
The Effect of Transcutaneous Vagus Nerve Stimulation in Patients with Polymyalgia Rheumatica

 ,
,
Abstract
:1. Introduction
2. Results
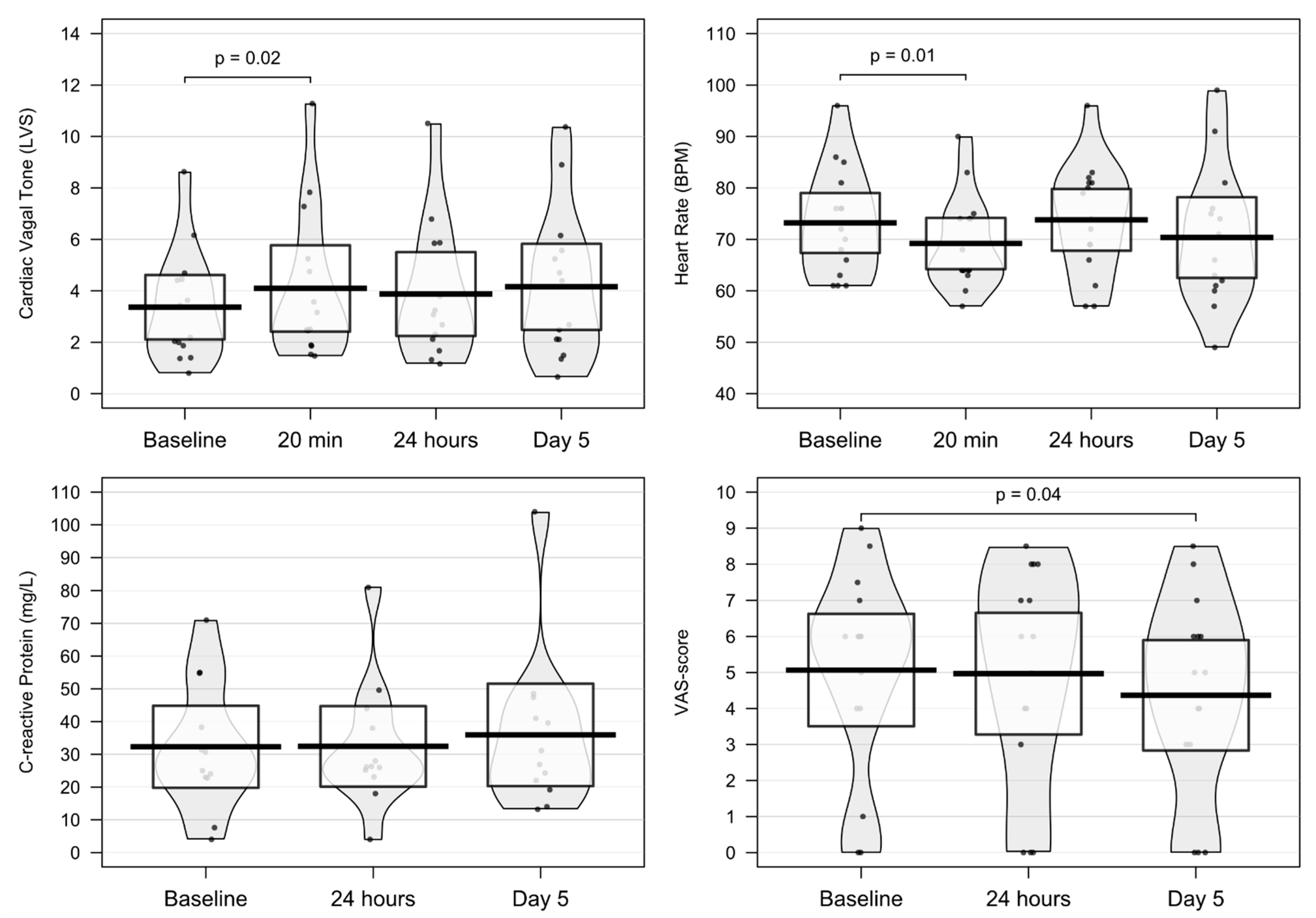
2.1. Changes in Primary Outcome: Cardiac Vagal Tone
2.2. Changes in Secondary Outcomes
2.2.1. Changes in Cardiac-Derived Parameters
2.2.2. Changes in CRP and Proinflammatory Analytes
2.2.3. Changes in Patient-Reported Outcome
3. Discussion
Limitations
4. Materials and Methods
4.1. Study Design
4.2. Cohort
4.3. Vagus Nerve Stimulation
4.4. Outcomes
4.4.1. Primary Outcome: Resting Cardiac Vagal Tone
4.4.2. Secondary Outcomes: Cardiac-Derived Parameters, CRP, Proinflammatory Analytes, and Patient-Reported Outcome
4.5. Statistical Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Camellino, D.; Giusti, A.; Girasole, G.; Bianchi, G.; Dejaco, C. Pathogenesis, Diagnosis and Management of Polymyalgia Rheumatica. Drugs Aging 2019. [Google Scholar] [CrossRef] [PubMed]
- Salvarani, C.; Cantini, F.; Hunder, G.G. Polymyalgia Rheumatica and Giant-Cell Arteritis. Lancet 2008, 372, 234–245. [Google Scholar] [CrossRef]
- Barraclough, K.; Liddell, W.G.; du Toit, J.; Foy, C.; Dasgupta, B.; Thomas, M.; Hamilton, W. Polymyalgia Rheumatica in Primary Care: A Cohort Study of the Diagnostic Criteria and Outcome. Fam. Pract. 2008, 25, 328–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Myklebust, G.; Wilsgaard, T.; Jacobsen, B.K.; Gran, J.T. Causes of Death in Polymyalgia RheumaticaA Prospective Longitudinal Study of 315 Cases and Matched Population Controls. Scand. J. Rheumatol. 2003, 32, 38–41. [Google Scholar] [CrossRef] [PubMed]
- Schaufelberger, C.; Bengtsson, B.-Å.; Andersson, R. Epidemiology and Mortality in 220 Patients with Polymyalgia Rheumatica. Rheumatology 1995, 34, 261–264. [Google Scholar] [CrossRef]
- Hutchings, A.; Hollywood, J.; Lamping, D.L.; Pease, C.T.; Chakravarty, K.; Silverman, B.; Choy, E.H.S.; Scott, D.G.I.; Hazleman, B.L.; Bourke, B.; et al. Clinical Outcomes, Quality of Life, and Diagnostic Uncertainty in the First Year of Polymyalgia Rheumatica. Arthritis Care Res. 2007, 57, 803–809. [Google Scholar] [CrossRef]
- Dejaco, C.; Singh, Y.P.; Perel, P.; Hutchings, A.; Camellino, D.; Mackie, S.; Abril, A.; Bachta, A.; Balint, P.; Barraclough, K.; et al. 2015 Recommendations for the Management of Polymyalgia Rheumatica: A European League Against Rheumatism/American College of Rheumatology Collaborative Initiative. Arthritis Rheumatol. 2015, 67, 2569–2580. [Google Scholar] [CrossRef]
- Curtis, J.R.; Westfall, A.O.; Allison, J.; Bijlsma, J.W.; Freeman, A.; George, V.; Kovac, S.H.; Spettell, C.M.; Saag, K.G. Population-Based Assessment of Adverse Events Associated with Long-Term Glucocorticoid Use. Arthritis Care Res. 2006, 55, 420–426. [Google Scholar] [CrossRef]
- Gaffo, A.; Saag, K.G.; Curtis, J.R. Treatment of Rheumatoid Arthritis. Am. J. Health Syst. Pharm. 2006, 63, 2451–2465. [Google Scholar] [CrossRef] [PubMed]
- Alvarez-Rodríguez, L.; Lopez-Hoyos, M.; Mata, C.; Marin, M.J.; Calvo-Alen, J.; Blanco, R.; Aurrecoechea, E.; Ruiz-Soto, M.; Martínez-Taboada, V.M. Circulating Cytokines in Active Polymyalgia Rheumatica. Ann. Rheum. Dis. 2010, 69, 263–269. [Google Scholar] [CrossRef]
- Van der Geest, K.S.M.; Abdulahad, W.H.; Rutgers, A.; Horst, G.; Bijzet, J.; Arends, S.; Roffel, M.P.; Boots, A.M.H.; Brouwer, E. Serum Markers Associated with Disease Activity in Giant Cell Arteritis and Polymyalgia Rheumatica. Rheumatology 2015, 54, 1397–1402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Macchioni, P.; Boiardi, L.; Catanoso, M.; Pulsatelli, L.; Pipitone, N.; Meliconi, R.; Salvarani, C. Tocilizumab for Polymyalgia Rheumatica: Report of Two Cases and Review of the Literature. Semin. Arthritis Rheum. 2013, 43, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Devauchelle-Pensec, V.; Berthelot, J.M.; Cornec, D.; Renaudineau, Y.; Marhadour, T.; Jousse-Joulin, S.; Querellou, S.; Garrigues, F.; Bandt, M.D.; Gouillou, M.; et al. Efficacy of First-Line Tocilizumab Therapy in Early Polymyalgia Rheumatica: A Prospective Longitudinal Study. Ann. Rheum. Dis. 2016, 75, 1506–1510. [Google Scholar] [CrossRef]
- Camellino, D.; Soldano, S.; Cutolo, M.; Cimmino, M.A. Dissecting the Inflammatory Response in Polymyalgia Rheumatica: The Relative Role of IL-6 and Its Inhibition. Rheumatol. Int. 2018, 38, 1699–1704. [Google Scholar] [CrossRef]
- Chino, K.; Kondo, T.; Sakai, R.; Saito, S.; Okada, Y.; Shibata, A.; Kurasawa, T.; Okuyama, A.; Takei, H.; Amano, K. Tocilizumab Monotherapy for Polymyalgia Rheumatica: A Prospective, Single-Center, Open-Label Study. Int. J. Rheum. Dis. 2019, 22, 2151–2157. [Google Scholar] [CrossRef]
- Borovikova, L.V.; Ivanova, S.; Zhang, M.; Yang, H.; Botchkina, G.I.; Watkins, L.R.; Wang, H.; Abumrad, N.; Eaton, J.W.; Tracey, K.J. Vagus Nerve Stimulation Attenuates the Systemic Inflammatory Response to Endotoxin. Nature 2000, 405, 458. [Google Scholar] [CrossRef]
- Borovikova, L.V.; Ivanova, S.; Nardi, D.; Zhang, M.; Yang, H.; Ombrellino, M.; Tracey, K.J. Role of Vagus Nerve Signaling in CNI-1493-Mediated Suppression of Acute Inflammation. Auton. Neurosci. 2000, 85, 141–147. [Google Scholar] [CrossRef]
- Rasmussen, S.E.; Pfeiffer-Jensen, M.; Drewes, A.M.; Farmer, A.D.; Deleuran, B.W.; Stengaard-Pedersen, K.; Brock, B.; Brock, C. Vagal Influences in Rheumatoid Arthritis. Scand. J. Rheumatol. 2018, 47, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Brock, C.; Brock, B.; Aziz, Q.; Møller, H.J.; Jensen, M.P.; Drewes, A.M.; Farmer, A.D. Transcutaneous Cervical Vagal Nerve Stimulation Modulates Cardiac Vagal Tone and Tumor Necrosis Factor-Alpha. Neurogastroenterol. Motil. 2017, 29, e12999. [Google Scholar] [CrossRef]
- Drewes, A.M.; Brock, C.; Rasmussen, S.E.; Møller, H.J.; Brock, B.; Deleuran, B.W.; Farmer, A.D.; Pfeiffer-Jensen, M. Short-Term Transcutaneous Non-Invasive Vagus Nerve Stimulation May Reduce Disease Activity and pro-Inflammatory Cytokines in Rheumatoid Arthritis: Results of a Pilot Study. Scand. J. Rheumatol. 2021, 50, 20–27. [Google Scholar] [CrossRef]
- Brock, C.; Rasmussen, S.E.; Drewes, A.M.; Møller, H.J.; Brock, B.; Deleuran, B.; Farmer, A.D.; Pfeiffer-Jensen, M. Vagal Nerve Stimulation-Modulation of the Anti-Inflammatory Response and Clinical Outcome in Psoriatic Arthritis or Ankylosing Spondylitis. Mediat. Inflamm. 2021, 2021, e9933532. [Google Scholar] [CrossRef] [PubMed]
- Farmer, A.D.; Coen, S.J.; Kano, M.; Weltens, N.; Ly, H.G.; Botha, C.; Paine, P.A.; Oudenhove, L.V.; Aziz, Q. Normal Values and Reproducibility of the Real-Time Index of Vagal Tone in Healthy Humans: A Multi-Center Study. Ann. Gastroenterol. Q. Publ. Hell. Soc. Gastroenterol. 2014, 27, 362–368. [Google Scholar]
- Juel, J.; Brock, C.; Olesen, S.S.; Madzak, A.; Farmer, A.D.; Aziz, Q.; Frøkjær, J.B.; Drewes, A.M. Acute Physiological and Electrical Accentuation of Vagal Tone Has No Effect on Pain or Gastrointestinal Motility in Chronic Pancreatitis. J. Pain Res. 2017, 10, 1347–1355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brock, C.; Jessen, N.; Brock, B.; Jakobsen, P.E.; Hansen, T.K.; Rantanen, J.M.; Riahi, S.; Dimitrova, Y.K.; Dons-Jensen, A.; Aziz, Q.; et al. Cardiac Vagal Tone, a Non-Invasive Measure of Parasympathetic Tone, Is a Clinically Relevant Tool in Type 1 Diabetes Mellitus. Diabet. Med. 2017, 34, 1428–1434. [Google Scholar] [CrossRef]
- Engel, T.; Ben-Horin, S.; Beer-Gabel, M. Autonomic Dysfunction Correlates with Clinical and Inflammatory Activity in Patients with Crohn’s Disease. Inflamm. Bowel Dis. 2015, 21, 2320–2326. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, B.; Hutchings, A.; Matteson, E.L. Polymyalgia Rheumatica: The Mess We Are Now in and What We Need to Do about It. Arthritis Care Res. 2006, 55, 518–520. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, B.; Cimmino, M.A.; Kremers, H.M.; Schmidt, W.A.; Schirmer, M.; Salvarani, C.; Bachta, A.; Dejaco, C.; Duftner, C.; Jensen, H.S.; et al. 2012 Provisional Classification Criteria for Polymyalgia Rheumatica: A European League Against Rheumatism/American College of Rheumatology Collaborative Initiative. Arthritis Rheum. 2012, 64, 943–954. [Google Scholar] [CrossRef]
- Koopman, F.A.; Chavan, S.S.; Miljko, S.; Grazio, S.; Sokolovic, S.; Schuurman, P.R.; Mehta, A.D.; Levine, Y.A.; Faltys, M.; Zitnik, R.; et al. Vagus Nerve Stimulation Inhibits Cytokine Production and Attenuates Disease Severity in Rheumatoid Arthritis. Proc. Natl. Acad. Sci. USA 2016, 113, 8284–8289. [Google Scholar] [CrossRef] [Green Version]
- Wegeberg, A.-M.; Lunde, E.D.; Riahi, S.; Ejskjaer, N.; Drewes, A.M.; Brock, B.; Pop-Busui, R.; Brock, C. Cardiac Vagal Tone as a Novel Screening Tool to Recognize Asymptomatic Cardiovascular Autonomic Neuropathy: Aspects of Utility in Type 1 Diabetes. Diabetes Res. Clin. Pract. 2020, 170, 108517. [Google Scholar] [CrossRef]
- Julu, P.O.O. A Linear Scale for Measuring Vagal Tone in Man. J. Auton. Pharmacol. 1992, 12, 109–115. [Google Scholar] [CrossRef]
- Malik, M. Heart Rate Variability. Ann. Noninvasive Electrocardiol. 1996, 1, 151–181. [Google Scholar] [CrossRef]


{kind=link}
| Characteristic | PMR Patients (n = 15) |
|---|---|
| Sex (female) | 13 (87) |
| Age (years) | 65 ± 10 |
| Height (cm) | 169 ± 6 |
| Weight (kg) | 72 ± 12 |
| Body mass index (kg/m2) | 25 ± 4 |
| Currently using NSAIDs (yes) | 6 (40.0) |
| Daily NSAID dose (mg ibuprofen) | 833 ± 480 |
| Ethnicity (Caucasian) | 15 (100.0) |
| Smoking, ever (yes) | 7 (47) |
| Smoking (pack-years) | 16 ± 12 |
| Daily caffeine intake (yes) | 15 (100) |
| Stimulations pr. patient (mean out of 26) | 24 (91) |
| Amplitude of baseline stimulation | 33 ± 6 |
| Baseline | 20 min | 24 h | Day 5 | p-Value | |
|---|---|---|---|---|---|
| Cardiac vagal tone (LVS) | 3.4 ± 2.2 | 4.1 ± 2.9 | 3.9 ± 2.7 | 4.2 ± 2.9 | 0.02 * |
| Systolic blood pressure (mmHG) | 139 ± 22 | 141 ± 22 | 135 ± 19 | 137 ± 24 | 0.38 |
| Diastolic blood pressure (mmHG) | 79 ± 10 | 81 ± 10 | 77 ± 8 | 82 ± 15 | 0.53 |
| Heart rate (BPM) | 73 ± 11 | 69 ± 9 | 74 ± 11 | 70 ± 14 | 0.01 * |
| MHAQ score | 0.9 ± 0.5 | - | 0.9 ± 0.5 | 0.8 ± 0.5 | 0.19 |
| VAS score of PMR-influence | 6.7 ± 2.6 | - | 6.4 ± 2.6 | 6.1 ± 2.5 | 0.23 |
| VAS score in hips | 5.1 ± 2.8 | - | 5.0 ± 3.1 | 4.4 ± 2.8 | 0.04 |
| Global VAS score | 6.2 ± 2.8 | - | 6.1 ± 2.7 | 5.9 ± 2.5 | 0.54 |
| Duration of morning stiffness (minutes) | 124 ± 89 | - | 120 ± 79 | 108 ± 65 | 0.19 |
| C-reactive protein (mg/L) | 32.3 ± 19.7 | - | 32.4 ± 19.3 | 35.9 ± 24.6 | 0.74 |
| IFN-γ (pg/mL) | 5.40 ± 2.67 | - | - | 6.20 ± 5.94 | 0.29 |
| IL-2 (pg/mL) | 0.06 (0.10) | - | - | 0.12 (0.24) | 0.06 |
| IL-4 (pg/mL) | 0.01 ± 0.01 | - | - | 0.03 ± 0.03 | 0.82 |
| IL-6 (ng/L) | 4.81 (4.80) | - | - | 4.50 (6.25) | 0.19 |
| IL-8 (pg/mL) | 12.72 ± 6.58 | - | - | 12.68 ± 6.90 | 0.37 |
| IL-10 (pg/mL) | 0.27 (0.14) | - | - | 0.32 (0.12) | 0.91 |
| TNF-α (pg/mL) | 1.35 ± 0.43 | - | - | 1.32 ± 0.44 | 0.67 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Venborg, J.; Wegeberg, A.-M.; Kristensen, S.; Brock, B.; Brock, C.; Pfeiffer-Jensen, M. The Effect of Transcutaneous Vagus Nerve Stimulation in Patients with Polymyalgia Rheumatica. Pharmaceuticals 2021, 14, 1166. https://doi.org/10.3390/ph14111166
Venborg J, Wegeberg A-M, Kristensen S, Brock B, Brock C, Pfeiffer-Jensen M. The Effect of Transcutaneous Vagus Nerve Stimulation in Patients with Polymyalgia Rheumatica. Pharmaceuticals. 2021; 14(11):1166. https://doi.org/10.3390/ph14111166
Chicago/Turabian StyleVenborg, Jacob, Anne-Marie Wegeberg, Salome Kristensen, Birgitte Brock, Christina Brock, and Mogens Pfeiffer-Jensen. 2021. "The Effect of Transcutaneous Vagus Nerve Stimulation in Patients with Polymyalgia Rheumatica" Pharmaceuticals 14, no. 11: 1166. https://doi.org/10.3390/ph14111166
APA StyleVenborg, J., Wegeberg, A.-M., Kristensen, S., Brock, B., Brock, C., & Pfeiffer-Jensen, M. (2021). The Effect of Transcutaneous Vagus Nerve Stimulation in Patients with Polymyalgia Rheumatica. Pharmaceuticals, 14(11), 1166. https://doi.org/10.3390/ph14111166