
A Sex- and Gender-Based Analysis of Adverse Drug Reactions: A Scoping Review of Pharmacovigilance Databases


 , ,
, ,
Abstract
1. Introduction
2. Background
3. Methods
3.1. Search Strategy
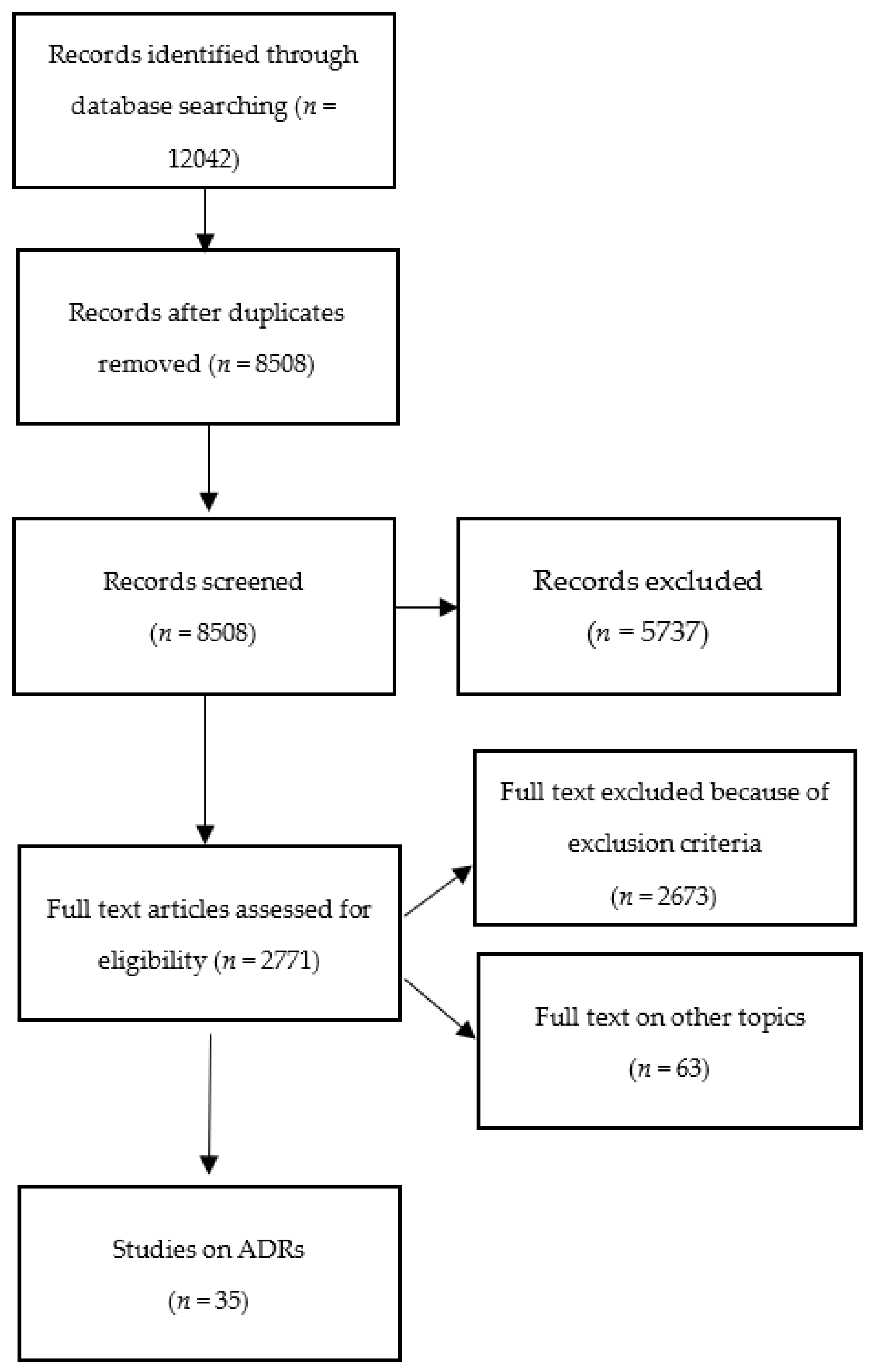
3.2. Literature Screening and Study Selection
3.3. Data Extraction
3.4. Sex- and Gender-Based Analysis of the Included Papers
4. Results
4.1. Study Characteristics
4.2. Drugs Associated with ADRs
4.3. ADR Reporting and Sex in Different Databases
5. Discussion
6. Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Uppsala Monitoring Centre. Glossary of Pharmacovigilance Terms; Uppsala Monitoring Centre: Uppsala, Sweden, 2021. [Google Scholar]
- Wiktorowicz, M.; Lexchin, J.; Moscou, K.; Silversides, A.; Eggertson, L. Keeping an Eye on Prescription Drugs, Keeping Canadians Safe; Health Council of Canada: Toronto, ON, Canada, 2010. [Google Scholar]
- Van Der Linden, C.M.; Jansen, P.A.; Van Marum, R.J.; Grouls, R.J.; Korsten, E.H.; Egberts, A.C. Recurrence of adverse drug reactions following inappropriate re-prescription: Better documentation, availability of information and monitoring are needed. Drug Saf. 2010, 33, 535–538. [Google Scholar] [CrossRef] [PubMed]
- Hazell, L.; Shakir, S.A. Under-reporting of adverse drug reactions: A systematic review. Drug Saf. 2006, 29, 385–396. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. Mandatory Reporting of Serious Adverse Drug Reactions and Medical Device Incidents by Hospitals. 2019. Available online: https://www.canada.ca/en/health-canada/services/drugs-health-products/medeffect-canada/adverse-reaction-reporting/mandatory-hospital-reporting/drugs-devices.html (accessed on 17 December 2021).
- Bailey, C.; Peddie, D.; Wickham, M.E.; Badke, K.; Small, S.S.; Doyle-Waters, M.M.; Balka, E.; Hohl, C.M. Adverse drug event reporting systems: A systematic review. Br. J. Clin. Pharmacol. 2016, 82, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, P.; Singh, A. Comparative evaluation of adverse drug reaction reporting forms for introduction of a spontaneous generic ADR form. J. Pharmacol. Pharmacother. 2012, 3, 228–232. [Google Scholar] [CrossRef]
- US Government Accountability Office (GAO). Drug Safety: Most Drugs Withdrawn in Recent Years Had Greater Health Risks for Women; General Accounting Office-01-286R; US Government Accountability Office (GAO): Washington, DC, USA, 2001.
- Johnson, J.L.; Greaves, L.; Repta, R. Better Science with Sex and Gender: A Primer for Health Research; Women’s Health Research Network: Vancouver, BC, Canada, 2007.
- Krieger, N. Genders, sexes, and health: What are the connections—And why does it matter? Int. J. Epidemiol. 2003, 32, 652–657. [Google Scholar] [CrossRef]
- Lippman, A. The Inclusion of Women in Clinical Trials: Are We Asking the Right Questions? Women and Health Protection: Toronto, ON, Canada, 2006.
- Yakerson, A. Women in clinical trials: A review of policy development and health equity in the Canadian context. Int. J. Equity Health 2019, 18, 56. [Google Scholar] [CrossRef] [PubMed]
- Welch, V.; Doull, M.; Yoganathan, M.; Jull, J.; Boscoe, M.; Coen, S.E.; Marshall, Z.; Pardo, J.P.; Pederson, A.; Petkovic, J.; et al. Reporting of sex and gender in randomized controlled trials in Canada: A cross-sectional methods study. Res. Integr. Peer Rev. 2017, 2, 15. [Google Scholar] [CrossRef] [PubMed]
- Parekh, A.; O Fadiran, E.; Uhl, K.; Throckmorton, D.C. Adverse effects in women: Implications for drug development and regulatory policies. Expert Rev. Clin. Pharmacol. 2011, 4, 453–466. [Google Scholar] [CrossRef] [PubMed]
- Beierle, I.; Meibohm, B.; Derendorf, H. Gender differences in pharmacokinetics and pharmacodynamics. Int. J. Clin. Pharmacol. Ther. 1999, 37, 529–547. [Google Scholar] [PubMed]
- Greenblatt, D.J.; von Moltke, L.L. Gender has a small but statistically significant effect on clearance of CYP3A substrate drugs. J. Clin. Pharmacol. 2008, 48, 1350–1355. [Google Scholar] [CrossRef]
- Anderson, G.D. Chapter 1 Gender Differences in Pharmacological Response. In International Review of Neurobiology; Academic Press: Cambridge, MA, USA, 2008; pp. 1–10. [Google Scholar] [CrossRef]
- Islam, M.; Iqbal, U.; Walther, B.A.; Nguyen, P.A.; Li, Y.C.J.; Dubey, N.K.; Poly, T.N.; Masud, J.H.B.; Atique, S.; Syed-Abdul, S. Gender-based personalized pharmacotherapy: A systematic review. Arch. Gynecol. Obstet. 2017, 295, 1305–1317. [Google Scholar] [CrossRef]
- Zucker, I.; Prendergast, B.J. Sex differences in pharmacokinetics predict adverse drug reactions in women. Biol. Sex Differ. 2020, 11, 32. [Google Scholar] [CrossRef]
- Gustafson, P.E. Gender Differences in Risk Perception: Theoretical and Methodological Perspectives. Risk Anal. 1998, 18, 805–811. [Google Scholar] [CrossRef] [PubMed]
- Ek, S. Gender differences in health information behaviour: A Finnish population-based survey. Health Promot. Int. 2015, 30, 736–745. [Google Scholar] [CrossRef] [PubMed]
- Arksey, H.; O’Malley, L. Scoping studies: Towards a methodological framework. Int. J. Soc. Res. Methodol. 2005, 8, 19–32. [Google Scholar] [CrossRef]
- Levac, D.; Colquhoun, H.; O’Brien, K.K. Scoping studies: Advancing the methodology. Implement. Sci. 2010, 5, 69. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Brabete, A.C.; Greaves, L.; Hemsing, N.; Stinson, J. Sex- and Gender-Based Analysis in Cannabis Treatment Outcomes: A Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 872. [Google Scholar] [CrossRef]
- Bondon-Guitton, E.; Mourgues, T.; Rousseau, V.; Cousty, S.; Cottin, J.; Drablier, G.; Micallef, J.; Montastruc, J.-L. Gingival bleeding, a possible “serious” adverse drug reaction: An observational study in the French PharmacoVigilance Database. J. Clin. Periodontol. 2017, 44, 898–904. [Google Scholar] [CrossRef]
- Castellana, E.; Chiappetta, M.R.; Cattel, F. Gender differences and pharmacovigilance: Analysis in the Italian population. Ital. J. Gend.-Specif. Med. 2018, 4, 27–33. [Google Scholar]
- Chavant, F.; Favrelière, S.; Lafay-Chebassier, C.; Plazanet, C.; Pérault-Pochat, M.-C. Memory disorders associated with consumption of drugs: Updating through a case/noncase study in the French PharmacoVigilance Database. Br. J. Clin. Pharmacol. 2011, 72, 898–904. [Google Scholar] [CrossRef] [PubMed]
- Chrétien, B.; Dolladille, C.; Hamel-Sénécal, L.; Sassier, M.; Faillie, J.L.; Miremont-Salamé, G.; Lelong-Boulouard, V.; Le Boisselier, R.; Fedrizzi, S.; Alexandre, J.; et al. Comparative study of hypoglycaemia induced by opioids. Is it a class effect? Expert Opin. Drug Saf. 2019, 18, 987–992. [Google Scholar] [CrossRef] [PubMed]
- De Vries, S.T.; Denig, P.; Ekhart, C.; Mol, P.G.; van Puijenbroek, E.P. Sex Differences in Adverse Drug Reactions of Metformin: A Longitudinal Survey Study. Drug Saf. 2020, 43, 489–495. [Google Scholar] [CrossRef] [PubMed]
- De Vries, S.T.; Denig, P.; Ekhart, C.; Burgers, J.S.; Kleefstra, N.; Mol, P.G.; van Puijenbroek, E.P. Sex differences in adverse drug reactions reported to the National Pharmacovigilance Centre in the Netherlands: An explorative observational study. Br. J. Clin. Pharmacol. 2019, 85, 1507–1515. [Google Scholar] [CrossRef] [PubMed]
- Dubrall, D.; Just, K.S.; Schmid, M.; Stingl, J.C.; Sachs, B. Adverse drug reactions in older adults: A retrospective comparative analysis of spontaneous reports to the German Federal Institute for Drugs and Medical Devices. BMC Pharmacol. Toxicol. 2020, 21, 25. [Google Scholar] [CrossRef] [PubMed]
- Ehrenpreis, E.D.; Parakkal, D.; Semer, R.; Du, H. Renal risks of sodium phosphate tablets for colonoscopy preparation: A review of adverse drug reactions reported to the US Food and Drug Administration. Color. Dis. 2011, 13, e270–e275. [Google Scholar] [CrossRef] [PubMed]
- Ekhart, C.; Van Hunsel, F.; Scholl, J.; De Vries, S.; Van Puijenbroek, E. Sex Differences in Reported Adverse Drug Reactions of Selective Serotonin Reuptake Inhibitors. Drug Saf. 2018, 41, 677–683. [Google Scholar] [CrossRef] [PubMed]
- Faye, E.; Centers, T.F.N.O.R.P.; Bondon-Guitton, E.; Olivier-Abbal, P.; Montastruc, J.-L. Spontaneous reporting of serious cutaneous reactions with protein kinase inhibitors. Eur. J. Clin. Pharmacol. 2013, 69, 1819–1826. [Google Scholar] [CrossRef]
- Holm, L.; Ekman, E.; Blomgren, K.J. Influence of age, sex and seriousness on reporting of adverse drug reactions in Sweden. Pharmacoepidemiol. Drug Saf. 2017, 26, 335–343. [Google Scholar] [CrossRef]
- Jia, Y.; Zhu, C.; Du, J.; Xiang, Y.; Chen, Y.; Wang, W.; Tao, C. Investigating safety profiles of human papillomavirus vaccine across group differences using VAERS data and MedDRA. PeerJ 2019, 7, e7490. [Google Scholar] [CrossRef]
- Du, J.; Cai, Y.; Chen, Y.; He, Y.; Tao, C. Analysis of Individual Differences in Vaccine Pharmacovigilance Using VAERS Data and MedDRA System Organ Classes: A Use Case Study with Trivalent Influenza Vaccine. Biomed. Inform. Insights 2017, 9, 1178222617700627. [Google Scholar] [CrossRef] [PubMed]
- Lindsey, N.P.; Rabe, I.B.; Miller, E.R.; Fischer, M.; Staples, J.E. Adverse event reports following yellow fever vaccination, 2007–2013. J. Travel Med. 2016, 23, taw045. [Google Scholar] [CrossRef] [PubMed]
- Lowe, G.; Costabile, R.A. 10-Year Analysis of Adverse Event Reports to the Food and Drug Administration for Phosphodiesterase Type-5 Inhibitors. J. Sex. Med. 2012, 9, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Luk, C.P.; Parsons, R.; Lee, Y.P.; Hughes, J.D. Proton Pump Inhibitor–Associated Hypomagnesemia: What Do FDA Data Tell Us? Ann. Pharmacother. 2013, 47, 773–780. [Google Scholar] [CrossRef] [PubMed]
- Macedo, A.F.; Alves, C.; Craveiro, N.; Marques, F.B. Multiple drug exposure as a risk factor for the seriousness of adverse drug reactions. J. Nurs. Manag. 2011, 19, 395–399. [Google Scholar] [CrossRef] [PubMed]
- McDonald, D.D. Predictors of gastrointestinal bleeding in older persons taking nonsteroidal anti-inflammatory drugs: Results from the FDA adverse events reporting system. J. Am. Assoc. Nurse Pract. 2019, 31, 206–213. [Google Scholar] [CrossRef] [PubMed]
- McLernon, D.J.; Bond, C.M.; Hannaford, P.C.; Watson, M.C.; Lee, A.J.; Hazell, L.; Avery, A. Adverse drug reaction reporting in the UK: A retrospective observational comparison of yellow card reports submitted by patients and healthcare professionals. Drug Saf. 2010, 33, 775–788. [Google Scholar] [CrossRef] [PubMed]
- McNeil, M.M.; Paradowska-Stankiewicz, I.; Miller, E.R.; Marquez, P.L.; Seshadri, S.; Collins, L.C.; Cano, M.V. Adverse events following adenovirus type 4 and type 7 vaccine, live, oral in the Vaccine Adverse Event Reporting System (VAERS), United States, October 2011–July 2018. Vaccine 2019, 37, 6760–6767. [Google Scholar] [CrossRef]
- McNeil, M.M.; Arana, J.; Stewart, B.; Hartshorn, M.; Hrncir, D.; Wang, H.; Lamias, M.; Locke, M.; Stamper, J.; Tokars, J.I.; et al. A cluster of nonspecific adverse events in a military reserve unit following pandemic influenza A (H1N1) 2009 vaccination—Possible stimulated reporting? Vaccine 2012, 30, 2421–2426. [Google Scholar] [CrossRef]
- Mertes, P.M.; Alla, F.; Tréchot, P.; Auroy, Y.; Jougla, E. Anaphylaxis during anesthesia in France: An 8-year national survey. J. Allergy Clin. Immunol. 2011, 128, 366–373. [Google Scholar] [CrossRef] [PubMed]
- Nevin, R.L.; Leoutsakos, J.-M. Identification of a Syndrome Class of Neuropsychiatric Adverse Reactions to Mefloquine from Latent Class Modeling of FDA Adverse Event Reporting System Data. Drugs RD 2017, 17, 199–210. [Google Scholar] [CrossRef] [PubMed][Green Version]
- O’Donovan, B.; Rodgers, R.M.; Cox, A.R.; Krska, J. Making medicines safer: Analysis of patient reports to the UK’s Yellow Card Scheme. Expert Opin. Drug Saf. 2019, 18, 1237–1243. [Google Scholar] [CrossRef] [PubMed]
- Ordoñez, L.; Salgueiro, E.; Jimeno, F.J.; Manso, G. Spontaneous reporting of Stevens-Johnson syndrome and toxic epidermal necrolysis associated with antiepileptic drugs. Eur. Rev. Med. Pharmacol. Sci. 2015, 19, 2732–2737. [Google Scholar]
- Reitter, M.; Petitpain, N.; Latarche, C.; Cottin, J.; Massy, N.; Demoly, P.; Gillet, P.; Mertes, P.M.; Centres, T.F.N.O.R.P. Fatal anaphylaxis with neuromuscular blocking agents: A risk factor and management analysis. Allergy 2014, 69, 954–959. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro-Vaz, I.; Marques, J.; Demoly, P.; Polonia, J.; Gomes, E. Drug-induced anaphylaxis: A decade review of reporting to the Portuguese Pharmacovigilance Authority. Eur. J. Clin. Pharmacol. 2012, 69, 673–681. [Google Scholar] [CrossRef]
- Ronaldson, K.J.; Fitzgerald, P.B.; Taylor, A.J.; Topliss, D.J.; McNeil, J.J. Clinical course and analysis of ten fatal cases of clozapine-induced myocarditis and comparison with 66 surviving cases. Schizophr. Res. 2011, 128, 161–165. [Google Scholar] [CrossRef] [PubMed]
- Rydberg, D.M.; Mejyr, S.; Loikas, D.; Schenck-Gustafsson, K.; Von Euler, M.; E Malmström, R. Sex differences in spontaneous reports on adverse drug events for common antihypertensive drugs. Eur. J. Clin. Pharmacol. 2018, 74, 1165–1173. [Google Scholar] [CrossRef] [PubMed]
- Rydberg, D.M.; Holm, L.; Mejyr, S.; Loikas, D.; Schenck-Gustafsson, K.; von Euler, M.; Wettermark, B.; Malmström, R.E. Sex differences in spontaneous reports on adverse bleeding events of antithrombotic treatment. Eur. J. Clin. Pharmacol. 2014, 70, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Serebruany, V.L.; Tomek, A.; Kim, M.H.; Litvinov, O.; Marciniak, T.A. Aspirin in the Food and Drug Administration Adverse Event Reporting System: Missing Demographics and Underreporting. TH Open 2017, 1, e101–e105. [Google Scholar] [CrossRef][Green Version]
- Tkachenko, E.; Singer, S.; Sharma, P.; Barbieri, J.; Mostaghimi, A. US Food and Drug Administration Reports of Pregnancy and Pregnancy-Related Adverse Events Associated with Isotretinoin. JAMA Dermatol. 2019, 155, 1175–1179. [Google Scholar] [CrossRef] [PubMed]
- Tkachenko, E.; Singer, S.B.; Sharma, P.; Barbieri, J.; Mostaghimi, A. FDA Reports of Alopecia as an Adverse Event to Isotretinoin. J. Cutan. Med. Surg. 2019, 23, 451–452. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Yu, Q.; Li, Q. Differences in reproductive toxicology between alopecia drugs: An analysis on adverse events among female and male cases. Oncotarget 2016, 7, 82074–82084. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Dingcheng, L.; Li, D.; Wang, L.; Wang, W.; Liu, H. Systematic Analysis of Adverse Event Reports for Sex Differences in Adverse Drug Events. Sci. Rep. 2016, 6, 24955. [Google Scholar] [CrossRef] [PubMed]
- De Jong, L.; Härmark, L.; van Puijenbroek, E. Time course, outcome and management of adverse drug reactions associated with metformin from patient’s perspective: A prospective, observational cohort study in the Netherlands. Eur. J. Clin. Pharmacol. 2016, 72, 615–622. [Google Scholar] [CrossRef]
- Franconi, F.; Campesi, I. Pharmacogenomics, pharmacokinetics and pharmacodynamics: Interaction with biological differences between men and women. J. Cereb. Blood Flow Metab. 2014, 171, 580–594. [Google Scholar] [CrossRef]
- Soldin, O.P.; Mattison, D. Sex Differences in Pharmacokinetics and Pharmacodynamics. Clin. Pharmacokinet. 2009, 48, 143–157. [Google Scholar] [CrossRef] [PubMed]
- Tannenbaum, C.; Day, D. Age and sex in drug development and testing for adults. Pharmacol. Res. 2017, 121, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Fadiran, E.O.; Zhang, L. Effects of Sex Differences in the Pharmacokinetics of Drugs and Their Impact on the Safety of Medicines in Women. Med. Women 2014, 41–68. [Google Scholar] [CrossRef]
- Farkas, R.H.; Unger, E.F.; Temple, R. Zolpidem and Driving Impairment—Identifying Persons at Risk. N. Engl. J. Med. 2013, 369, 689–691. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, G. Adverse drug reactions: Classification, susceptibility and reporting. Nurs. Stand. 2016, 30, 53–63. [Google Scholar] [CrossRef] [PubMed]
- Dinh, Q.Q.; Sinclair, R. Female pattern hair loss: Current treatment concepts. Clin. Interv. Aging 2007, 2, 189–199. [Google Scholar]
- Hunt, N.; McHale, S. The psychological impact of alopecia. BMJ 2005, 331, 951–953. [Google Scholar] [CrossRef]
- ICH. Clinical Safety Data Management: Definitions and Standards for Expedited Reporting E2A; ICH (International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use): Geneva, Switzerland, 1995. [Google Scholar]


{kind=link}
| Author(s) and Year | Country | Study Design | Research Aim | Drug(s) | SGBA+ |
|---|---|---|---|---|---|
| Bondon-Guitton et al. (2017) [26] | France | Cross-sectional | To identify the drugs most frequently suspected in the occurrence of gingival bleeding | Discovering which drugs are associated with gingival bleeding was the main outcome. Among drugs known to increase the risk of gingival bleeding, the most frequently involved were fluindione, furosemide, paracetamol, amiodarone, amoxicillin, paroxetine, or ketoprofen. The authors also identified signals for drugs not usually known to be involved in bleeding, like zolpidem, enalapril, or ramipril | Sex-disaggregated outcomes (no testing for significance) |
| Castellana et al. (2018) [27] | Italy | Cross-sectional | To investigate the gender-related differences in adverse drug reactions (ADRs) in the Italian population, on the basis of sex, during a 15-year observation period | The most-reported ATCs (Anatomic, Therapeutic, Chemical Classification): protease inhibitors, reverse transcriptase nucleoside inhibitors, thyroid hormones, aminoquinoline antimalarials, COX-inhibitor anti-inflammatory and antirheumatic drugs, selective serotonin reuptake inhibitor antidepressants, benzodiazepine derivative anxiolytics, acetic acid derivative anti-inflammatory and antirheumatic drugs and related substances, broad-spectrum penicillins, penicillin associations including beta-lactamase inhibitors and propionic acid derivative anti-inflammatory and antirheumatic drugs | Sex-disaggregated outcomes (%) (no testing for significance) |
| Chavant et al. (2011) [28] | France | Cross-sectional | To examine which drugs are associated with memory disorders | The main therapeutic classes suspected were hypnotics (76 cases), anticonvulsants (68 cases), anxiolytics (66 cases), antidepressants (55 cases), analgesics (45 cases), and antipsychotic drugs (29 cases) | Sex-disaggregated outcomes (no testing for significance) |
| Chretien et al. (2019) [29] | France | Cross-sectional | To determine if drug-induced hypoglycemia could be a class effect for opioids | Opioids (codeine, fentanyl, hydromorphone, methadone, morphine, oxycodone, tramadol, buprenorphine, and nalbuphine) | Sex-disaggregated outcomes (no testing for significance) |
| De Vries et al. (2020) [30] | Netherlands | Cohort study (prospective or retrospective) | To assess whether sex differences in reported adverse drug reactions (ADRs) for metformin are observed at different times after initiation and to explore their concurrence with sex differences in the dose of metformin over time | Metformin | Sex-disaggregated outcomes and testing for significance |
| de Vries et al. (2019) [31] | Netherlands | Cross-sectional | To assess sex differences in adverse drug reactions (ADRs) reported to the national pharmacovigilance center in the Netherlands, taking sex differences in the number of drug users into account. The secondary aims of this study were to assess for which drugs and for which ADRs sex differences were identified most often | 74 different drugs from many different classes were identified as having a potentially significant sex difference in experiences ADRs | Sex-disaggregated outcomes and testing for significance |
| Dubrall et al. (2020) [32] | Germany | Cross-sectional | The first aim of the study was to determine the number of ADR reports regarding older adults (>65 years) and to set these reports in relation to (i) the number of spontaneous ADR reports regarding younger adults (19–65) and (ii) the number of inhabitants and assumed drug-exposed inhabitants, and to oppose the ADR reports to the number of defined daily doses (DDD) used per insured person. The second aim was to analyze if some of the reported characteristics are more often described in the ADR reports of older adults compared to younger adults | The ten drug classes most frequently suspected in older adults: antithrombotic agents, antineoplastic agents, antiphlogistics and antirheumatics, systemic antibiotics, agents acting on the renin–angiotensin system, psycholanaleptics, psycholeptics, lipid-modifying agents, antidiabetics, and analgesics. The ten drug classes most frequently suspected in psycholeptics, systemic antibiotics, antineoplastic agents, psychoanaleptics, immunostimulants, antithrombotic agents, immunosuppressives, sex hormones, antiepileptics, antiphlogistics, and antirheumatics | Sex-disaggregated outcomes and testing for significance |
| Ehrenpreis et al. (2011) [33] | USA | Cross-sectional | To analyze renal risks of sodium phosphate tablets, especially the role of body weight and gender as risk factors for renal complications | Sodium-phosphate-containing colonoscopy preparations, such as sodium phosphate tablets sold as OsmoPrep and Visicol, as well as polyethylene glycol (PEG) colonoscopy preparations | Sex-disaggregated outcomes (no testing for significance) |
| Ekhart et al. (2018) [34] | Netherlands | Cross-sectional | To investigate whether reports of adverse drug reactions (ADRs) when using selective serotonin reuptake inhibitors (SSRIs) concern women and men equally in the database of the Netherlands Pharmacovigilance Centre Lareb, taking into account the differences in the number of users. The secondary aim was to explore if differences could be explained by the daily dosage received of the SSRIs under study | Selective serotonin reuptake inhibitors (SSRIs): citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, sertraline, and venlafaxine. Venlafaxine in daily doses up to 150 mg can be regarded as an SSRI | Sex-disaggregated outcomes and testing for significance |
| Faye et al. (2013) [35] | France | Cohort study (prospective or retrospective) | To describe all ADRs for oral protein kinase inhibitors, their characteristics, and whether they were labeled | Protein kinase inhibitors (erlotinib, gefitinib, imatinib, nilotinib, dasatinib, sunitinib, sorafenib, pazopanib, and lapatinib) | Sex-disaggregated outcomes and testing for significance |
| Holm et al. (2017) [36] | Sweden | Cross-sectional | To investigate how reporting of adverse drug reactions (ADRs) among adults in Sweden is associated with age and sex, in addition to seriousness of the reaction and drug utilization | Several ATC: blood and blood forming organs, cardiovascular system, general anti-infectives for systemic use, nervous system and a fifth composite group, consisting of suspected drugs belonging to the remaining ATC codes | Sex-disaggregated outcomes and testing for significance |
| Jia et al. (2019) [37] | USA | Cohort | To evaluate the safety profiles of human papillomavirus (HPV) vaccines with regard to the distribution of adverse events (AE) across gender and age, and the correlations across various AEs using the Food and Drug Administration/Centers for Disease Control and Prevention Vaccine Adverse Event Reporting System (VAERS). Research questions: (1) Are the frequencies of AEs different across different gender and age groups? If significant differences are observed, it is essential to develop a more precise vaccine information statement for these targeted subgroups. (2) Are there any correlations among the AEs? Specifically, we explored whether some AEs were more likely to occur together | Human papillomavirus (HPV) vaccine (vaccine types: HPVX/HPV2/HPV4/HPV9 (HPV vaccine with no brand name/HPV Cervarix/HPV Gardasil/HPV Gardasil 9)) | Sex-disaggregated outcomes and testing for significance |
| Jingcheng et al. (2017) [38] | USA | Cross-sectional | To study individual differences, considering sex and age, in adverse reactions following vaccination of the trivalent influenza vaccine | Trivalent influenza virus vaccine (FLU3) | Sex-disaggregated outcomes and testing for significance |
| Lindsey et al. (2016) [39] | USA | Cross-sectional | To describe adverse events following yellow fever (YF) vaccination reported to the U.S. Vaccine Adverse Event Reporting System (VAERS) from 2007 to 2013 and to calculate age- and sex-specific reporting rates of all serious adverse events (SAE), anaphylaxis, YF-vaccine-associated neurologic disease (YEL-AND) and YF-vaccine-associated viscerotropic disease (YEL-AVD) | Yellow fever vaccine | Sex-disaggregated outcomes (no testing for significance) |
| Lowe & Costabile (2012) [40] | USA | Cross-sectional | To document the rate of reported significant adverse cardiovascular events or mortality associated with each of three phosphodiesterase type-5 inhibitors (PDE5-I) used to treat erectile dysfunction over 10 years by a review of industry and non-industry reports submitted to the FDA | Sildenafil, tadalafil, and vardenafil | Outcomes for one sex/gender group only—males |
| Luk et al. (2013) [41] | USA | Cohort | To examine the association between use of different proton pump inhibitors (PPIs) and hypomagnesemia by examining frequency of occurrence among reported ADRs from the FDA AERS database | Proton pump inhibitors (esomeprazole, lansoprazole, omeprazole, pantoprazole, rabeprazole, and dexlansoprazole) | Sex/gender used as a confounder/controlled for (e.g., included in a regression model) |
| Macedo et al. (2011) [42] | Portugal | Cross-sectional | To evaluate the role of multiple drug exposure as an independent risk factor for serious ADRs and to validate the hypothesis of a trend for increased seriousness of ADRs in the presence of an increased number of simultaneous drug exposures | The drugs most commonly reported as responsible for the suspected ADRs were anti-infectives for systemic use (including vaccines; n = 452; 30.5%), drugs active on the muscle-skeletal system (n = 257; 17.3%), the nervous system (n = 240; 16.2%) and the cardiovascular system (n = 210; 14.2%). Together they accounted for 78.2% of all ADRs | Sex-disaggregated outcomes and testing for significance Sex/gender used as a confounder/controlled for (e.g., included in a regression model) |
| McDonald et al. (2019) [43] | USA | Cross-sectional | To identify predictors of gastrointestinal (GI) bleeding in older adults (65–100 years) when a nonsteroidal anti-inflammatory drug (NSAID) was identified as the primary suspect for an adverse drug event (ADE) | Nonsteroidal anti-inflammatory drug (NSAID) | Sex-disaggregated outcomes and testing for significance |
| McLernon et al. (2010) [44] | UK | Cohort study | To compare patient characteristics, suspected drugs, and suspected adverse reactions (ADRs) reported by patients with those reported by healthcare professionals using the Yellow Card Scheme (YCS) | The 20 most frequent suspect drugs reported: simvastatin, paroxetine, atorvastatin, diclofenac, amlodipine, venlafaxine, citalopram, tramadol, cyproterone and estrogen, trimethoprim, erythromycin, fluoxetine, ibuprofen, atenolol, olanzapine, omeprazole, bendroflumethiazide, paracetamol, combinations excluding psycholeptics, risperidone | Sex-disaggregated outcomes and testing for significance |
| McNeil et al. (2019) [45] | USA | Cross-sectional | To evaluate the safety profile of the adenovirus vaccine by reviewing reports submitted to the Vaccine Adverse Event Reporting System (VAERS) | Adenovirus vaccination | Sex-disaggregated outcomes and testing for significance |
| McNeil et al. (2012) [46] | USA | Cross-sectional | The aim of this pharmacovigilance study was to examine the spectrum of adverse events among reservists in a US military unit after receiving monovalent pandemic 2009 (H1N1) vaccine (MIV) and to investigate the factors contributing to a cluster of reports to the Vaccine Adverse Event Reporting System (VAERS) that occurred on 20 February 2010 from members of this unit | Monovalent pandemic 2009 (H1N1) vaccine (MIV) | Sex-disaggregated outcomes and testing for significance |
| Mertes et al. (2011) [47] | France | Cohort study | To report the results of an 8-year survey of anaphylaxis during anesthesia in France | The ADRs were associated to NMBAs (n = 539; 31.97%) and antibiotics (n = 511; 9.02%) | Sex-disaggregated outcomes and testing for significance |
| Nevin & Leoutsakos (2017) [48] | USA | Case control | To identify a distinct neuropsychiatric syndrome class associated with reports of adverse reactions from mefloquine use, to confirm the association of this syndrome with prodromal symptoms, and to identify other specific symptoms commonly associated with it that might inform improvements in case findings | Mefloquinem atovaquine-proguanil, doxycycline, chloroqine, and loperamide | Sex-disaggregated outcomes |
| O’Donovan et al. (2019) [49] | UK | Cross-sectional | To analyze a large sample of patient Yellow Card reports from July to December 2015. Objectives were to (1) describe all patient reports submitted to the Medicines and Healthcare Regulatory Agency (MHRA) over a 6-month period in terms of reporter characteristics, drugs, reactions, and outcomes; (2) explore factors associated with reports classed by the MHRA as serious; and (3) compare selected parameters to the analysis of reports from the first 2 years | Vaccines and other drugs | Sex- and age-disaggregated outcomes |
| Ordonez et al. (2015) [50] | Spain | Cohort | To assess the association between Stevens–Johnson Syndrome (SJS)/toxic epidermal necrolysis (TENS) and antiepileptics, including the most recently authorized drugs, based on the information provided by the spontaneous reporting of suspected adverse drug reactions (ADR) | Antiepileptic drugs (phenytoin, lamotrigine, carbamazepine, valproate, phenobarbital oxcarbazepine, levetiracetam, primidone, and gabapentin) | Sex-disaggregated outcomes and testing for significance |
| Reitter et al. (2014) [51] | France | Cohort study (prospective or retrospective) | To evaluate the mortality rate in France from anaphylactic reactions to neuromuscular blocking agents (NMBAs), to identify risk factors for a fatal outcome, and to describe management of the cases that proved fatal | Neuromuscular blocking agents (NMBAs): atracurium, cisatracurium, mivacurium, pancuronium, rocuronium, sux-amethonium, and vecuronium | Sex/gender used as a confounder/controlled for (e.g., included in a regression model) |
| Ribeiro-Vaz et al. (2013) [52] | Portugal | Case series | To characterize a case series of anaphylactic reactions reported to the Portuguese Pharmacovigilance authority during the past decade | Drugs associated with the reporting cases: antibiotics (17%), nonsteroidal anti-inflammatory drugs/acetaminophen (13%), antineoplastic/cytotoxic drugs, immune-modulators, vaccines, and radiographic contrast media | Sex-disaggregated outcomes and testing for significance |
| Ronaldson et al. (2011) [53] | Australia | Cohort | To compare key characteristics between clozapine-induced myocarditis fatal and non-fatal cases and to identify factors that may serve as clues to the prevention of myocarditis-related fatality in patients starting clozapine | Clozapine | Sex-disaggregated outcomes and testing for significance |
| Rydberg et al. (2018) [54] | Sweden | Cross-sectional | To explore sex differences regarding reported adverse drug events (ADEs) from the 10 most commonly prescribed antihypertensive medicines in Sweden, using the Swedish Spontaneous Adverse Drug Event Reporting System (SWEDIS) and the Swedish Prescribed Drug Register (SPDR) | 10 selected groups of antihypertensives; ACE-Is, ACE-I/thiazide combinations, ARBs, ARB/thiazide combinations, Thiazides, diuretics and potassium-sparing agents, sulfonamides, aldosterone antagonists, dihydropyridines, and beta blockers | Sex-disaggregated outcomes and testing for significance |
| Rydberg et al. (2014) [55] | Sweden | Cross-sectional | To analyze sex differences in reported bleeding events of warfarin, low-dose aspirin, and clopidogrel in Swedish Spontaneous Adverse Drug Event Reporting System (SWEDIS), adjusted by drug utilization data from the Swedish Prescribed Drug register | Warfarin, low-dose aspirin, and clopidogrel | Sex-disaggregated outcomes and testing for significance |
| Serebruany et al. (2017) [56] | USA | Cross-sectional | To assess the quality and completeness of aspirin and other oral antiplatelet agents (OAAs) cases reported to the U.S. Food and Drug Administration (FDA) Adverse Event (AE) Reporting System (FAERS) in terms of age and gender | Oral antiplatelet agents (OAAs): Aspirin, clopidogrel, prasugrel, ticagrelor, and vorapaxar | % gender and age missing from reports of AEs. |
| Tkachenko et al. (2019) [57] | USA | Cross-sectional | To determine the frequency and rate of pregnancy and pregnancy-related adverse events among women taking isotretinoin reported to the US FDA. The authors were interested in understanding how AEs might change in the age of iPLEDGE, a program initiated in 2006 to reduce fetal exposure to isotretinoin as it carries a risk of teratogenesis | Isotretinoin | Outcomes for one sex/gender group only—females |
| Tkachenko et al. (2019) [58] | USA | Cross-sectional | To investigate the frequency of FDA reports of alopecia for patients taking isotretinoin from 1997 to 2017, with attention to age and gender differences | Isotretinoin | Sex-disaggregated outcomes (no testing for significance) |
| Wu et al. (2016) [59] | USA | Cross-sectional | To examine the clinical reports submitted to FAERS from 2004 to 2014 to compare the adverse effects of finasteride and minoxidil, the only 2 FDA-approved alopecia drugs | Finasteride (approved only in males for alopecia) and minoxidil | Sex-disaggregated outcomes and testing for significance |
| Yu et al. (2016) [60] | USA | Cross-sectional | To assess the extent of sex differences in ADEs across a wide range of treatments, to identify the drugs that show significant sex differences in 20 treatment regimens and 668 specific drugs, and to pinpoint the specific ADEs that account for the observed sex differences in the effects of these drugs | Antihypertensives, lipid-regulating agents, antidepressants, antiulcer agents, narcotic analgesics, antidiabetics, thyroid agents, antiepileptics, contraceptives, respiratory system agents, anticoagulants ADHD agents, insomnia agents, benign prostate hyperplasia agents, antipsychotics, osteoporosis agents, overactive bladder agents, antiparkinsonian agents, antimigraine agents, and Alzheimer agents | Sex-disaggregated outcomes and testing for significance |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brabete, A.C.; Greaves, L.; Maximos, M.; Huber, E.; Li, A.; Lê, M.-L. A Sex- and Gender-Based Analysis of Adverse Drug Reactions: A Scoping Review of Pharmacovigilance Databases. Pharmaceuticals 2022, 15, 298. https://doi.org/10.3390/ph15030298
Brabete AC, Greaves L, Maximos M, Huber E, Li A, Lê M-L. A Sex- and Gender-Based Analysis of Adverse Drug Reactions: A Scoping Review of Pharmacovigilance Databases. Pharmaceuticals. 2022; 15(3):298. https://doi.org/10.3390/ph15030298
Chicago/Turabian StyleBrabete, Andreea C., Lorraine Greaves, Mira Maximos, Ella Huber, Alice Li, and Mê-Linh Lê. 2022. "A Sex- and Gender-Based Analysis of Adverse Drug Reactions: A Scoping Review of Pharmacovigilance Databases" Pharmaceuticals 15, no. 3: 298. https://doi.org/10.3390/ph15030298
APA StyleBrabete, A. C., Greaves, L., Maximos, M., Huber, E., Li, A., & Lê, M.-L. (2022). A Sex- and Gender-Based Analysis of Adverse Drug Reactions: A Scoping Review of Pharmacovigilance Databases. Pharmaceuticals, 15(3), 298. https://doi.org/10.3390/ph15030298