Combining Sorafenib and Immunosuppression in Liver Transplant Recipients with Hepatocellular Carcinoma

 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Results
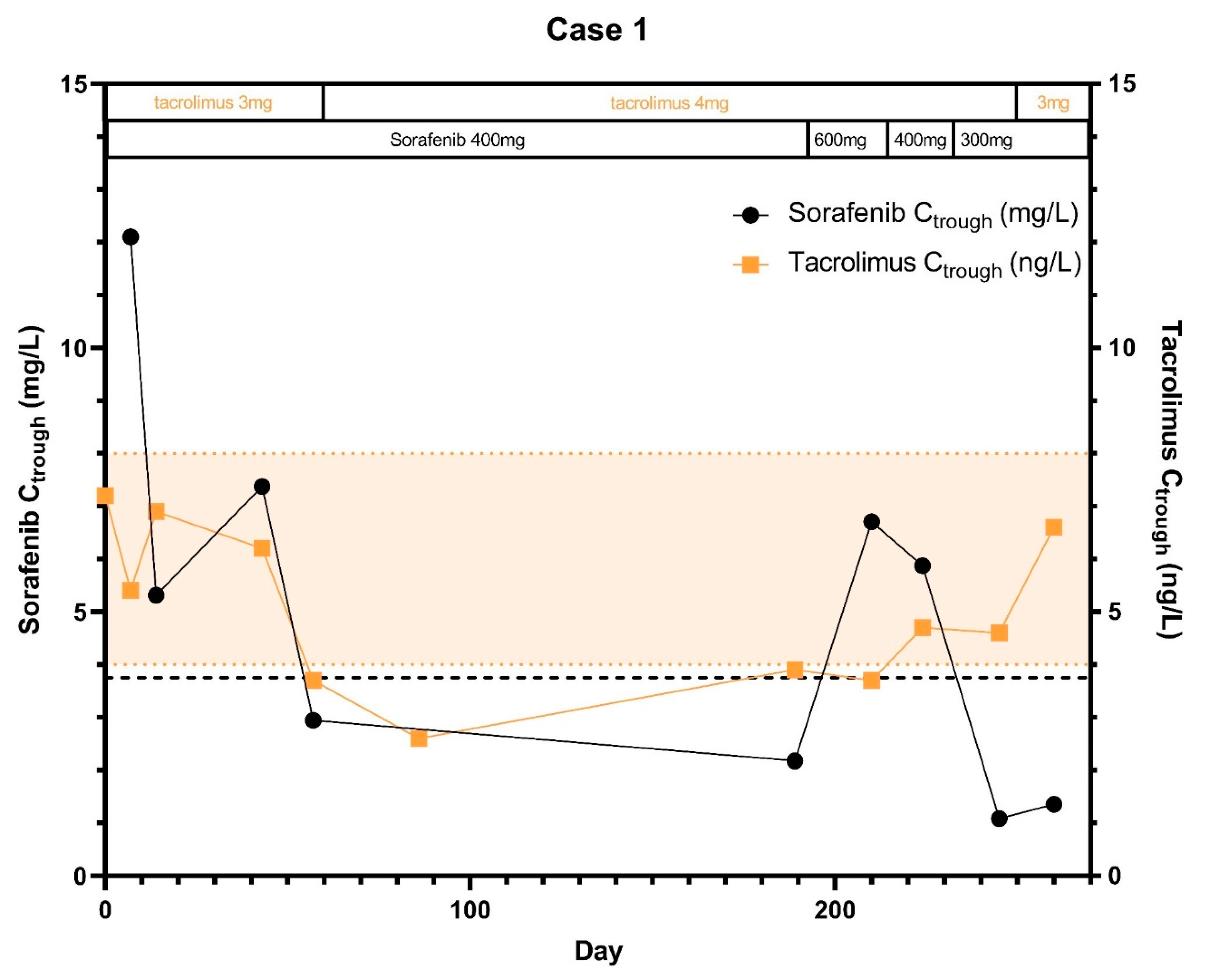
2.1. Case 1
2.2. Case 2
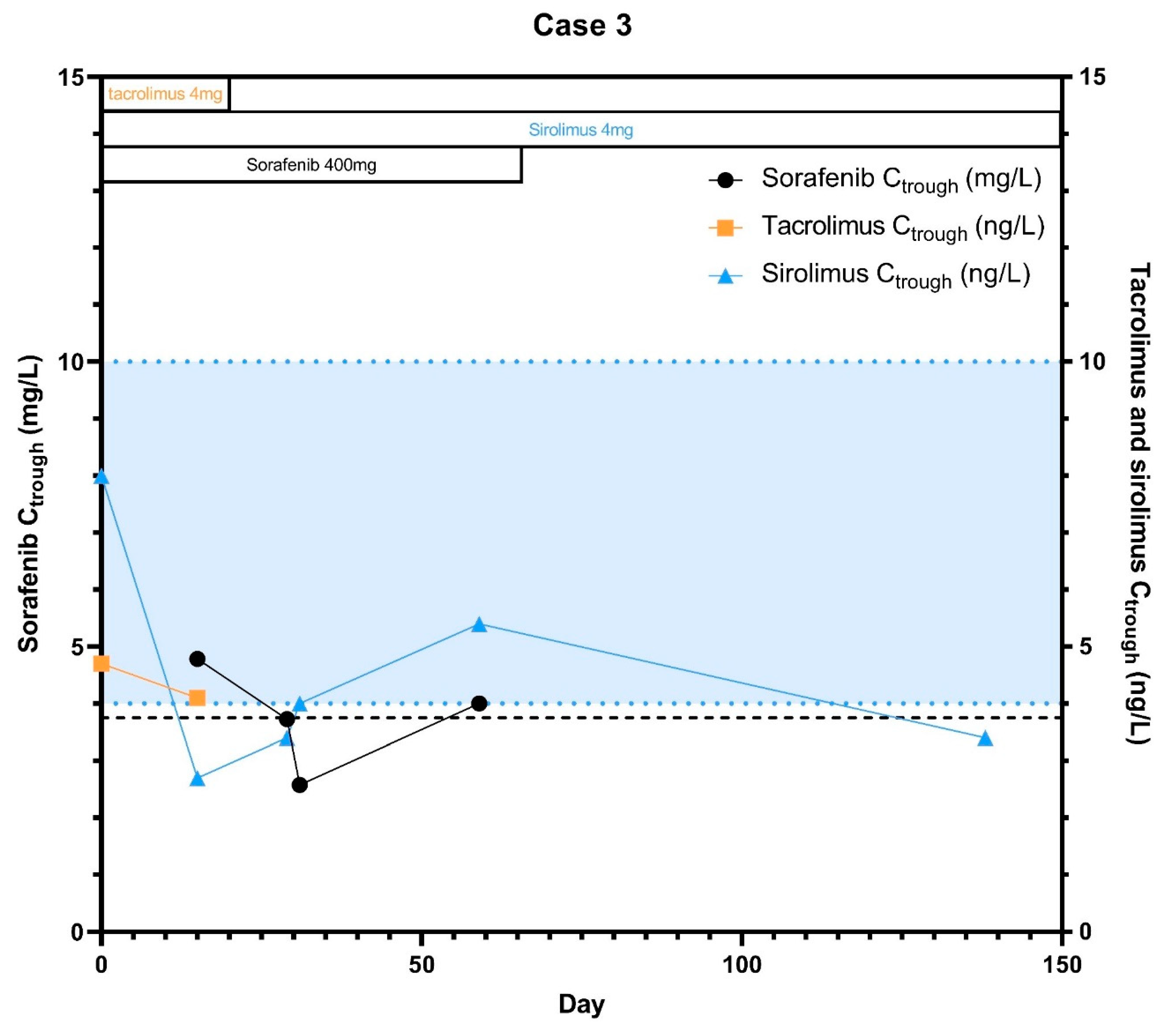
2.3. Case 3
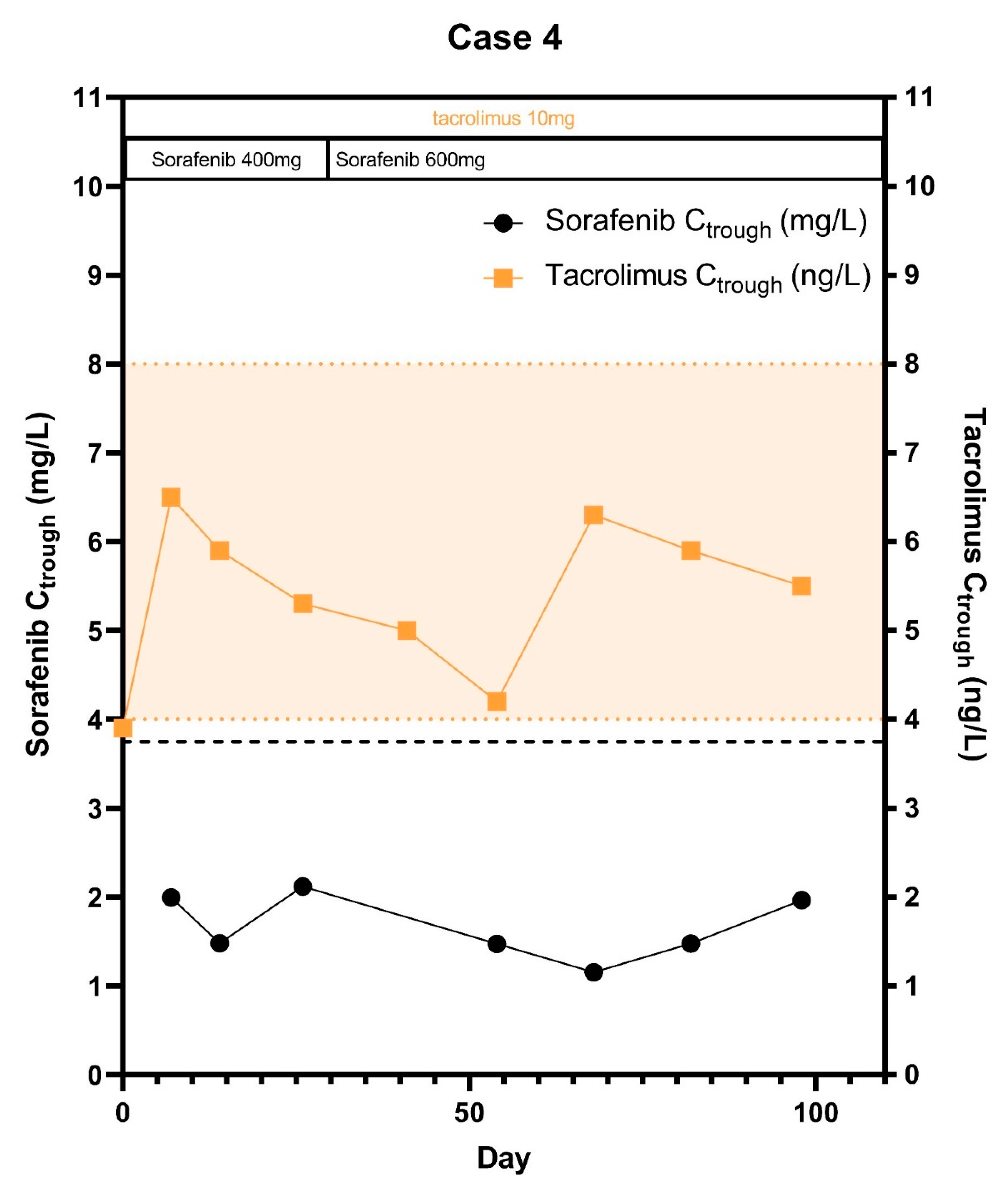
2.4. Case 4
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [PubMed]
- Iavarone, M.; Invernizzi, F.; Czauderna, C.; Sanduzzi-Zamparelli, M.; Bhoori, S.; Amaddeo, G.; Manini, M.A.; López, M.F.; Anders, M.; Pinter, M.; et al. Preliminary experience on safety of regorafenib after sorafenib failure in recurrent hepatocellular carcinoma after liver transplantation. Am. J. Transplant. 2019, 19, 3176–3184. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, M.A.; Ghobrial, R.M.; Tong, M.J.; Hiatt, J.R.; Cameron, A.M.; Hong, J.; Busuttil, R.W. Recurrence of Hepatocellular Carcinoma Following Liver Transplantation: A Review of Preoperative and Postoperative Prognostic Indicators. Arch. Surg. 2008, 143, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.H.; Cho, H.; Cho, E.J.; Lee, J.H.; Yu, S.J.; Kim, Y.J.; Yi, N.J.; Lee, K.W.; Suh, K.S.; Yoon, J.H. Efficacy of Sorafenib for the Treatment of Post-Transplant Hepatocellular Carcinoma Recurrence. J. Korean Med. Sci. 2018, 33, e283. [Google Scholar] [CrossRef] [PubMed]
- Sposito, C.; Mariani, L.; Germini, A.; Reyes, M.F.; Bongini, M.; Grossi, G.; Bhoori, S.; Mazzaferro, V. Comparative efficacy of sorafenib versus best supportive care in recurrent hepatocellular carcinoma after liver transplantation: A case-control study. J. Hepatol. 2013, 59, 59–66. [Google Scholar] [CrossRef]
- Verna, E.C.; Patel, Y.A.; Aggarwal, A.; Desai, A.P.; Frenette, C.; Pillai, A.A.; Salgia, R.; Seetharam, A.; Sharma, P.; Sherman, C.; et al. Liver transplantation for hepatocellular carcinoma: Management after the transplant. Am. J. Transplant. 2020, 20, 333–347. [Google Scholar] [CrossRef] [PubMed]
- Berenguer, M.; Burra, P.; Ghobrial, M.; Hibi, T.; Metselaar, H.; Sapisochin, G.; Bhoori, S.; Man, N.K.; Mas, V.; Ohira, M.; et al. Posttransplant management of recipients undergoing liver transplantation for hepatocellular carcinoma. Working Group Report from the ILTS Transplant Oncology Consensus Conference. Transplantation 2020, 104, 1143–1149. [Google Scholar] [CrossRef]
- Li, Y.; Gao, Z.H.; Qu, X.J. The adverse effects of sorafenib in patients with advanced cancers. Basic Clin. Pharmacol. Toxicol. 2015, 116, 216–221. [Google Scholar] [CrossRef]
- Staufer, K.; Fischer, L.; Seegers, B.; Vettorazzi, E.; Nashan, B.; Sterneck, M. High toxicity of sorafenib for recurrent hepatocellular carcinoma after liver transplantation. Transpl. Int. 2012, 25, 1158–1164. [Google Scholar] [CrossRef]
- Kim, R.; El-Gazzaz, G.; Tan, A.; Elson, P.; Byrne, M.; Chang, Y.D.; Aucejo, F. Safety and feasibility of using sorafenib in recurrent hepatocellular carcinoma after orthotopic liver transplantation. Oncology 2010, 79, 62–66. [Google Scholar] [CrossRef]
- Takahara, T.; Nitta, H.; Hasegawa, Y.; Itou, N.; Takahashi, M.; Wakabayashi, G. Using sorafenib for recurrent hepatocellular carcinoma after liver transplantation—Interactions between calcineurin inhibitor: Two case reports. Transplant. Proc. 2011, 43, 2800–2805. [Google Scholar] [CrossRef] [PubMed]
- Bins, S.; van Doorn, L.; Phelps, M.A.; Gibson, A.A.; Hu, S.; Li, L.; Vasilyeva, A.; Du, G.; Hamberg, P.; Eskens, F.A.L.M.; et al. Influence of OATP1B1 Function on the Disposition of Sorafenib-beta-D-Glucuronide. Clin. Transl. Sci. 2017, 10, 271–279. [Google Scholar] [CrossRef] [PubMed]
- Filppula, A.M.; Laitila, J.; Neuvonen, P.J.; Backman, J.T. Potent mechanism-based inhibition of CYP3A4 by imatinib explains its liability to interact with CYP3A4 substrates. Br. J. Pharmacol. 2012, 165, 2787–2798. [Google Scholar] [CrossRef] [PubMed]
- Eechoute, K.; Fransson, M.N.; Reyners, A.K.; De Jong, F.A.; Sparreboom, A.; Van Der Graaf, W.T.A.; Friberg, L.E.; Schiavon, G.; Wiemer, E.A.C.; Verweij, J.; et al. A long-term prospective population pharmacokinetic study on imatinib plasma concentrations in GIST patients. Clin. Cancer Res. 2012, 18, 5780–5787. [Google Scholar] [CrossRef] [PubMed]
- Hussaarts, K.; Veerman, G.D.M.; Jansman, F.G.A.; van Gelder, T.; Mathijssen, R.H.J.; van Leeuwen, R.W. Clinically relevant drug interactions with multikinase inhibitors: A review. Ther. Adv. Med. Oncol. 2019, 11, 1758835918818347. [Google Scholar] [CrossRef]
- Timmers, L.; Boons, C.C.L.M.; Verbrugghe, M.; Bemt, B.J.F.V.D.; Van Hecke, A.; Hugtenburg, J.G. Supporting adherence to oral anticancer agents: Clinical practice and clues to improve care provided by physicians, nurse practitioners, nurses and pharmacists. BMC Cancer 2017, 17, 122. [Google Scholar] [CrossRef]
- De Simone, P.; Crocetti, L.; Pezzati, D.; Bargellini, I.; Ghinolfi, D.; Carrai, P.; Leonardi, G.; Della Pina, C.; Cioni, D.; Pollina, L.; et al. Efficacy and Safety of Combination Therapy With Everolimus and Sorafenib for Recurrence of Hepatocellular Carcinoma After Liver Transplantation. Transplant. Proc. 2014, 46, 241–244. [Google Scholar] [CrossRef]
- Weinmann, A.; Niederle, I.M.; Koch, S.; Hoppe-Lotichius, M.; Heise, M.; Düber, C.; Schuchmann, M.; Otto, G.; Galle, P.; Wörns, M.A. Sorafenib for recurrence of hepatocellular carcinoma after liver transplantation. Dig. Liver Dis. 2012, 44, 432–437. [Google Scholar] [CrossRef]
- Castelli, G.; Burra, P.; Giacomin, A.; Vitale, A.; Senzolo, M.; Cillo, U.; Farinati, F. Sorafenib use in the transplant setting. Liver Transpl. 2014, 20, 1021–1028. [Google Scholar] [CrossRef]
- Pinter, M.; Scheiner, B.; Peck-Radosavljevic, M. Immunotherapy for advanced hepatocellular carcinoma: A focus on special subgroups. Gut 2020, 70, 204–214. [Google Scholar] [CrossRef]
- Ramadori, G.; Füzesi, L.; Grabbe, E.; Pieler, T.; Armbrust, T. Successful treatment of hepatocellular carcinoma with the tyrosine kinase inhibitor imatinib in a patient with liver cirrhosis. Anticancer Drugs. 2004, 15, 405–409. [Google Scholar] [CrossRef] [PubMed]
- Lin, A.Y.; Fisher, G.A.; So, S.; Tang, C.; Levitt, L. Phase II study of imatinib in unresectable hepatocellular carcinoma. Am. J. Clin. Oncol. 2008, 31, 84–88. [Google Scholar] [CrossRef] [PubMed]
- Delos Santos, S.; Udayakumar, S.; Nguyen, A.; Ko, Y.J.; Berry, S.; Doherty, M.; Chan, K.K. A systematic review and network meta-analysis of second-line therapy in hepatocellular carcinoma. Curr. Oncol. 2020, 27, 300–306. [Google Scholar] [CrossRef] [PubMed]
- Siegel, A.B.; El-Khoueiry, A.B.; Finn, R.S.; Guthrie, K.A.; Goyal, A.; Venook, A.P.; Blanke, C.D.; Verna, E.C.; Dove, L.; Emond, J.C.; et al. Phase I trial of sorafenib following liver transplantation in patients with high-risk hepatocellular carcinoma. Liver Cancer 2015, 4, 115–125. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Day 7 | Day 14 | |||||
|---|---|---|---|---|---|---|
| Case | AUC0–7.5h Sorafenib (mg*h/L) | Cmax Sorafenib (mg/L) | AUC0–7.5h Sorafenib (mg*h/L) | Cmax Sorafenib (mg/L) | RD AUC0–7.5h (%) | RD (%) Cmax |
| 1 | 33.4 | 8.5 | 34.1 | 6.4 | +2.1 | −24.4 |
| 2 | 47.8 | 8.7 | 48.2 | 10.7 | +0.9 | +22.1 |
| 3 | 37.6 | 6.3 | 22.6 | 4.0 | −37.3 | −40.0 |
| 4 | 24.9 | 6.0 | 13.9 | 2.3 | −62.1 | −44.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hussaarts, K.G.A.M.; van Doorn, L.; Bins, S.; Sprengers, D.; de Bruijn, P.; van Leeuwen, R.W.F.; Koolen, S.L.W.; van Gelder, T.; Mathijssen, R.H.J. Combining Sorafenib and Immunosuppression in Liver Transplant Recipients with Hepatocellular Carcinoma. Pharmaceuticals 2021, 14, 46. https://doi.org/10.3390/ph14010046
Hussaarts KGAM, van Doorn L, Bins S, Sprengers D, de Bruijn P, van Leeuwen RWF, Koolen SLW, van Gelder T, Mathijssen RHJ. Combining Sorafenib and Immunosuppression in Liver Transplant Recipients with Hepatocellular Carcinoma. Pharmaceuticals. 2021; 14(1):46. https://doi.org/10.3390/ph14010046
Chicago/Turabian StyleHussaarts, Koen G. A. M., Leni van Doorn, Sander Bins, Dave Sprengers, Peter de Bruijn, Roelof W. F. van Leeuwen, Stijn L. W. Koolen, Teun van Gelder, and Ron H. J. Mathijssen. 2021. "Combining Sorafenib and Immunosuppression in Liver Transplant Recipients with Hepatocellular Carcinoma" Pharmaceuticals 14, no. 1: 46. https://doi.org/10.3390/ph14010046
APA StyleHussaarts, K. G. A. M., van Doorn, L., Bins, S., Sprengers, D., de Bruijn, P., van Leeuwen, R. W. F., Koolen, S. L. W., van Gelder, T., & Mathijssen, R. H. J. (2021). Combining Sorafenib and Immunosuppression in Liver Transplant Recipients with Hepatocellular Carcinoma. Pharmaceuticals, 14(1), 46. https://doi.org/10.3390/ph14010046