

Mechanistic Assessment of Cardiovascular State Informed by Vibroacoustic Sensors

Abstract
1. Introduction
2. Proposed Method and Algorithm
- For each cardiac cycle with vibroacoustic feature vector , find the and corresponding from the atlas that is closest to .
- Repeat across n cardiac cycles, i.e., for , to obtain sets and
- Learn the function g using these sets. Learning candidates considered are a linear model and a shallow neural network.
3. Case Study
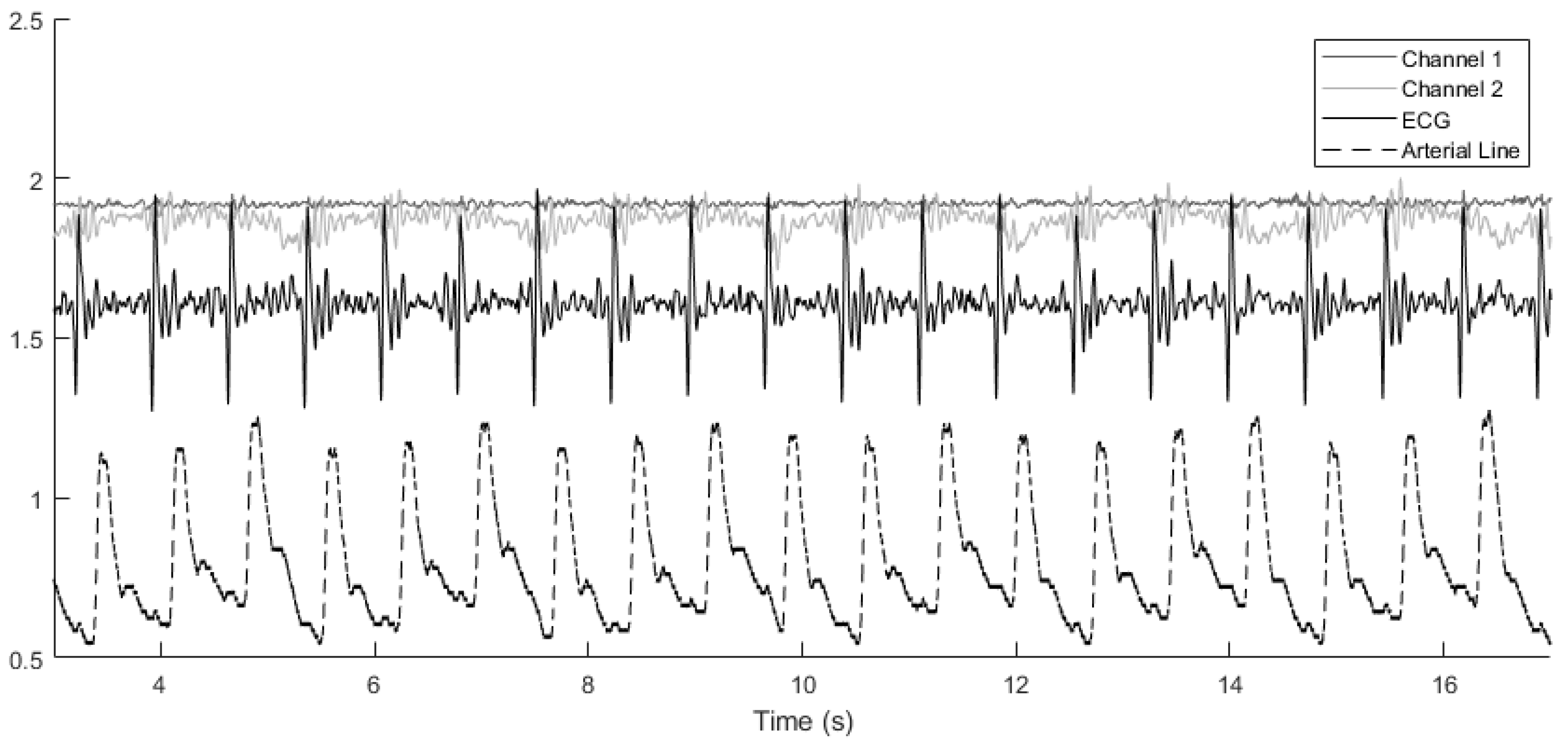
3.1. Vibroacoustic Signals
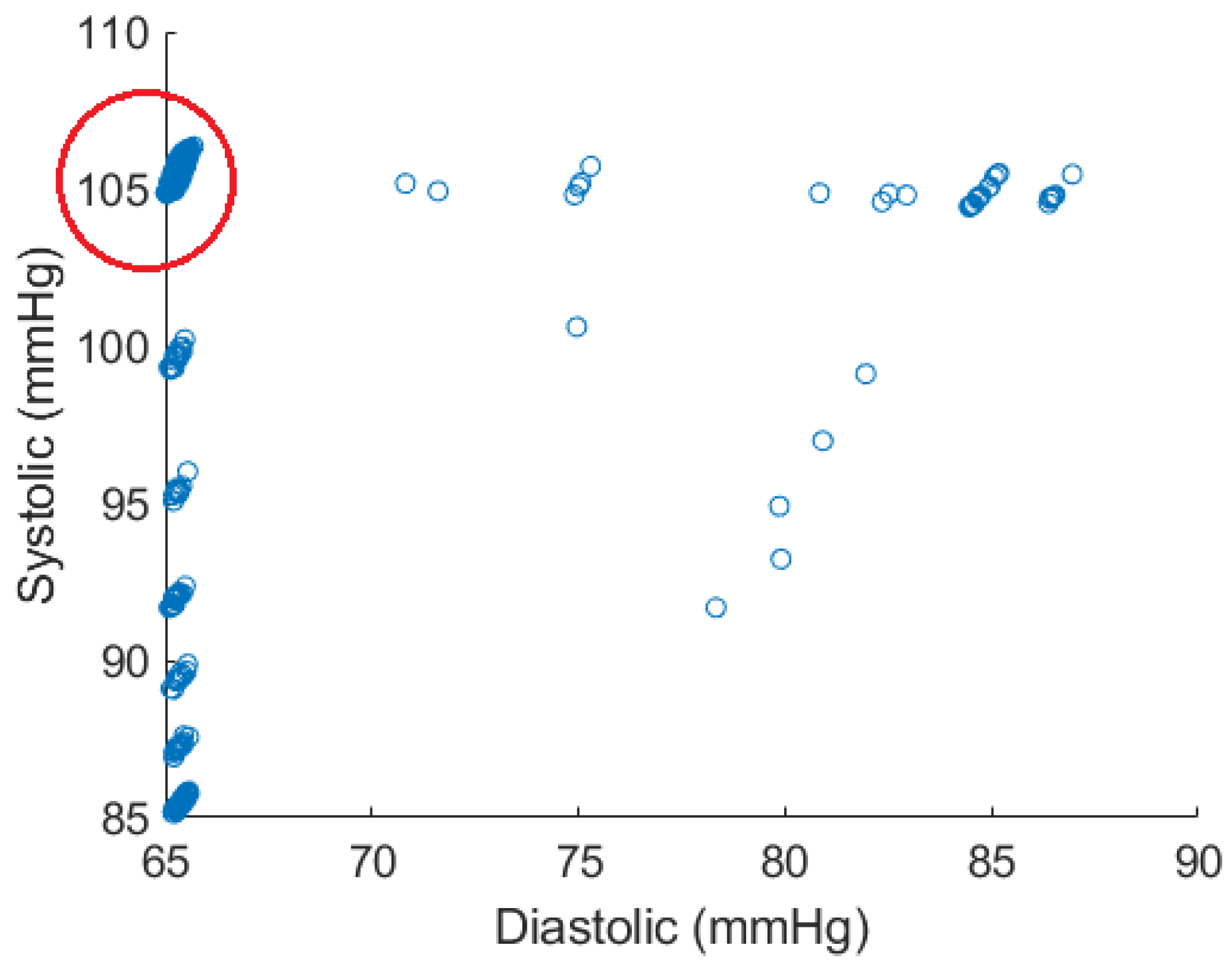
3.2. Arterial Line and ECG Signals
3.3. Choice of Parameters
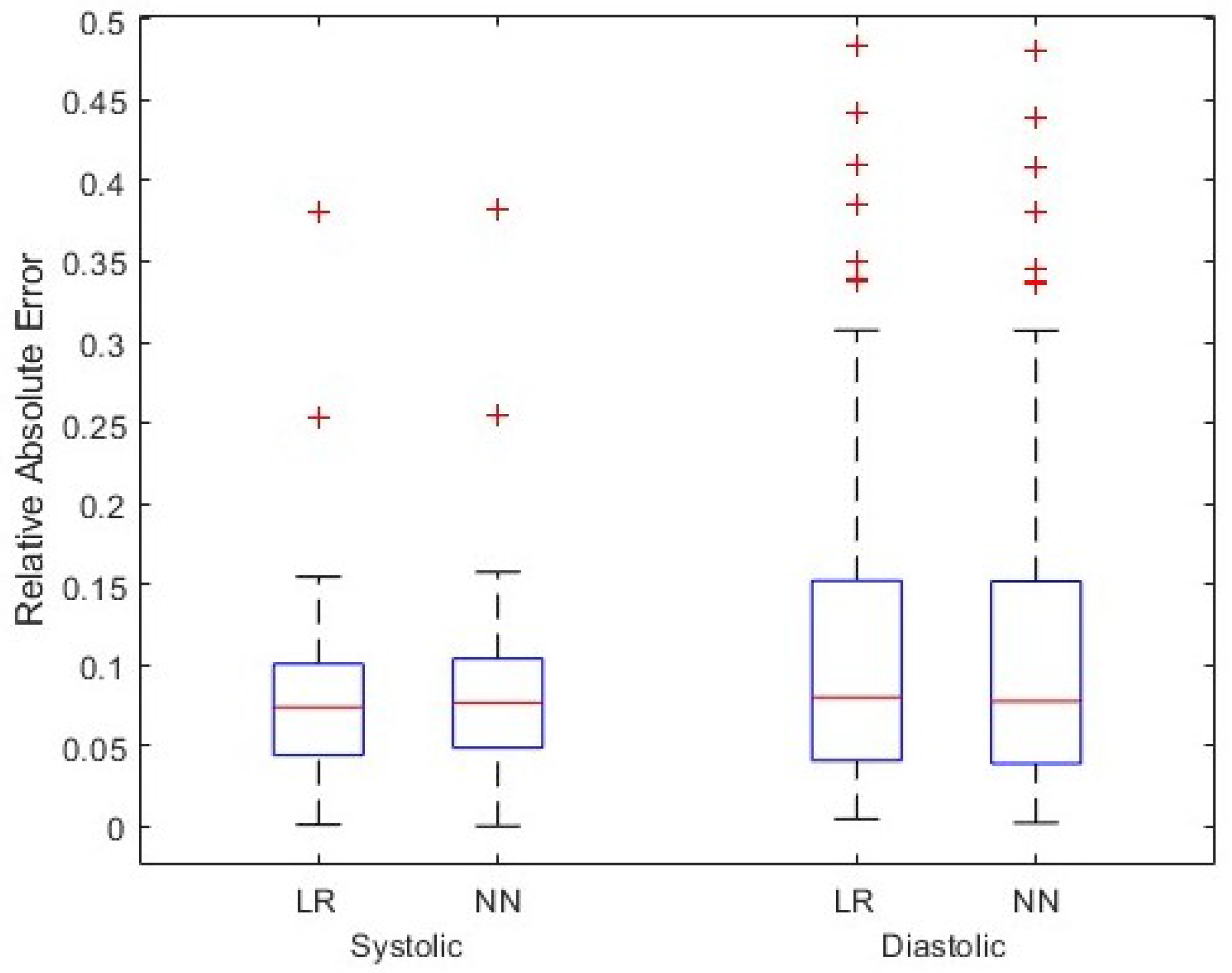
4. Simulation and Results
Results and Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Rosalia, L.; Ozturk, C.; Van Story, D.; Horvath, M.A.; Roche, E.T. Object-Oriented Lumped-Parameter Modeling of the Cardiovascular System for Physiological and Pathophysiological Conditions. Adv. Theory Simulations 2021, 4, 2000216. [Google Scholar] [CrossRef]
- Guo, L.; Davenport, S.; Peng, Y. Deep CardioSound: An Ensembled Deep Learning Model for Heart Sound MultiLabelling. arXiv 2022, arXiv:2204.07420. [Google Scholar]
- Abduh, Z.; Nehary, E.A.; Wahed, M.A.; Kadah, Y.M. Classification of heart sounds using fractional fourier transform based mel-frequency spectral coefficients and traditional classifiers. Biomed. Signal Process. Control 2020, 57, 101788. [Google Scholar] [CrossRef]
- Chen, L.; Wu, S.F.; Xu, Y.; Lyman, W.D.; Kapur, G. Calculating blood pressure based on measured heart sounds. J. Comput. Acoust. 2017, 25, 1750014. [Google Scholar] [CrossRef]
- Chobanian, A.; Bakris, G.; Black, H.; Cushman, W.; Green, L.; Izzo, J., Jr.; Jones, D.; Materson, B.; Oparil, S.; Wright, J., Jr.; et al. Seventh report of the joint national committee on prevention, detection, evaluation, and treatment of high blood pressure. Hypertension 2003, 42, 1206–1252. [Google Scholar] [CrossRef] [PubMed]
- De Canete, J.F.; del Saz-Orozco, P.; Moreno-Boza, D.; Duran-Venegas, E. Object-oriented modeling and simulation of the closed loop cardiovascular system by using SIMSCAPE. Comput. Biol. Med. 2013, 43, 323–333. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Tompkins, W.J. A Real-Time QRS Detection Algorithm. IEEE Trans. Biomed. Eng. 1985, BME-32, 230–236. [Google Scholar] [CrossRef]
- Sedghamiz, H. Matlab Implementation of Pan Tompkins ECG QRS Detector. Code Available at the File Exchange Site of MathWorks. 2014. Available online: https://www.researchgate.net/publication/313673153_Matlab_Implementation_of_Pan_Tompkins_ECG_QRS_detector (accessed on 14 March 2024).
- Donoho, D.L.; Johnstone, I.M. Adapting to unknown smoothness via wavelet shrinkage. J. Am. Stat. Assoc. 1995, 90, 1200–1224. [Google Scholar] [CrossRef]
- American Heart Association, Inc. Understanding Blood Pressure Readings. 2023. Available online: www.heart.org (accessed on 6 February 2024).
- Kallioinen, N.; Hill, A.; Horswill, M.; Ward, H.; Watson, M. Sources of inaccuracy in the measurement of adult patients’ resting blood pressure in clinical settings: A systematic review. J. Hypertens. 2017, 35, 421. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Range | Unit |
|---|---|---|
| – | cm | |
| 6–8 | cm | |
| – | cm | |
| 4–6 | cm | |
| 4–6 | cm | |
| – | cm | |
| – | cm | |
| 4–6 | cm | |
| – | N/A | |
| – | ||
| – | N/A | |
| – | ||
| – | N/A | |
| – | ||
| – | N/A | |
| – |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zare, A.; Wittrup, E.; Najarian, K. Mechanistic Assessment of Cardiovascular State Informed by Vibroacoustic Sensors. Sensors 2024, 24, 2189. https://doi.org/10.3390/s24072189
Zare A, Wittrup E, Najarian K. Mechanistic Assessment of Cardiovascular State Informed by Vibroacoustic Sensors. Sensors. 2024; 24(7):2189. https://doi.org/10.3390/s24072189
Chicago/Turabian StyleZare, Ali, Emily Wittrup, and Kayvan Najarian. 2024. "Mechanistic Assessment of Cardiovascular State Informed by Vibroacoustic Sensors" Sensors 24, no. 7: 2189. https://doi.org/10.3390/s24072189
APA StyleZare, A., Wittrup, E., & Najarian, K. (2024). Mechanistic Assessment of Cardiovascular State Informed by Vibroacoustic Sensors. Sensors, 24(7), 2189. https://doi.org/10.3390/s24072189