

Therapeutic Outcomes of High Dose-Dexamethasone versus Prednisolone + Azathioprine, Rituximab, Eltrombopag, and Romiplostim Strategies in Persistent, Chronic, Refractory, and Relapsed Immune Thrombocytopenia Patients
 , , , ,
, , , ,
Abstract
:
1. Introduction
2. Results
2.1. Demographic Data
2.2. Effect of Gender and Age on PLT Counts after Therapeutic Regimens
2.3. Effect of ITP Phases on PLT Counts after Therapeutic Regimens
2.4. Response Results
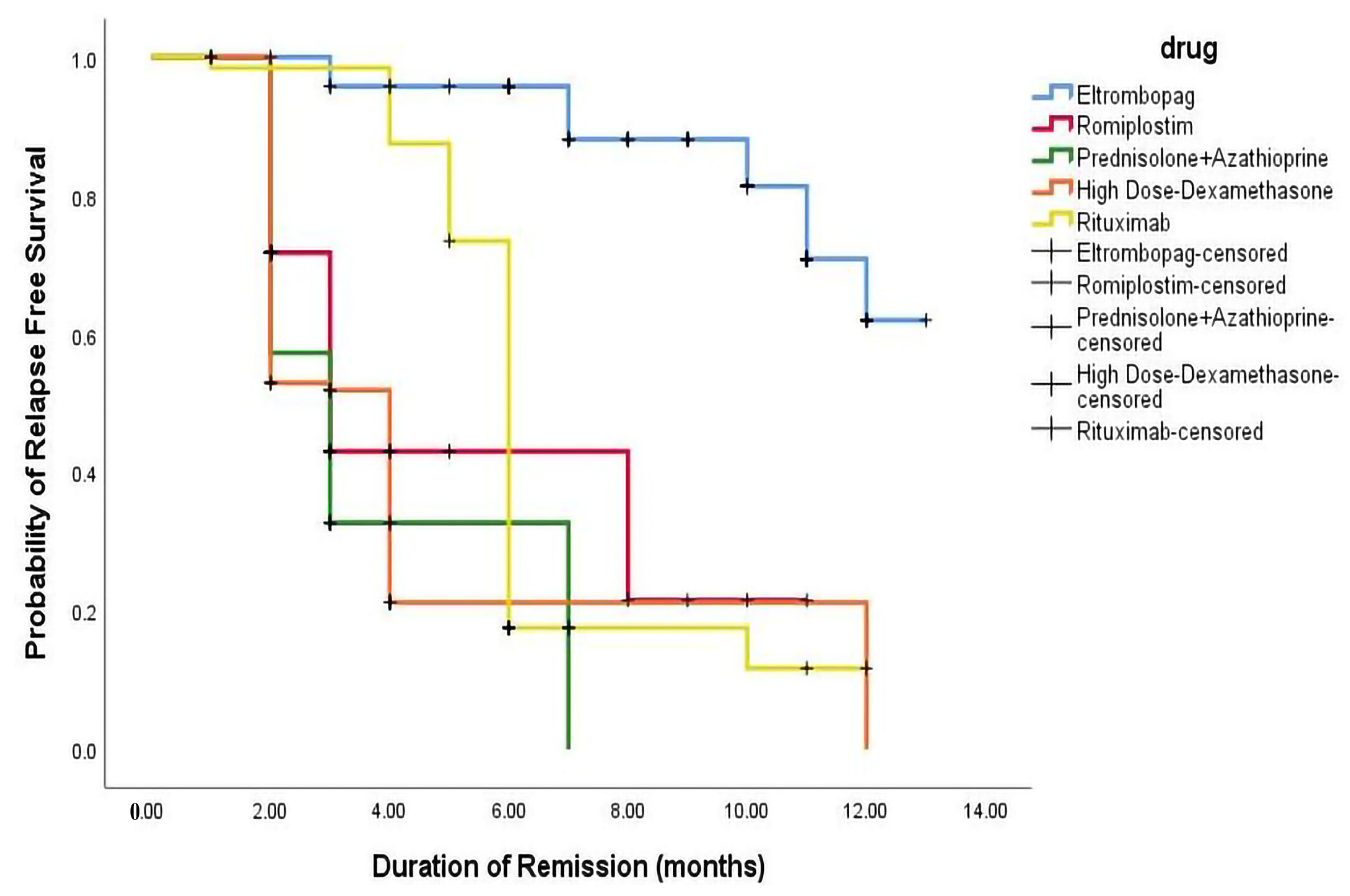
2.5. Relapse-Free Survival
3. Discussion
4. Materials and Methods
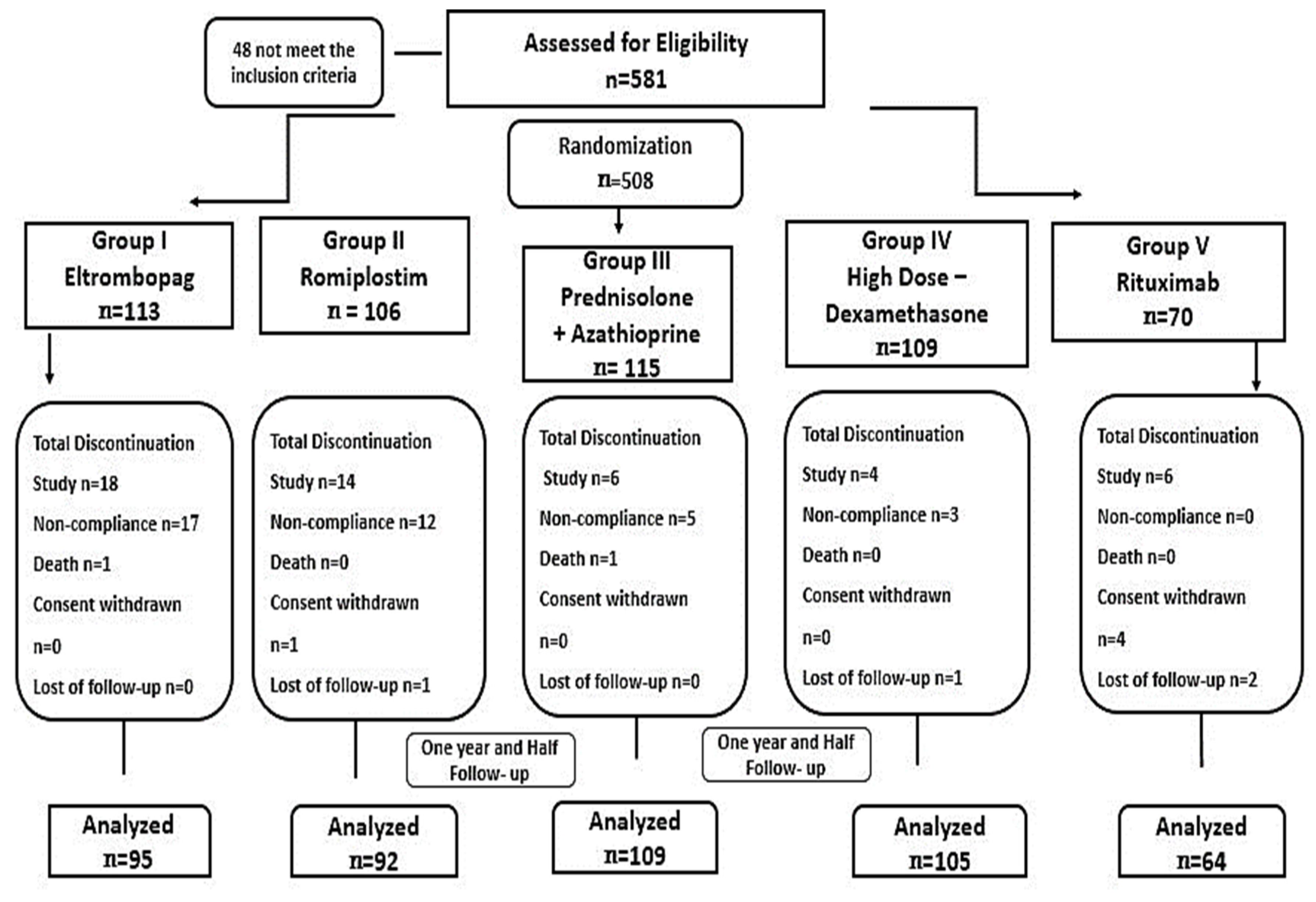
4.1. Patients Selection
4.2. Study Design
4.2.1. Interventions
4.2.2. Randomization
4.3. Outcome Measures
4.4. Statistical Analyses
4.5. Sample Size
4.6. Power of Sample Size
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Ibrahim, L.; Dong, S.X.; O’Hearn, K.; Grimes, A.B.; Kaicker, S.; FritchLilla, S.; Breakey, V.R.; Grace, R.F.; Lebensburger, J.D.; Klaassen, R.J.; et al. Pediatric refractory immune thrombocytopenia: A systematic review. Pediatr. Blood Cancer 2022, 70, e30173. [Google Scholar] [CrossRef]
- Li, N.; Mahamad, S.; Parpia, S.; Iorio, A.; Foroutan, F.; Heddle, N.M.; Hsia, C.C.; Sholzberg, M.; Rimmer, E.; Shivakumar, S.; et al. Development and internal validation of a clinical prediction model for the diagnosis of immune thrombocytopenia. J. Thromb. Haemost. 2022, 20, 2988–2997. [Google Scholar] [CrossRef]
- Hamed, E.M.; Ibrahim, A.R.N.; Meabed, M.H.; Khalaf, A.M.; El Demerdash, D.M.; Elgendy, M.O.; Saeed, H.; Salem, H.F.; Rabea, H. The Outcomes and Adverse Drug Patterns of Immunomodulators and Thrombopoietin Receptor Agonists in Primary Immune Thrombocytopenia Egyptian Patients with Hemorrhage Comorbidity. Pharmaceuticals 2023, 16, 868. [Google Scholar] [CrossRef]
- Al-Samkari, H.; Kuter, D.J. Immune Thrombocytopenia in Adults: Modern Approaches to Diagnosis and Treatment. Semin. Thromb. Hemost. 2020, 46, 275–288. [Google Scholar] [CrossRef]
- Yasser, A.; Khasahba, E.O.; El Rahman Shokeir, M.A.; El Mabood, S.A. Treatment lines of childhood chronic ITP: A retrospective single-center analysis. Pediatr. Hematol./Oncol. Immunopathol. 2020, 19, 26–30. Available online: https://www.hemoncim.com/jour/article/view/378 (accessed on 5 June 2023). [CrossRef]
- Doobaree, I.U.; Conway, K.; Miah, H.; Miah, A.; Makris, M.; Hill, Q.; Cooper, N.; Bradbury, C.; Newland, A.; Provan, D.; et al. Incidence of adult primary immune thrombocytopenia in England—An update. Eur. J. Haematol. 2022, 109, 238–249. [Google Scholar] [CrossRef] [PubMed]
- Dal, M.S.; Karakus, A.; Aydin, B.B.; Ekmen, M.O.; Ulas, T.; Ayyildiz, O. Serum uric acid and inflammation in patients with immune thrombocytopenic purpura: Preliminary results. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 4385–4389. Available online: http://www.europeanreview.org/wp/wp-content/uploads/4385-4389.pdf (accessed on 17 May 2023). [PubMed]
- Lugus, J.J.; Park, C.; Ma, Y.D.; Choi, K. Both primitive and definitive blood cells are derived from Flk-1+ mesoderm. Blood 2009, 113, 563–566. [Google Scholar] [CrossRef] [PubMed]
- Lang, D.; Dohle, F.; Terstesse, M.; Bangen, P.; August, C.; Pauels, H.-G.; Heidenreich, S. Down-regulation of monocyte apoptosis by phagocytosis of platelets: Involvement of a caspase-9, caspase-3, and heat shock protein 70-dependent pathway. J. Immunol. 2002, 168, 6152–6158. [Google Scholar] [CrossRef]
- Kuter, D.J.; Newland, A.; Chong, B.H.; Rodeghiero, F.; Romero, M.T.; Pabinger, I.; Chen, Y.; Wang, K.; Mehta, B.; Eisen, M. Romiplostim in adult patients with newly diagnosed or persistent immune thrombocytopenia (ITP) for up to 1 year and in those with chronic ITP for more than 1 year: A subgroup analysis of integrated data from completed romiplostim studies. Br. J. Haematol. 2019, 185, 503–513. [Google Scholar] [CrossRef]
- Rodeghiero, F.; Stasi, R.; Gernsheimer, T.; Michel, M.; Provan, D.; Arnold, D.M.; Bussel, J.B.; Cines, D.B.; Chong, B.H.; Cooper, N.; et al. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: Report from an international working group. Blood 2009, 113, 2386–2393. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.-G.; Bai, X.-C.; Chen, F.-P.; Cheng, Y.-F.; Dai, K.-S.; Fang, M.-Y.; Feng, J.-M.; Gong, Y.-P.; Guo, T.; Guo, X.-H.; et al. Chinese guidelines for treatment of adult primary immune thrombocytopenia. Int. J. Hematol. 2018, 107, 615–623. [Google Scholar] [CrossRef] [PubMed]
- Vianelli, N.; Auteri, G.; Buccisano, F.; Carrai, V.; Baldacci, E.; Clissa, C.; Bartoletti, D.; Giuffrida, G.; Magro, D.; Rivolti, E.; et al. Refractory primary immune thrombocytopenia (ITP): Current clinical challenges and therapeutic perspectives. Ann. Hematol. 2022, 101, 963–978. [Google Scholar] [CrossRef]
- Torere, B.E.; Aiwuyo, H.O.; Weigold, J.; Gerlach, G.; Ilerhunmwuwa, N.; Khan, U.; Belousova, T. The Roles and Challenges of Advanced Therapies in the Management of Refractory Immune Thrombocytopenia: A Case Report and Review of the Literature. Cureus 2023, 15, e36146. [Google Scholar] [CrossRef]
- Miltiadous, O.; Hou, M.; Bussel, J.B. Identifying and treating refractory ITP: Difficulty in diagnosis and role of combination treatment. Blood 2020, 135, 472–490. [Google Scholar] [CrossRef] [PubMed]
- Woolley, P.; Newton, R.; Mc Guckin, S.; Thomas, M.; Westwood, J.; Scully, M.A. Immune thrombocytopenia in adults: A single-centre review of demographics, clinical features and treatment outcomes. Eur. J. Haematol. 2020, 105, 344–351. [Google Scholar] [CrossRef]
- Neunert, C.; Terrell, D.R.; Arnold, D.M.; Buchanan, G.; Cines, D.B.; Cooper, N.; Cuker, A.; Despotovic, J.M.; George, J.N.; Grace, R.F.; et al. American Society of Hematology 2019 guidelines for immune thrombocytopenia. Blood Adv. 2020, 4, 252. [Google Scholar] [CrossRef]
- Ahmed, R.; Devasia, A.J.; Viswabandya, A.; Lakshmi, K.M.; Abraham, A.; Karl, S.; Mathai, J.; Jacob, P.M.; Abraham, D.; Srivastava, A.; et al. Long-term outcome following splenectomy for chronic and persistent immune thrombocytopenia (ITP) in adults and children: Splenectomy in ITP. Ann. Hematol. 2016, 95, 1429–1434. [Google Scholar] [CrossRef]
- Podstawka, J.; Wall, E.; Bolster, L.; Patterson, J.M.; Goodyear, M.D.; Rydz, N.; Sun, H.L. Treatment patterns and outcomes of second-line rituximab and thrombopoietin receptor agonists in adult immune thrombocytopenia: A Canadian retrospective cohort study. Thromb. Res. 2022, 220, 5–11. [Google Scholar] [CrossRef]
- Provan, D.; Arnold, D.M.; Bussel, J.B.; Chong, B.H.; Cooper, N.; Gernsheimer, T.; Ghanima, W.; Godeau, B.; González-López, T.J.; Grainger, J.; et al. Updated international consensus report on the investigation and management of primary immune thrombocytopenia. Blood Adv. 2019, 3, 3780–3817. Available online: https://ashpublications.org/bloodadvances/article-abstract/3/22/3780/428877 (accessed on 28 June 2023). [CrossRef]
- Mageau, A.; Terriou, L.; Ebbo, M.; Souchaud-Debouverie, O.; Orvain, C.; Graveleau, J.; Lega, J.; Ruivard, M.; Viallard, J.; Cheze, S.; et al. Splenectomy for primary immune thrombocytopenia revisited in the era of thrombopoietin receptor agonists: New insights for an old treatment. Am. J. Hematol. 2021, 97, 10–17. [Google Scholar] [CrossRef]
- Sandal, R.; Mishra, K.; Jandial, A.; Sahu, K.K.; Siddiqui, A.D. Update on diagnosis and treatment of immune thrombocytopenia. Expert Rev. Clin. Pharmacol. 2021, 14, 553–568. [Google Scholar] [CrossRef]
- Kuwana, M.; Ikeda, Y. The role of autoreactive T-cells in the pathogenesis of idiopathic thrombocytopenic purpura. Int. J. Hematol. 2005, 81, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Mei, H.; Xu, M.; Yuan, G.; Zhu, F.; Guo, J.; Huang, R.; Qin, J.; Lv, T.; Qin, F.; Cai, H.; et al. A multicentre double-blind, double-dummy, randomised study of recombinant human thrombopoietin versus eltrombopag in the treatment of immune thrombocytopenia in Chinese adult patients. Br. J. Haematol. 2021, 195, 781–789. [Google Scholar] [CrossRef]
- Sasazawa, Y.; Sato, N.; Suzuki, T.; Dohmae, N.; Simizu, S. C-Mannosylation of thrombopoietin receptor (c-Mpl) regulates thrombopoietin-dependent JAK-STAT signaling. Biochem. Biophys. Res. Commun. 2015, 468, 262–268. [Google Scholar] [CrossRef]
- Gilbert, M.M.; Grimes, A.B.; Kim, T.O.; Despotovic, J.M. Romiplostim for the treatment of immune thrombocytopenia: Spotlight on patient acceptability and ease of use. Patient Prefer. Adherence 2020, 14, 1237–1250. [Google Scholar] [CrossRef]
- Kuter, D.J. The biology of thrombopoietin and thrombopoietin receptor agonists. Int. J. Hematol. 2013, 98, 10–23. [Google Scholar] [CrossRef] [PubMed]
- Kashiwagi, H.; Kuwana, M.; Hato, T.; Takafuta, T.; Fujimura, K.; Kurata, Y.; Murata, M.; Tomiyama, Y. Reference guide for management of adult immune thrombocytopenia in Japan: 2019 Revision. Int. J. Hematol. 2020, 111, 329–351. [Google Scholar] [CrossRef] [PubMed]
- Puavilai, T.; Thadanipon, K.; Rattanasiri, S.; Ingsathit, A.; McEvoy, M.; Attia, J.; Thakkinstian, A. Treatment efficacy for adult persistent immune thrombocytopenia: A systematic review and network meta-analysis. Br. J. Haematol. 2019, 188, 450–459. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Zong, H.; Li, F.; Luo, S.; Zhang, X.; Xu, Y.; Zhang, X. Eltrombopag modulates the phenotypic evolution and potential immunomodulatory roles of monocytes/macrophages in immune thrombocytopenia. Platelets 2022, 34, 2135694. [Google Scholar] [CrossRef]
- Lozano, M.L.; Segú-Vergés, C.; Coma, M.; Álvarez-Roman, M.T.; González-Porras, J.R.; Gutiérrez, L.; Valcárcel, D.; Butta, N. Elucidating the mechanism of action of the attributed immunomodulatory role of eltrombopag in primary immune thrombocytopenia: An in silico approach. Int. J. Mol. Sci. 2021, 22, 6907. [Google Scholar] [CrossRef]
- Crickx, E.; Chappert, P.; Sokal, A.; Weller, S.; Azzaoui, I.; Vandenberghe, A.; Bonnard, G.; Rossi, G.; Fadeev, T.; Storck, S.; et al. Rituximab-resistant splenic memory B cells and newly engaged naive B cells fuel relapses in patients with immune thrombocytopenia. Sci. Transl. Med. 2021, 13, 589. [Google Scholar]
- Mazza, P.; Minoia, C.; Melpignano, A.; Polimeno, G.; Cascavilla, N.; Di Renzo, N.; Specchia, G. The use of thrombopoietin-receptor agonists (TPO-RAs) in immune thrombocytopenia (ITP): A “real life” retrospective multicenter experience of the Rete Ematologica Pugliese (REP). Ann. Hematol. 2015, 95, 239–244. [Google Scholar] [CrossRef]
- Wang, Y.; Guo, X.; Jiao, G.; Luo, L.; Zhou, L.; Zhang, J.; Wang, B. Splenectomy Promotes Macrophage Polarization in a Mouse Model of Concanavalin A- (ConA-) Induced Liver Fibrosis. BioMed Res. Int. 2019, 2019, 5756189. [Google Scholar] [CrossRef] [PubMed]
- Feng, Q.; Xu, M.; Yu, Y.Y.; Hou, Y.; Mi, X.; Sun, Y.X.; Ma, S.; Zuo, X.Y.; Shao, L.L.; Hou, M.; et al. High-dose Dexamethasone or all-trans-retinoic acid restores the balance of macrophages towards M2 in immune thrombocytopenia. J. Thromb. Haemost. 2017, 15, 1845–1858. [Google Scholar] [CrossRef]
- Winkelhorst, D.; Kamphuis, M.M.; de Kloet, L.C.; Zwaginga, J.J.; Oepkes, D.; Lopriore, E. Severe bleeding complications other than intracranial hemorrhage in neonatal alloimmune thrombocytopenia: A case series and review of the literature. Transfusion 2016, 56, 1230–1235. [Google Scholar] [CrossRef]
- Eser, A.; Toptas, T.; Kara, O.; Sezgin, A.; Noyan–Atalay, F.; Yilmaz, G.; Ozgumus, T.; Pepedil-Tanrikulu, F.; Kaygusuz-Atagunduz, I.; Firatli-Tuglular, T. Efficacy and safety of eltrombopag in treatment-refractory primary immune thrombocytopenia: A retrospective study. Blood Coagul. Fibrinolysis 2016, 27, 47–52. [Google Scholar] [CrossRef]
- Zhang, L.; Zhang, M.; Du, X.; Cheng, Y.; Cheng, G. Safety and efficacy of eltrombopag plus pulsed Dexamethasone as first-line therapy for immune thrombocytopenia. Br. J. Haematol. 2020, 189, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Tran, H.; Brighton, T.; Grigg, A.; McRae, S.; Dixon, J.; Thurley, D.; Gandhi, M.K.; Truman, M.; Marlton, P.; Catalano, J. A multi-centre, single-arm, open-label study evaluating the safety and efficacy of fixed dose rituximab in patients with refractory, relapsed or chronic idiopathic thrombocytopenic purpura (R-ITP 1000 study). Br. J. Haematol. 2014, 167, 243–251. [Google Scholar] [CrossRef]
- Yu, Y.; Wang, M.; Hou, Y.; Qin, P.; Zeng, Q.; Yu, W.; Guo, X.; Wang, J.; Wang, X.; Liu, G.; et al. High-dose Dexamethasone plus recombinant human thrombopoietin vs high-dose Dexamethasone alone as frontline treatment for newly diagnosed adult primary immune thrombocytopenia: A prospective, multicenter, randomized trial. Am. J. Hematol. 2020, 95, 1542–1552. [Google Scholar] [CrossRef] [PubMed]
- Meyer, O.; Richter, H.; Lebioda, A.; Schill, M. Treatment patterns in adults with immune thrombocytopenia before, during and after use of thrombopoietin receptor agonists: A longitudinal prescription database study from Germany. Hematology 2021, 26, 697–708. [Google Scholar] [CrossRef] [PubMed]
- González-López, T.J.; Fernández-Fuertes, F.; Hernández-Rivas, J.A.; Sánchez-González, B.; Martínez-Robles, V.; Alvarez-Román, M.T.; Pérez-Rus, G.; Pascual, C.; Bernat, S.; Arrieta-Cerdán, E.; et al. Efficacy and safety of eltrombopag in persistent and newly diagnosed ITP in clinical practice. Int. J. Hematol. 2017, 106, 508–516. [Google Scholar] [CrossRef]
- Tripathi, A.K.; Shukla, A.; Mishra, S.; Yadav, Y.S.; Yadav, D.K. Eltrombopag therapy in newly diagnosed steroid non-responsive ITP patients. Int. J. Hematol. 2014, 99, 413–417. [Google Scholar] [CrossRef]
- Tjønnfjord, E.; Holme, P.A.; Darne, B.; Khelif, A.; Waage, A.; Michel, M.; Ben Romdhan, N.; Ghanima, W. Long-term outcomes of patients treated with Rituximab as second-line treatment for adult immune thrombocytopenia–Follow-up of the RITP study. Br. J. Haematol. 2020, 191, 460–465. [Google Scholar] [CrossRef]
- Lal, L.S.; Said, Q.; Andrade, K.; Cuker, A. Second-line treatments and outcomes for immune thrombocytopenia: A retrospective study with electronic health records. Res. Pract. Thromb. Haemost. 2020, 4, 1131–1140. [Google Scholar] [CrossRef] [PubMed]
- Cuker, A.; Neunert, C.E. How I treat refractory immune thrombocytopenia. Blood 2016, 128, 1547–1554. [Google Scholar] [CrossRef]
- Cuker, A.; Liebman, H.A. Corticosteroid overuse in adults with immune thrombocytopenia: Cause for concern. Res. Pract. Thromb. Haemost. 2021, 5, e12592. [Google Scholar] [CrossRef] [PubMed]
- Visco, C.; Rodeghiero, F.; Romano, A.; Valeri, F.; Merli, M.; Quaresimini, G.; Volpetti, S.; Santi, R.M.; Carli, G.; Lucchini, E.; et al. Eltrombopag for immune thrombocytopenia secondary to chronic lymphoproliferative disorders: A phase 2 multicenter study. Blood 2019, 134, 1708–1711. [Google Scholar] [CrossRef] [PubMed]
- Ishiyama, M.; Shiseki, M.; Yoshinaga, K.; Ryuzaki, M.; Izuka, Y.; Watanabe, A.; Tanaka, N.; Shinohara, A.; Hagiwara, S.; Tanaka, J. Very early increased platelet count within a week after initiation of high-dose dexamethasone treatment is associated with long-term response in newly diagnosed immune thrombocytopenia patients. Acta Haematol. 2021, 145, 193–200. [Google Scholar] [CrossRef] [PubMed]
- Tavakolpour, S.; Aryanian, Z.; Seirafianpour, F.; Dodangeh, M.; Etesami, I.; Daneshpazhooh, M.; Balighi, K.; Mahmoudi, H.; Goodarzi, A. A systematic review on efficacy, safety, and treatment-durability of low-dose Rituximab for the treatment of Pemphigus: Special focus on COVID-19 pandemic concerns. Immunopharmacol. Immunotoxicol. 2021, 43, 507–518. [Google Scholar] [CrossRef]
- Kuter, D.J.; Bussel, J.B.; Newland, A.; Baker, R.I.; Lyons, R.M.; Wasser, J.; Viallard, J.-F.; Macik, G.; Rummel, M.; Nie, K.; et al. Long-term treatment with romiplostim in patients with chronic immune thrombocytopenia: Safety and efficacy. Br. J. Haematol. 2013, 161, 411–423. [Google Scholar] [CrossRef]
- Hubulashvili, D.; Marzella, N. Romiplostim (Nplate), a treatment option for immune (idiopathic) thrombocytopenic purpura. Pharm. Ther. 2009, 34, 482–485. [Google Scholar]
- Mishra, K.; Pramanik, S.; Jandial, A.; Sahu, K.K.; Sandal, R.; Ahuja, A.; Yanamandra, U.; Kumar, R.; Kapoor, R.; Verma, T.; et al. Real-world experience of eltrombopag in immune thrombocytopenia. Am. J. Blood Res. 2020, 10, 240. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2799136/ (accessed on 7 June 2023).
- Guo, C.; Chu, X.; Shi, Y.; He, W.; Li, L.; Wang, L.; Wang, Y.; Peng, J.; Hou, M. Correction of Th1-dominant cytokine profiles by high-dose Dexamethasone in patients with chronic idiopathic thrombocytopenic purpura. J. Clin. Immunol. 2007, 27, 557–562. [Google Scholar] [CrossRef]
- Bidika, E.; Fayyaz, H.; Salib, M.; Memon, A.N.; Gowda, A.S.; Rallabhandi, B.; Cancarevic, I. Romiplostim and eltrombopag in immune thrombocytopenia as a second-line treatment. Cureus 2020, 12, e9920. [Google Scholar] [CrossRef]
- Lambert, M.P.; Gernsheimer, T.B. Clinical updates in adult immune thrombocytopenia. Blood 2017, 129, 2829–2835. [Google Scholar] [CrossRef] [PubMed]
- Tarantino, M.D.; Bussel, J.B.; Blanchette, V.S.; Despotovic, J.; Bennett, C.; Raj, A.; Williams, B.; Beam, D.; Morales, J.; Rose, M.J.; et al. Romiplostim in children with immune thrombocytopenia: A phase 3, randomised, double-blind, placebo-controlled study. Lancet 2016, 388, 45–54. [Google Scholar] [CrossRef]
- Shimano, K.A.; Grace, R.F.; Despotovic, J.M.; Neufeld, E.J.; Klaassen, R.J.; Bennett, C.M.; Ma, C.; London, W.B.; Neunert, C. Phase 3 randomised trial of eltrombopag versus standard first-line pharmacological management for newly diagnosed immune thrombocytopaenia (ITP) in children: Study protocol. BMJ Open 2021, 11, e044885. [Google Scholar] [CrossRef]
- Zaja, F.; Baccarani, M.; Mazza, P.; Bocchia, M.; Gugliotta, L.; Zaccaria, A.; Vianelli, N.; Defina, M.; Tieghi, A.; Amadori, S.; et al. Dexamethasone plus Rituximab yields higher sustained response rates than dexamethasone monotherapy in adults with primary immune thrombocytopenia. Blood 2010, 115, 2755–2762. [Google Scholar] [CrossRef] [PubMed]
- Ghanima, W.; Khelif, A.; Waage, A.; Michel, M.; E Tjønnfjord, G.; Ben Romdhan, N.; Kahrs, J.; Darne, B.; Holme, P.A. Rituximab as second-line treatment for adult immune thrombocytopenia (the RITP trial): A multicentre, randomised, double-blind, placebo-controlled trial. Lancet 2015, 385, 1653–1661. [Google Scholar] [CrossRef] [PubMed]
- Gudbrandsdottir, S.; Birgens, H.S.; Frederiksen, H.; Jensen, B.A.; Jensen, M.K.; Kjeldsen, L.; Klausen, T.W.; Larsen, H.; Mourits-Andersen, H.T.; Nielsen, C.H.; et al. Rituximab and Dexamethasone vs dexamethasone monotherapy in newly diagnosed patients with primary immune thrombocytopenia. Blood 2013, 121, 1976–1981. [Google Scholar] [CrossRef]
- Dong, Y.; Yue, M.; Hu, M. The efficacy and safety of different dosages of Rituximab for adults with immune thrombocytopenia: A systematic review and meta-analysis. BioMed Res. Int. 2021, 2021, 9992086. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Eltrombopag (n = 95) | Romiplostim (n = 92) | Prednisolone + Azathioprine (n = 109) | HD-Dexamethasone (n = 105) | Rituximab (n = 64) | p-Value | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Age, median (range): years | 34.3 | 32.5 | 27.8 | 29.5 | 34.5 | 0.09 | |||||
| (18–65) | (18–65) | (18–65) | (18–65) | (18–65) | |||||||
| Gender; n (%) | |||||||||||
| Male | 17 (17.8%) | 30 (32.6%) | 18 (17.4%) | 15 (14.3%) | 15 (23.4%) | 0.60 | |||||
| Female | 78 (82.1%) | 62 (67.4%) | 91 (83.4%) | 90 (85.7%) | 49 (76.5%) | 0.08 | |||||
| Age (years) | Male | Female | Male | Female | Male | Female | Male | Female | Male | Female | |
| 18–35 (%) | 18.50% | 81.50% | 31.40% | 68.60% | 13.50% | 0.455 | 19.40% | 80.60% | 22.70% | 77.30% | 0.455 |
| 35–45 (%) | 19.50% | 80.50% | 37.50% | 62.50% | 19.50% | 0.199 | 12.80% | 87.20% | 17.40% | 82.60% | 0.199 |
| 45–65 (%) | 15.60% | 84.40% | 28% | 72% | 16.60% | 0.331 | 10% | 90% | 31.60% | 68.40% | 0.331 |
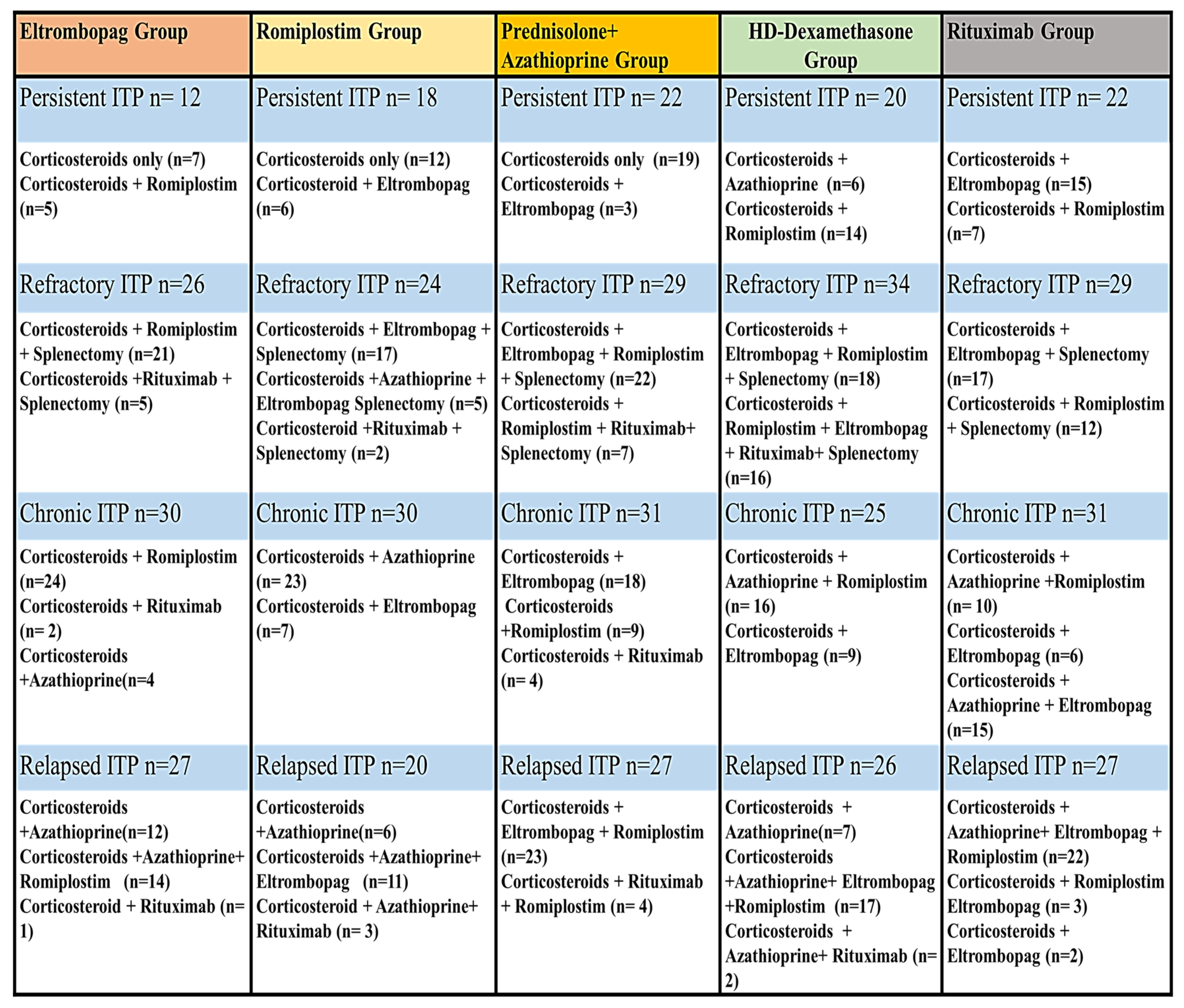
| Persistent ITP; n (%) | 12 (12.6%) | 18 (19.5%) | 22 (20.1%) | 20 (19%) | 22 (20.1%) | 0.769 | |||||
| Chronic ITP; n (%) | 30 (31.5%) | 30 (32.6%) | 31 (28.4%) | 25 (23.8%) | 31 (28.4%) | 0.227 | |||||
| Refractory ITP; n (%) | 26 (27.3%) | 24 (26.08%) | 29 (26.6%) | 34 (32.3%) | 29 (26.6%) | 0.805 | |||||
| Relapsed ITP; n (%) | 27 (28.4%) | 20 (21.7%) | 27 (24.7%) | 26 (24.7%) | 27 (24.7%) | 0.660 | |||||
| Treatment Response | Persistent ITP | Chronic ITP | Refractory ITP | Relapsed ITP | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ORR (%) | SR (%) | NR (%) | ORR (%) | SR (%) | NR (%) | ORR (%) | SR (%) | NR (%) | ORR (%) | SR (%) | NR (%) | |
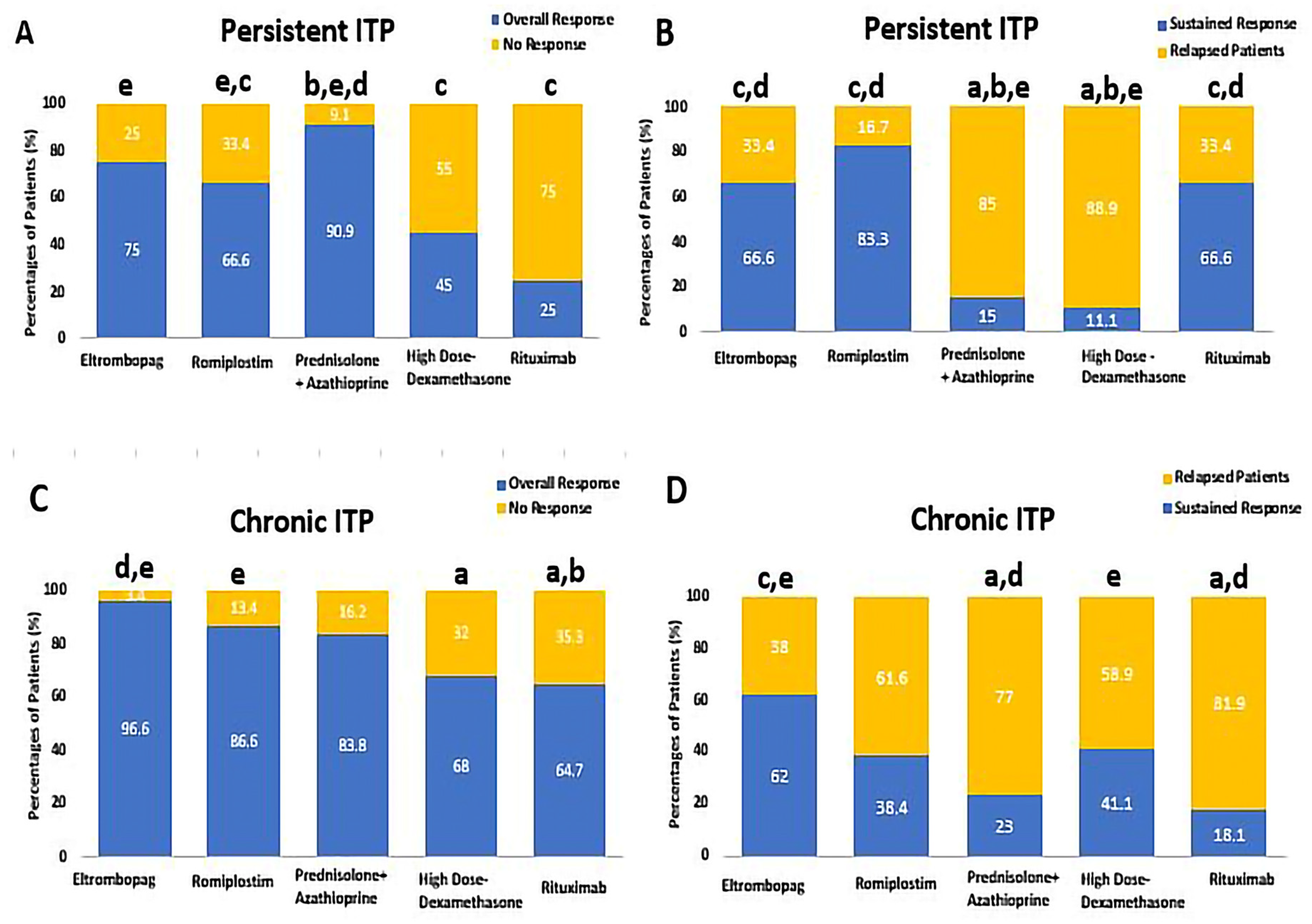
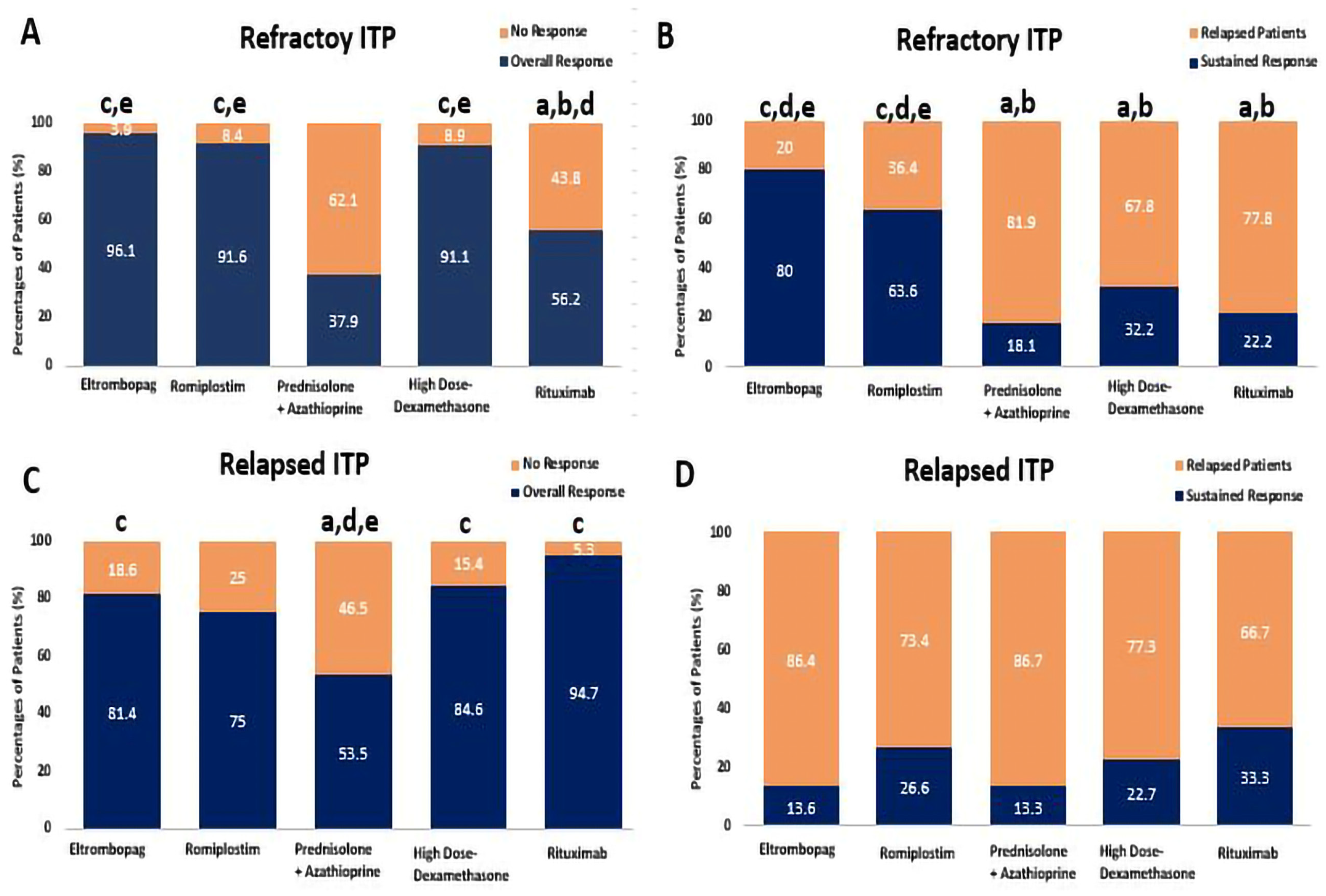
| Eltrombopag (n = 95) | 9/12 (75%) | 6/9 (66.6%) | 3/12 (25%) | 29/30 (96.6%) | 18/29 (62%) | 1/30 (3.3%) | 25/26 (96.1%) | 20/25 (80%) | 1/26 (3.8%) | 22/27 (81.4%) | 3/22 (13.6%) | 5/27 (18.5%) |
| Romiplostim (n = 92) | 12/18 (66.6%) | 10/12 (83.3%) | 6/18 (33.3%) | 26/ 30 (86.6%) | 10/ 26 (38.4%) | 4/30 (13.3%) | 22/24 (91.6%) | 14/22 (63.6%) | 2/24 (8.3%) | 15/20 (75%) | 4/15 (26.6%) | 5/20 (25%) |
| Prednisolone + Azathioprine (n = 109) | 20/22 (90.9%) | 3/20 (15%) | 2/22 (9.09%) | 26/31 (83.8%) | 6/26 (23.07%) | 5/31 (16.1%) | 11/29 (37.9%) | 2/11 (18.1%) | 18/29 (62.06%) | 15 /27 (55.5%) | 2/15 (13.3%) | 12/27 (44.4%) |
| High-Dose Dexamethasone (n = 105) | 9/20 (45%) | 1/9 (11.1%) | 11/20 (55%) | 17/25 (68%) | 7/17 (41.1%) | 8/25 (32%) | 31/34 (91.1%) | 10/31 (32.2%) | 3/34 (8.8%) | 22/26 (84.6%) | 5 /22 (22.7%) | 4/26 (15.3%) |
| Rituximab (n = 64) | 3/12 (25%) | 2/3 (66.6%) | 9/12 (75%) | 11/17 (64.7%) | 2/11 (18.1%) | 6/17 (35.2%) | 9/16 (56.2%) | 2/9 (22.2%) | 7/16 (43.7%) | 18/19 (94.7%) | 6/18 (33.3%) | 1/19 (5.2%) |
| p-value | 0.013 * | 0.001 * | 0.013 * | 0.008 * | 0.030 * | 0.008 * | <0.0001 * | 0.001 * | <0.0001 * | 0.026 * | 0.722 | 0.026 * |
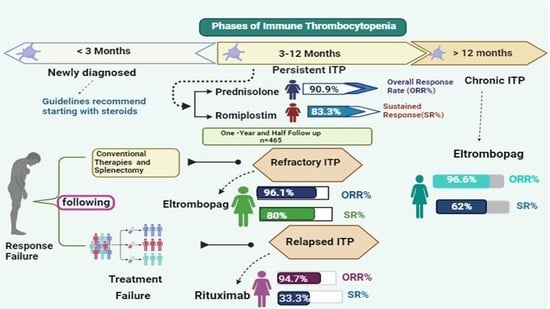
| ITP Phases | The Most Effective Drug, According to PLT Count | Overall Response, ORR (%) | Sustained Response, SR (%) | ORR p-Value | SR p-Value |
|---|---|---|---|---|---|
| Persistent ITP | Prednisolone | Prednisolone (90.9%) | Romiplostim (83.3%) | 0.013 * | 0.001 * |
| Chronic ITP | Prednisolone | Eltrombopag (96.6%) | Eltrombopag (62%) | 0.008 * | 0.030 * |
| Refractory ITP | Prednisolone | Eltrombopag (96.1%) | Eltrombopag (80%) | <0.0001 * | 0.001 * |
| Relapsed ITP | Prednisolone | Rituximab | Rituximab | 0.026 * | 0.722 |
| Corticosteroids (High Dose of Dexamethasone and Prednisolone [20] | |
| Platelet Response | Dose Adjustment |
| If platelet counts <30 × 109/L | Corticosteroids are the standard initial therapeutic regimen for ITP adults: either Prednisolone at 1 mg/kg (to a maximum of 80 mg, even in patients weighing 80 kg) for two weeks, to a maximum of three weeks, or dexamethasone 40 mg/d for 4 days, repeated up to 3 times. |
| Platelet counts >50 ×109/L | Prednisolone dose was tapered to discontinue it within 6 weeks (maximum 8 weeks), even if the platelet count decreased during the decline. |
| No response to the starting dose during two weeks. | Prednisolone was rapidly decreased over 1 week and stopped. |
| Eltrombopag [20,38] | |
| Platelet response | Dose Adjustments |
| If platelet counts <50 × 109/L post at least two weeks of the regimen | The daily dose was elevated by 25 mg to a maximum of 75 mg. |
| Platelet counts were between 50–350 × 109/L. | The Eltrombopag dose was not changed. |
| Platelet counts were between 350–400 × 109/L. | In this condition, the daily dose was reduced by 25 mg and was delayed two weeks to judge the clinical effects. |
| Platelet counts >400 | Eltrombopag was discontinued; PLT counts were monitored every three days and repeated at the previous dose. |
| Romiplostim [51,52] | |
| Platelet response | Dose Adjustments |
| If platelet counts <30 × 109/L | Romiplostim was initiated subcutaneously at a dose of 1 μg/kg per week, with adjustments up to 10 μg/kg per week based on platelet response over 10 weeks. |
| Platelet counts (30–50 × 109/L) | Romiplostim was administrated at a maximum dose of 10 μg/kg |
| Platelet counts, 50–200 × 109/L | The dose was maintained (5–8 μg/kg). |
| Platelet counts > 400 × 109/L | The Romiplostim was discontinued, and platelet count was evaluated each week. When the platelet count dropped below 200 × 109/L, the weekly dose was resumed for 1 week, then 1 μg/kg reduction. |
| No response | If the platelet counts have not increased after four weeks of therapy (at a maximum of 10 mg/kg every week), the Romiplostim was stopped. |
| Rituximab | |
| Platelet response | Dose Adjustments |
| All Rituximab group received 375 mg/m2 of intravenous injection of RTX once weekly for one month. | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hamed, E.M.; Ibrahim, A.R.N.; Meabed, M.H.; Khalaf, A.M.; El Demerdash, D.M.; Elgendy, M.O.; Saeed, H.; Salem, H.F.; Rabea, H. Therapeutic Outcomes of High Dose-Dexamethasone versus Prednisolone + Azathioprine, Rituximab, Eltrombopag, and Romiplostim Strategies in Persistent, Chronic, Refractory, and Relapsed Immune Thrombocytopenia Patients. Pharmaceuticals 2023, 16, 1215. https://doi.org/10.3390/ph16091215
Hamed EM, Ibrahim ARN, Meabed MH, Khalaf AM, El Demerdash DM, Elgendy MO, Saeed H, Salem HF, Rabea H. Therapeutic Outcomes of High Dose-Dexamethasone versus Prednisolone + Azathioprine, Rituximab, Eltrombopag, and Romiplostim Strategies in Persistent, Chronic, Refractory, and Relapsed Immune Thrombocytopenia Patients. Pharmaceuticals. 2023; 16(9):1215. https://doi.org/10.3390/ph16091215
Chicago/Turabian StyleHamed, Eman Mostafa, Ahmed R. N. Ibrahim, Mohamed Hussein Meabed, Ahmed M. Khalaf, Doaa Mohamed El Demerdash, Marwa O. Elgendy, Haitham Saeed, Heba F. Salem, and Hoda Rabea. 2023. "Therapeutic Outcomes of High Dose-Dexamethasone versus Prednisolone + Azathioprine, Rituximab, Eltrombopag, and Romiplostim Strategies in Persistent, Chronic, Refractory, and Relapsed Immune Thrombocytopenia Patients" Pharmaceuticals 16, no. 9: 1215. https://doi.org/10.3390/ph16091215
APA StyleHamed, E. M., Ibrahim, A. R. N., Meabed, M. H., Khalaf, A. M., El Demerdash, D. M., Elgendy, M. O., Saeed, H., Salem, H. F., & Rabea, H. (2023). Therapeutic Outcomes of High Dose-Dexamethasone versus Prednisolone + Azathioprine, Rituximab, Eltrombopag, and Romiplostim Strategies in Persistent, Chronic, Refractory, and Relapsed Immune Thrombocytopenia Patients. Pharmaceuticals, 16(9), 1215. https://doi.org/10.3390/ph16091215