
Comprehensive Analysis of Chemotherapeutic Agents That Induce Infectious Neutropenia



Abstract
1. Introduction
2. Results
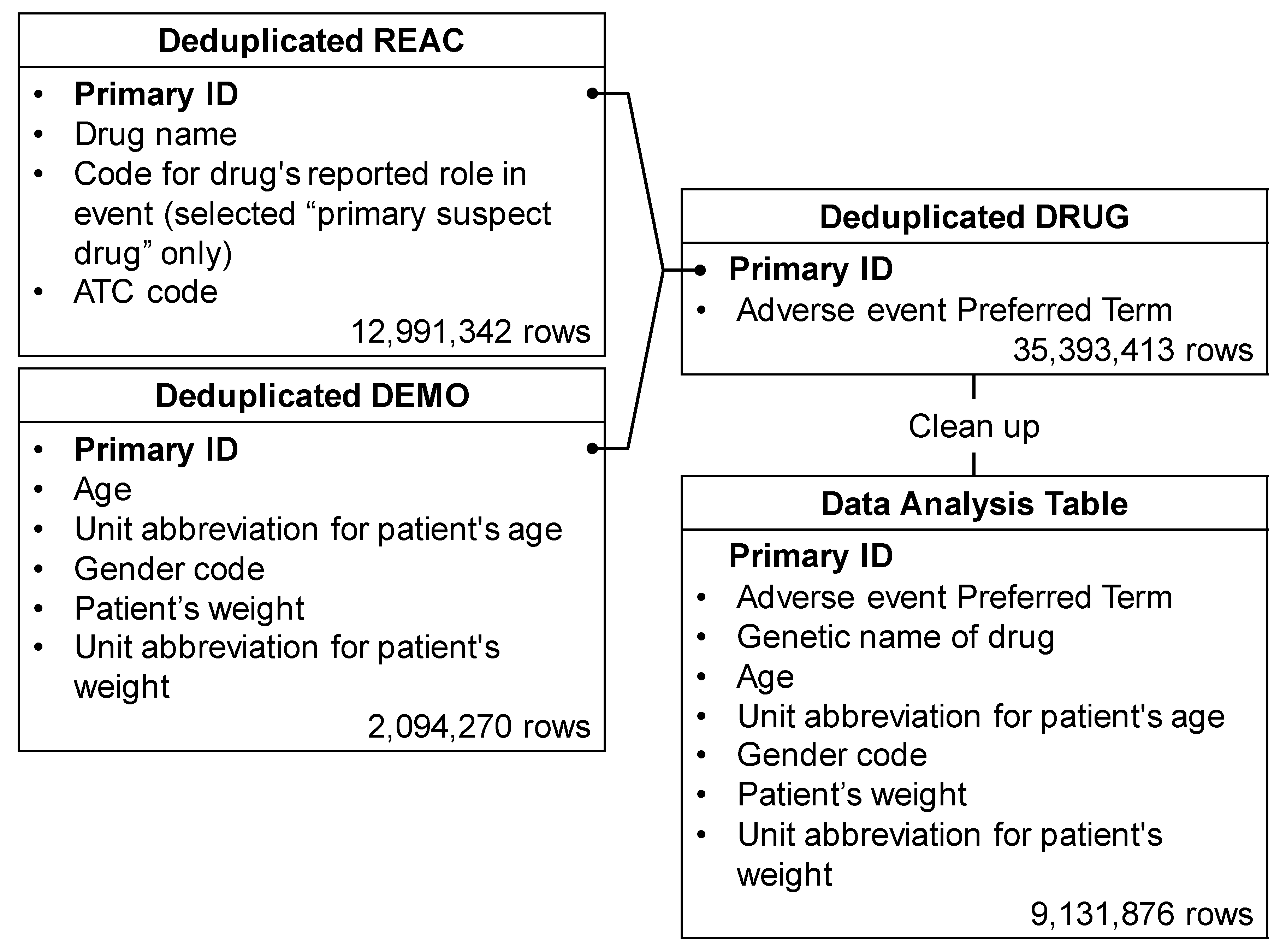
2.1. Data Presentation
2.2. Patients Characteristics
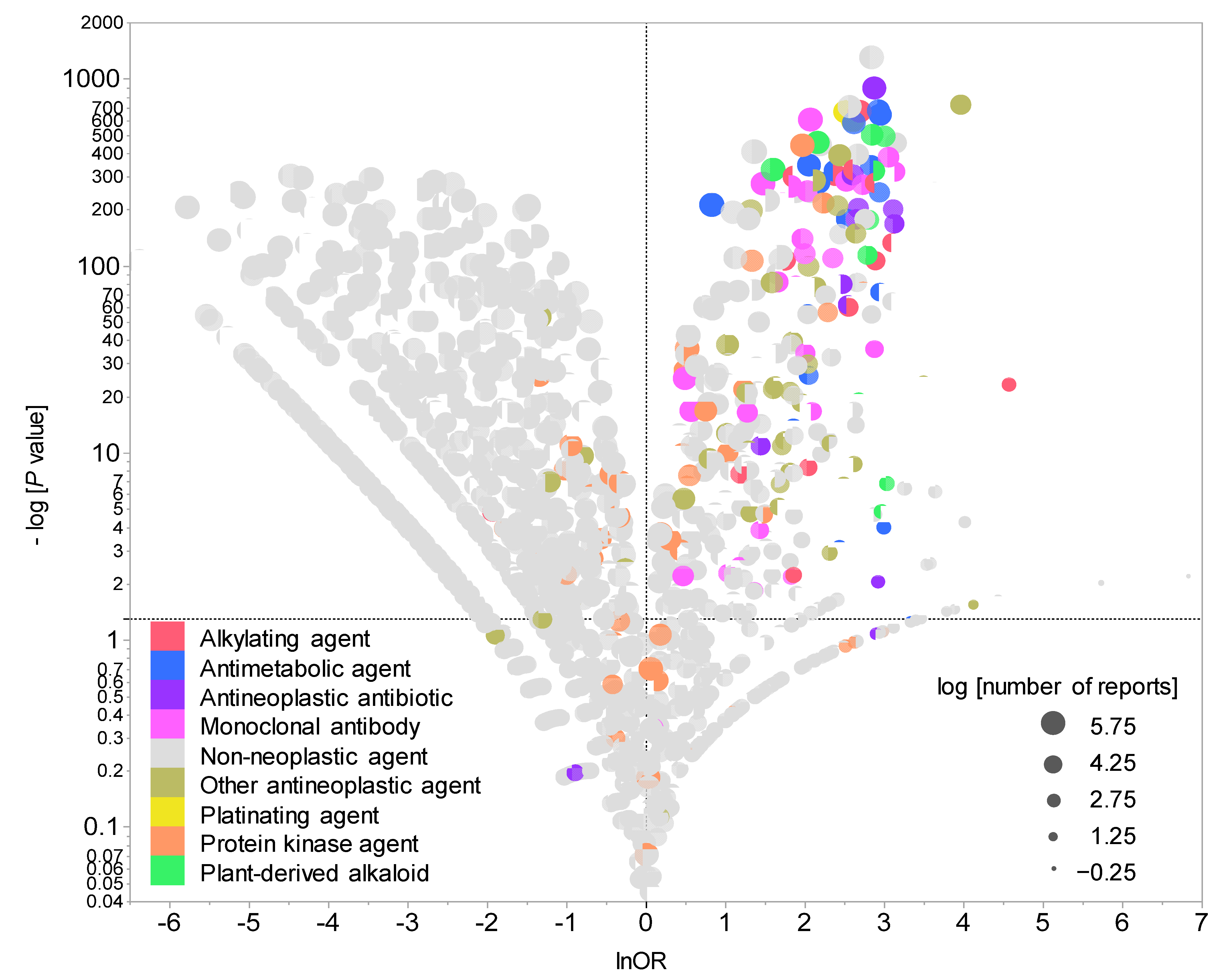
2.3. CIN-Inducing Drugs
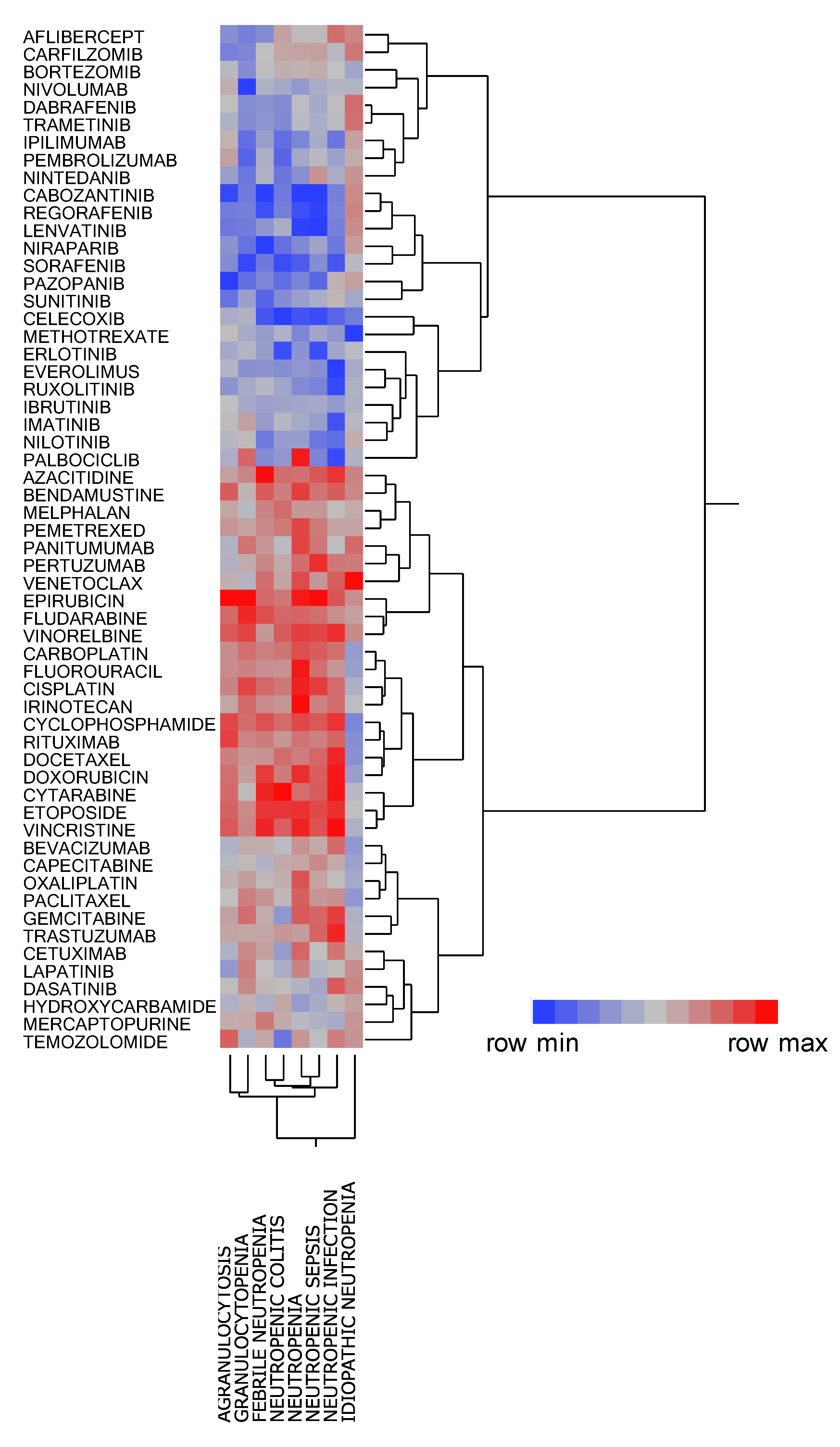
2.4. Cluster Analyses of CIN-inducing Drugs
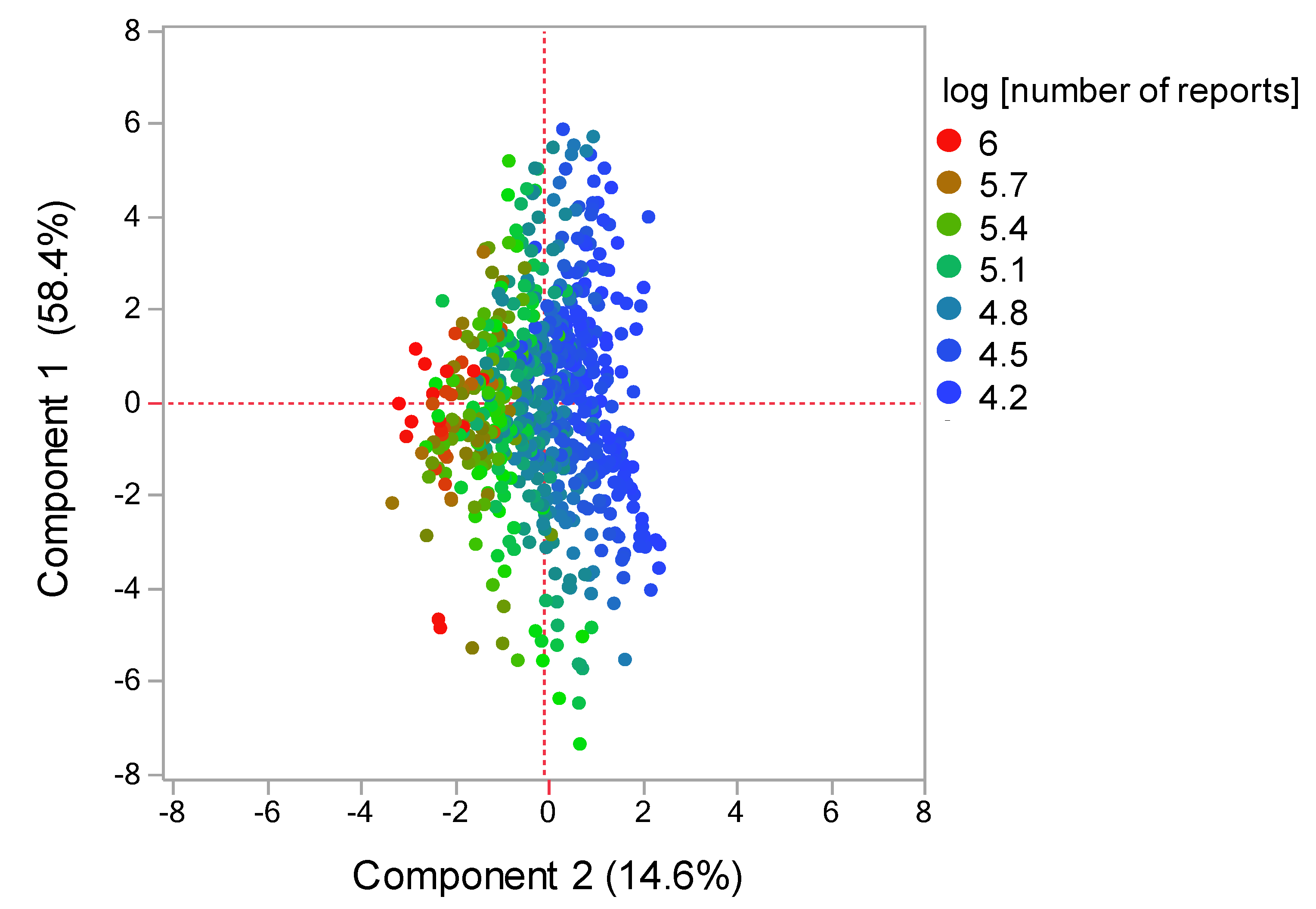
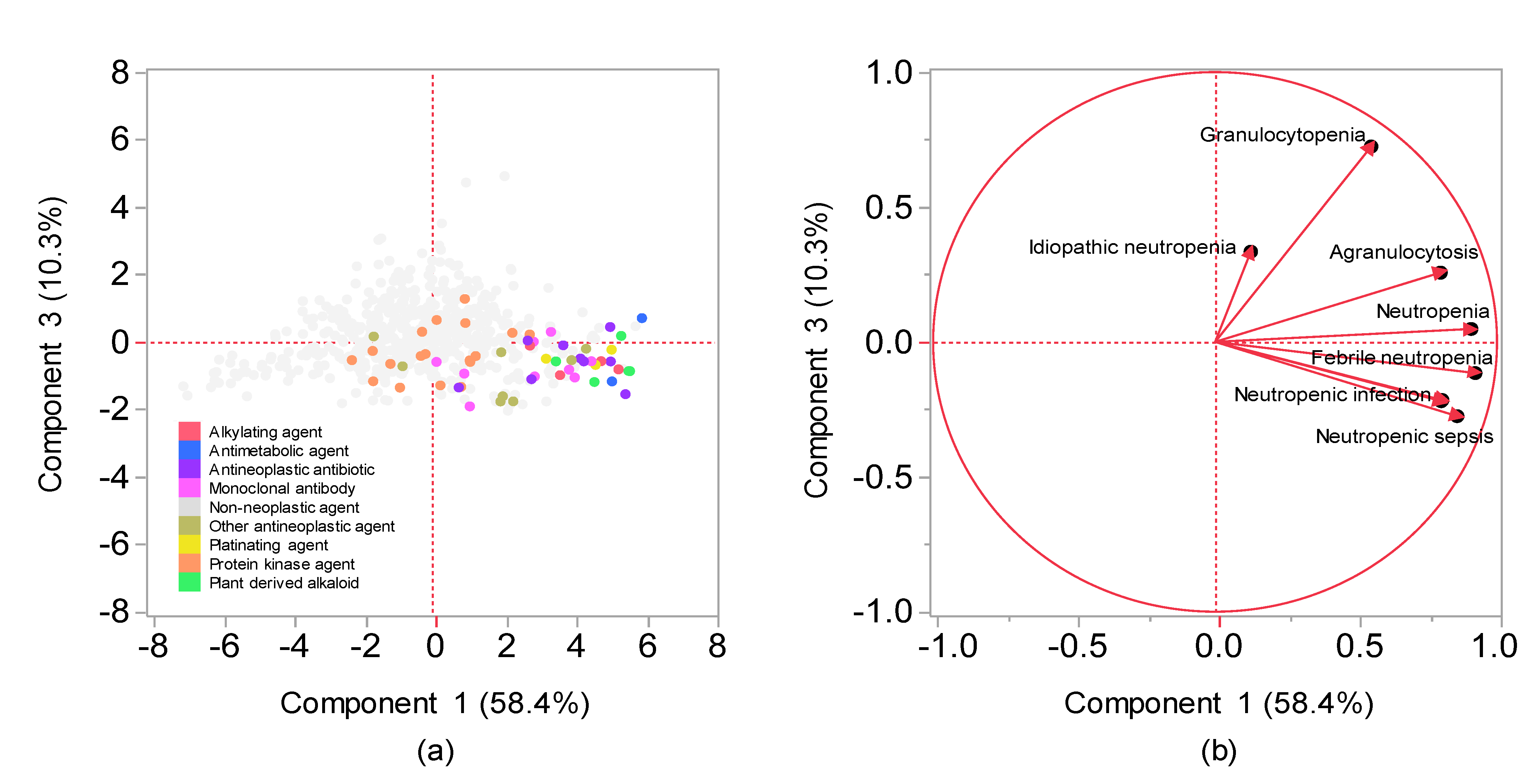
2.5. Principal Component Analysis Related to CIN
3. Discussion
Limitations
4. Materials and Methods
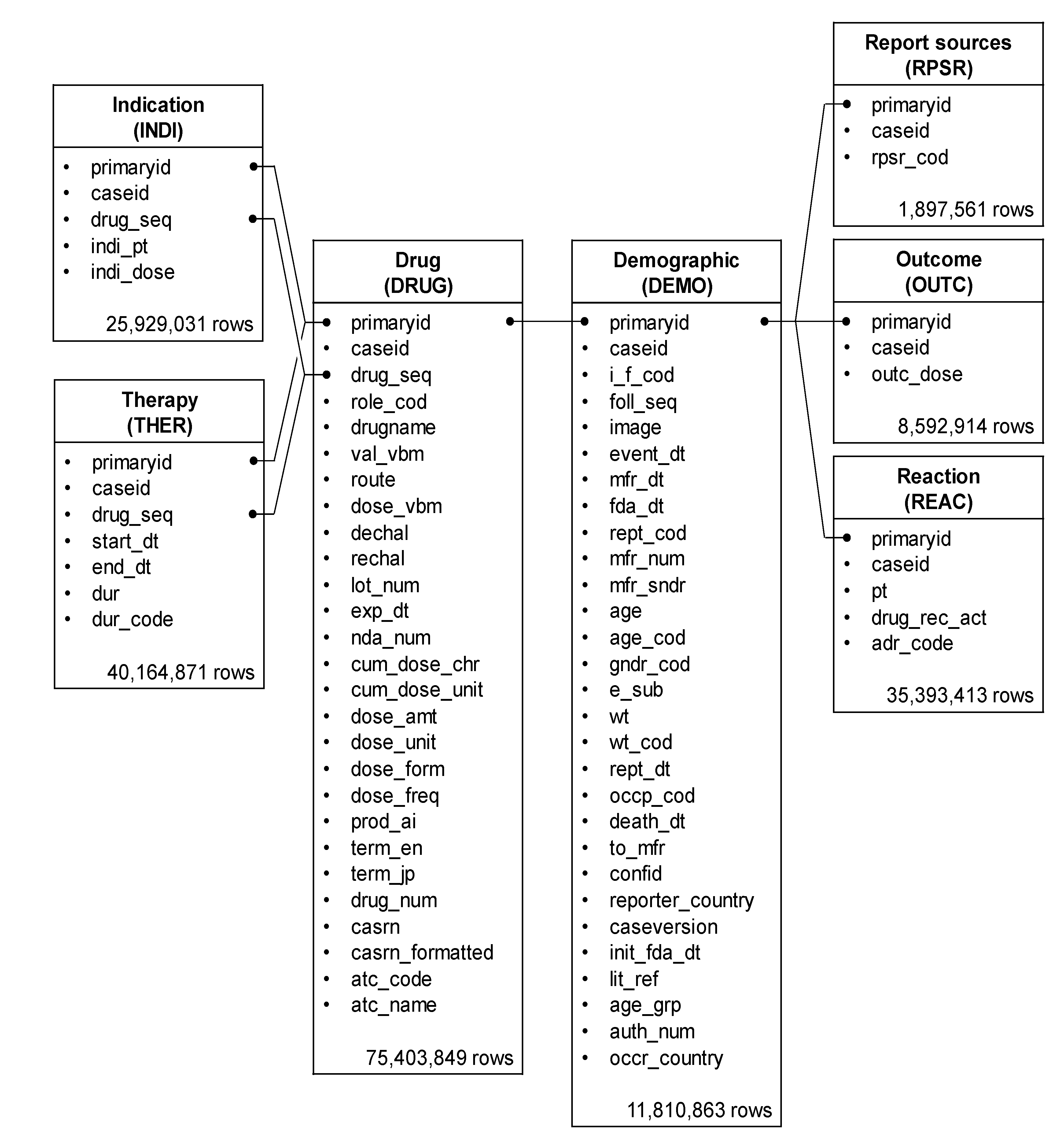
4.1. Database Information
4.2. Terminology of Analyzed Drugs and Adverse Events
4.3. Production of Data Analysis Table
4.4. Patient Characteristics Associated with Neutropenia
4.5. Univariate Analysis of Relationship between Drugs and Neutropenia
4.6. Cluster Analyses of CIN-Related Drugs
4.7. Principal Component Analysis Related to CIN
4.8. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Patel, K.; West, H.J. Febrile neutropenia. JAMA Oncol. 2017, 3, 1751. [Google Scholar] [CrossRef]
- Jiang, C.; Hu, X.; Wang, L.; Cheng, H.; Lin, Y.; Pang, Y.; Yuan, W.; Cheng, T.; Wang, J. Excessive proliferation and impaired function of primitive hematopoietic cells in bone marrow due to senescence post chemotherapy in a T cell acute lymphoblastic leukemia model. J. Transl. Med. 2015, 13, 234–245. [Google Scholar] [CrossRef]
- Basu, S.; Hodgson, G.; Katz, M.; Dunn, A.R. Evaluation of role of G-CSF in the production, survival, and release of neutrophils from bone marrow into circulation. Blood 2002, 100, 854–861. [Google Scholar] [CrossRef]
- Crawford, J.; Dale, D.C.; Lyman, G.H. Chemotherapy-induced neutropenia; risks, consequences, and new directions for its management. Cancer 2004, 100, 228–237. [Google Scholar] [CrossRef]
- Taplitz, R.A.; Kennedy, E.B.; Bow, E.J.; Crews, J.; Gleason, C.; Hawley, D.K.; Langston, A.A.; Nastoupil, L.J.; Rajotte, M.; Rolston, K.; et al. Outpatient management of fever and neutropenia in adults treated for malignancy: American Society of Clinical Oncology and Infectious Diseases Society of America Clinical Practice Guideline Update. J. Clin. Oncol. 2018, 36, 1443–1453. [Google Scholar] [CrossRef]
- Kasi, P.M.; Grothey, A. Chemotherapy-induced neutropenia as a prognostic and predictive marker of outcomes in solid-tumor patients. Drugs 2018, 78, 737–745. [Google Scholar] [CrossRef]
- Kalinka-Warzocha, E.; Plazas, J.G.; Mineur, L.; Salek, T.; Hendlisz, A.; DeCosta, L.; Vogl, F.D.; Passalacqua, R. Chemotherapy treatment patterns and neutropenia management in gastric cancer. Gastric Cancer 2015, 18, 360–367. [Google Scholar] [CrossRef][Green Version]
- Weycker, D.; Li, X.; Edelsberg, J.; Barron, R.; Kartashov, A.; Xu, H.; Lyman, G.H. Risk and consequences of chemotherapy-induced febrile neutropenia in patients with metastatic solid tumors. J. Oncol. Pract. 2015, 11, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Goldman, S.A. Limitations and strengths of spontaneous reports data. Clin. Ther. 1998, 20 (Suppl. C), C40–C44. [Google Scholar] [CrossRef]
- FDA Adverse Event Reporting System (FAERS). Available online: https://www.fda.gov/drugs/drug-approvals-and-databases/fda-adverse-event-reporting-system-faers (accessed on 5 June 2021).
- Lyman, G.H.; Abella, E.; Pettengell, R. Risk factors for febrile neutropenia among patients with cancer receiving chemotherapy: A systematic review. Crit. Rev. Oncol. Hematol. 2014, 90, 190–199. [Google Scholar] [CrossRef] [PubMed]
- Everitt, B.S.; Landau, S.; Leese, M.; Stahl, D. Cluster Analysis, 5th ed.; John Wiley & Sons: Hoboken, NJ, USA, 2011. [Google Scholar]
- Cristofanilli, M.; Turner, N.C.; Bondarenko, I.; Ro, J.; Im, S.A.; Masuda, N.; Colleoni, M.; DeMichele, A.; Loi, S.; Verma, S.; et al. Fulvestrant plus palbociclib versus fulvestrant plus placebo for treatment of hormone-receptor-positive, HER2-negative metastatic breast cancer that progressed on previous endocrine therapy (PALOMA-3): Final analysis of the Multicentre, Double-Blind, phase 3 Randomised Controlled Trial. Lancet Oncol. 2016, 17, 425–439. [Google Scholar]
- HIGHLIGHTS OF PRESCRIBING INFORMATION for IBRANCE. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/207103s004lbl.pdf (accessed on 14 July 2021).
- Jolliffe, I.T. Principal Component Analysis, 2nd ed.; Springer: New York, NY, USA, 2002. [Google Scholar]
- Pariente, A.; Avillach, P.; Salvo, F.; Thiessard, F.; Miremont-Salamé, G.; Fourrier-Reglat, A.; Haramburu, F.; Bégaud, B.; Moore, N. Association Française des Centres Régionaux de Pharmacovigilance (CRPV). Effect of competition bias in safety signal generation: Analysis of a research database of spontaneous reports in France. Drug. Saf. 2012, 35, 855–864. [Google Scholar] [CrossRef]
- Avillach, P.; Salvo, F.; Thiessard, F.; Miremont-Salamé, G.; Fourrier-Reglat, A.; Haramburu, F.; Bégaud, B.; Moore, N.; Pariente, A. l’Association des Centres Régionaux de Pharmacovigilance Pilot. Evaluation of an automated method to decrease false-positive signals induced by co-prescriptions in spontaneous reporting databases. Pharmacoepidemiol. Drug. Saf. 2014, 23, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Maeda, R. 5. JADER from pharmacovigilance point of view. Jpn. J. Pharmacoepidemiol. Yakuzai Ekigaku 2014, 19, 51–56. [Google Scholar] [CrossRef]
- Lumini, A.; Nanni, L. Convolutional neural networks for ATC classification. Curr. Pharm. Des. 2018, 24, 4007–4012. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, H.; Matsushita, Y.; Watanabe, A.; Maeda, T.; Nukui, K.; Ogawa, Y.; Sawa, J.; Maeda, H. Early detection of important safety information. Recent methods for signal detection. Jpn. J. Biomet. 2004, 25, 37–60. [Google Scholar] [CrossRef]
- Ohyama, K.; Sugiura, M. Evaluation of the association between topical prostaglandin F2α analogs and asthma using the JADER database: Comparison with β-blockers. Yakugaku Zasshi 2018, 138, 559–564. [Google Scholar] [CrossRef]
- Van Puijenbroek, E.P.; Bate, A.; Leufkens, H.G.M.; Lindquist, M.; Orre, R.; Egberts, A.C. A Comparison of measures of disproportionality for signal detection in spontaneous reporting systems for adverse drug reactions. Pharmacoepidemiol. Drug. Saf. 2002, 11, 3–10. [Google Scholar] [CrossRef]
- Chen, J.J.; Wang, S.J.; Tsai, C.A.; Lin, C.J. Selection of differentially expressed genes in microarray data analysis. Pharm. J. 2007, 7, 212–220. [Google Scholar] [CrossRef] [PubMed]
- Hosoya, R.; Uesawa, Y.; Ishii-Nozawa, R.; Kagaya, H. Analysis of factors associated with hiccups based on the Japanese Adverse Drug Event Report Database. PLoS ONE 2017, 12, e0172057. [Google Scholar] [CrossRef]
- Toriumi, S.; Kobayashi, A.; Uesawa, Y. Comprehensive study of the risk factors for medication-related osteonecrosis of the jaw based on the Japanese Adverse Drug Event Report Database. Pharmaceuticals 2020, 13, 467. [Google Scholar] [CrossRef] [PubMed]
- Okunaka, M.; Kano, D.; Matsui, R.; Kawasaki, T.; Uesawa, Y. Evaluation of the expression profile of irinotecan-induced diarrhea in patients with colorectal cancer. Pharmaceuticals 2021, 14, 377. [Google Scholar] [CrossRef]
- Kan, Y.; Nagai, J.; Uesawa, Y. Evaluation of antibiotic-induced taste and smell disorders using the FDA Adverse Event Reporting System Database. Sci. Rep. 2021, 11, 9625. [Google Scholar] [CrossRef] [PubMed]
- Umetsu, R.; Abe, J.; Ueda, N.; Kato, Y.; Nakayama, Y.; Kinosada, Y.; Nakamura, M. Adverse event trends associated with over-the-counter drugs: Data mining of the Japanese Adverse Drug Event Report Database. Yakugaku Zasshi 2015, 135, 991–1000. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Nagai, J.; Uesawa, Y.; Shimamura, R.; Kagaya, H. Characterization of the adverse effects induced by acetaminophen and nonsteroidal anti-inflammatory drugs based on the analysis of the Japanese Adverse Drug Event Report Database. Clin. J. Pain. 2017, 33, 667–675. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | CIN | Non-CIN | p Value |
|---|---|---|---|
| Age (years) | |||
| Median [range] | 61 (0–103) | 58 (0–110) | |
| ≥65 years | 13,397 (41.4%) | 731,626 (35.9%) | <0.0001 |
| <65 years | 18,994 (58.6%) | 1,309,160 (64.1%) | |
| Sex, No | |||
| Female | 16,751 (51.7%) | 1,235,937 (60.6%) | <0.0001 |
| Male | 15,640 (48.3%) | 804,849 (39.4%) | |
| Weight (kg) | |||
| Median [range] | 68.0 (0.0–150.0) | 73.0 (0.0–150.0) | <0.0001 |
| Antineoplastic agents | |||
| Yes | 19,720 (60.9%) | 260,981 (12.8%) | <0.0001 |
| No | 12,671 (39.1%) | 1,779,805 (87.2%) | |
| ATC classification | |||
| Alkylating agent | 1890 (4.8%) | 10,279 (0.3%) | <0.0001 |
| Antimetabolic agent | 4078 (10.4%) | 34,168 (1.2%) | |
| Antineoplastic agent | 1054 (2.7%) | 5843 (0.2%) | |
| Monoclonal antibody | 3534 (9.0%) | 59,542 (2.0%) | |
| Platinating agent | 2111 (5.4%) | 17,077 (0.6%) | |
| Protein kinase agent | 2430 (6.2%) | 72,130 (2.4%) | |
| Plant-derived alkaloids | 2347 (6.0%) | 27,673 (0.9%) |
| Variables | Category | Univariate Analysis | |
|---|---|---|---|
| Odds Ratio (95% CI) | p Value | ||
| Age (years) | ≥65 vs. <65 | 1.394 (1.365–1.424) | <0.0001 |
| Sex | Female vs. male | 1.434 (1.403–1.466) | <0.0001 |
| Chemotherapeutic agents | Yes vs. No | 10.614 (10.375–10.857) | <0.0001 |
| Adverse Event | First Component | Second Component |
|---|---|---|
| Granulocytopenia | 0.594 | 0.670 |
| Idiopathic neutropenia | 0.167 | 0.383 |
| Agranulocytosis | 0.801 | 0.242 |
| Neutropenia | 0.904 | 0.0118 |
| Febrile neutropenia | 0.913 | −0.141 |
| Neutropenic colitis | 0.794 | −0.179 |
| Neutropenic infection | 0.802 | −0.187 |
| Neutropenic sepsis | 0.853 | −0.288 |
| Report Type | CIN | Non-CIN |
|---|---|---|
| Reports with the suspected medicine | a | c |
| All other reports | b | d |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Okunaka, M.; Kano, D.; Matsui, R.; Kawasaki, T.; Uesawa, Y. Comprehensive Analysis of Chemotherapeutic Agents That Induce Infectious Neutropenia. Pharmaceuticals 2021, 14, 681. https://doi.org/10.3390/ph14070681
Okunaka M, Kano D, Matsui R, Kawasaki T, Uesawa Y. Comprehensive Analysis of Chemotherapeutic Agents That Induce Infectious Neutropenia. Pharmaceuticals. 2021; 14(7):681. https://doi.org/10.3390/ph14070681
Chicago/Turabian StyleOkunaka, Mashiro, Daisuke Kano, Reiko Matsui, Toshikatsu Kawasaki, and Yoshihiro Uesawa. 2021. "Comprehensive Analysis of Chemotherapeutic Agents That Induce Infectious Neutropenia" Pharmaceuticals 14, no. 7: 681. https://doi.org/10.3390/ph14070681
APA StyleOkunaka, M., Kano, D., Matsui, R., Kawasaki, T., & Uesawa, Y. (2021). Comprehensive Analysis of Chemotherapeutic Agents That Induce Infectious Neutropenia. Pharmaceuticals, 14(7), 681. https://doi.org/10.3390/ph14070681