.8) | 0.50 |
| Myocardium edema, n (%) | 8 (19.0) | 1 (4.8) | 7 (33.3) | 0.02 |
| Myocardium edema, % (SD) | 9.7 (3.7) | 5.4 (-) | 10.3 (3.6) | - |
| MVO, n (%) | 0 (0) | 0 (0) | 0 (0) | - |
| MVO, % (SD) | 0 (0) | 0 (0) | 0 (0) | - |
| IMH *, n (%) | 8 (19.0) | 1 (4.8) | 7 (33.3) | 0.02 |
| T2 mapping, ms (SD) | 43.9 (8.5) | 40.4 (5.2) | 47.4 (9.6) | <0.01 |
| T1 mapping | ||||
| Infarct core, ms (SD) | 1242.6 (93.9) | 1274.9 (53.7) | 1210.2 (112.5) | 0.02 |
| Peri-infarct zone, ms (SD) | 1309.0 (113.7) | 1286.8 (115.1) | 1331.2 (107.2) | 0.21 |
| Remote myocardium, ms (SD) | 1330.4 (151.5) | 1298.7 (123.9) | 1362.1 (168.9) | 0.18 |
| Three months after PCI | ||||
| LVEF, % (SD) | 49.5 (11.1) | 50.1 (11.8) | 48.9 (10.3) | 0.72 |
| dLVEF, % (SD) | 5.1 (7.6) | 5.3 (6.9) | 5.0 (8.1) | 0.89 |
| IS, % (SD) | 23.2 (8.7) | 22.7 (6.6) | 23.7 (10.4) | 0.71 |
| Myocardium edema, n (%) | 2 (4.8) | 0 (0) | 2 (9.5) | - |
| Myocardium edema, % (SD) | 1 (2.4) | 0 (0) | 1 (4.76) | - |
| MVO, n (%) | 0 (0) | 0 (0) | 0 (0) | - |
| MVO, % (SD) | 0 (0) | 0 (0) | 0 (0) | - |
| IMH *, n (%) | 8 (19.0) | 1 (4.8) | 7 (33.3) | 0.02 |
| T2 mapping, ms (SD) | 42.6 (9.6) | 40.1 (8.6) | 45.1 (9.8) | 0.09 |
| T1 mapping | ||||
| Infarct core, ms (SD) | 1287.0 (96.1) | 1306.0 (56.0) | 1267.9 (121.0) | 0.21 |
| Peri-infarct zone, ms (SD) | 1288.2 (107.3) | 1282.7 (118.5) | 1293.7 (94.5) | 0.75 |
| Remote myocardium, ms (SD) | 1306.3 (156.0) | 1270.9 (131.6) | 1341.8 (169.8) | 0.15 |
| T1/T2 Mapping | All (n = 42) | Bivalirudin Group (n = 21) | UFH Group (n = 21) | p Value |
|---|---|---|---|---|
| Within one week after PCI | ||||
| T2 mapping, ms (SD) | 48.8 (7.5) | 46.11 (3.2) | 51.5 (9.3) | 0.02 |
| T1 mapping | ||||
| Infarct core, ms (SD) | 1247.9 (96.1) | 1284.0 (49.8) | 1211.8 (115.6) | 0.01 |
| Peri-infarct zone, ms (SD) | 1319.1 (107.4) | 1296.1 (110.8) | 1342.0 (98.7) | 0.17 |
| Remote myocardium, ms (SD) | 1339.1 (147.2) | 1306.8 (119.9) | 1371.9 (163.7) | 0.16 |
| One month after PCI | ||||
| T2 mapping, ms (SD) | 48.8 (7.5) | 46.11 (3.2) | 51.5 (9.3) | 0.02 |
| T1 mapping | ||||
| Infarct core, ms (SD) | 1247.9 (96.1) | 1284.0 (49.8) | 1211.8 (115.6) | 0.01 |
| Peri-infarct zone, ms (SD) | 1319.1 (107.4) | 1296.1 (110.8) | 1342.0 (98.7) | 0.17 |
| Remote myocardium, ms (SD) | 1339.1 (147.2) | 1306.8 (119.9) | 1371.9 (163.7) | 0.16 |
| Thirty days after PCI | ||||
| T2 mapping, ms (SD) | 42.6 (9.6) | 40.1 (8.6) | 45.1 (9.8) | 0.09 |
| T1 mapping, ms (SD) | ||||
| Infarct core, ms (SD) | 1287.0 (96.1) | 1306.0 (56.0) | 1267.9 (121.0) | 0.21 |
| Peri-infarct zone, ms (SD) | 1288.2 (107.3) | 1282.7 (118.5) | 1293.7 (94.5) | 0.75 |
| Remote myocardium, ms (SD) | 1306.3 (156.0) | 1270.9 (131.6) | 1341.8 (169.8) | 0.15 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, Y.; Zou, Z.; Xu, B.; Chen, B.; Ge, H.; Ding, S.; Pu, J. Impact of Bivalirudin on Ischemia/Reperfusion Injury in Patients with Reperfused STEMI Assessed by Cardiac Magnetic Resonance. Pharmaceuticals 2024, 17, 196. https://doi.org/10.3390/ph17020196
Zhang Y, Zou Z, Xu B, Chen B, Ge H, Ding S, Pu J. Impact of Bivalirudin on Ischemia/Reperfusion Injury in Patients with Reperfused STEMI Assessed by Cardiac Magnetic Resonance. Pharmaceuticals. 2024; 17(2):196. https://doi.org/10.3390/ph17020196
Chicago/Turabian StyleZhang, Yizhi, Zhiguo Zou, Bihe Xu, Binghua Chen, Heng Ge, Song Ding, and Jun Pu. 2024. "Impact of Bivalirudin on Ischemia/Reperfusion Injury in Patients with Reperfused STEMI Assessed by Cardiac Magnetic Resonance" Pharmaceuticals 17, no. 2: 196. https://doi.org/10.3390/ph17020196
APA StyleZhang, Y., Zou, Z., Xu, B., Chen, B., Ge, H., Ding, S., & Pu, J. (2024). Impact of Bivalirudin on Ischemia/Reperfusion Injury in Patients with Reperfused STEMI Assessed by Cardiac Magnetic Resonance. Pharmaceuticals, 17(2), 196. https://doi.org/10.3390/ph17020196