
Quantification of 3D Kinematic Measurements for Knee Flexion and Tibial Rotation Using an IMU-Based Sensor and Ultrasound Imaging System: A Cadaveric Study

Abstract
1. Introduction
1.1. Clinical Significance of Knee Rotational Stability
1.2. Limitations of Current Assessment Methods
1.3. Challenges with Existing Measurement Technologies
1.4. Objective
2. Materials and Methods
2.1. GATOR System Description
2.2. Reference Measurement System
2.3. Cadaveric Specimens
2.4. Experimental Setup
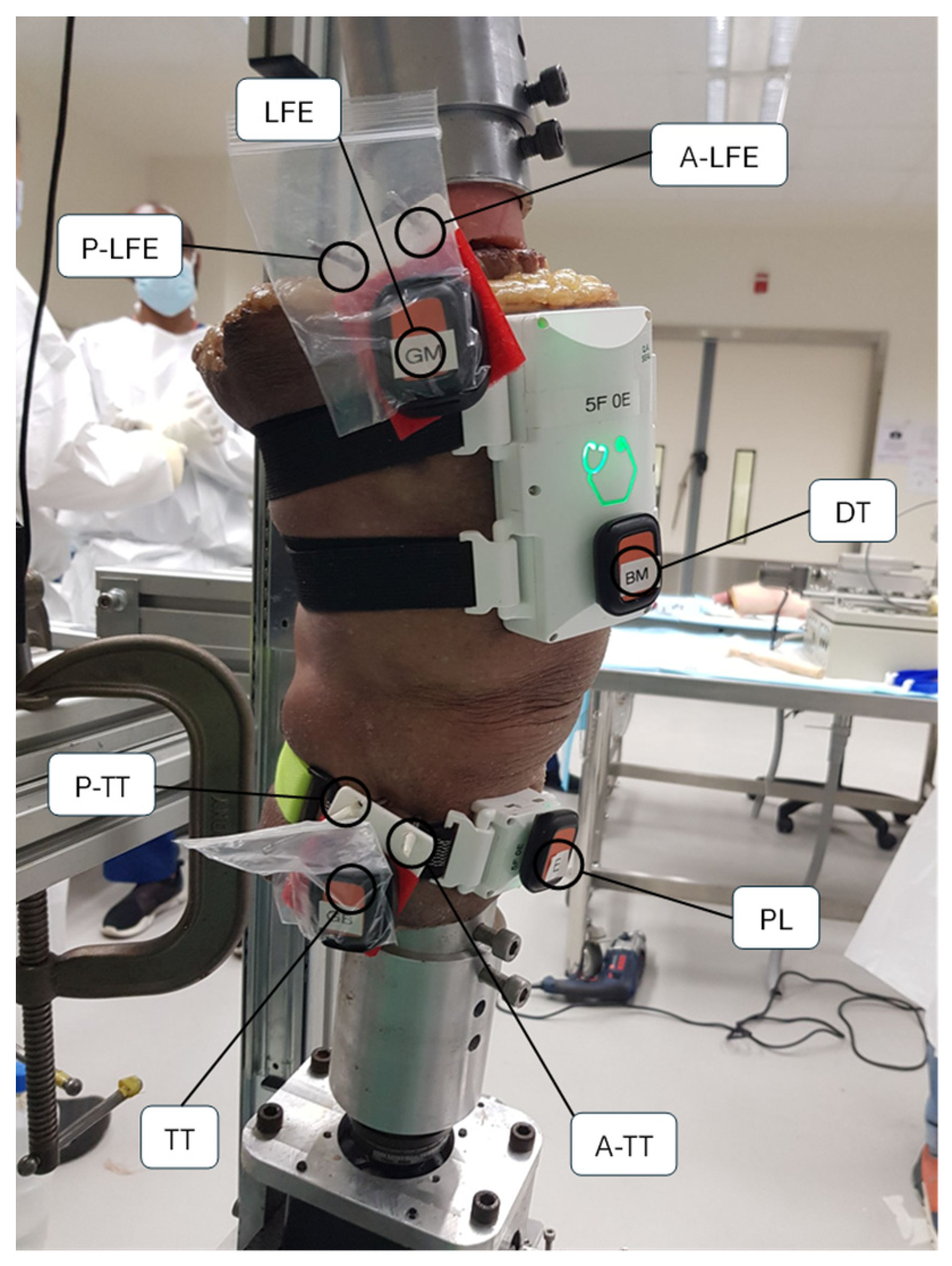
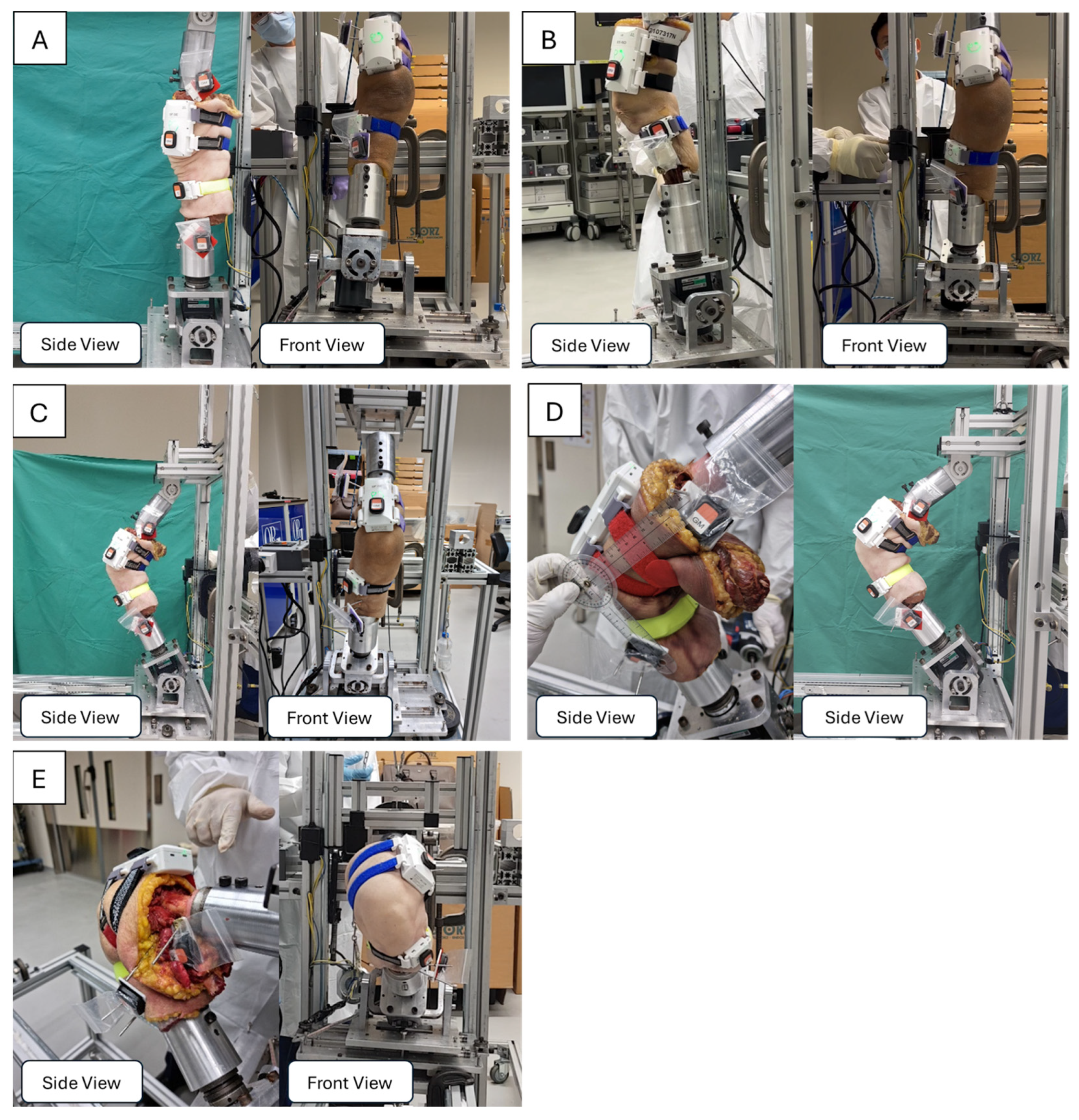
2.4.1. Specimen Fixation and Positioning
2.4.2. Instrumentation and Data Acquisition
2.5. Calibration Procedures
2.6. Experimental Protocols
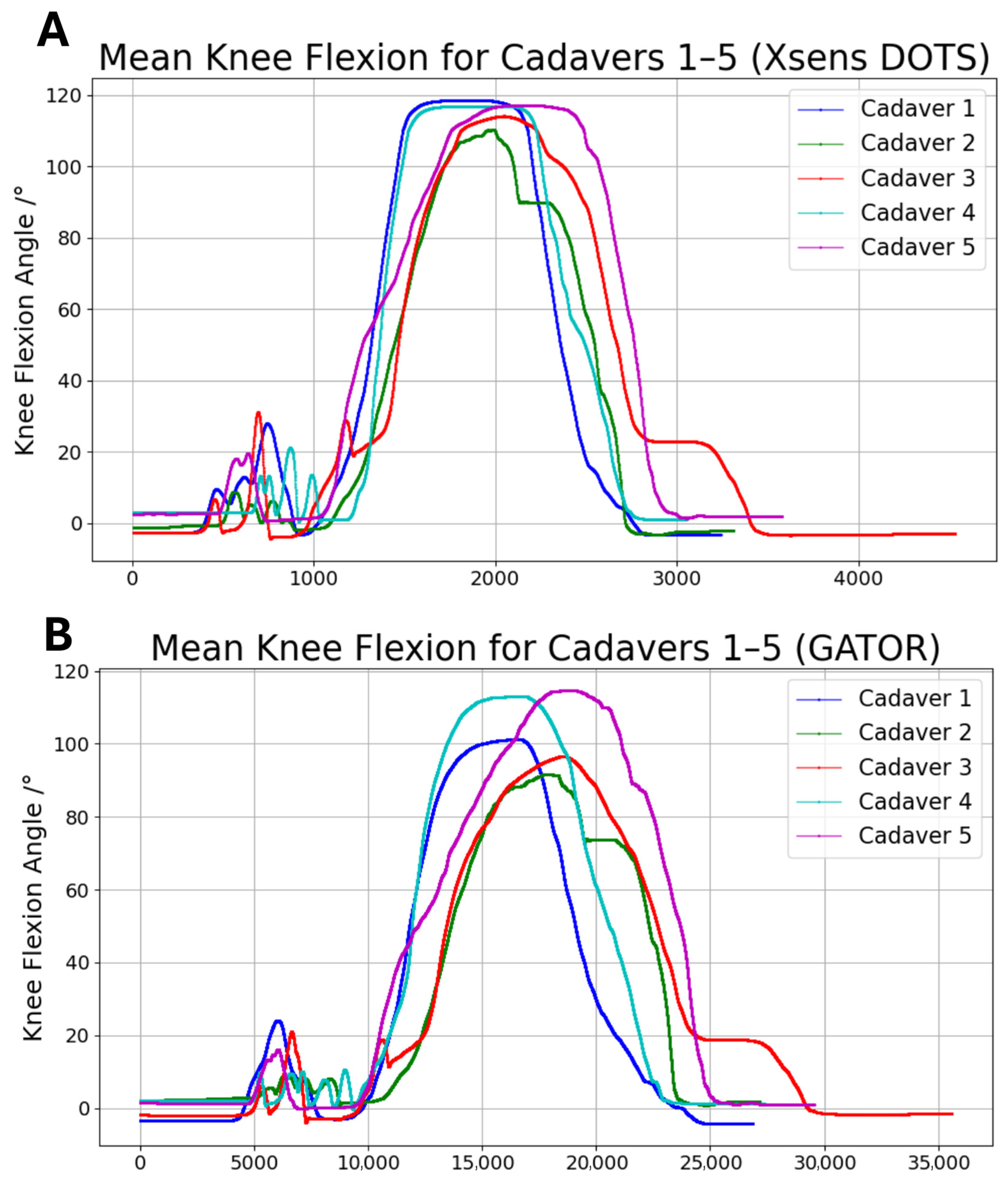
2.6.1. Experiment A: Measurement of Flexion Range of Motion
2.6.2. Experiment B: Measurement of Relative Tibial and Femoral Rotation
2.6.3. Statistical Analysis
3. Results
4. Discussion
4.1. Accuracy and Repeatability of GATOR
4.2. Limitations
4.3. Potential Clinical Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACL | Anterior Cruciate Ligament |
| IMU | Inertial Measurement Unit |
| STA | Soft Tissue Artifact |
| RMSE | Root Mean Square Error |
| LoA | Limits of Agreement |
| R2 | Coefficient of Determination |
| SD | Standard Deviation |
| CI | Confidence Interval |
References
- Hallén, L.G.; Lindahl, O. Rotation in the Knee-Joint in Experimental Injury to the Ligaments. Acta Orthop. Scand. 1965, 36, 400–407. [Google Scholar] [CrossRef] [PubMed]
- Fuss, F.K. Principles and Mechanisms of Automatic Rotation during Terminal Extension in the Human Knee Joint. J. Anat. 1992, 180 Pt 2, 297–304. [Google Scholar]
- Hallén, L.G.; Lindahl, O. The “Screw-Home” Movement in the Knee-Joint. Acta Orthop. Scand. 1966, 37, 97–106. [Google Scholar] [CrossRef] [PubMed]
- Kuegler, P.; Wurzer, P.; Tuca, A.; Sendlhofer, G.; Lumenta, D.B.; Giretzlehner, M.; Kamolz, L.-P. Goniometer-Apps in Hand Surgery and Their Applicability in Daily Clinical Practice. Saf. Health 2015, 1, 11. [Google Scholar] [CrossRef]
- Lohmander, L.S.; Englund, P.M.; Dahl, L.L.; Roos, E.M. The Long-Term Consequence of Anterior Cruciate Ligament and Meniscus Injuries: Osteoarthritis. Am. J. Sports Med. 2007, 35, 1756–1769. [Google Scholar] [CrossRef]
- Lopomo, N.; Signorelli, C.; Bonanzinga, T.; Marcheggiani Muccioli, G.M.; Visani, A.; Zaffagnini, S. Quantitative Assessment of Pivot-Shift Using Inertial Sensors. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 713–717. [Google Scholar] [CrossRef] [PubMed]
- Sundemo, D.; Alentorn-Geli, E.; Hoshino, Y.; Musahl, V.; Karlsson, J.; Samuelsson, K. Objective Measures on Knee Instability: Dynamic Tests: A Review of Devices for Assessment of Dynamic Knee Laxity through Utilization of the Pivot Shift Test. Curr. Rev. Musculoskelet. Med. 2016, 9, 148–159. [Google Scholar] [CrossRef]
- Lee, D.W.; Lee, J.H.; Kim, D.H.; Park, J.H.; Kim, J.G. Quantitative Measures of Pivot Shift on Knee Rotatory Instability. Aosm 2018, 5, 11–18. [Google Scholar] [CrossRef]
- Grassi, A.; Lopomo, N.F.; Rao, A.M.; Abuharfiel, A.N.; Zaffagnini, S. No Proof for the Best Instrumented Device to Grade the Pivot Shift Test: A Systematic Review. J. ISAKOS 2016, 1, 269–275. [Google Scholar] [CrossRef]
- Hoshino, Y.; Araujo, P.; Ahlden, M.; Moore, C.G.; Kuroda, R.; Zaffagnini, S.; Karlsson, J.; Fu, F.H.; Musahl, V. Standardized Pivot Shift Test Improves Measurement Accuracy. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 732–736. [Google Scholar] [CrossRef]
- Horvath, A.; Meredith, S.J.; Nishida, K.; Hoshino, Y.; Musahl, V. Objectifying the Pivot Shift Test. Sports Med. Arthrosc. Rev. 2020, 28, 36–40. [Google Scholar] [CrossRef]
- Vind, T.D.; Petersen, E.T.; Sørensen, O.G.; Lindgren, L.; Stilling, M. Dynamic Radiostereometry Can Objectively Quantify the Kinematic Laxity Patterns and Rotation Instability of the Knee during a Pivot-shift Test. Knee Surg. Sports Traumatol. Arthrosc. 2024, 32, 1492–1506. [Google Scholar] [CrossRef] [PubMed]
- Tan, T.; Gatti, A.A.; Fan, B.; Shea, K.G.; Sherman, S.L.; Uhlrich, S.D.; Hicks, J.L.; Delp, S.L.; Shull, P.B.; Chaudhari, A.S. A Scoping Review of Portable Sensing for Out-of-Lab Anterior Cruciate Ligament Injury Prevention and Rehabilitation. npj Digit. Med. 2023, 6, 46. [Google Scholar] [CrossRef] [PubMed]
- Lam, M.-H.; Fong, D.T.; Yung, P.S.; Ho, E.P.; Chan, W.-Y.; Chan, K.-M. Knee Stability Assessment on Anterior Cruciate Ligament Injury: Clinical and Biomechanical Approaches. BMC Sports Sci. Med. Rehabil. 2009, 1, 20. [Google Scholar] [CrossRef]
- Lange, T.; Freiberg, A.; Dröge, P.; Lützner, J.; Schmitt, J.; Kopkow, C. The Reliability of Physical Examination Tests for the Diagnosis of Anterior Cruciate Ligament Rupture—A Systematic Review. Man. Ther. 2015, 20, 402–411. [Google Scholar] [CrossRef]
- Peeler, J.; Leiter, J.; MacDonald, P. Accuracy and Reliability of Anterior Cruciate Ligament Clinical Examination in a Multidisciplinary Sports Medicine Setting. Clin. J. Sport Med. 2010, 20, 80–85. [Google Scholar] [CrossRef]
- Kuroda, R.; Hoshino, Y.; Kubo, S.; Araki, D.; Oka, S.; Nagamune, K.; Kurosaka, M. Similarities and Differences of Diagnostic Manual Tests for Anterior Cruciate Ligament Insufficiency: A Global Survey and Kinematics Assessment. Am. J. Sports Med. 2012, 40, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Prakash, U.; Wigderowitz, C.A.; McGurty, D.W.; Rowley, D.I. Computerised Measurement of Tibiofemoral Alignment. J. Bone Jt. Surg. Br. Vol. 2001, 83-B, 819–824. [Google Scholar] [CrossRef]
- Mizner, R.L.; Chmielewski, T.L.; Toepke, J.J.; Tofte, K.B. Comparison of 2-Dimensional Measurement Techniques for Predicting Knee Angle and Moment During a Drop Vertical Jump. Clin. J. Sport Med. 2012, 22, 221–227. [Google Scholar] [CrossRef]
- Cappozzo, A.; Della Croce, U.; Leardini, A.; Chiari, L. Human Movement Analysis Using Stereophotogrammetry. Gait Posture 2005, 21, 186–196. [Google Scholar] [CrossRef]
- Cooper, G.; Sheret, I.; McMillian, L.; Siliverdis, K.; Sha, N.; Hodgins, D.; Kenney, L.; Howard, D. Inertial Sensor-Based Knee Flexion/Extension Angle Estimation. J. Biomech. 2009, 42, 2678–2685. [Google Scholar] [CrossRef] [PubMed]
- Ghattas, J.; Jarvis, D.N. Validity of Inertial Measurement Units for Tracking Human Motion: A Systematic Review. Sports Biomech. 2024, 23, 1853–1866. [Google Scholar] [CrossRef] [PubMed]
- Caruso, K. Validation of Meta Motion IMU Sensors Through Measurement of Knee Angles During Gait. Master’s Thesis, Old Dominion University, Norfolk, Virginia, 2023. [Google Scholar] [CrossRef]
- Beyea, J.; McGibbon, C.A.; Sexton, A.; Noble, J.; O’Connell, C. Convergent Validity of a Wearable Sensor System for Measuring Sub-Task Performance during the Timed Up-and-Go Test. Sensors 2017, 17, 934. [Google Scholar] [CrossRef]
- Morishige, Y.; Harato, K.; Oki, S.; Kaneda, K.; Niki, Y.; Nakamura, M.; Nagura, T. Four-Dimensional Computed Tomographic Analysis of Screw Home Movement in Patients with Anterior Cruciate Ligament Deficient Knee—A 3D-3D Registration Technique. Skelet. Radiol. 2022, 51, 1679–1685. [Google Scholar] [CrossRef] [PubMed]
- Miranda, D.L.; Rainbow, M.J.; Crisco, J.J.; Fleming, B.C. Kinematic Differences between Optical Motion Capture and Biplanar Videoradiography during a Jump–Cut Maneuver. J. Biomech. 2013, 46, 567–573. [Google Scholar] [CrossRef]
- Wang, S.; Zeng, X.; Huangfu, L.; Xie, Z.; Ma, L.; Huang, W.; Zhang, Y. Validation of a Portable Marker-Based Motion Analysis System. J. Orthop. Surg. Res. 2021, 16, 425. [Google Scholar] [CrossRef]
- Giphart, J.E.; Zirker, C.A.; Myers, C.A.; Pennington, W.W.; LaPrade, R.F. Accuracy of a Contour-Based Biplane Fluoroscopy Technique for Tracking Knee Joint Kinematics of Different Speeds. J. Biomech. 2012, 45, 2935–2938. [Google Scholar] [CrossRef]
- Kessler, S.E.; Rainbow, M.J.; Lichtwark, G.A.; Cresswell, A.G.; D’Andrea, S.E.; Konow, N.; Kelly, L.A. A Direct Comparison of Biplanar Videoradiography and Optical Motion Capture for Foot and Ankle Kinematics. Front. Bioeng. Biotechnol. 2019, 7, 199. [Google Scholar] [CrossRef]
- Gransberg, L. Velocity Controlled Dynamometry and Gait Analysis: Development of Methods and Applications; Karolinska Institutets bibl.: Stockholm, Sweden, 2001. [Google Scholar]
- Mills, P.M.; Morrison, S.; Lloyd, D.G.; Barrett, R.S. Repeatability of 3D Gait Kinematics Obtained from an Electromagnetic Tracking System during Treadmill Locomotion. J. Biomech. 2007, 40, 1504–1511. [Google Scholar] [CrossRef]
- Aminian, K.; Najafi, B. Capturing Human Motion Using Body-fixed Sensors: Outdoor Measurement and Clinical Applications. Comput. Animat. Virtual 2004, 15, 79–94. [Google Scholar] [CrossRef]
- Pacher, L.; Chatellier, C.; Vauzelle, R.; Fradet, L. Sensor-to-Segment Calibration Methodologies for Lower-Body Kinematic Analysis with Inertial Sensors: A Systematic Review. Sensors 2020, 20, 3322. [Google Scholar] [CrossRef] [PubMed]
- Bonci, T.; Camomilla, V.; Dumas, R.; Chèze, L.; Cappozzo, A. Rigid and Non-Rigid Geometrical Transformations of a Marker-Cluster and Their Impact on Bone-Pose Estimation. J. Biomech. 2015, 48, 4166–4172. [Google Scholar] [CrossRef] [PubMed]
- Dumas, R.; Camomilla, V.; Bonci, T.; Cheze, L.; Cappozzo, A. A Qualitative Analysis of Soft Tissue Artefact during Running. Comput. Methods Biomech. Biomed. Eng. 2014, 17 (Suppl. S1), 124–125. [Google Scholar] [CrossRef] [PubMed]
- Benoit, D.L.; Damsgaard, M.; Andersen, M.S. Surface Marker Cluster Translation, Rotation, Scaling and Deformation: Their Contribution to Soft Tissue Artefact and Impact on Knee Joint Kinematics. J. Biomech. 2015, 48, 2124–2129. [Google Scholar] [CrossRef]
- Barre, A.; Thiran, J.-P.; Jolles, B.M.; Theumann, N.; Aminian, K. Soft Tissue Artifact Assessment During Treadmill Walking in Subjects with Total Knee Arthroplasty. IEEE Trans. Biomed. Eng. 2013, 60, 3131–3140. [Google Scholar] [CrossRef]
- Andersen, M.S.; Damsgaard, M.; Rasmussen, J.; Ramsey, D.K.; Benoit, D.L. A Linear Soft Tissue Artefact Model for Human Movement Analysis: Proof of Concept Using in Vivo Data. Gait Posture 2012, 35, 606–611. [Google Scholar] [CrossRef]
- Clément, J.; De Guise, J.A.; Fuentes, A.; Hagemeister, N. Comparison of Soft Tissue Artifact and Its Effects on Knee Kinematics between Non-Obese and Obese Subjects Performing a Squatting Activity Recorded Using an Exoskeleton. Gait Posture 2018, 61, 197–203. [Google Scholar] [CrossRef]
- Alcala, E.R.; Voerman, J.A.; Konrath, J.M.; Vydhyanathan, A. Xsens DOT Wearable Sensor Platform White Paper. 2021. Available online: https://www.movella.com/hubfs/Downloads/Whitepapers/Xsens%20DOT%20WhitePaper.pdf (accessed on 2 July 2025).
- Di Raimondo, G.; Vanwanseele, B.; Van Der Have, A.; Emmerzaal, J.; Willems, M.; Killen, B.A.; Jonkers, I. Inertial Sensor-to-Segment Calibration for Accurate 3D Joint Angle Calculation for Use in OpenSim. Sensors 2022, 22, 3259. [Google Scholar] [CrossRef]
- Buckley, N.; Davey, P.; Jensen, L.; Baptist, K.; Jansen, B.; Campbell, A.; Downs, J. Can Wearable Inertial Measurement Units Be Used to Measure Sleep Biomechanics? Establishing Initial Feasibility and Validity. Biomimetics 2022, 8, 2. [Google Scholar] [CrossRef]
- Beange, K.H.E.; Chan, A.D.C.; Graham, R.B. Can We Reliably Assess Spine Movement Quality in Clinics? A Comparison of Systems to Evaluate Movement Reliability in a Healthy Population. J. Biomech. 2025, 179, 112415. [Google Scholar] [CrossRef]
- Cudejko, T.; Button, K.; Al-Amri, M. Validity of Orientations and Accelerations Measured Using Xsens DOT Inertial Measurement Unit during Functional Activities. Gait Posture 2022, 97, S341–S342. [Google Scholar] [CrossRef]
- Roetenberg, D.; Slycke, P.J.; Veltink, P.H. Ambulatory Position and Orientation Tracking Fusing Magnetic and Inertial Sensing. IEEE Trans. Biomed. Eng. 2007, 54, 883–890. [Google Scholar] [CrossRef]
- Nüesch, C.; Roos, E.; Pagenstert, G.; Mündermann, A. Measuring Joint Kinematics of Treadmill Walking and Running: Comparison between an Inertial Sensor Based System and a Camera-Based System. J. Biomech. 2017, 57, 32–38. [Google Scholar] [CrossRef]
- Andersen, A.M.; Rasmussen, B.S.B.; Graumann, O.; Overgaard, S.; Lundemann, M.; Haubro, M.H.; Varnum, C.; Rasmussen, J.; Jensen, J. Minimal Hip Joint Space Width Measured on X-Rays by an Artificial Intelligence Algorithm—A Study of Reliability and Agreement. BioMedInformatics 2023, 3, 714–723. [Google Scholar] [CrossRef]
- Naylor, J.M.; Ko, V.; Adie, S.; Gaskin, C.; Walker, R.; Harris, I.A.; Mittal, R. Validity and Reliability of Using Photography for Measuring Knee Range of Motion: A Methodological Study. BMC Musculoskelet. Disord. 2011, 12, 77. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Measuring Agreement in Method Comparison Studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef] [PubMed]
- Giavarina, D. Understanding Bland Altman Analysis. Biochem. Med. 2015, 25, 141–151. [Google Scholar] [CrossRef]
- Incavo, S.; Beynnon, B.; Coughlin, K. In Vitro Kinematics of the Replaced Knee. In Total Knee Arthroplasty; Bellemans, J., Ries, M.D., Victor, J.M.K., Eds.; Springer: Berlin/Heidelberg, Germany, 2005; pp. 152–158. [Google Scholar] [CrossRef]
- Parsa, K.; Lasky, T.A.; Ravani, B. Design and Implementation of a Mechatronic, All-Accelerometer Inertial Measurement Unit. IEEE/ASME Trans. Mechatron. 2007, 12, 640–650. [Google Scholar] [CrossRef]
- Cappa, P.; Patanè, F.; Rossi, S. A Redundant Accelerometric Cluster for the Measurement of Translational and Angular Acceleration and Angular Velocity of the Head. J. Med. Devices 2007, 1, 14–22. [Google Scholar] [CrossRef]
- Cappa, P.; Patanè, F.; Rossi, S. Two Calibration Procedures for a Gyroscope-Free Inertial Measurement System Based on a Double-Pendulum Apparatus. Meas. Sci. Technol. 2008, 19, 055204. [Google Scholar] [CrossRef]
- Sabatini, A.M. Quaternion-Based Extended Kalman Filter for Determining Orientation by Inertial and Magnetic Sensing. IEEE Trans. Biomed. Eng. 2006, 53, 1346–1356. [Google Scholar] [CrossRef]
- Sabatini, A.M. Adaptive filtering algorithms enhance the accuracy of low-cost inertial/magnetic sensing in pedestrian navigation systems. Int. J. Comp. Intel. Appl. 2008, 07, 351–361. [Google Scholar] [CrossRef]
- Weygers, I.; Kok, M.; Konings, M.; Hallez, H.; De Vroey, H.; Claeys, K. Inertial Sensor-Based Lower Limb Joint Kinematics: A Methodological Systematic Review. Sensors 2020, 20, 673. [Google Scholar] [CrossRef]
- Niswander, W.; Wang, W.; Kontson, K. Optimization of IMU Sensor Placement for the Measurement of Lower Limb Joint Kinematics. Sensors 2020, 20, 5993. [Google Scholar] [CrossRef] [PubMed]
- Reinschmidt, C.; Van Den Bogert, A.J.; Lundberg, A.; Nigg, B.M.; Murphy, N.; Stacoff, A.; Stano, A. Tibiofemoral and Tibiocalcaneal Motion during Walking: External vs. Skeletal Markers. Gait Posture 1997, 6, 98–109. [Google Scholar] [CrossRef]
- Palermo, E.; Rossi, S.; Marini, F.; Patanè, F.; Cappa, P. Experimental Evaluation of Accuracy and Repeatability of a Novel Body-to-Sensor Calibration Procedure for Inertial Sensor-Based Gait Analysis. Measurement 2014, 52, 145–155. [Google Scholar] [CrossRef]
- Vitali, R.; Cain, S.; McGinnis, R.; Zaferiou, A.; Ojeda, L.; Davidson, S.; Perkins, N. Method for Estimating Three-Dimensional Knee Rotations Using Two Inertial Measurement Units: Validation with a Coordinate Measurement Machine. Sensors 2017, 17, 1970. [Google Scholar] [CrossRef]
- Bailey, C.A.; Uchida, T.K.; Nantel, J.; Graham, R.B. Validity and Sensitivity of an Inertial Measurement Unit-Driven Biomechanical Model of Motor Variability for Gait. Sensors 2021, 21, 7690. [Google Scholar] [CrossRef]
- Robert-Lachaine, X.; Parent, G.; Fuentes, A.; Hagemeister, N.; Aissaoui, R. Inertial Motion Capture Validation of 3D Knee Kinematics at Various Gait Speed on the Treadmill with a Double-Pose Calibration. Gait Posture 2020, 77, 132–137. [Google Scholar] [CrossRef]
- Seel, T.; Raisch, J.; Schauer, T. IMU-Based Joint Angle Measurement for Gait Analysis. Sensors 2014, 14, 6891–6909. [Google Scholar] [CrossRef]
- Weber, J.G.; Ortigas-Vásquez, A.; Sauer, A.; Dupraz, I.; Utz, M.; Maas, A.; Grupp, T.M. Comparison of IMU-Based Knee Kinematics with and without Harness Fixation against an Optical Marker-Based System. Bioengineering 2024, 11, 976. [Google Scholar] [CrossRef] [PubMed]
- Sagasser, S.; Sauer, A.; Thorwächter, C.; Weber, J.G.; Maas, A.; Woiczinski, M.; Grupp, T.M.; Ortigas-Vásquez, A. Validation of Inertial-Measurement-Unit-Based Ex Vivo Knee Kinematics during a Loaded Squat before and after Reference-Frame-Orientation Optimisation. Sensors 2024, 24, 3324. [Google Scholar] [CrossRef] [PubMed]
- Papi, E.; Osei-Kuffour, D.; Chen, Y.-M.A.; McGregor, A.H. Use of Wearable Technology for Performance Assessment: A Validation Study. Med. Eng. Phys. 2015, 37, 698–704. [Google Scholar] [CrossRef]
- Zhu, Y.; Li, H.; Wu, X.; Chen, N. Accuracy Validation of a Sensor-Based Inertial Measurement Unit and Motion Capture System for Assessment of Lower Limb Muscle Strength in Older Adults—A Novel and Convenient Measurement Approach. Sensors 2024, 24, 6040. [Google Scholar] [CrossRef]
- Favre, J.; Aissaoui, R.; Jolles, B.M.; De Guise, J.A.; Aminian, K. Functional Calibration Procedure for 3D Knee Joint Angle Description Using Inertial Sensors. J. Biomech. 2009, 42, 2330–2335. [Google Scholar] [CrossRef]
- Fain, A.; McCarthy, A.; Nindl, B.C.; Fuller, J.T.; Wills, J.A.; Doyle, T.L.A. IMUs Can Estimate Hip and Knee Range of Motion during Walking Tasks but Are Not Sensitive to Changes in Load or Grade. Sensors 2024, 24, 1675. [Google Scholar] [CrossRef] [PubMed]
- Chan, L.Y.T.; Chua, C.S.; Chou, S.M.; Seah, R.Y.B.; Huang, Y.; Luo, Y.; Dacy, L.; Bin Abd Razak, H.R. Assessment of Shoulder Range of Motion Using a Commercially Available Wearable Sensor—A Validation Study. mHealth 2022, 8, 30. [Google Scholar] [CrossRef]
- Buford, W.L.; Ivey, F.M.; Nakamura, T.; Patterson, R.M.; Nguyen, D.K. Internal/External Rotation Moment Arms of Muscles at the Knee: Moment Arms for the Normal Knee and the ACL-Deficient Knee. Knee 2001, 8, 293–303. [Google Scholar] [CrossRef]
- Perry, J.; Burnfield, J.M. Gait Analysis: Normal and Pathological Function, 2nd ed.; SLACK: Thorofare, NJ, USA, 2010. [Google Scholar]
- Neumann, D.A.; Kelly, E.R.; Kiefer, C.L.; Martens, K.; Grosz, C.M. Kinesiology of the Musculoskeletal System: Foundations for Rehabilitation, 3rd ed.; Elsevier: St. Louis, MO, USA, 2017. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Exercise, ° | Xsen Dots IMU Mean, ° (SD 3) | GATOR Mean, ° (SD) | Mean Bias 1, ° (SD) | LoA 2,4 95% CI 5, ° |
|---|---|---|---|---|
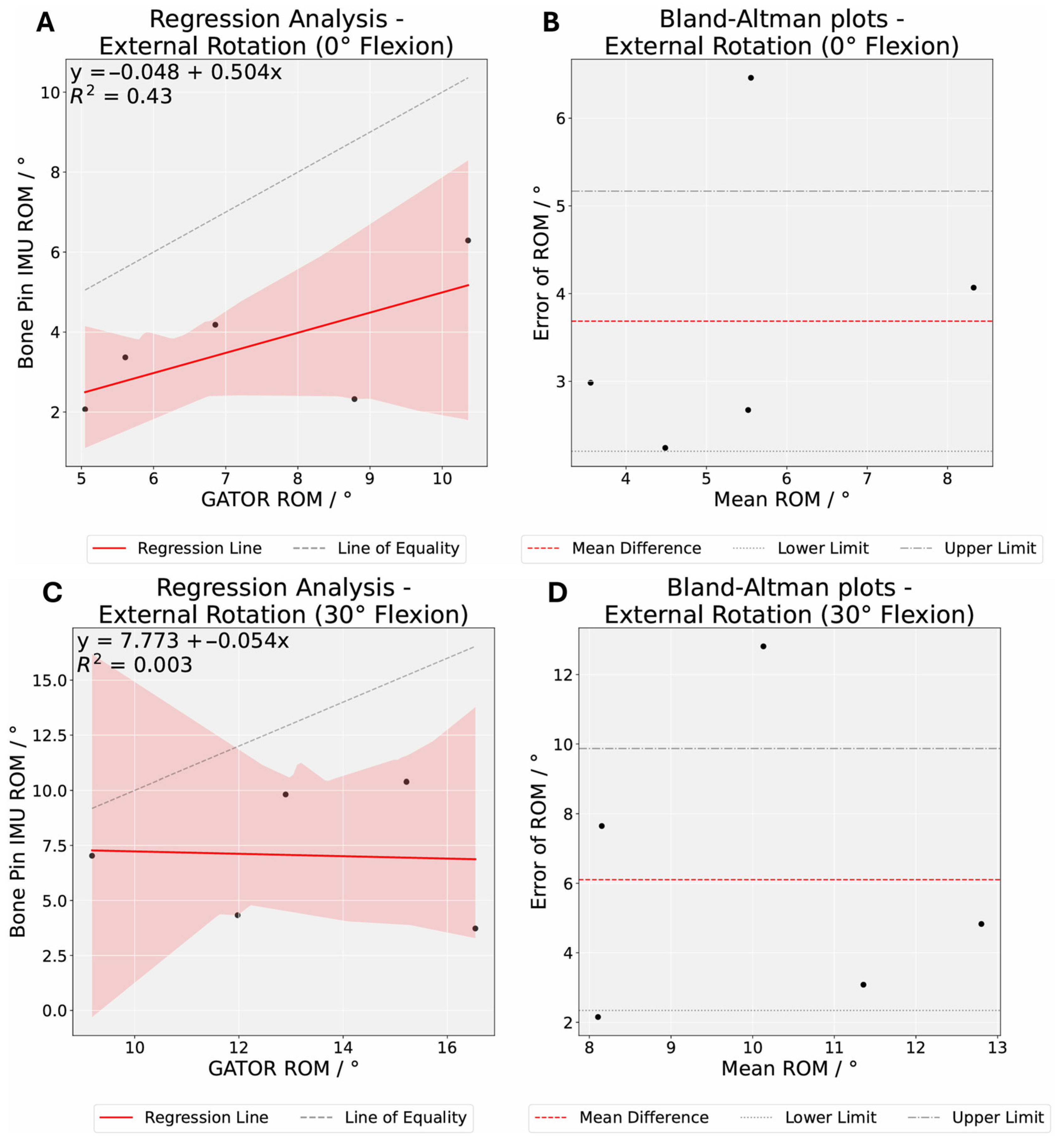
| External Rotation (0) | 7.33 (1.98) | 3.65 (1.52) | 3.69 (1.69) | [2.20, 5.17] |
| External Rotation (30) | 13.16 (2.57) | 7.06 (2.73) | 6.10 (4.29) | [2.34, 9.87] |
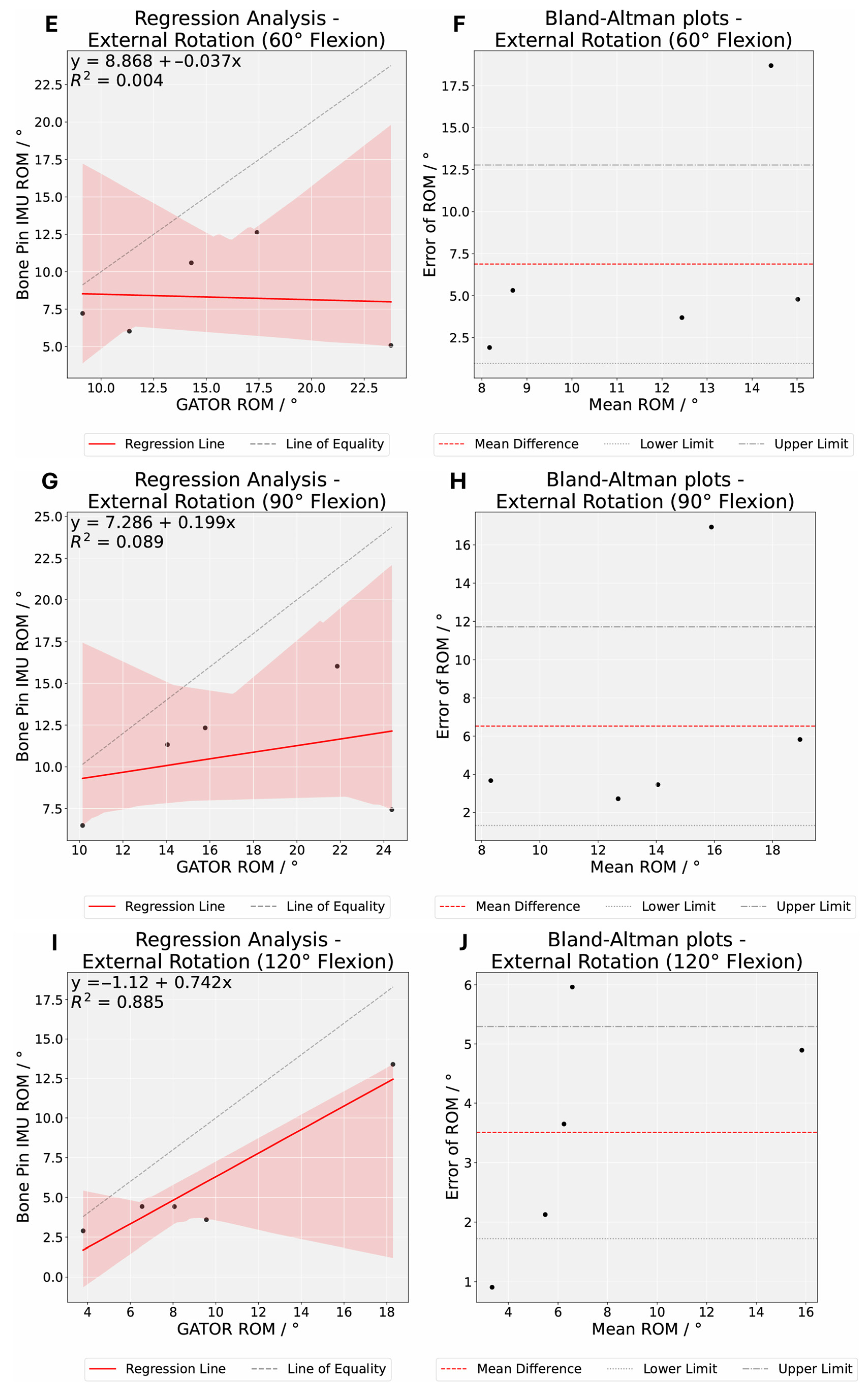
| External Rotation (60) | 15.19 (5.12) | 8.31 (2.85) | 6.88 (6.73) | [0.98, 12.78] |
| External Rotation (90) | 17.24 (5.19) | 10.72 (3.46) | 6.52 (5.94) | [1.31, 11.72] |
| External Rotation (120) | 9.25 (4.90) | 5.74 (3.87) | 3.51 (2.04) | [1.72, 5.30] |
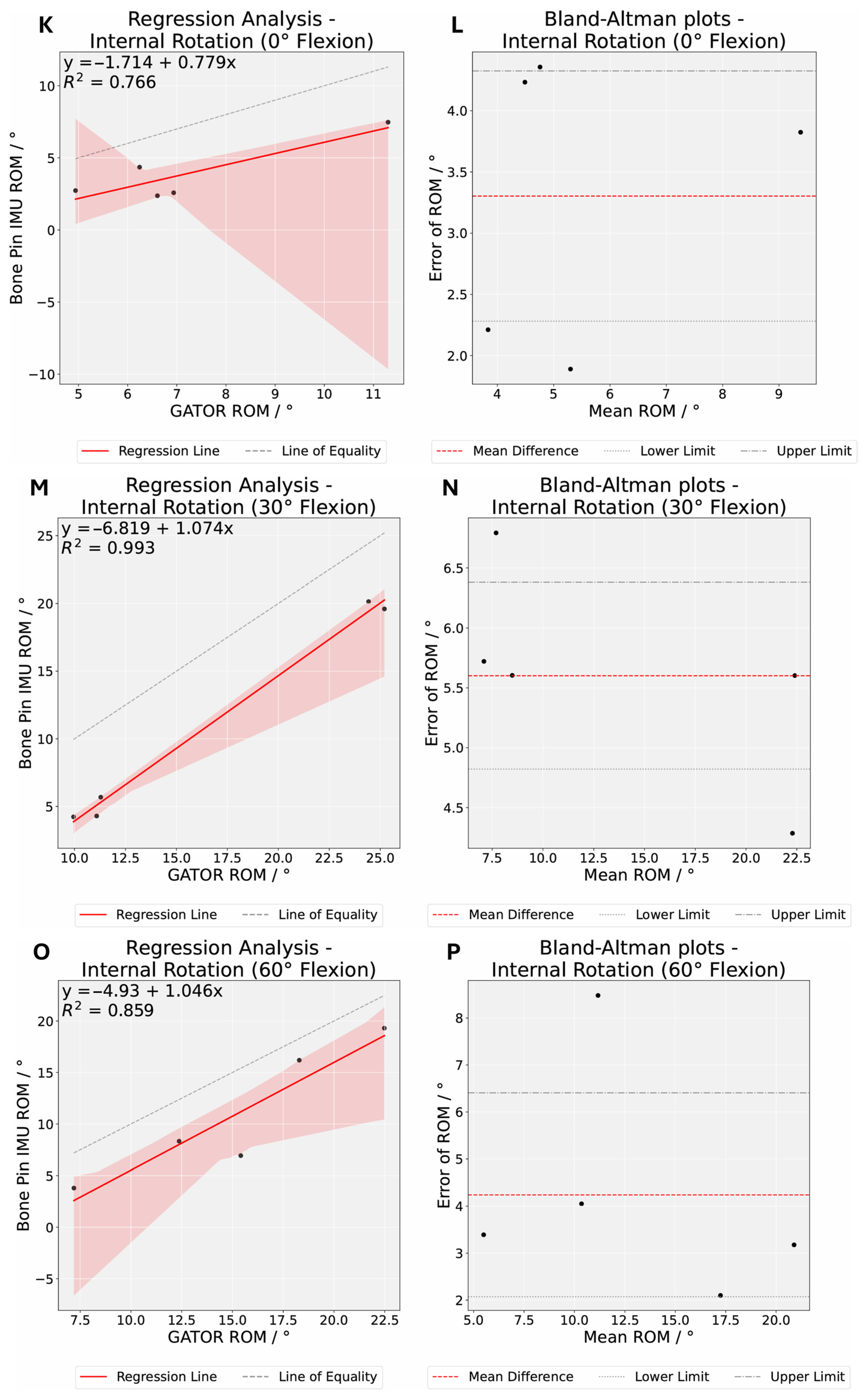
| Internal Rotation (0) | 7.20 (2.16) | 3.90 (1.92) | 3.30 (1.17) | [2.28, 4.33] |
| Internal Rotation (30) | 16.39 (6.90) | 10.79 (7.44) | 5.60 (0.89) | [4.82, 6.38] |
| Internal Rotation (60) | 15.15 (5.19) | 10.91 (5.86) | 4.24 (2.47) | [2.07, 6.41] |
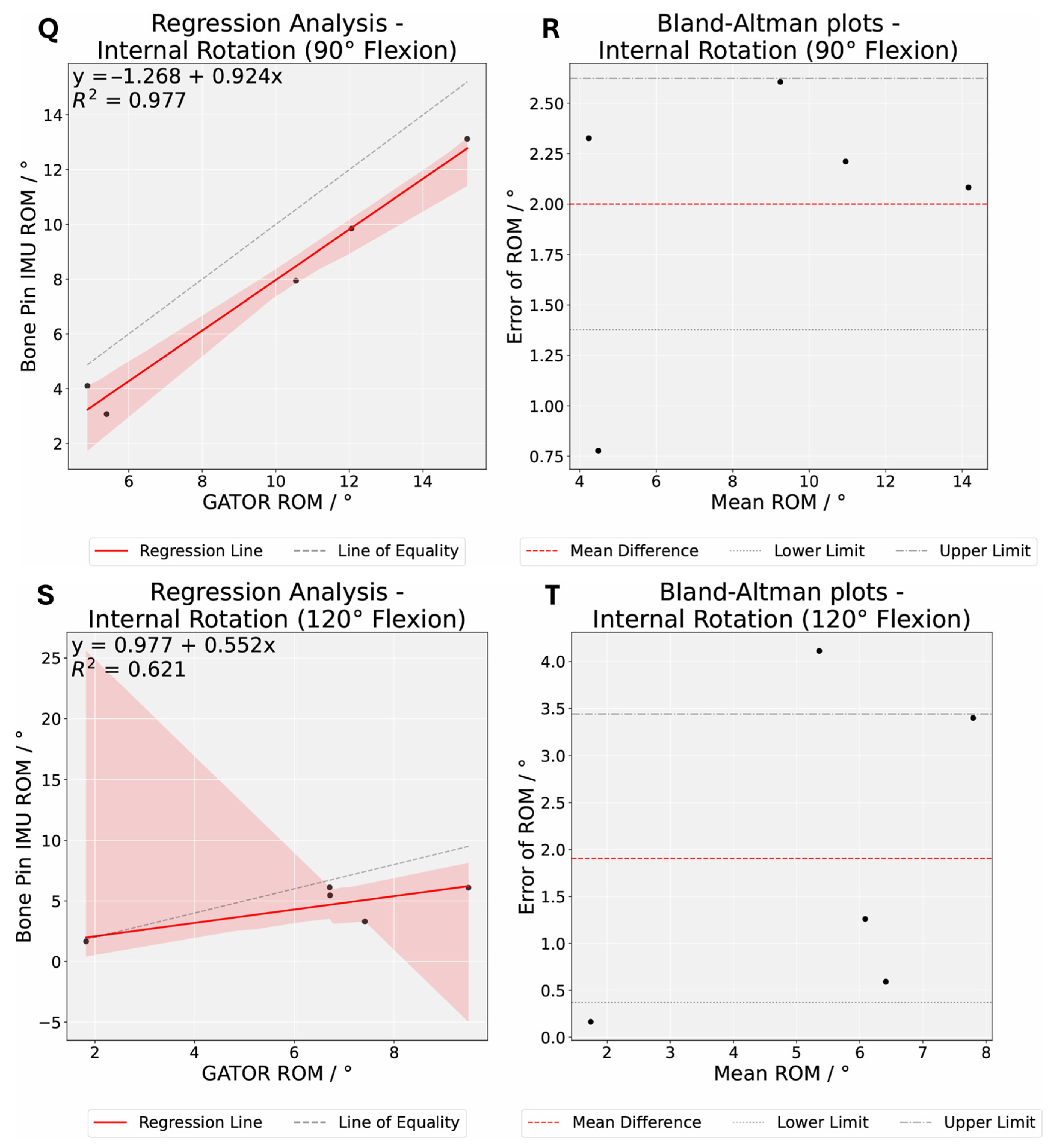
| Internal Rotation (90) | 9.62 (3.96) | 7.62 (3.70) | 2.00 (0.71) | [1.38, 2.62] |
| Internal Rotation (120) | 6.43 (2.52) | 4.53 (1.77) | 1.91 (1.75) | [0.37, 3.44] |
| Exercise, ° | Percentage of Trials Within 5° of Mean Error, % (n 1) | Percentage of Trials Within 10° of Mean Error, % (n 1) | R2 | RMSE 2, ° | P | P Bonferroni | Random Error |
|---|---|---|---|---|---|---|---|
| External Rotation (0) | 80.0 (4) | 100.0 (5) | 0.43 | 3.98 | 0.008 | 0.09 | 1.69 |
| External Rotation (30) | 60.0 (3) | 80.0 (4) | 0.0026 | 7.21 | 0.034 | 0.369 | 4.29 |
| External Rotation (60) | 60.0 (3) | 80.0 (4) | 0.0044 | 9.14 | 0.084 | 0.927 | 6.73 |
| External Rotation (90) | 60.0 (3) | 80.0 (4) | 0.09 | 8.41 | 0.07 | 0.771 | 5.94 |
| External Rotation (120) | 80.0 (4) | 100.0 (5) | 0.88 | 3.95 | 0.018 | 0.202 | 2.04 |
| Internal Rotation (0) | 100.0 (5) | 100.0 (5) | 0.77 | 3.46 | 0.003 | 0.035 | 1.17 |
| Internal Rotation (30) | 20.0 (1) | 100.0 (5) | 0.99 | 5.66 | 0.0 | 0.002 | 0.89 |
| Internal Rotation (60) | 80.0 (4) | 100.0 (5) | 0.86 | 4.78 | 0.019 | 0.204 | 2.47 |
| Internal Rotation (90) | 100.0 (5) | 100.0 (5) | 0.98 | 2.1 | 0.003 | 0.036 | 0.71 |
| Internal Rotation (120) | 100.0 (5) | 100.0 (5) | 0.62 | 2.47 | 0.072 | 0.791 | 1.75 |
| Exercise Type | RMSE |
|---|---|
| External Rotation | 6.90 |
| Internal Rotation | 3.93 |
| External-Internal Rotation | 5.61 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Razak, H.R.B.A.; Chua, N.; Lai, K.W. Quantification of 3D Kinematic Measurements for Knee Flexion and Tibial Rotation Using an IMU-Based Sensor and Ultrasound Imaging System: A Cadaveric Study. Sensors 2025, 25, 4211. https://doi.org/10.3390/s25134211
Razak HRBA, Chua N, Lai KW. Quantification of 3D Kinematic Measurements for Knee Flexion and Tibial Rotation Using an IMU-Based Sensor and Ultrasound Imaging System: A Cadaveric Study. Sensors. 2025; 25(13):4211. https://doi.org/10.3390/s25134211
Chicago/Turabian StyleRazak, Hamid Rahmatullah Bin Abd, Nicolas Chua, and Kah Weng Lai. 2025. "Quantification of 3D Kinematic Measurements for Knee Flexion and Tibial Rotation Using an IMU-Based Sensor and Ultrasound Imaging System: A Cadaveric Study" Sensors 25, no. 13: 4211. https://doi.org/10.3390/s25134211
APA StyleRazak, H. R. B. A., Chua, N., & Lai, K. W. (2025). Quantification of 3D Kinematic Measurements for Knee Flexion and Tibial Rotation Using an IMU-Based Sensor and Ultrasound Imaging System: A Cadaveric Study. Sensors, 25(13), 4211. https://doi.org/10.3390/s25134211