Current Status of PSMA-Radiotracers for Prostate Cancer: Data Analysis of Prospective Trials Listed on ClinicalTrials.gov

 ,
, 
Abstract
1. Introduction
Research Question
2. Material and Methods
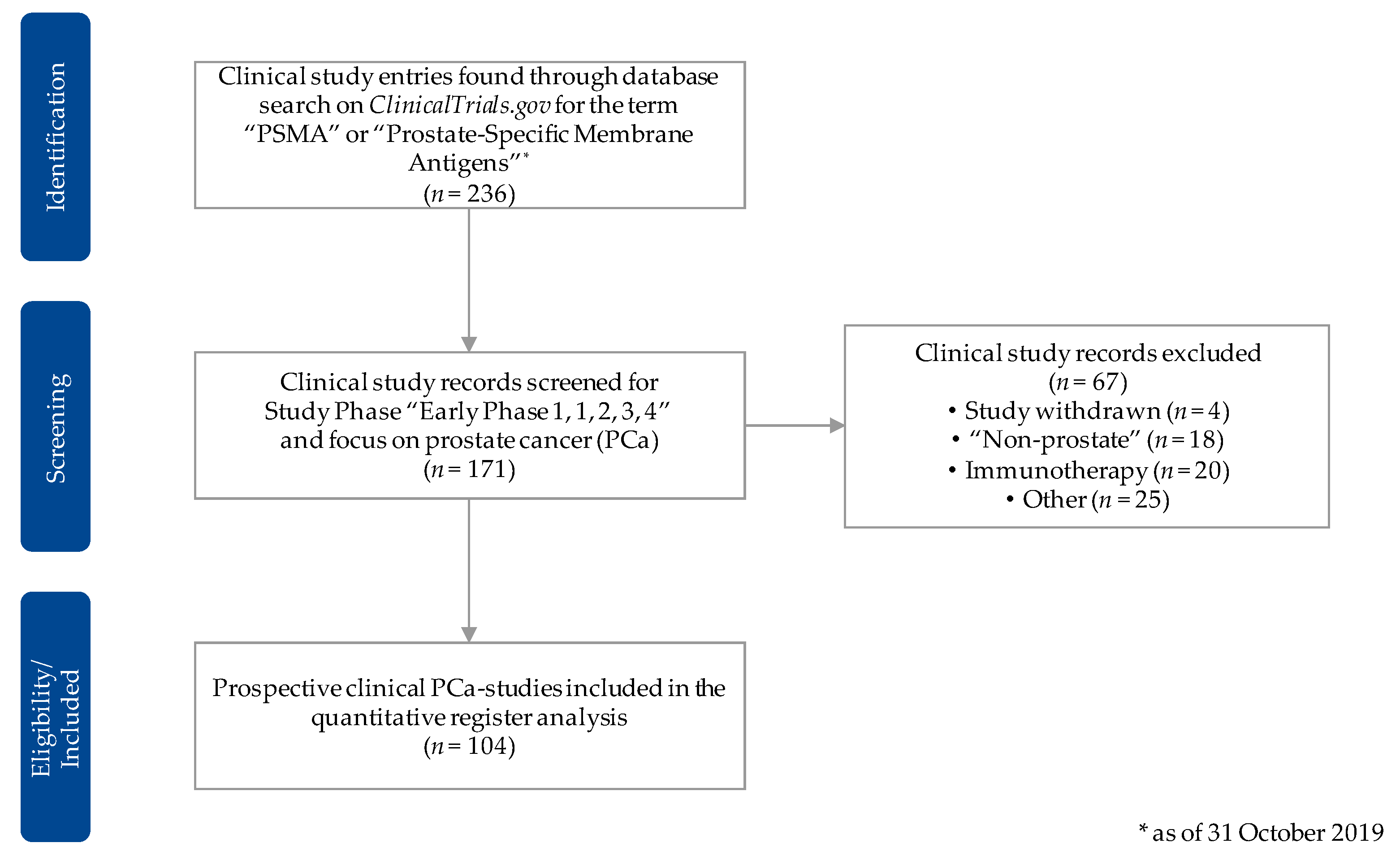
2.1. Data Source
2.2. Data Acquisition and Preprocessing
2.3. Evaluation Criteria
- Organization/cooperation: for example, study-specific collaborations and funding details;
- Recruitment: for example, the estimated enrollment, recruitment status and location;
- Study type/-design: for example, primary purpose of the study, clinical phase and type of masking or intervention model.
2.4. Statistical Analysis
3. Results
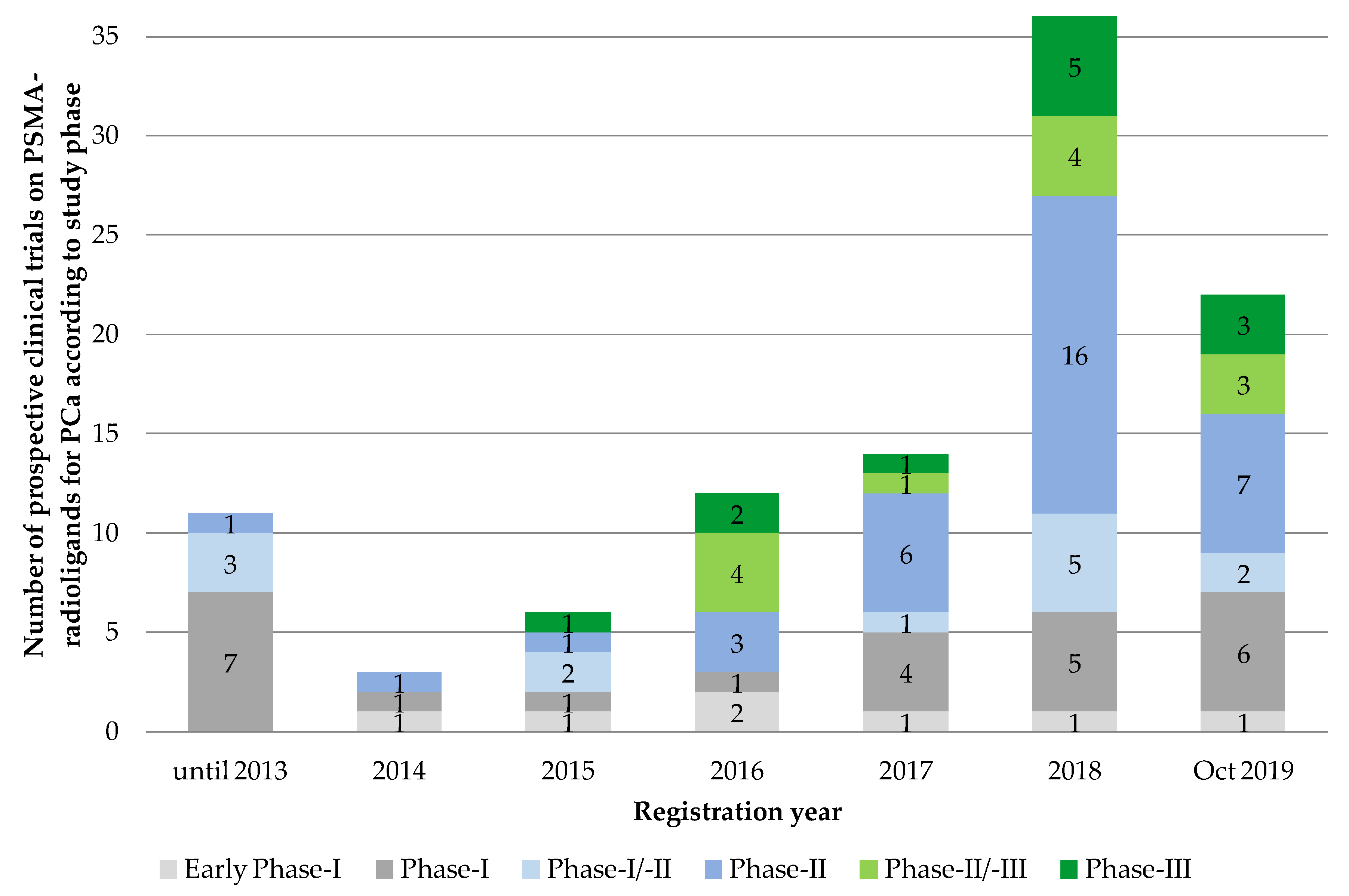
3.1. Applied PSMA-Radioligand
3.2. Study Organization
3.3. Patient Recruitment
3.4. Study Type and Design
4. Discussion and Conclusions
4.1. Development and Current Status of the Clinical Translation of PSMA-Radioligands
4.2. Study Organization and Patient Recruitment
4.3. Research Perspectives
- Multivariate analyses, for example of comparable study designs;
- Study (design) specific subanalyses of the different PSMA-radiotracers and their application fields (primary/secondary staging, BCR, radioligand-therapy, patient management);
- Compare and combine the prostate cancer-related trial registry entries on ClinicalTrials.gov with the data from other registries such as from Europe (e.g., DRKS), Asia (JPRN, ChiCTR) or Oceania (ANZCTR);
- Longitudinal studies to identify future developments in the field of novel PSMA-radiotracers, be they diagnostic or therapeutic;
- Additional detailed analyses of the free-text sections of the evaluated registry data concerning, for example, primary/secondary end points, inclusion/exclusion criteria and outcome measures.
4.4. Limitations
Author Contributions
Funding
Conflicts of Interest
References
- Kopka, K.; Benesova, M.; Barinka, C.; Haberkorn, U.; Babich, J. Glu-ureido-based inhibitors of prostate-specific membrane antigen: Lessons learned during the development of a novel class of low-molecular-weight theranostic radiotracers. J. Nucl. Med. 2017, 58, 17s–26s. [Google Scholar] [CrossRef] [PubMed]
- Virgolini, I.; Decristoforo, C.; Haug, A.; Fanti, S.; Uprimny, C. Current status of theranostics in prostate cancer. Eur. J. Nucl. Med. Mol. Imaging 2018, 45, 471–495. [Google Scholar] [CrossRef] [PubMed]
- Hope, T.A.; Afshar-Oromieh, A.; Eiber, M.; Emmett, L.; Fendler, W.P.; Lawhn-Heath, C.; Rowe, S.P. Imaging prostate cancer with prostate-specific membrane antigen pet/ct and pet/mri: Current and future applications. AJR. Am. J. Roentgenol. 2018, 211, 286–294. [Google Scholar] [CrossRef] [PubMed]
- Ruigrok, E.A.M.; van Weerden, W.M.; Nonnekens, J.; de Jong, M. The future of psma-targeted radionuclide therapy: An overview of recent preclinical research. Pharmaceutics 2019, 11, 560. [Google Scholar] [CrossRef]
- Eder, M.; Schafer, M.; Bauder-Wust, U.; Hull, W.E.; Wangler, C.; Mier, W.; Haberkorn, U.; Eisenhut, M. 68Ga-complex lipophilicity and the targeting property of a urea-based psma inhibitor for pet imaging. Bioconj. Chem. 2012, 23, 688–697. [Google Scholar] [CrossRef]
- Eder, M.; Neels, O.; Muller, M.; Bauder-Wust, U.; Remde, Y.; Schafer, M.; Hennrich, U.; Eisenhut, M.; Afshar-Oromieh, A.; Haberkorn, U.; et al. Novel preclinical and radiopharmaceutical aspects of [68Ga]Ga-PSMA-HBED-CC: A new pet tracer for imaging of prostate cancer. Pharmaceuticals 2014, 7, 779–796. [Google Scholar] [CrossRef]
- Benesova, M.; Schafer, M.; Bauder-Wust, U.; Afshar-Oromieh, A.; Kratochwil, C.; Mier, W.; Haberkorn, U.; Kopka, K.; Eder, M. Preclinical evaluation of a tailor-made dota-conjugated psma inhibitor with optimized linker moiety for imaging and endoradiotherapy of prostate cancer. J. Nucl. Med. 2015, 56, 914–920. [Google Scholar] [CrossRef]
- Cardinale, J.; Martin, R.; Remde, Y.; Schafer, M.; Hienzsch, A.; Hubner, S.; Zerges, A.M.; Marx, H.; Hesse, R.; Weber, K.; et al. Procedures for the gmp-compliant production and quality control of [(18)f]psma-1007: A next generation radiofluorinated tracer for the detection of prostate cancer. Pharmaceuticals 2017, 10, 77. [Google Scholar] [CrossRef]
- Cardinale, J.; Schafer, M.; Benesova, M.; Bauder-Wust, U.; Leotta, K.; Eder, M.; Neels, O.C.; Haberkorn, U.; Giesel, F.L.; Kopka, K. Preclinical evaluation of (18)f-psma-1007, a new prostate-specific membrane antigen ligand for prostate cancer imaging. J. Nucl. Med. 2017, 58, 425–431. [Google Scholar] [CrossRef]
- Robu, S.; Schottelius, M.; Eiber, M.; Maurer, T.; Gschwend, J.; Schwaiger, M.; Wester, H.J. Preclinical evaluation and first patient application of 99mtc-psma-i&s for spect imaging and radioguided surgery in prostate cancer. J. Nucl. Med. 2017, 58, 235–242. [Google Scholar]
- Chen, Y.; Pullambhatla, M.; Foss, C.A.; Byun, Y.; Nimmagadda, S.; Senthamizhchelvan, S.; Sgouros, G.; Mease, R.C.; Pomper, M.G. 2-(3-{1-carboxy-5-[(6-[18f]fluoro-pyridine-3-carbonyl)-amino]-pentyl}-ureido)-pen tanedioic acid, [18f]dcfpyl, a psma-based pet imaging agent for prostate cancer. Clin. Cancer Res. 2011, 17, 7645–7653. [Google Scholar] [CrossRef] [PubMed]
- Cho, S.Y.; Gage, K.L.; Mease, R.C.; Senthamizhchelvan, S.; Holt, D.P.; Jeffrey-Kwanisai, A.; Endres, C.J.; Dannals, R.F.; Sgouros, G.; Lodge, M.; et al. Biodistribution, tumor detection, and radiation dosimetry of 18f-dcfbc, a low-molecular-weight inhibitor of prostate-specific membrane antigen, in patients with metastatic prostate cancer. J. Nucl. Med. 2012, 53, 1883–1891. [Google Scholar] [CrossRef] [PubMed]
- Afshar-Oromieh, A.; Malcher, A.; Eder, M.; Eisenhut, M.; Linhart, H.G.; Hadaschik, B.A.; Holland-Letz, T.; Giesel, F.L.; Kratochwil, C.; Haufe, S.; et al. Pet imaging with a [68Ga]gallium-labelled psma ligand for the diagnosis of prostate cancer: Biodistribution in humans and first evaluation of tumour lesions. Eur. J. Nucl. Med. Mol. Imaging 2013, 40, 486–495. [Google Scholar] [CrossRef] [PubMed]
- Afshar-Oromieh, A.; Babich, J.W.; Kratochwil, C.; Giesel, F.L.; Eisenhut, M.; Kopka, K.; Haberkorn, U. The rise of psma ligands for diagnosis and therapy of prostate cancer. J. Nucl. Med. 2016, 57, 79s–89s. [Google Scholar] [CrossRef] [PubMed]
- Giesel, F.L.; Hadaschik, B.; Cardinale, J.; Radtke, J.; Vinsensia, M.; Lehnert, W.; Kesch, C.; Tolstov, Y.; Singer, S.; Grabe, N.; et al. F-18 labelled psma-1007: Biodistribution, radiation dosimetry and histopathological validation of tumor lesions in prostate cancer patients. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 678–688. [Google Scholar] [CrossRef]
- Rahbar, K.; Ahmadzadehfar, H.; Kratochwil, C.; Haberkorn, U.; Schafers, M.; Essler, M.; Baum, R.P.; Kulkarni, H.R.; Schmidt, M.; Drzezga, A.; et al. German multicenter study investigating 177Lu-PSMA-617 radioligand therapy in advanced prostate cancer patients. J. Nucl. Med. 2017, 58, 85–90. [Google Scholar] [CrossRef]
- Rowe, S.P.; Macura, K.J.; Mena, E.; Blackford, A.L.; Nadal, R.; Antonarakis, E.S.; Eisenberger, M.; Carducci, M.; Fan, H.; Dannals, R.F.; et al. PSMA-based [18F]DCFPyL PET/CT is superior to conventional imaging for lesion detection in patients with metastatic prostate cancer. Mol. Imaging Biol. 2016, 18, 411–419. [Google Scholar] [CrossRef]
- Rowe, S.P.; Macura, K.J.; Ciarallo, A.; Mena, E.; Blackford, A.; Nadal, R.; Antonarakis, E.S.; Eisenberger, M.A.; Carducci, M.A.; Ross, A.E.; et al. Comparison of prostate-specific membrane antigen-based 18f-dcfbc pet/ct to conventional imaging modalities for detection of hormone-naive and castration-resistant metastatic prostate cancer. J. Nucl. Med. 2016, 57, 46–53. [Google Scholar] [CrossRef]
- Nielsen, J.B.; Zacho, H.D.; Haberkorn, U.; Nielsen, K.M.; Dettmann, K.; Langkilde, N.C.; Petersen, L.J. A comprehensive safety evaluation of 68Ga-labeled ligand prostate-specific membrane antigen 11 pet/ct in prostate cancer: The results of 2 prospective, multicenter trials. Clin. Nucl. Med. 2017, 42, 520–524. [Google Scholar] [CrossRef]
- Hofman, M.S.; Violet, J.; Hicks, R.J.; Ferdinandus, J.; Thang, S.P.; Akhurst, T.; Iravani, A.; Kong, G.; Ravi Kumar, A.; Murphy, D.G.; et al. [177Lu]-PSMA-617 radionuclide treatment in patients with metastatic castration-resistant prostate cancer (lupsma trial): A single-centre, single-arm, phase 2 study. Lancet Oncol. 2018, 19, 825–833. [Google Scholar] [CrossRef]
- Fendler, W.P.; Calais, J.; Eiber, M.; Flavell, R.R.; Mishoe, A.; Feng, F.Y.; Nguyen, H.G.; Reiter, R.E.; Rettig, M.B.; Okamoto, S.; et al. Assessment of 68Ga-PSMA-11 pet accuracy in localizing recurrent prostate cancer: A prospective single-arm clinical trial. JAMA Oncol. 2019, 5, 856–863. [Google Scholar] [CrossRef]
- McCray, A.T.; Ide, N.C. Design and implementation of a national clinical trials registry. J. Am. Med. Inform. Assoc. JAMIA 2000, 7, 313–323. [Google Scholar] [CrossRef] [PubMed]
- Hirsch, B.R.; Califf, R.M.; Cheng, S.K.; Tasneem, A.; Horton, J.; Chiswell, K.; Schulman, K.A.; Dilts, D.M.; Abernethy, A.P. Characteristics of oncology clinical trials: Insights from a systematic analysis of ClinicalTrials.gov. JAMA Intern. Med. 2013, 173, 972–979. [Google Scholar] [CrossRef] [PubMed]
- Bell, S.A.; Tudur Smith, C. A comparison of interventional clinical trials in rare versus non-rare diseases: An analysis of ClinicalTrials.gov. Orphanet J. Rare Dis. 2014, 9, 170. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.P.; Lv, J.W.; Liu, X.; Zhang, Y.; Guo, Y.; Lin, A.H.; Sun, Y.; Mao, Y.P.; Ma, J. The landscape of clinical trials evaluating the theranostic role of pet imaging in oncology: Insights from an analysis of ClinicalTrials.gov database. Theranostics 2017, 7, 390–399. [Google Scholar] [CrossRef] [PubMed]
- Zarin, D.A.; Tse, T.; Ide, N.C. Trial registration at ClinicalTrials.gov between may and october 2005. N. Engl. J. Med. 2005, 353, 2779–2787. [Google Scholar] [CrossRef]
- Zarin, D.A.; Tse, T.; Williams, R.J.; Califf, R.M.; Ide, N.C. The ClinicalTrials.gov results database—Update and key issues. N. Engl. J. Med. 2011, 364, 852–860. [Google Scholar] [CrossRef]
- McCray, A.T. Better access to information about clinical trials. Ann. Intern. Med. 2000, 133, 609–614. [Google Scholar] [CrossRef]
- Zarin, D.A.; Keselman, A. Registering a clinical trial in ClinicalTrials.gov. Chest 2007, 131, 909–912. [Google Scholar] [CrossRef]
- U.S. National Library of Medicine. ClinicalTrials.gov → Advanced Search. Available online: https://clinicaltrials.gov/ct2/search/advanced (accessed on 31 October 2019).
- Kiess, A.P.; Banerjee, S.R.; Mease, R.C.; Rowe, S.P.; Rao, A.; Foss, C.A.; Chen, Y.; Yang, X.; Cho, S.Y.; Nimmagadda, S.; et al. Prostate-specific membrane antigen as a target for cancer imaging and therapy. Q. J. Nucl. Med. Mol. Imaging 2015, 59, 241–268. [Google Scholar]
- Rahbar, K.; Afshar-Oromieh, A.; Jadvar, H.; Ahmadzadehfar, H. Psma theranostics: Current status and future directions. Mol. Imaging 2018, 17. [Google Scholar] [CrossRef]
- Kratochwil, C.; Haberkorn, U.; Giesel, F.L. Radionuclide therapy of metastatic prostate cancer. Semin. Nucl. Med. 2019, 49, 313–325. [Google Scholar] [CrossRef] [PubMed]
- Kesch, C.; Kratochwil, C.; Mier, W.; Kopka, K.; Giesel, F.L. 68Ga or 18F for prostate cancer imaging? J. Nucl. Med. 2017, 58, 687–688. [Google Scholar] [CrossRef] [PubMed]
- Zippel, C.; Neels, O.C.; Hennrich, U.; Giesel, F.L.; Kopka, K. Initiation of clinical multicentre studies with local radiotracer production—Regulatory environment and radiopharmaceutical-organisational aspects. Nuklearmed. Nucl. Med. 2019, 58, 77–85. [Google Scholar]
- Decristoforo, C.; Penuelas, I.; Patt, M.; Todde, S. European regulations for the introduction of novel radiopharmaceuticals in the clinical setting. Q. J. Nucl. Med. Mol. Imaging 2017, 61, 135–144. [Google Scholar]
- Rahbar, K.; Bodei, L.; Morris, M.J. Is the vision of radioligand therapy for prostate cancer becoming a reality? An overview of the phase iii vision trial and its importance for the future of theranostics. J. Nucl. Med. 2019, 60, 1504–1506. [Google Scholar] [CrossRef]
- Iravani, A.; Violet, J.; Azad, A.; Hofman, M.S. Lutetium-177 prostate-specific membrane antigen (PSMA) theranostics: Practical nuances and intricacies. Prostate Cancer Prostatic Dis. 2019, 1–15. [Google Scholar] [CrossRef]
- Califf, R.M.; Zarin, D.A.; Kramer, J.M.; Sherman, R.E.; Aberle, L.H.; Tasneem, A. Characteristics of clinical trials registered in ClinicalTrials.gov, 2007–2010. JAMA 2012, 307, 1838–1847. [Google Scholar] [CrossRef]
- Zarin, D.A.; Tse, T.; Williams, R.J.; Carr, S. Trial reporting in ClinicalTrials.gov—The Final Rule. N. Engl. J. Med. 2016, 375, 1998–2004. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Absolute (n) | Relative (%) * | |
|---|---|---|
| Applied PSMA radioligand | ||
| [68Ga]Ga-PSMA-11 | 33 | 32 |
| [18F]DCFPyL | 25 | 24 |
| [177Lu]Lu-PSMA-617 | 10 | 10 |
| Other (e.g., [99mTc]Tc-MIP-1404, [18F]DCFBC, [18F]PSMA-1007) | 36 | 35 |
| Organization/Cooperation | ||
| Single-center/Multi-center | ||
| Single-center | 88 | 85 |
| Multi-center | 16 | 15 |
| National/International | ||
| National | 99 | 95 |
| International | 5 | 5 |
| Funding source ** | ||
| Industry | 31 | 30 |
| NIH | 20 | 19 |
| Other U.S. Federal agency | 1 | 1 |
| All others (individuals, universities, organizations) | 81 | 78 |
| Absolute (n) | Relative (%) * | |
|---|---|---|
| Study status ** | ||
| Patient recruitment | ||
| Open | 60 | 58 |
| Not open | 44 | 42 |
| Recruitment status | ||
| Recruiting | 50 | 48 |
| Completed | 25 | 24 |
| Active, not recruiting | 13 | 13 |
| Not yet recruiting | 10 | 10 |
| Enrolling by invitation | 5 | 5 |
| Unknown status | 1 | 1 |
| Estimated enrollment (number of patients) | ||
| 1–25 | 29 | 28 |
| 26–50 | 23 | 22 |
| 51–100 | 16 | 15 |
| 101–250 | 21 | 20 |
| 251–1000 | 14 | 13 |
| >1000 | 1 | 1 |
| Location/country *** | ||
| United States of America | 73 | 70 |
| Canada | 14 | 13 |
| France | 6 | 6 |
| Belgium | 5 | 5 |
| Australia | 3 | 3 |
| Other (Austria, Germany, UK, China, etc.) | 15 | 14 |
| Absolute (n) | Relative (%) * | |
|---|---|---|
| Study phase | ||
| Early Phase-I | 7 | 7 |
| Phase-I | 25 | 24 |
| Phase-I/-II | 13 | 13 |
| Phase-II | 35 | 34 |
| Phase-II/-III | 12 | 12 |
| Phase-III | 12 | 12 |
| Primary purpose | ||
| Diagnostic | 75 | 72 |
| Treatment | 24 | 23 |
| Screening | 3 | 3 |
| Basic Science | 1 | 1 |
| Other | 1 | 1 |
| Allocation | ||
| Non-Randomized | 17 | 16 |
| Randomized | 17 | 16 |
| Not specified | 70 | 67 |
| Masking | ||
| None (Open Label) | 99 | 95 |
| Masked | 5 | 5 |
| Single (investigator) | 1 | 1 |
| Single (participant) | 2 | 2 |
| Double or triple | 2 | 2 |
| Intervention model | ||
| Single Group Assignment | 72 | 69 |
| Parallel Assignment | 20 | 19 |
| Sequential Assignment | 6 | 6 |
| Crossover Assignment | 6 | 6 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zippel, C.; Ronski, S.C.; Bohnet-Joschko, S.; Giesel, F.L.; Kopka, K. Current Status of PSMA-Radiotracers for Prostate Cancer: Data Analysis of Prospective Trials Listed on ClinicalTrials.gov. Pharmaceuticals 2020, 13, 12. https://doi.org/10.3390/ph13010012
Zippel C, Ronski SC, Bohnet-Joschko S, Giesel FL, Kopka K. Current Status of PSMA-Radiotracers for Prostate Cancer: Data Analysis of Prospective Trials Listed on ClinicalTrials.gov. Pharmaceuticals. 2020; 13(1):12. https://doi.org/10.3390/ph13010012
Chicago/Turabian StyleZippel, Claus, Sarah C. Ronski, Sabine Bohnet-Joschko, Frederik L. Giesel, and Klaus Kopka. 2020. "Current Status of PSMA-Radiotracers for Prostate Cancer: Data Analysis of Prospective Trials Listed on ClinicalTrials.gov" Pharmaceuticals 13, no. 1: 12. https://doi.org/10.3390/ph13010012
APA StyleZippel, C., Ronski, S. C., Bohnet-Joschko, S., Giesel, F. L., & Kopka, K. (2020). Current Status of PSMA-Radiotracers for Prostate Cancer: Data Analysis of Prospective Trials Listed on ClinicalTrials.gov. Pharmaceuticals, 13(1), 12. https://doi.org/10.3390/ph13010012