





Validity and Reliability of Gait Speed and Knee Flexion Estimated by a Novel Vision-Based Smartphone Application

Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Equipment
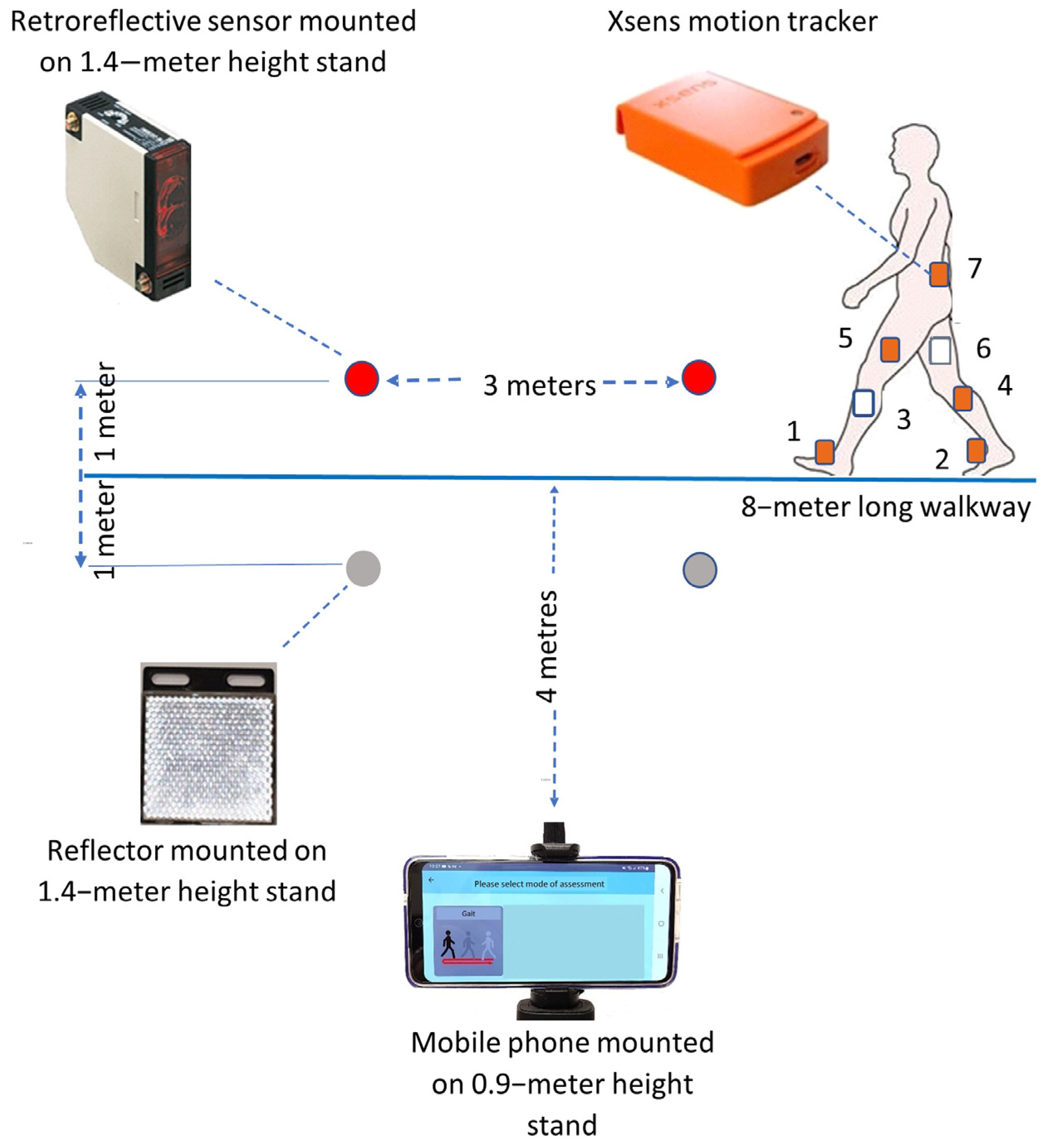
2.3. Equipment Setup
2.4. Experimental Procedures
2.5. Statistical Analysis
3. Results
3.1. Participants
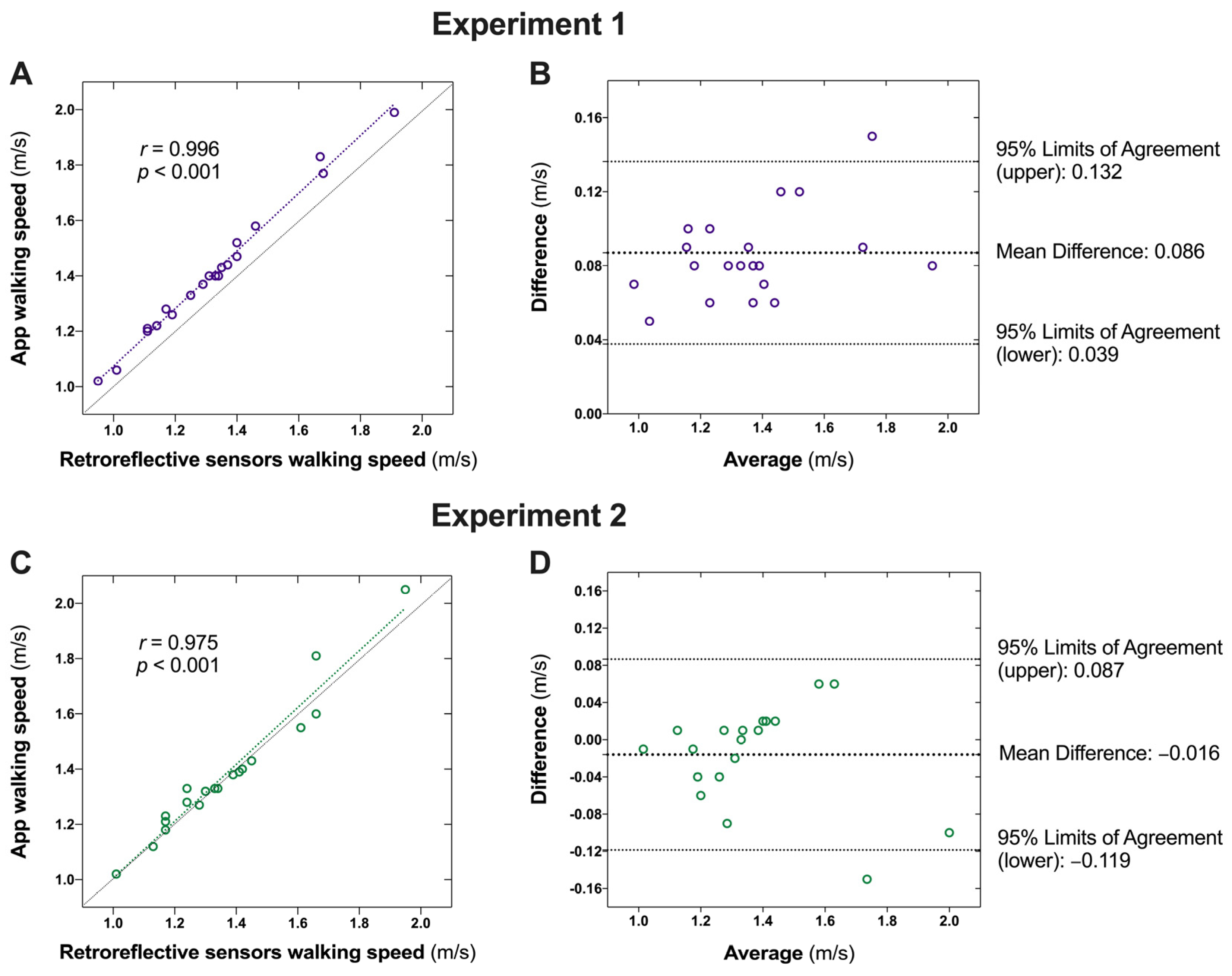
3.2. Validity of Walking Speed
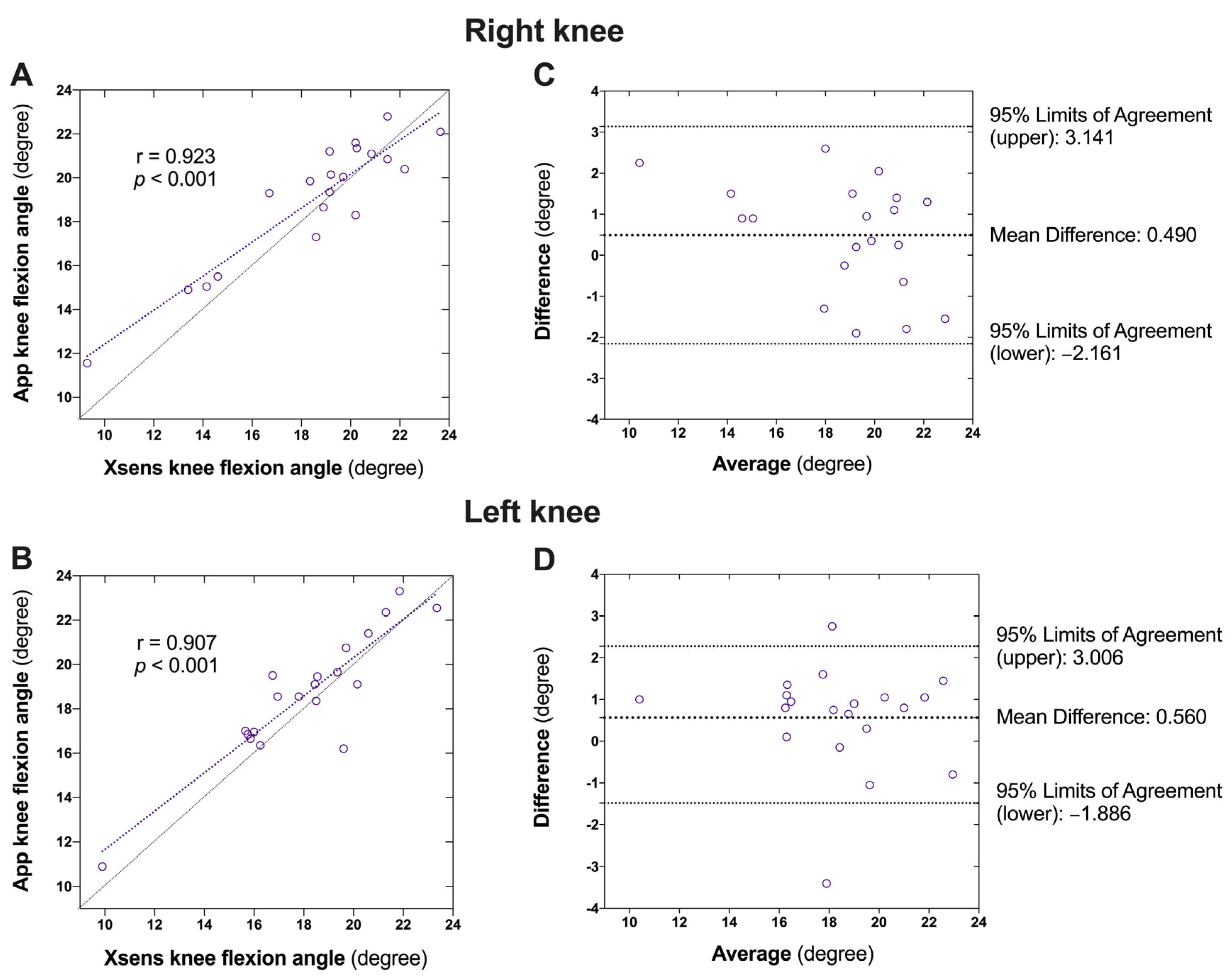
3.3. Validity of the Knee Flexion Angle
3.4. Reliability of the App for Walking Speed and Knee Flexion Angle
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Partridge, L.; Deelen, J.; Slagboom, P.E. Facing up to the global challenges of ageing. Nature 2018, 561, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Sharma, L. Osteoarthritis of the knee. N. Engl. J. Med. 2021, 384, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Bergen, G.; Stevens, M.R.; Burns, E.R. Falls andFall Injuries Among Adults Aged ≥65 Years—United States, 2014. Morb. Mortal. Wkly. Rep. 2016, 65, 993–998. [Google Scholar] [CrossRef] [PubMed]
- Dieppe, P.A.; Lohmander, L.S. Pathogenesis and management of pain in osteoarthritis. Lancet 2005, 365, 965–973. [Google Scholar] [CrossRef]
- Bennell, K.L.; Hunt, M.A.; Wrigley, T.V.; Lim, B.-W.; Hinman, R.S. Role of Muscle in the Genesis and Management of Knee Osteoarthritis. Rheum. Dis. Clin. N. Am. 2008, 34, 731–754. [Google Scholar] [CrossRef]
- Steultjens, M.; Dekker, J.; Van Baar, M.; Oostendorp, R.; Bijlsma, J. Range of joint motion and disability in patients with osteoarthritis of the knee or hip. Rheumatology 2000, 39, 955–961. [Google Scholar] [CrossRef]
- Rosadi, R.; Jankaew, A.; Wu, P.-T.; Kuo, L.-C.; Lin, C.-F. Factors associated with falls in patients with knee osteoarthritis: A cross-sectional study. Medicine 2022, 101, e32146. [Google Scholar] [CrossRef]
- Hartholt, K.A.; van Beeck, E.F.; Polinder, S.; van der Velde, N.; van Lieshout, E.M.; Panneman, M.J.; van der Cammen, T.J.; Patka, P. Societal consequences of falls in the older population: Injuries, healthcare costs, and long-term reduced quality of life. J. Trauma 2011, 71, 748–753. [Google Scholar] [CrossRef]
- Ganz, D.A.; Latham, N.K. Prevention of falls in community-dwelling older adults. N. Engl. J. Med. 2020, 382, 734–743. [Google Scholar] [CrossRef]
- Adam, C.E.; Fitzpatrick, A.L.; Leary, C.S.; Hajat, A.; Ilango, S.D.; Park, C.; Phelan, E.A.; Semmens, E.O. Change in gait speed and fall risk among community-dwelling older adults with and without mild cognitive impairment: A retrospective cohort analysis. BMC Geriatr. 2023, 23, 328. [Google Scholar] [CrossRef]
- Dixon, S.J.; Hinman, R.S.; Creaby, M.W.; Kemp, G.; Crossley, K.M. Knee joint stiffness during walking in knee osteoarthritis. Arthritis Care Res. 2010, 62, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Heiden, T.L.; Lloyd, D.G.; Ackland, T.R. Knee joint kinematics, kinetics and muscle cocontraction in knee osteoarthritis patient gait. Clin. Biomech. 2009, 24, 833–841. [Google Scholar] [CrossRef] [PubMed]
- McCarthy, I.; Hodgins, D.; Mor, A.; Elbaz, A.; Segal, G. Analysis of knee flexion characteristics and how they alter with the onset of knee osteoarthritis: A case control study. BMC Musculoskelet. Disord. 2013, 14, 169. [Google Scholar] [CrossRef] [PubMed]
- Childs, J.D.; Sparto, P.J.; Fitzgerald, G.K.; Bizzini, M.; Irrgang, J.J. Alterations in lower extremity movement and muscle activation patterns in individuals with knee osteoarthritis. Clin. Biomech. 2004, 19, 44–49. [Google Scholar] [CrossRef]
- Li, Z.; Leung, K.L.; Huang, C.; Huang, X.; Su, S.; Chung, R.C.; Ding, C.; Fu, S.N. Associations amongst dynamic knee stiffness during gait, quadriceps stiffness, and the incidence of knee osteoarthritis over 24 months: A cohort study with a mediation analysis. BMC Musculoskelet. Disord. 2024, 25, 511. [Google Scholar] [CrossRef]
- Li, Z.; Leung, K.L.; Huang, C.; Huang, X.; Su, S.; Chung, R.C.; Fu, S.N. Higher knee flexion moment during walking is associated with a lower risk of knee pain developing among the elderly after 24 months. Eur. J. Phys. Rehabil. Med. 2023, 59, 386–395. [Google Scholar] [CrossRef]
- Espy, D.D.; Yang, F.; Bhatt, T.; Pai, Y.C. Independent influence of gait speed and step length on stability and fall risk. Gait Posture 2010, 32, 378–382. [Google Scholar] [CrossRef]
- Whittle, M.W. Gait Analysis: An Introduction; Butterworth-Heinemann: Oxford, UK, 2007. [Google Scholar]
- Yoo, J.-H.; Nixon, M.S. Automated Markerless Analysis of Human Gait Motion for Recognition and Classification. ETRI J. 2011, 33, 259–266. [Google Scholar] [CrossRef]
- Verlekar, T.T.; Soares, L.D.; Correia, P.L. Automatic Classification of Gait Impairments Using a Markerless 2D Video-Based System. Sensors 2018, 18, 2743. [Google Scholar] [CrossRef]
- Corazza, S.; Mellone, S.; Micera, S.; Citi, L. Markerless human motion estimation for rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2010, 18, 265–275. [Google Scholar]
- Roetenberg, D.; Luinge, H.; Slycke, P. Xsens MVN: Full 6DOF human motion tracking using miniature inertial sensors. Xsens Motion Technol. BV Tech. Rep. 2009, 1, 1–7. [Google Scholar]
- Woodman, O.J. An Introduction to Inertial Navigation; University of Reading: Reading, UK, 2007. [Google Scholar]
- Iso, T.; Yamazaki, K. Gait analyzer based on a cell phone with a single three-axis accelerometer. In Proceedings of the 8th International Conference on Human-Computer Interaction with Mobile Devices and Services (MobileHCI ′06), Helsinki, Finland, 12–15 September 2006; p. 141. [Google Scholar]
- Nishiguchi, S.; Yamada, M.; Nagai, K.; Mori, S.; Kajiwara, Y.; Sonoda, T.; Yoshimura, K.; Yoshitomi, H.; Ito, H.; Okamoto, K. Reliability and validity of gait analysis by android-based smartphone. Telemed. J. E-Health 2012, 18, 292–296. [Google Scholar] [CrossRef] [PubMed]
- Bittel, A.J.; Elazzazi, A.; Bittel, D.C. Accuracy and precision of an accelerometer-based smartphone app designed to monitor and record angular movement over time. Telemed. J. E-Health 2016, 22, 302–309. [Google Scholar] [CrossRef] [PubMed]
- Capela, N.A.; Lemaire, E.D.; Baddour, N. Novel algorithm for a smartphone-based 6-minute walk test application: Algorithm, application development, and evaluation. J. Neuroeng. Rehabil. 2015, 12, 19. [Google Scholar] [CrossRef]
- Soltani, A.; Aminian, K.; Mazza, C.; Cereatti, A.; Palmerini, L.; Bonci, T.; Paraschiv-lonescu, A. Algorithms for walking speed estimation using a lower-back-worn inertial sensor: A cross-validation on speed ranges. IEEE Trans. Neural Syst. Rehabil. Eng. 2021, 29, 1955–1964. [Google Scholar] [CrossRef]
- World Health Organization. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Wiles, J.L.; Leibing, A.; Guberman, N.; Reeve, J.; Allen, R.E. The meaning of “aging in place” to older people. Gerontologist 2012, 52, 357–366. [Google Scholar] [CrossRef]
- Rantz, M.J.; Skubic, M.; Miller, S.J.; Galambos, C.; Alexander, G.; Keller, J.; Popescu, M. Sensor technology to support aging in place. J. Am. Med. Dir. Assoc. 2013, 14, 386–391. [Google Scholar] [CrossRef]
- Kim, K.I.; Gollamudi, S.S.; Steinhubl, S. Digital technology to enable aging in place. Exp. Gerontol. 2017, 88, 25–31. [Google Scholar] [CrossRef]
- ENISA. Threat Landscape for 5G Networks; European Union Agency for Cybersecurity: Heraklion, Greece, 2019. [Google Scholar]
- Ota, M.; Tateuchi, H.; Hashiguchi, T.; Ichihashi, N. Verification of validity of gait analysis systems during treadmill walking and running using human pose tracking algorithm. Gait Posture 2021, 85, 290–297. [Google Scholar] [CrossRef]
- Richards, J.; Levine, D.; Whittle, M.W. Whittle’s Gait Analysis; Elsevier Limited: Edinburgh, Scotland, UK, 2023. [Google Scholar]
- Zhang, J.-T.; Novak, A.C.; Brouwer, B.; Li, Q. Concurrent validation of Xsens MVN measurement of lower limb joint angular kinematics. Physiol. Meas. 2013, 34, N63. [Google Scholar] [CrossRef]
- Debertin, D.; Wargel, A.; Mohr, M. Reliability of Xsens IMU-Based Lower Extremity Joint Angles during In-Field Running. Sensors 2024, 24, 871. [Google Scholar] [CrossRef] [PubMed]
- Guo, L.; Xiong, S. Accuracy of Base of Support Using an Inertial Sensor Based Motion Capture System. Sensors 2017, 17, 2045. [Google Scholar] [CrossRef] [PubMed]
- Mukaka, M.M. A guide to appropriate use of correlation coefficient in medical research. Malawi Med. J. 2012, 24, 69–71. [Google Scholar] [PubMed]
- Koo, T.K.; Li, M.Y. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice; Pearson/Prentice Hall: Upper Saddle River, NJ, USA, 2009. [Google Scholar]
- Chiari, L.; Della Croce, U.; Leardini, A.; Cappozzo, A. Human movement analysis using stereophotogrammetry. Part 1: Theory. Gait Posture 2005, 21, 186–196. [Google Scholar] [CrossRef]
- Moon, G.; Chang, J.Y.; Lee, K.M. Camera Distance-Aware Top-Down Approach for 3D Multi-Person Pose Estimation from a Single RGB Image. In Proceedings of the 2019 IEEE/CVF International Conference on Computer Vision (ICCV), Seoul, Republic of Korea, 27 October–2 November 2019. [Google Scholar]
- Clavijo-Buendía, S.; Molina-Rueda, F.; Martín-Casas, P.; Ortega-Bastidas, P.; Monge-Pereira, E.; Laguarta-Val, S.; Morales-Cabezas, M.; Cano-De-La-Cuerda, R. Construct validity and test-retest reliability of a free mobile application for spatio-temporal gait analysis in Parkinson’s disease patients. Gait Posture 2020, 79, 86–91. [Google Scholar] [CrossRef]
- Silsupadol, P.; Teja, K.; Lugade, V. Reliability and validity of a smartphone-based assessment of gait parameters across walking speed and smartphone locations: Body, bag, belt, hand, and pocket. Gait Posture 2017, 58, 516–522. [Google Scholar] [CrossRef]
- Hahn, S.; Kröger, I.; Willwacher, S.; Augat, P. Reliability and validity varies among smartphone apps for range of motion measurements of the lower extremity: A systematic review. Gait Posture 2021, 66, 537–555. [Google Scholar] [CrossRef]
- Keogh, J.W.; Cox, A.; Anderson, S.; Liew, B.; Olsen, A.; Schram, B.; Furness, J. Reliability and validity of clinically accessible smartphone applications to measure joint range of motion: A systematic review. PLoS ONE 2019, 14, e0215806. [Google Scholar] [CrossRef]
- Cunha, A.B.; Babik, I.; Harbourne, R.; Cochran, N.J.; Stankus, J.; Szucs, K.; Lobo, M.A. Assessing the validity and reliability of a new video goniometer app for measuring joint angles in adults and children. Arch. Phys. Med. Rehabil. 2020, 101, 275–282. [Google Scholar] [CrossRef]
- Astephen, J.L.; Deluzio, K.J.; Caldwell, G.E.; Dunbar, M.J. Biomechanical changes at the hip, knee, and ankle joints during gait are associated with knee osteoarthritis severity. J. Orthop. Res. 2008, 26, 332–341. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, L.C.; Rudolph, K.S. Influences on knee movement strategies during walking in persons with medial knee osteoarthritis. Arthritis Care Res. 2007, 57, 1018–1026. [Google Scholar] [CrossRef]
- Woo, J. Walking speed: A summary indicator of frailty? J. Am. Med. Dir. Assoc. 2015, 16, 635–637. [Google Scholar] [CrossRef] [PubMed]
- Beck Jepsen, D.; Robinson, K.; Ogliari, G.; Montero-Odasso, M.; Kamkar, N.; Ryg, J.; Freiberger, E.; Masud, T. Predicting falls in older adults: An umbrella review of instruments assessing gait, balance, and functional mobility. BMC Geriatr. 2022, 22, 615. [Google Scholar]
- Shinkai, S.; Watanabe, S.; Kumagai, S.; Fujiwara, Y.; Amano, H.; Yoshida, H.; Ishizaki, T.; Yukawa, H.; Suzuki, T.; Shibata, H. Walking speed as a good predictor for the onset of functional dependence in a Japanese rural community population. Age Ageing 2000, 29, 441–446. [Google Scholar] [CrossRef] [PubMed]
- Veronese, N.; Stubbs, B.; Volpato, S.; Zuliani, G.; Maggi, S.; Cesari, M.; Lipnicki, D.M.; Smith, L.; Schofield, P.; Firth, J. Association between gait speed with mortality, cardiovascular disease and cancer: A systematic review and meta-analysis of prospective cohort studies. J. Am. Med. Dir. Assoc. 2018, 19, 981–988. [Google Scholar] [CrossRef]
- White, D.K.; Niu, J.; Zhang, Y. Is symptomatic knee osteoarthritis a risk factor for a trajectory of fast decline in gait speed? Results from a longitudinal cohort study. Arthritis Care Res. 2013, 65, 187–194. [Google Scholar] [CrossRef]
- Chen, X.; Jafari, R.; Kehtarnavaz, N. Deep learning approaches for markerless motion capture: A review. Sensors 2021, 21, 2744. [Google Scholar]
- Flynn, P.J. Privacy concerns with video surveillance systems. IEEE Secur. Priv. 2003, 1, 32–39. [Google Scholar]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n = 20 | |
|---|---|
| Age (years) | 35.5 ± 12.8 |
| Sex (n, % of females) | 11, 55% |
| Body height (m) | 1.7 ± 0.1 |
| Body mass (kg) | 60.5 ± 14.5 |
| BMI (kg/m2) | 21.9 ± 3.3 |
| Measurements | Correlation | Agreement | ||||||
|---|---|---|---|---|---|---|---|---|
| Retroreflective Sensors (m/s) | APP (m/s) | r | p | Difference (%) | Difference (m/s) | 95% Limits of Agreement (m/s) | p † | |
| Experiment 1 | 1.32 ± 0.23 | 1.41 ± 0.24 | 0.996 | <0.001 | 6.5 | 0.086 ± 0.024 | (0.039, 0.132) | <0.001 |
| Experiment 2 | 1.38 ± 0.23 | 1.36 ± 0.22 | 0.975 | <0.001 | −0.7 | −0.016 ± 0.052 | (−0.119, 0.087) | 0.281 |
| Measurements | Correlation | Agreement | ||||||
|---|---|---|---|---|---|---|---|---|
| Xsens (Degree) | APP (Degree) | r | p | Difference (%) | Difference (Degree) | 95% Limits of Agreement (Degree) | p † | |
| Right knee | 18.8 ± 2.8 | 19.1 ± 2.7 | 0.923 | <0.001 | 2.6 | 0.490 ± 1.353 | (−2.161, 3.141) | 0.122 |
| Left knee | 18.9 ± 3.9 | 19.8 ± 3.8 | 0.907 | <0.001 | 3.2 | 0.560 ± 1.248 | (−1.886, 3.006) | 0.059 |
| Mean ± SD (Degree) | SEM (Degree) | MDD95 (Degree) | ICC (2, 1) (95% CI) | |||
|---|---|---|---|---|---|---|
| Walking speed | Test 1 | 1.35 ± 0.22 | 0.05 | 0.20 | 0.94 | |
| Test 2 | 1.38 ± 0.23 | 0.05 | 0.20 | (0.84, 0.97) | ||
| Knee flexion | Right knee | Test 1 | 18.1 ± 3.5 | 0.91 | 3.57 | 0.86 |
| Test 2 | 19.3 ± 3.0 | 0.77 | 3.02 | (0.63, 0.95) | ||
| Left knee | Test 1 | 17.7 ± 3.1 | 0.80 | 3.14 | 0.88 | |
| Test 2 | 18.9 ± 2.7 | 0.71 | 2.78 | (0.69, 0.95) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leung, K.L.; Li, Z.; Huang, C.; Huang, X.; Fu, S.N. Validity and Reliability of Gait Speed and Knee Flexion Estimated by a Novel Vision-Based Smartphone Application. Sensors 2024, 24, 7625. https://doi.org/10.3390/s24237625
Leung KL, Li Z, Huang C, Huang X, Fu SN. Validity and Reliability of Gait Speed and Knee Flexion Estimated by a Novel Vision-Based Smartphone Application. Sensors. 2024; 24(23):7625. https://doi.org/10.3390/s24237625
Chicago/Turabian StyleLeung, Kam Lun, Zongpan Li, Chen Huang, Xiuping Huang, and Siu Ngor Fu. 2024. "Validity and Reliability of Gait Speed and Knee Flexion Estimated by a Novel Vision-Based Smartphone Application" Sensors 24, no. 23: 7625. https://doi.org/10.3390/s24237625
APA StyleLeung, K. L., Li, Z., Huang, C., Huang, X., & Fu, S. N. (2024). Validity and Reliability of Gait Speed and Knee Flexion Estimated by a Novel Vision-Based Smartphone Application. Sensors, 24(23), 7625. https://doi.org/10.3390/s24237625