
Zoledronic Acid Ameliorates the Bone Turnover Activity and Periprosthetic Bone Preservation in Cementless Total Hip Arthroplasty

 , ,
, ,
Abstract
:
1. Introduction
2. Results
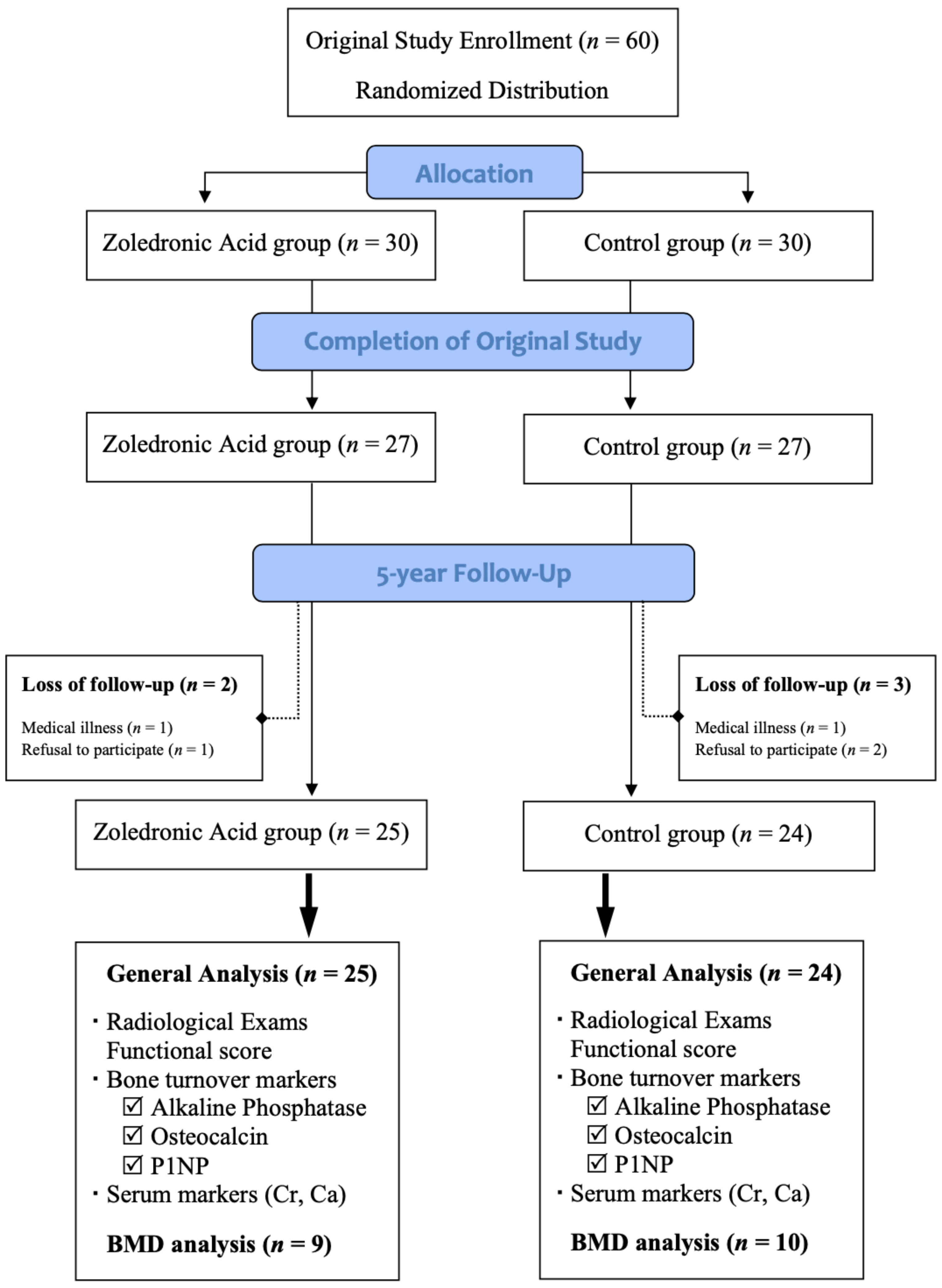
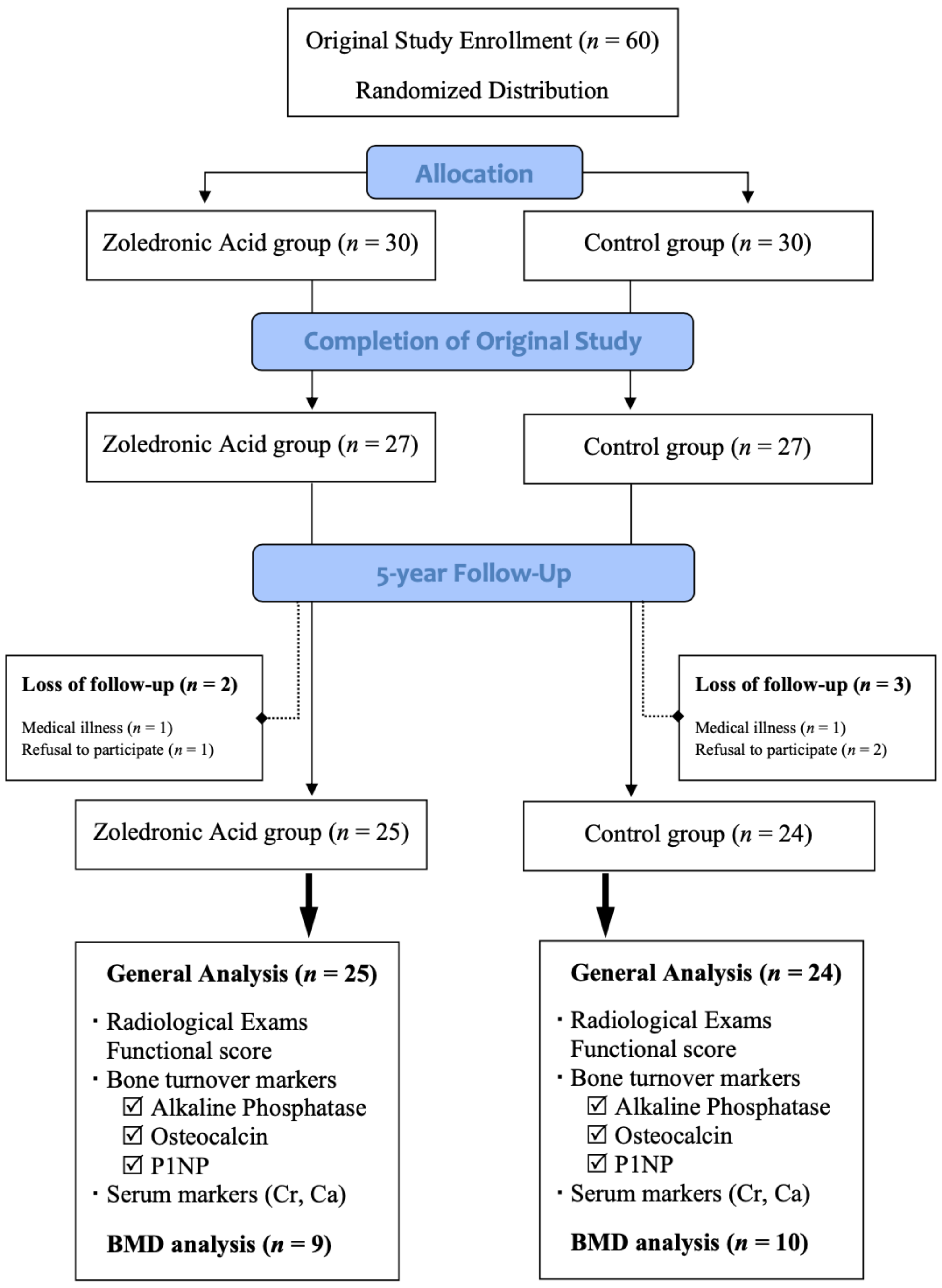
2.1. Patient Deposition
2.2. Functional Outcomes and Adverse Events
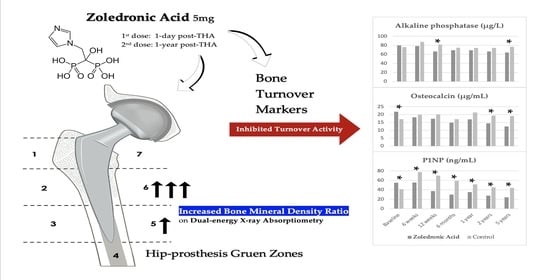
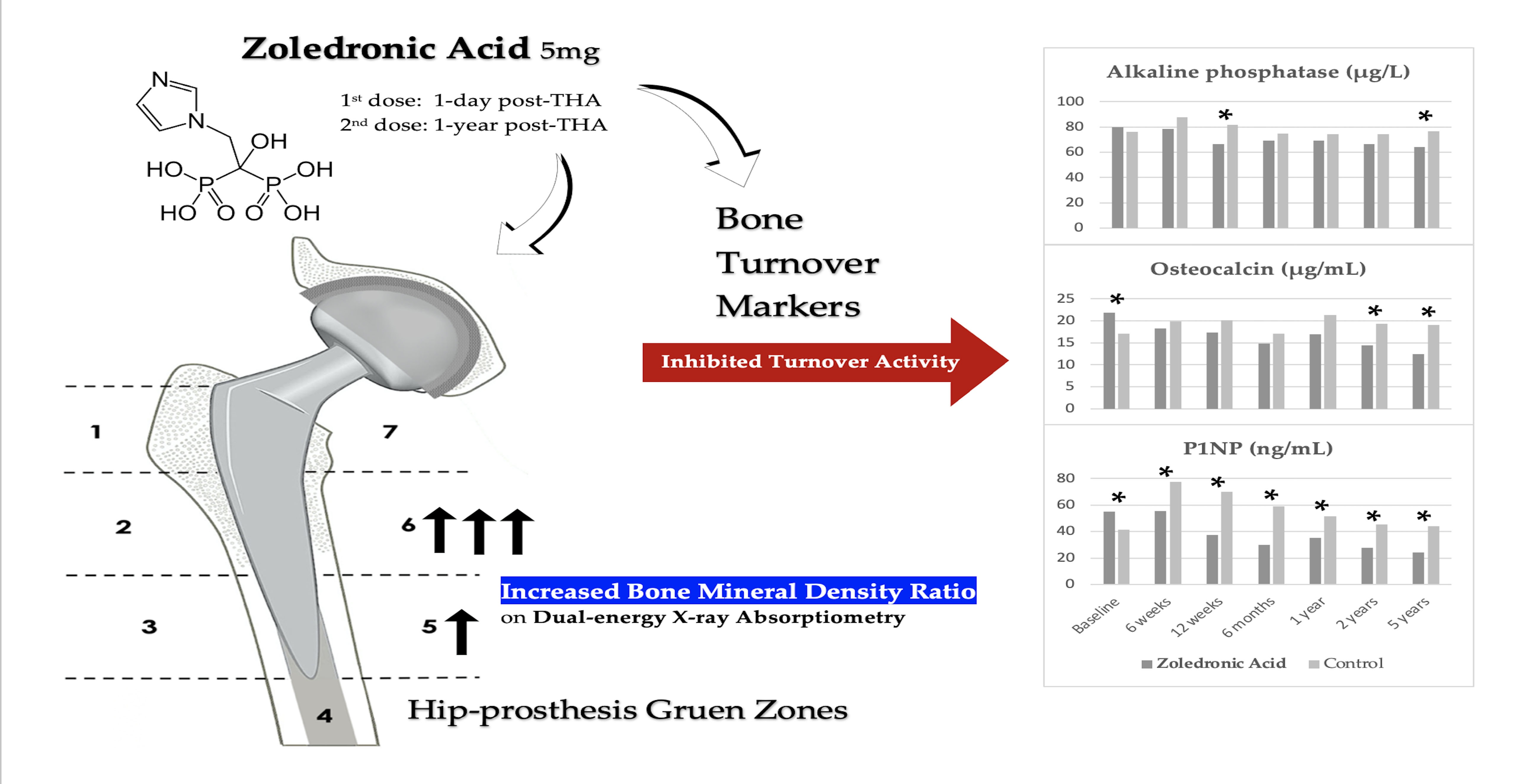
2.3. Serum Biomarkers and Bone Turnover Markers (BTMs)
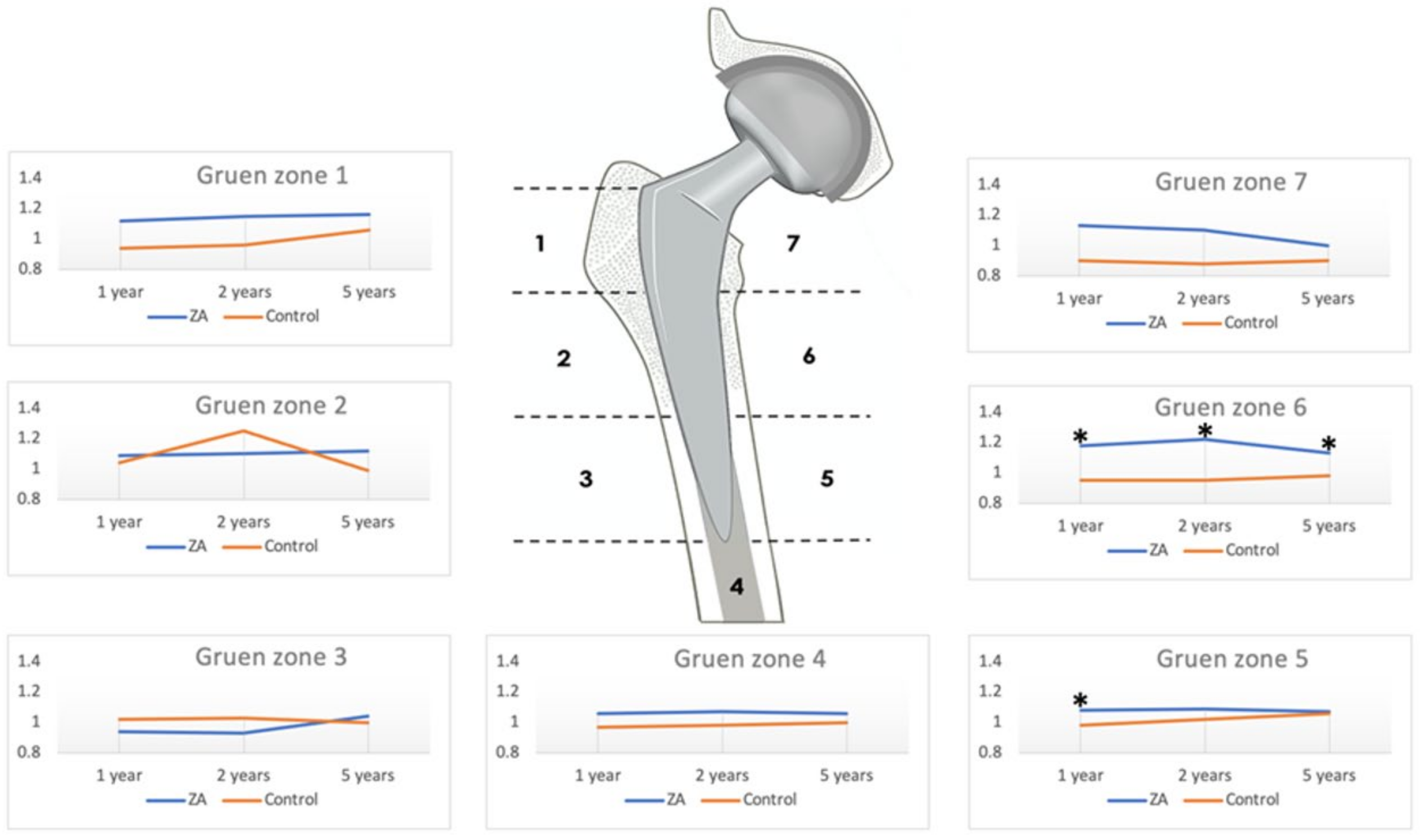
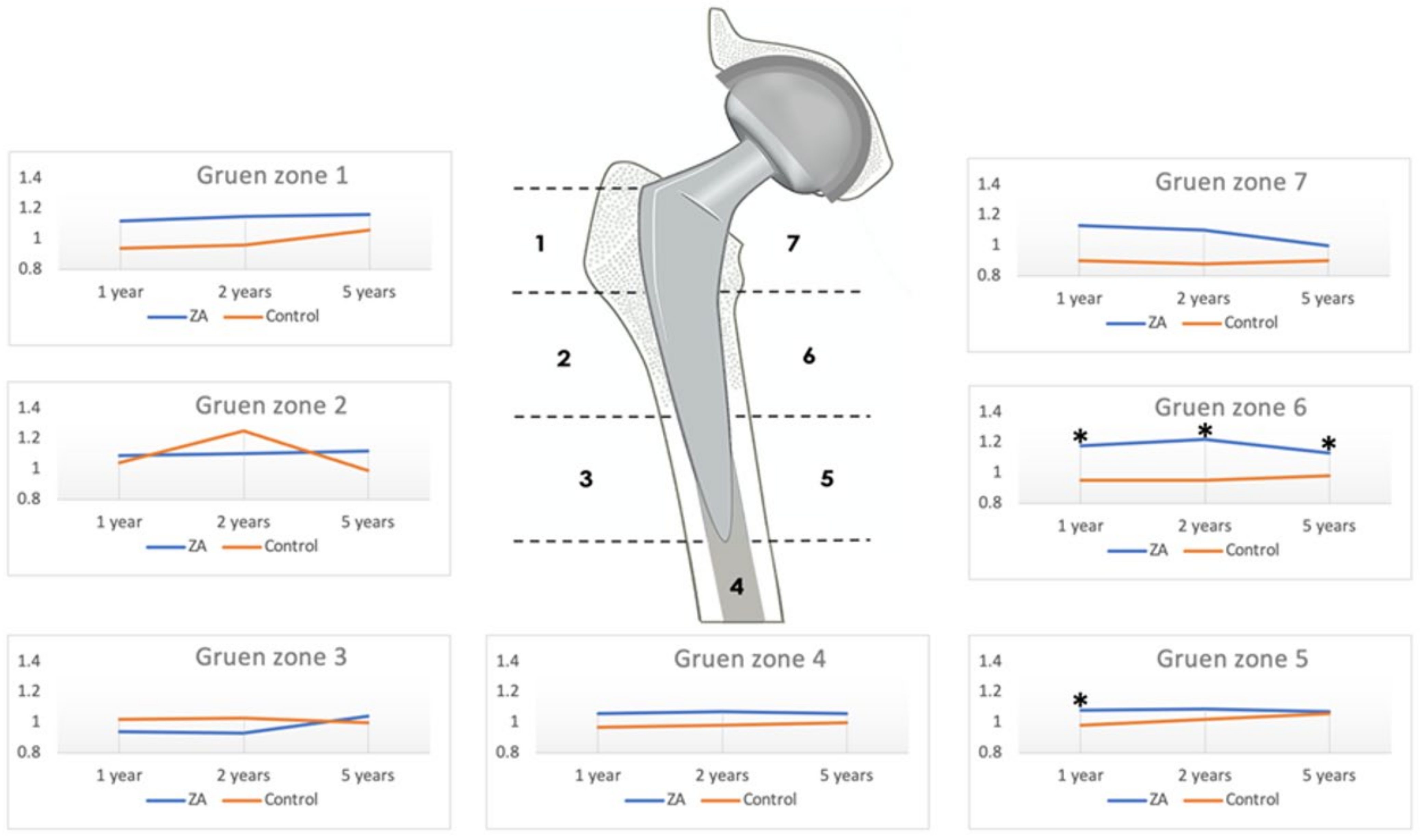
2.4. Periprosthetic Bone Mineral Density
2.5. Radiologic Evaluation
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Mc Clung, M.; Recker, R.; Miller, P.; Fiske, D.; Minkoff, J.; Kriegman, A.; Zhou, W.; Adera, M.; Davis, J. Intravenous zoledronic acid 5 mg in the treatment of postmenopausal women with low bone density previously treated with alendronate. Bone 2007, 41, 122–128. [Google Scholar] [CrossRef] [PubMed]
- Saag, K.; Lindsay, R.; Kriegman, A.; Beamer, E.; Zhou, W. A single zoledronic acid infusion reduces bone resorption markers more rapidly than weekly oral alendronate in postmenopausal women with low bone mineral density. Bone 2007, 40, 1238–1243. [Google Scholar] [CrossRef] [PubMed]
- Orwoll, E.S.; Binkley, N.C.; Lewiecki, E.M.; Gruntmanis, U.; Fries, M.A.; Dasic, G. Efficacy and safety of monthly ibandronate in men with low bone density. Bone 2010, 46, 970–976. [Google Scholar] [CrossRef] [PubMed]
- Russell, R.G.; Watts, N.B.; Ebetino, F.H.; Rogers, M.J. Mechanisms of action of bisphosphonates: Similarities and differences and their potential influence on clinical efficacy. Osteoporos. Int. 2008, 19, 733–759. [Google Scholar] [CrossRef]
- Black, D.M.; Reid, I.R.; Boonen, S.; Bucci-Rechtweg, C.; Cauley, J.A.; Cosman, F.; Cummings, S.R.; Hue, T.F.; Lippuner, K.; Lakatos, P.; et al. The effect of 3 versus 6 years of zoledronic acid treatment of osteoporosis: A randomized extension to the HORIZON-Pivotal Fracture Trial (PFT). J. Bone Miner. Res. 2012, 27, 243–254. [Google Scholar] [CrossRef] [PubMed]
- Oh, I.; Harris, W.H. Proximal strain distribution in the loaded femur. An in vitro comparison of the distributions in the intact femur and after insertion of different hip-replacement femoral components. J. Bone Jt. Surg. Am. 1978, 60, 75–85. [Google Scholar] [CrossRef]
- Aro, H.T.; Alm, J.J.; Moritz, N.; Makinen, T.J.; Lankinen, P. Low BMD affects initial stability and delays stem osseointegration in cementless total hip arthroplasty in women: A 2-year RSA study of 39 patients. Acta Orthop. 2012, 83, 107–114. [Google Scholar] [CrossRef]
- Skoldenberg, O.G.; Salemyr, M.O.; Boden, H.S.; Ahl, T.E.; Adolphson, P.Y. The effect of weekly risedronate on periprosthetic bone resorption following total hip arthroplasty: A randomized, double-blind, placebo-controlled trial. J. Bone Jt. Surg. Am. 2011, 93, 1857–1864. [Google Scholar] [CrossRef] [Green Version]
- Alm, J.J.; Makinen, T.J.; Lankinen, P.; Moritz, N.; Vahlberg, T.; Aro, H.T. Female patients with low systemic BMD are prone to bone loss in Gruen zone 7 after cementless total hip arthroplasty. Acta Orthop. 2009, 80, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Shi, J.; Liang, G.; Huang, R.; Liao, L.; Qin, D. Effects of bisphosphonates in preventing periprosthetic bone loss following total hip arthroplasty: A systematic review and meta-analysis. J. Orthop. Surg. Res. 2018, 13, 225. [Google Scholar] [CrossRef] [PubMed]
- Knusten, A.R.; Ebramzadeh, E.; Longjohn, D.B.; Sangiorgio, S.N. Systematic analysis of bisphosphonate intervention on periprosthetic BMD as a function of stem design. J. Arthroplast. 2014, 29, 1292–1297. [Google Scholar] [CrossRef]
- Lin, T.; Yan, S.G.; Cai, X.Z.; Ying, Z.M. Bisphosphonates for periprosthetic bone loss after joint arthroplasty: A meta-analysis of 14 randomized controlled trials. Osteoporos. Int. 2012, 23, 1823–1834. [Google Scholar] [CrossRef] [PubMed]
- Ott, S.M. What is the optimal duration of bisphosphonate therapy? Cleve. Clin. J. Med. 2011, 78, 619–630. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, M.; Bajammal, S.; Guyatt, G.H.; Griffith, L.; Busse, J.W.; Schunemann, H.; Einhorn, T.A. Effect of bisphosphonates on periprosthetic bone mineral density after total joint arthroplasty. A meta-analysis. J. Bone Jt. Surg. Am. 2005, 87, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Huang, T.W.; Wang, C.J.; Shih, H.N.; Chang, Y.; Huang, K.C.; Peng, K.T.; Lee, M.S. Bone turnover and periprosthetic bone loss after cementless total hip arthroplasty can be restored by zoledronic acid: A prospective, randomized, open-label, controlled trial. BMC Musculoskelet. Disord. 2017, 18, 209. [Google Scholar] [CrossRef] [PubMed]
- Scott, D.F.; Woltz, J.N.; Smith, R.R. Effect of zoledronic acid on reducing femoral bone mineral density loss following total hip arthroplasty: Preliminary results of a prospective randomized trial. J. Arthroplast. 2013, 28, 671–675. [Google Scholar] [CrossRef]
- Arabmotlagh, M.; Pilz, M.; Warzecha, J.; Rauschmann, M. Changes of femoral periprosthetic bone mineral density 6 years after treatment with alendronate following total hip arthroplasty. J. Orthop. Res. 2009, 27, 183–188. [Google Scholar] [CrossRef]
- Venesmaa, P.K.; Kroger, H.P.; Miettinen, H.J.; Jurvelin, J.S.; Suomalainen, O.T.; Alhava, E.M. Monitoring of periprosthetic BMD after uncemented total hip arthroplasty with dual-energy X-ray absorptiometry—A 3-year follow-up study. J. Bone Miner. Res. 2001, 16, 1056–1061. [Google Scholar] [CrossRef] [PubMed]
- Aro, E.; Moritz, N.; Mattila, K.; Aro, H.T. A long-lasting bisphosphonate partially protects periprosthetic bone, but does not enhance initial stability of uncemented femoral stems: A randomized placebo-controlled trial of women undergoing total hip arthroplasty. J. Biomech. 2018, 75, 35–45. [Google Scholar] [CrossRef]
- Johnston, R.C.; Fitzgerald, R.H.J.; Harris, W.H.; Poss, R.; Müller, M.E.; Sledge, C.B. Clinical and radiographic evaluation of total hip replacement. A standard system of terminology for reporting results. J. Bone Jt. Surg. A 1990, 72, 161–168. [Google Scholar] [CrossRef]
- Zhao, X.; Hu, D.; Qin, J.; Mohanan, R.; Chen, L. Effect of bisphosphonates in preventing femoral periprosthetic bone resorption after primary cementless total hip arthroplasty: A meta-analysis. J. Orthop. Surg. Res. 2015, 10, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nixon, M.; Taylor, G.; Sheldon, P.; Iqbal, S.J.; Harper, W. Does bone quality predict loosening of cemented total hip replacements? J. Bone Jt. Surg. Br. 2007, 89, 1303–1308. [Google Scholar] [CrossRef]
- Van der Voort, P.; Pijls, B.G.; Nieuwenhuijse, M.J.; Jasper, J.; Fiocco, M.; Plevier, J.W.; Middeldorp, S.; Valstar, E.R.; Nelissen, R.G. Early subsidence of shape-closed hip arthroplasty stems is associated with late revision. A systematic review and meta-analysis of 24 RSA studies and 56 survival studies. Acta Orthop. 2015, 86, 575–585. [Google Scholar] [CrossRef]
- Biver, E.; Chopin, F.; Coiffier, G.; Brentano, T.F.; Bouvard, B.; Garnero, P.; Cortet, B. Bone turnover markers for osteoporotic status assessment? A systematic review of their diagnosis value at baseline in osteoporosis. Jt. Bone Spine 2012, 79, 20–25. [Google Scholar] [CrossRef]
- Schousboe, J.T.; Bauer, D.C. Clinical use of bone turnover markers to monitor pharmacologic fracture prevention therapy. Curr. Osteoporos. Rep. 2012, 10, 56–63. [Google Scholar] [CrossRef] [Green Version]
- Garnero, P. Biomarkers for osteoporosis management: Utility in diagnosis, fracture risk prediction and therapy monitoring. Mol. Diagn. Ther. 2008, 12, 157–170. [Google Scholar] [CrossRef]
- Koivula, M.K.; Risteli, L.; Risteli, J. Measurement of aminoterminal propeptide of type I procollagen (PINP) in serum. Clin. Biochem. 2012, 45, 920–927. [Google Scholar] [CrossRef]
- Rogers, A.; Glover, S.J.; Eastell, R. A randomised, double-blinded, placebo-controlled, trial to determine the individual response in bone turnover markers to lasofoxifene therapy. Bone 2009, 45, 1044–1052. [Google Scholar] [CrossRef]
- Black, D.M.; Reid, I.R.; Cauley, J.A.; Cosman, F.; Leung, P.C.; Lakatos, P.; Lippuner, K.; Cummings, S.R.; Hue, T.F.; Mukhopadhyay, A.; et al. The effect of 6 versus 9 years of zoledronic acid treatment in osteoporosis: A randomized second extension to the HORIZON-Pivotal Fracture Trial (PFT). J. Bone Miner. Res. 2015, 30, 934–944. [Google Scholar] [CrossRef] [Green Version]
- Muren, O.; Akbarian, E.; Salemyr, M.; Boden, H.; Eisler, T.; Stark, A.; Skoldenberg, O. No effect of risedronate on femoral periprosthetic bone loss following total hip arthroplasty. A 4-year follow-up of 61 patients in a double-blind, randomized placebo-controlled trial. Acta Orthop. 2015, 86, 569–574. [Google Scholar] [CrossRef]
- Wang, C.J.; Wang, J.W.; Ko, J.Y.; Weng, L.H.; Huang, C.C. Three-year changes in bone mineral density around the knee after a six-month course of oral alendronate following total knee arthroplasty. A prospective, randomized study. J. Bone Jt. Surg. Am. 2006, 88, 267–272. [Google Scholar] [CrossRef]
- Shetty, N.; Hamer, A.; Stockley, I.; Eastell, R.; Willkinson, J. Clinical and radiological outcome of total hip replacement five years after pamidronate therapy: A trial extension. J. Bone Jt. Surg. Br. 2006, 88, 1309–1315. [Google Scholar] [CrossRef] [PubMed]
- Friedl, G.; Radl, R.; Stihsen, C.; Rehak, P.; Aigner, R.; Windhager, R. The effect of a single infusion of zoledronic acid on early implant migration in total hip arthroplasty. A randomized, double-blind, controlled trial. J. Bone Jt. Surg. Am. 2009, 91, 274–281. [Google Scholar] [CrossRef]
- Grey, A.; Bolland, M.J.; Horne, A.; Wattie, D.; House, M.; Gamble, G.; Reid, I.R. Five years of anti-resorptive activity after a single dose of zoledronate—Results from a randomized double-blind placebo-controlled trial. Bone 2012, 50, 1389–1393. [Google Scholar] [CrossRef]
- Reid, I.R.; Black, D.M.; Eastell, R.; Bucci-Rechtweg, C.; Su, G.; Hue, T.F.; Mesenbrink, P.; Lyles, K.W.; Boonen, S.; Trial, H.P.F.; et al. Reduction in the risk of clinical fractures after a single dose of zoledronic Acid 5 milligrams. J. Clin. Endocrinol. Metab. 2013, 98, 557–563. [Google Scholar] [CrossRef] [Green Version]
- Thillemann, T.M.; Pedersen, A.B.; Mehnert, F.; Johnsen, S.P.; Soballe, K. Postoperative use of bisphosphonates and risk of revision after primary total hip arthroplasty: A nationwide population-based study. Bone 2010, 46, 946–951. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Gong, H.S.; Kim, T.H.; Park, S.Y.; Shin, J.H.; Cho, S.W.; Byun, D.W. Position Statement: Drug Holiday in Osteoporosis Treatment with Bisphosphonates in South Korea. J. Bone Metab. 2015, 22, 167–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lamy, O.; Stoll, D.; Aubry-Rozier, B.; Rodriguez, E.G. Stopping Denosumab. Curr. Osteoporos. Rep. 2019, 17, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Tsourdi, E.; Zillikens, M.C. Certainties and Uncertainties About Denosumab Discontinuation. Calcif. Tissue Int. 2018, 103, 1–4. [Google Scholar] [CrossRef]
- Nebergall, A.K.; Rolfson, O.; Rubash, H.E.; Malchau, H.; Troelsen, A.; Greene, M.E. Stable Fixation of a Cementless, Proximally Coated, Double Wedged, Double Tapered Femoral Stem in Total Hip Arthroplasty: A 5-Year Radiostereometric Analysis. J. Arthroplast. 2016, 31, 1267–1274. [Google Scholar] [CrossRef]
- Berthon, B.S.; McLoughlin, R.F.; Jensen, M.E.; Hosseini, B.; Williams, E.J.; Baines, K.J.; Taylor, S.L.; Rogers, G.B.; Ivey, K.L.; Morten, M.; et al. The effects of increasing fruit and vegetable intake in children with asthma: A randomised controlled trial. Clin. Exp. Allergy 2021, 51, 1144–1156. [Google Scholar] [CrossRef]
- Engh, C.A.; Massin, P.; Suthers, K.E. Roentgenographic assessment of the biologic fixation of porous-surfaced femoral components. Clin. Orthop. Relat. Res. 1990, 257, 107–128. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Baseline | 6 Weeks | 12 Weeks | 6 Months | 1 Year | 2 Years | 5 Years | |
|---|---|---|---|---|---|---|---|
| Alkaline phosphatase (µg/L) | |||||||
| ZA | 79.8 (17.9) | 78.3 (19.4) | 66.6 (11.4) | 69.1 (27) | 69.4 (24.7) | 66.6 (17.5) | 64.3 (11.3) |
| Control | 76 (18.3) | 87.9 (21.9) | 81.9 (22.4) | 74.8 (20.6) | 74.6 (18.4) | 74.5 (15.6) | 76.7 (14.7) |
| p-value | 0.091 | 0.062 | 0.004 * | 0.095 | 0.088 | 0.060 | 0.002 * |
| Osteocalcin (µg/mL) | |||||||
| ZA | 21.9 (8.6) | 18.3 (8.2) | 17.3 (10.6) | 14.8 (5) | 16.9 (7.1) | 14.5 (7) | 12.5 (6.8) |
| Control | 17.1 (7.4) | 19.9 (12.2) | 20.1 (10.8) | 17.1 (5.4) | 21.3 (9.8) | 19.4 (8.5) | 19.1 (8.6) |
| p-value | 0.044 * | 0.11 | 0.083 | 0.087 | 0.078 | 0.034 * | 0.007 * |
| P1NP (procollagen 1 intact N-terminal) (ng/mL) | |||||||
| ZA | 55.2 (23.1) | 55.5 (22) | 37.5 (14.8) | 30 (12.2) | 35.2 (19.7) | 27.7 (11.4) | 24.3 (13.2) |
| Control | 41.3 (20.2) | 77.7 (39.3) | 70.2 (37.5) | 58.9 (25.1) | 51.6 (34) | 45.4 (19.6) | 44.1 (20.4) |
| p-value | 0.030 * | 0.020 * | 0.000 * | 0.000 * | 0.047 * | 0.001 * | 0.020 * |
| Baseline | 6 Weeks | 12 Weeks | 6 Months | 1 Year | 2 Years | 5 Years | |
|---|---|---|---|---|---|---|---|
| Creatinine (mg/dL) | |||||||
| ZA | 0.77 (0.21) | 0.74 (0.24) | 0.8 (0.28) | 0.84 (0.61) | 0.77 (0.25) | 0.78 (0.25) | 0.82 (0.27) |
| Control | 0.82 (0.2) | 0.79 (0.22) | 0.78 (0.18) | 0.78 (0.19) | 0.81 (0.2) | 0.81 (0.21) | 0.82 (0.21) |
| GFR (mL/min) | |||||||
| ZA | 59.7 (1.7) | 60.5 (4.8) | 62 (11.1) | 79.1 (27.7) | 84.8 (28.6) | 94.7 (22.6) | 90.8 (25.8) |
| Control | 59.8 (0.6) | 59.8 (1.2) | 63.6 (13.3) | 73.7 (24.1) | 81.4 (21.8) | 87.7 (18.4) | 85.9 (21) |
| Calcium (mg/dL) | |||||||
| ZA | 9.51 (0.5) | 9.27 (0.53) | 9.52 (0.45) | 9.44 (0.46) | 9.41 (0.48) | 9.37 (0.37) | 9.25 (0.4) |
| Control | 9.6 (0.43) | 9.16 (1.88) | 9.53 (0.37) | 9.43 (0.51) | 9.48 (0.36) | 9.28 (0.3) | 9.38 (0.42) |
| Gruen Zone | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| Baseline | |||||||
| ZA | 0.65 (0.12) | 1.26 (0.22) | 1.51 (0.38) | 1.66 (0.25) | 1.62 (0.22) | 1.26 (0.19) | 0.99 (0.17) |
| Control | 0.63 (0.16) | 1.28 (0.23) | 1.57 (0.25) | 1.69 (0.18) | 1.65 (0.21) | 1.30 (0.23) | 0.95 (0.25) |
| p-value | 0.767 | 0.806 | 0.708 | 0.784 | 0.761 | 0.703 | 0.713 |
| 1 year | |||||||
| ZA | 0.71 (0.08) | 1.39 (0.15) | 1.48 (0.35) | 1.76 (0.23) | 1.72 (0.17) | 1.43 (0.15) | 1.04 (0.20) |
| Control | 0.57 (0.20) | 1.30 (0.34) | 1.57 (0.30) | 1.62 (0.20) | 1.58 (0.17) | 1.19 (0.30) | 0.80 (0.29) |
| p-value | 0.072 | 0.437 | 0.552 | 0.199 | 0.096 | 0.047 * | 0.054 |
| 2 years | |||||||
| ZA | 0.70 (0. 80) | 1.37 (0.19) | 1.43 (0.36) | 1.75 (0.21) | 1.72 (0.16) | 1.46 (0.13) | 0.99 (0.13) |
| Control | 0.57 (0.14) | 1.60 (1.06) | 1.58 (0.23) | 1.63 (0.20) | 1.64 (0.21) | 1.21 (0.28) | 0.79 (0.23) |
| p-value | 0.033 * | 0.552 | 0.290 | 0.278 | 0.388 | 0.032 * | 0.043 * |
| 5 years | |||||||
| ZA | 0.72 (0.10) | 1.41 (0.14) | 1.61 (0.14) | 1.76 (0.19) | 1.72 (0.16) | 1.38 (0.21) | 0.93 (0.27) |
| Control | 0.63 (0.16) | 1.23 (0.28) | 1.52 (0.20) | 1.66 (0.21) | 1.71 (0.26) | 1.24 (0.26) | 0.81 (0.21) |
| p-value | 0.154 | 0.098 | 0.317 | 0.305 | 0.962 | 0.239 | 0.297 |
| Gruen Zone | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| 1 year | |||||||
| ZA | 1.12 (0.28) | 1.09 (0.11) | 0.94 (0.21) | 1.06 (0.13) | 1.08 (0.11) | 1.18 (0.18) | 1.13 (0.31) |
| Control | 0.94 (0.22) | 1.04 (0.20) | 1.02 (0.14) | 0.97(0.08) | 0.98 (0.07) | 0.95 (0.23) | 0.90 (0.32) |
| p-value | 0.140 | 0.202 | 0.958 | 0.116 | 0.026 * | 0.031 * | 0.094 |
| 2 years | |||||||
| ZA | 1.15 (0.33) | 1.10 (0.12) | 0.93 (0.23) | 1.07 (0.18) | 1.09 (0.13) | 1.22 (0.16) | 1.10 (0.29) |
| Control | 0.96 (0.14) | 1.25 (0.64) | 1.03 (0.09) | 0.98 (0.08) | 1.02 (0.06) | 0.95 (0.18) | 0.88 (0.25) |
| p-value | 0.114 | 0.524 | 0.233 | 0.097 | 0.234 | 0.005 * | 0.109 |
| 5 years | |||||||
| ZA | 1.16 (0.36) | 1.12 (0.17) | 1.04 (0.17) | 1.06 (0.12) | 1.07 (0.12) | 1.13 (0.16) | 1.00 (0.34) |
| Control | 1.06 (0.27) | 0.99 (0.19) | 1.00 (0.14) | 1.00 (0.09) | 1.06 (0.10) | 0.98 (0.11) | 0.90 (0.19) |
| p-value | 0.485 | 0.158 | 0.596 | 0.190 | 0.811 | 0.032 * | 0.465 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, A.H.S.; Yen, C.-H.; Kuo, F.-C.; Wu, C.-T.; Huang, T.-W.; Cheng, J.-T.; Lee, M.S. Zoledronic Acid Ameliorates the Bone Turnover Activity and Periprosthetic Bone Preservation in Cementless Total Hip Arthroplasty. Pharmaceuticals 2022, 15, 420. https://doi.org/10.3390/ph15040420
Hsu AHS, Yen C-H, Kuo F-C, Wu C-T, Huang T-W, Cheng J-T, Lee MS. Zoledronic Acid Ameliorates the Bone Turnover Activity and Periprosthetic Bone Preservation in Cementless Total Hip Arthroplasty. Pharmaceuticals. 2022; 15(4):420. https://doi.org/10.3390/ph15040420
Chicago/Turabian StyleHsu, Allen Herng Shouh, Chun-Hsien Yen, Feng-Chih Kuo, Cheng-Ta Wu, Tsan-Wen Huang, Juei-Tang Cheng, and Mel S. Lee. 2022. "Zoledronic Acid Ameliorates the Bone Turnover Activity and Periprosthetic Bone Preservation in Cementless Total Hip Arthroplasty" Pharmaceuticals 15, no. 4: 420. https://doi.org/10.3390/ph15040420
APA StyleHsu, A. H. S., Yen, C.-H., Kuo, F.-C., Wu, C.-T., Huang, T.-W., Cheng, J.-T., & Lee, M. S. (2022). Zoledronic Acid Ameliorates the Bone Turnover Activity and Periprosthetic Bone Preservation in Cementless Total Hip Arthroplasty. Pharmaceuticals, 15(4), 420. https://doi.org/10.3390/ph15040420