
Instrumented Pre-Hospital Care Simulation Mannequin for Use in Spinal Motion Restrictions Scenarios: Validation of Cervical and Lumbar Motion Assessment



Abstract
1. Introduction
2. Materials and Methods
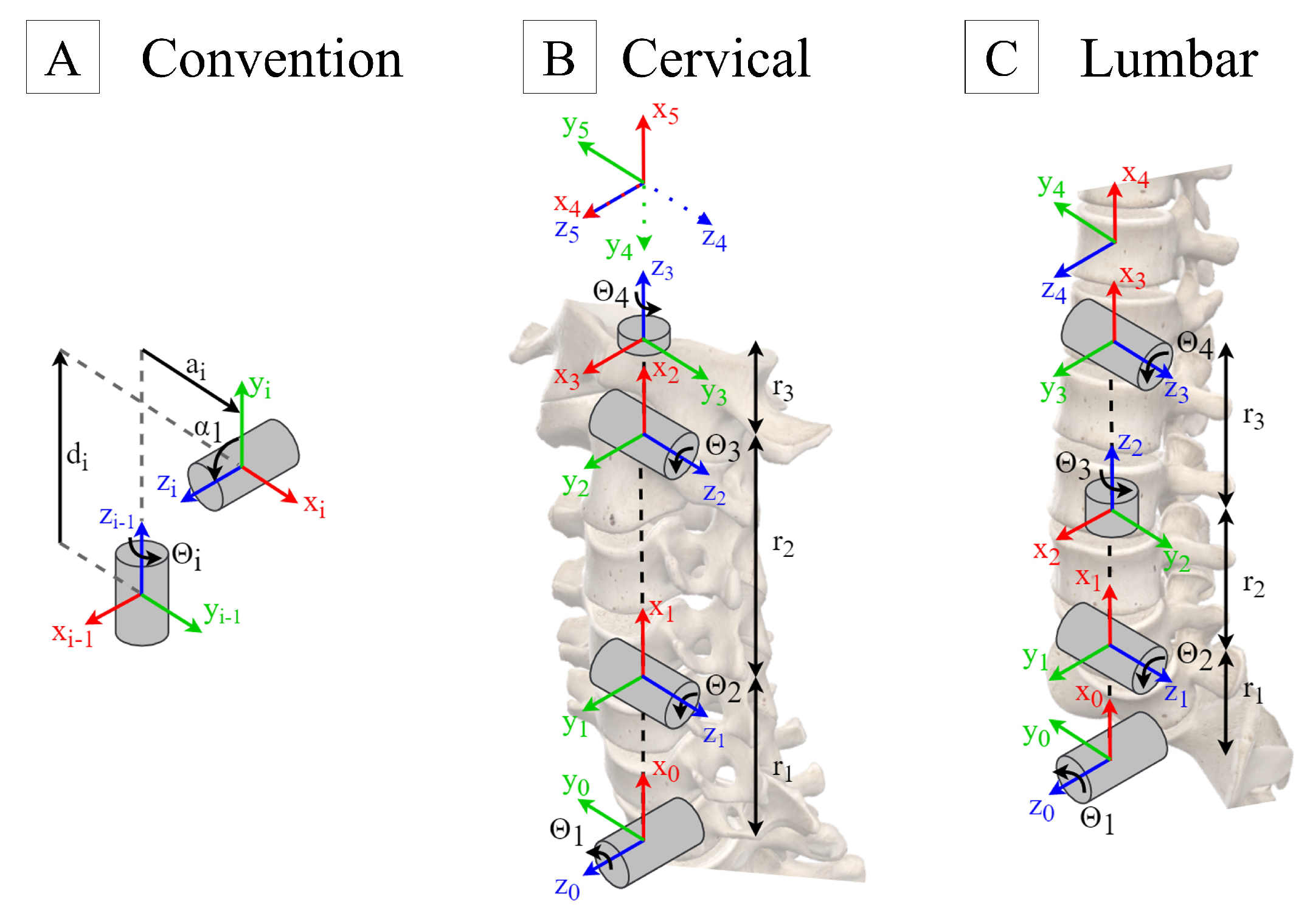
2.1. Anatomical Model Definition
2.1.1. Cervical and Lumbar Assembly Model
- The axis must be located along the axis of the joint i.
- The axis must be normal to the and axis. If and are parallel, the direction of is chosen arbitrarily.
- The must be defined with respect to the right-hand rule.
- The joint length, , defined as the distance between the and axis, along the axis.
- The joint twist, , defined as the angle between the and axis, along the axis.
- The joint offset, , defined as the distance between the and axis, along the axis.
- The joint angle, , defined as the angle between the and axis, along the axis.
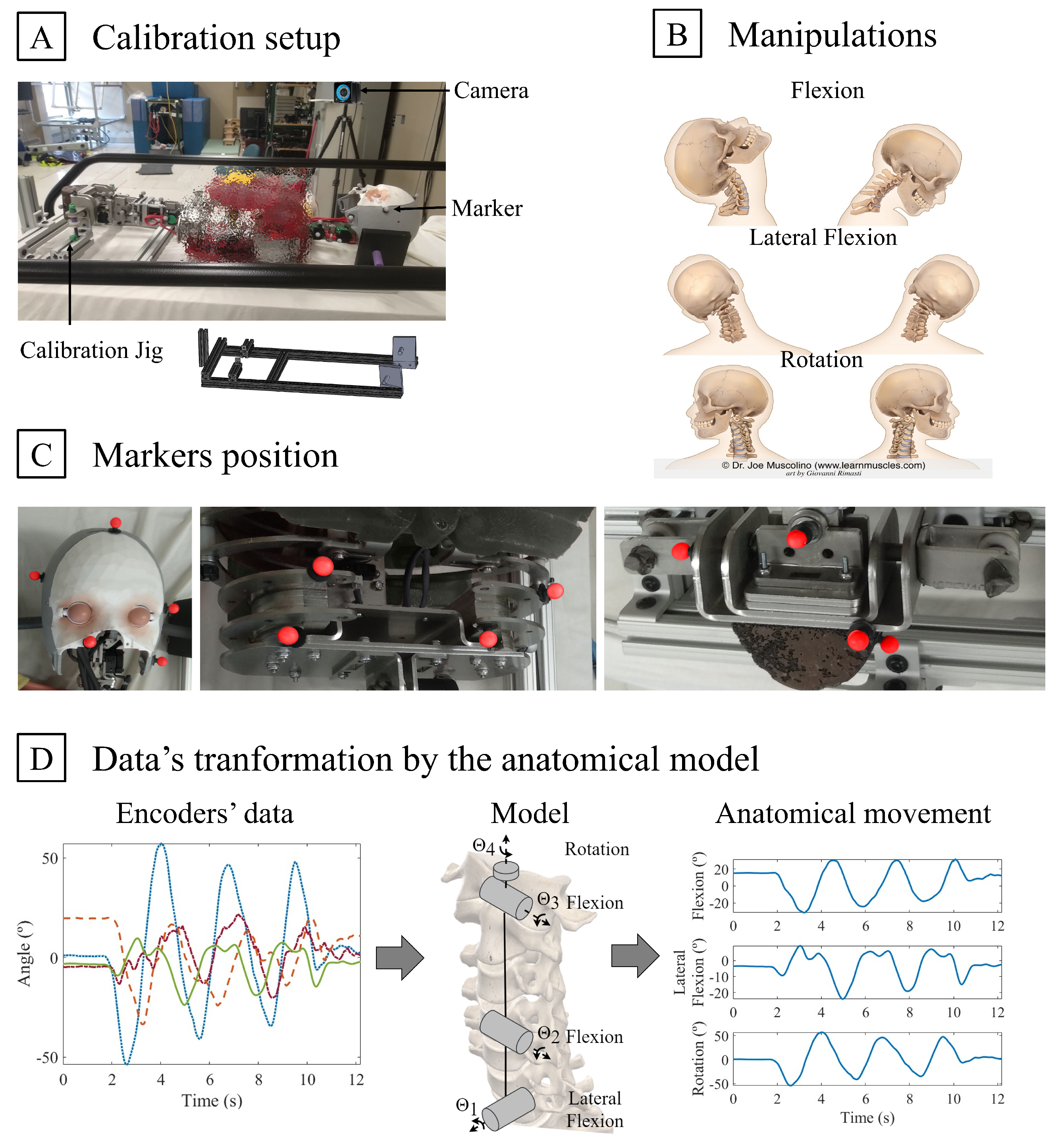
2.1.2. Neutral Calibration
2.2. Data Collection
2.3. Data Reduction and Analysis
2.3.1. Data Pre-Processing
2.3.2. Performance Markers
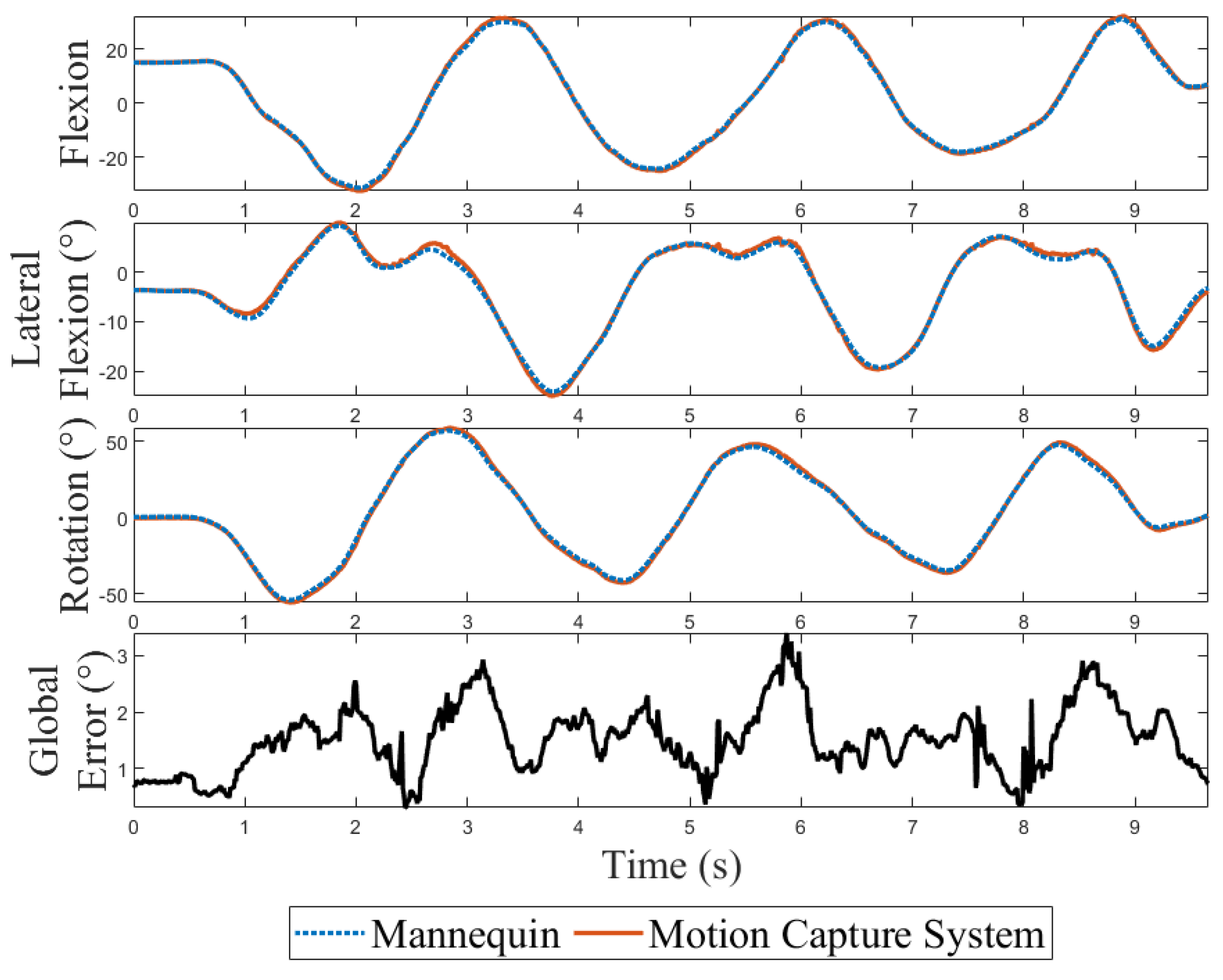
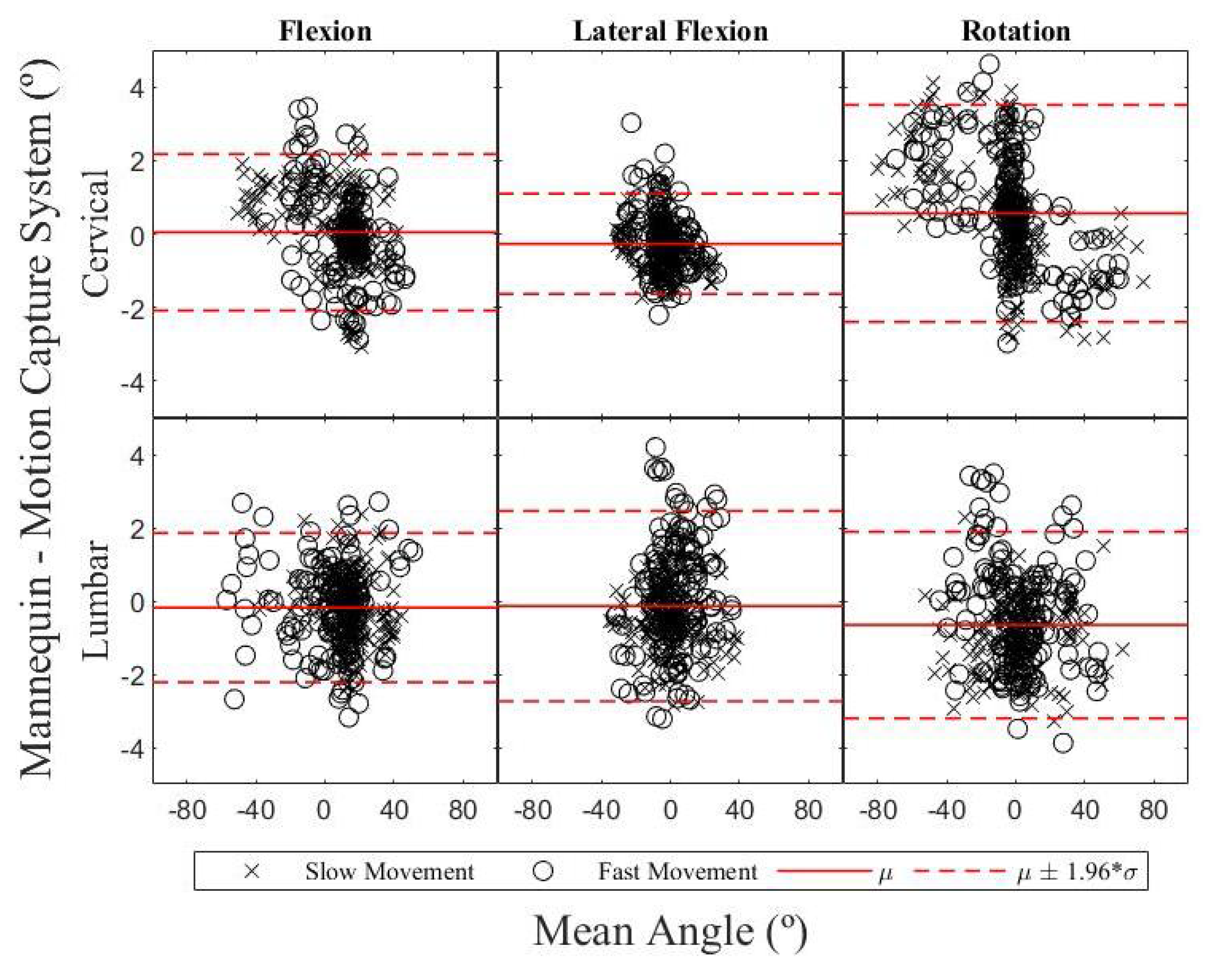
3. Results
3.1. Mannequin’s Accuracy
3.2. Influence of Motion Speed on Accuracy
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| SMR | Spinal motion restriction |
| SCI | Spinal cord injury |
| IMU | Inertial measurement unit |
| CPR | Cardiopulmonaty resuscitation |
| RMSE | Root-mean-square error |
| MDC | Minimal detectable change |
References
- Singh, A.; Tetreault, L.; Kalsi-Ryan, S.; Nouri, A.; Fehlings, M.G. Global prevalence and incidence of traumatic spinal cord injury. Clin. Epidemiol. 2014, 6, 309–331. [Google Scholar] [CrossRef] [PubMed]
- Furlan, J.C.; Noonan, V.; Singh, A.; Fehlings, M.G. Assessment of Impairment in Patients with Acute Traumatic Spinal Cord Injury: A Systematic Review of the Literature. J. Neurotrauma 2011, 28, 1445–1477. [Google Scholar] [CrossRef] [PubMed]
- Zileli, M.; Osorio-Fonseca, E.; Konovalov, N.; Cardenas-Jalabe, C.; Kaprovoy, S.; Mlyavykh, S.; Pogosyan, A. Early Management of Cervical Spine Trauma: WFNS Spine Committee Recommendations. Neurospine 2020, 17, 710–722. [Google Scholar] [CrossRef] [PubMed]
- Shrier, I.; Boissy, P.; Brière, S.; Mellette, J.; Fecteau, L.; Matheson, G.O.; Garza, D.; Meeuwisse, W.H.; Segal, E.; Boulay, J.; et al. Can a rescuer or simulated patient accurately assess motion during cervical spine stabilization practice sessions? J. Athl. Train. 2012, 47, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Conrad, B.P.; Marchese, D.L.; Rechtine, G.R.; Horodyski, M.B. Motion in the unstable thoracolumbar spine when spine boarding a prone patient. J. Spinal Cord Med. 2012, 35, 53–57. [Google Scholar] [CrossRef]
- Conrad, B.P.; Marchese, D.L.; Rechtine, G.R.; Prasarn, M.; Rossi, G.D.; Horodyski, M.B.H. Motion in the unstable cervical spine when transferring a patient positioned prone to a spine board. J. Athl. Train. 2013, 48, 797–803. [Google Scholar] [CrossRef] [PubMed]
- Grenier, G.; Despatis, M.A.; Lebel, K.; Hamel, M.; Martin, C.; Boissy, P. Removal of the cervical collar from alpine rescue protocols? A biomechanical non-inferiority trial in real-life mountain conditions. Scand. J. Trauma Resusc. Emerg. Med. 2022, 30, 42. [Google Scholar] [CrossRef] [PubMed]
- Weerts, J.O.; Schier, L.; Schmidt, H.; Kreinest, M. Review of existing measurement tools to assess spinal motion during prehospital immobilization. Eur. J. Emerg. Med. 2018, 25, 161–168. [Google Scholar] [CrossRef] [PubMed]
- van der Kruk, E.; Reijne, M.M. Accuracy of human motion capture systems for sport applications; state-of-the-art review. Eur. J. Sport Sci. 2018, 18, 806–819. [Google Scholar] [CrossRef] [PubMed]
- Lebel, K.; Boissy, P.; Nguyen, H.; Duval, C. Inertial measurement systems for segments and joints kinematics assessment: Towards an understanding of the variations in sensors accuracy. Biomed. Eng. Online 2017, 16, 56. [Google Scholar] [CrossRef] [PubMed]
- FrankSim. Frank’s Life. Available online: https://www.youtube.com/playlist?list=PL2TgiN6ISYrpt8c89GKYbs-RX0I5uSdq9. (accessed on 14 August 2022).
- Winter, D.A. Biomechanics and Motor Control of Human Movement; John Wiley & Sons: Hoboken, NJ, USA, 2009. [Google Scholar]
- Gordon, C.C.; Churchill, T.; Clauser, C.E.; Bradtmiller, B.; McConville, J.T. Anthropometric Survey of US Army Personnel: Methods and Summary Statistics 1988. Technical Report. 1989. Available online: https://apps.dtic.mil/sti/citations/ADA209600. (accessed on 18 January 2023).
- Vasavada, A.N.; Danaraj, J.; Siegmund, G.P. Head and neck anthropometry, vertebral geometry and neck strength in height-matched men and women. J. Biomech. 2008, 41, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Plaga, J.A.; Albery, C.; Boehmer, M.; Goodyear, C.; Thomas, G. Design and Development of Anthropometrically Correct Head Forms for Joint Strike Fighter Ejection Seat Testing. Technical Report. 2005. Available online: https://apps.dtic.mil/sti/citations/ADA449446. (accessed on 18 January 2023).
- Yoganandan, N.; Pintar, F.A.; Zhang, J.; Baisden, J.L. Physical properties of the human head: Mass, center of gravity and moment of inertia. J. Biomech. 2009, 42, 1177–1192. [Google Scholar] [CrossRef] [PubMed]
- Robinette, K.M.; Blackwell, S.; Daanen, H.; Boehmer, M.; Fleming, S. Civilian American and European Surface Anthropometry Resource (Caesar), Final Report. Volume 1. Summary. Technical Report. 2002. Available online: https://apps.dtic.mil/sti/citations/ADA406704. (accessed on 18 January 2023).
- Sforza, C.; Grassi, G.; Fragnito, N.; Turci, M.; Ferrario, V.F. Three-dimensional analysis of active head and cervical spine range of motion: Effect of age in healthy male subjects. Clin. Biomech. 2002, 17, 611–614. [Google Scholar] [CrossRef] [PubMed]
- AMS. AS5048A High-Resolution Position Sensor. 2021. Available online: https://ams.com/as5048a#tab/documents (accessed on 4 August 2021).
- Menditto, A.; Patriarca, M.; Magnusson, B. Understanding the meaning of accuracy, trueness and precision. Accredit. Qual. Assur. 2007, 12, 45–47. [Google Scholar] [CrossRef]
- McGinley, J.L.; Baker, R.; Wolfe, R.; Morris, M.E. The reliability of three-dimensional kinematic gait measurements: A systematic review. Gait Posture 2009, 29, 360–369. [Google Scholar] [CrossRef] [PubMed]
- Hilger, N.; Beauducel, A. Parallel-Forms Reliability. In Encyclopedia of Personality and Individual Differences; Zeigler-Hill, V., Shackelford, T.K., Eds.; Springer International Publishing: Berlin/Heidelberg, Germany, 2017; pp. 1–3. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Cervical | Lumbar | |||||||
|---|---|---|---|---|---|---|---|---|
| Joint | ||||||||
| 1 | 0 | 0 | ||||||
| 2 | 0 | 0 | 0 | 0 | ||||
| 3 | 0 | 0 | 0 | |||||
| 4 | 0 | 0 | 0 | |||||
| 5 | 0 | 0 | ||||||
| RMSE Values | Accuracy Interpretation |
|---|---|
| RMSE ≤ 2 | Good |
| 2 < RMSE ≤ 5 | Acceptable |
| 5 < RMSE ≤ 10 | Tolerable |
| RMSE > 10 | Unbearable |
| Cervical | Lumbar | |||
|---|---|---|---|---|
| RMSE (°) | SD (°) | RMSE (°) | SD (°) | |
| Global | 1.9 | 0.5 | 2.3 | 0.5 |
| Flexion | 1.1 | 0.3 | 1.1 | 0.2 |
| Lateral Flexion | 0.7 | 0.2 | 1.3 | 0.5 |
| Rotation | 1.5 | 0.5 | 1.5 | 0.4 |
| Cervical | Lumbar | |||
|---|---|---|---|---|
| Bias (°) | CI95 (°) | Bias (°) | CI95 (°) | |
| Flexion | 0.0 | −2.2–2.2 | −0.2 | −2.3–1.9 |
| Lateral Flexion | −0.3 | −1.7–1.2 | −0.1 | −2.8–2.6 |
| Rotation | 0.6 | −2.4–3.5 | −0.7 | −3.3–2.0 |
| Cervical | Lumbar | |||||||
|---|---|---|---|---|---|---|---|---|
| r | SD (°) | SEm (°) | MDC (°) | r | SD (°) | SEm (°) | MDC (°) | |
| Global | 0.999 | 19.7 | 0.7 | 2.1 | 0.997 | 17.5 | 0.9 | 2.5 |
| Flexion | 0.998 | 17.3 | 0.7 | 1.9 | 0.998 | 17.6 | 0.7 | 2.0 |
| Lateral Flexion | 0.998 | 10.0 | 0.5 | 1.3 | 0.996 | 14.1 | 0.9 | 2.6 |
| Rotation | 0.999 | 25.2 | 0.8 | 2.4 | 0.997 | 19.0 | 0.9 | 2.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Martin, C.; Boissy, P.; Hamel, M.; Lebel, K. Instrumented Pre-Hospital Care Simulation Mannequin for Use in Spinal Motion Restrictions Scenarios: Validation of Cervical and Lumbar Motion Assessment. Sensors 2024, 24, 1055. https://doi.org/10.3390/s24041055
Martin C, Boissy P, Hamel M, Lebel K. Instrumented Pre-Hospital Care Simulation Mannequin for Use in Spinal Motion Restrictions Scenarios: Validation of Cervical and Lumbar Motion Assessment. Sensors. 2024; 24(4):1055. https://doi.org/10.3390/s24041055
Chicago/Turabian StyleMartin, Camille, Patrick Boissy, Mathieu Hamel, and Karina Lebel. 2024. "Instrumented Pre-Hospital Care Simulation Mannequin for Use in Spinal Motion Restrictions Scenarios: Validation of Cervical and Lumbar Motion Assessment" Sensors 24, no. 4: 1055. https://doi.org/10.3390/s24041055
APA StyleMartin, C., Boissy, P., Hamel, M., & Lebel, K. (2024). Instrumented Pre-Hospital Care Simulation Mannequin for Use in Spinal Motion Restrictions Scenarios: Validation of Cervical and Lumbar Motion Assessment. Sensors, 24(4), 1055. https://doi.org/10.3390/s24041055