
Differences in Trapezius Muscle H-Reflex between Asymptomatic Subjects and Symptomatic Shoulder Pain Subjects
 , , , ,
, , , ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Instrumentation
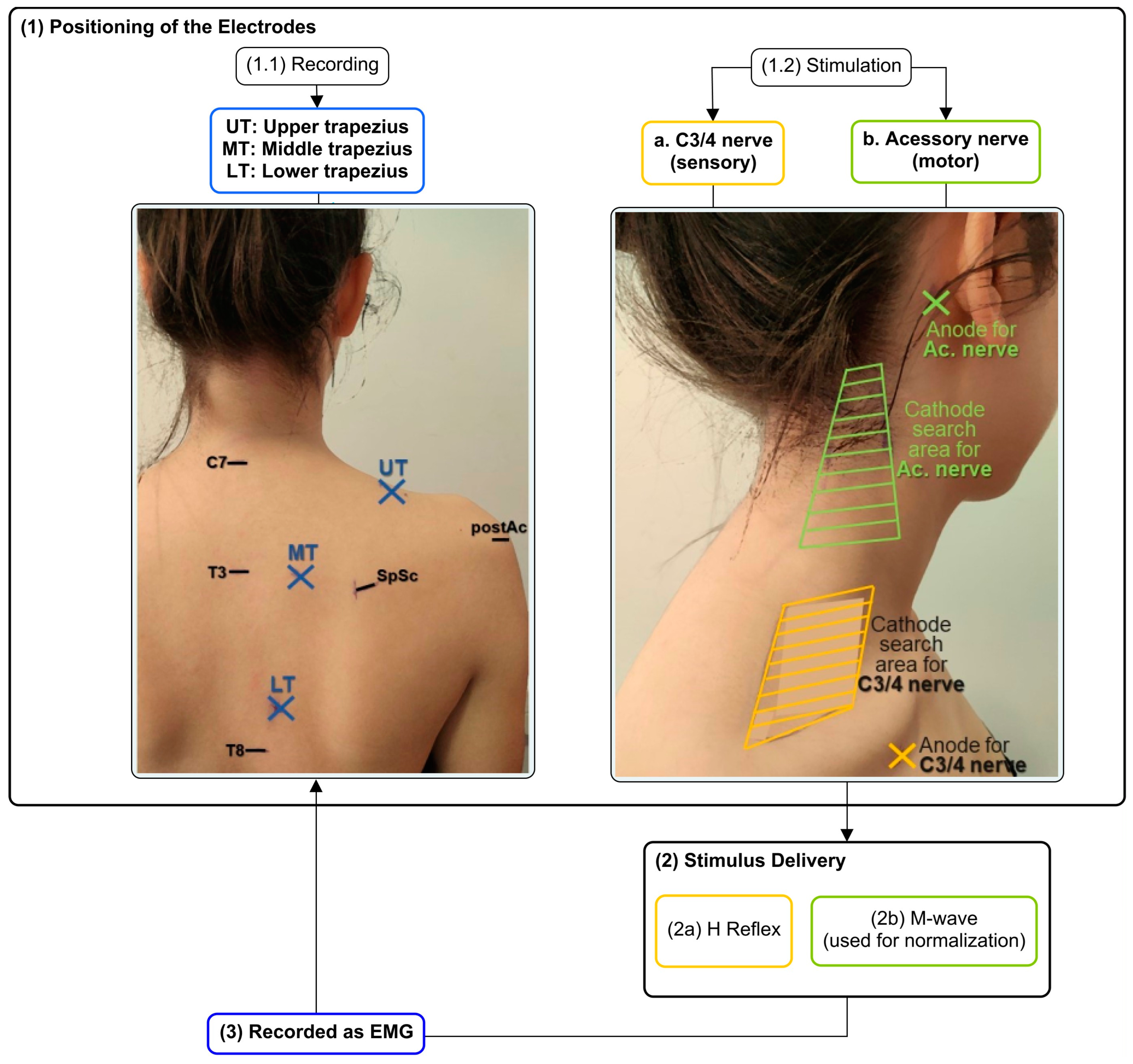
2.3. Positioning of Electrodes for H Reflex and M-Wave Recordings through Electromyography
2.4. Electrical Stimulation of C3/4 and Accessory Nerves
2.5. Maximal Voluntary Isometric Contractions (MVICs)
2.6. Data Processing
2.7. Statistical Analysis
3. Results
Comparison of Trapezius H Reflex and M-Wave between Symptomatic and Asymptomatic Subjects
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Badawy, R.A.; Loetscher, T.; Macdonell, R.A.; Brodtmann, A. Cortical excitability and neurology: Insights into the pathophysiology. Funct. Neurol. 2012, 27, 131–145. [Google Scholar]
- Nijs, J.; Paul van Wilgen, C.; Van Oosterwijck, J.; van Ittersum, M.; Meeus, M. How to explain central sensitization to patients with ‘unexplained’ chronic musculoskeletal pain: Practice guidelines. Man. Ther. 2011, 16, 413–418. [Google Scholar] [CrossRef]
- Alburquerque-Sendín, F.; Camargo, P.R.; Vieira, A.; Salvini, T.F. Bilateral Myofascial Trigger Points and Pressure Pain Thresholds in the Shoulder Muscles in Patients With Unilateral Shoulder Impingement Syndrome: A Blinded, Controlled Study. Clin. J. Pain 2013, 29, 478–486. [Google Scholar] [CrossRef]
- Borstad, J.; Woeste, C. The role of sensitization in musculoskeletal shoulder pain. Braz. J. Phys. Ther. 2015, 19, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Sanchis, M.N.; Lluch, E.; Nijs, J.; Struyf, F.; Kangasperko, M. The role of central sensitization in shoulder pain: A systematic literature review. Semin. Arthritis Rheum. 2015, 44, 710–716. [Google Scholar] [CrossRef] [PubMed]
- Pertoldi, S.; Di Benedetto, P. Shoulder-hand syndrome after stroke. A complex regional pain syndrome. Eura. Medicophys. 2005, 41, 283–292. [Google Scholar] [PubMed]
- Hodges, P.W.; Tucker, K. Moving differently in pain: A new theory to explain the adaptation to pain. Pain 2011, 152, S90–S98. [Google Scholar] [CrossRef]
- Muceli, S.; Falla, D.; Farina, D. Reorganization of muscle synergies during multidirectional reaching in the horizontal plane with experimental muscle pain. J. Neurophysiol. 2014, 111, 1615–1630. [Google Scholar] [CrossRef]
- De Oliveira Silva, D.; Magalhaes, F.H.; Faria, N.C.; Pazzinatto, M.F.; Ferrari, D.; Pappas, E.; de Azevedo, F.M. Lower Amplitude of the Hoffmann Reflex in Women With Patellofemoral Pain: Thinking Beyond Proximal, Local, and Distal Factors. Arch. Phys. Med. Rehabil. 2016, 97, 1115–1120. [Google Scholar] [CrossRef]
- Coronado, R.A.; Simon, C.B.; Valencia, C.; George, S.Z. Experimental pain responses support peripheral and central sensitization in patients with unilateral shoulder pain. Clin. J. Pain 2014, 30, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Larkin-Kaiser, K.A.; Parr, J.J.; Borsa, P.A.; George, S.Z. Range of motion as a predictor of clinical shoulder pain during recovery from delayed-onset muscle soreness. J. Athl. Train. 2015, 50, 289–294. [Google Scholar] [CrossRef] [PubMed]
- Luime, J.J.; Koes, B.W.; Hendriksen, I.J.; Burdorf, A.; Verhagen, A.P.; Miedema, H.S.; Verhaar, J.A. Prevalence and incidence of shoulder pain in the general population; a systematic review. Scand. J. Rheumatol. 2004, 33, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Vangsgaard, S.; Taylor, J.L.; Hansen, E.A.; Madeleine, P. Changes in H reflex and neuromechanical properties of the trapezius muscle after 5 weeks of eccentric training: A randomized controlled trial. J. Appl. Physiol. 2014, 116, 1623–1631. [Google Scholar] [CrossRef] [PubMed]
- Falla, D.; Farina, D.; Graven-Nielsen, T. Experimental muscle pain results in reorganization of coordination among trapezius muscle subdivisions during repetitive shoulder flexion. Exp. Brain Res. 2007, 178, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Magee, D.J.; Zachazewski, J.E.; Quillen, W.S. Pathology and Intervention in Musculoskeletal Rehabilitation; Saunders/Elsevier: St. Louis, MO, USA, 2008. [Google Scholar]
- Worsley, P.; Warner, M.; Mottram, S.; Gadola, S.; Veeger, H.E.; Hermens, H.; Morrissey, D.; Little, P.; Cooper, C.; Carr, A.; et al. Motor control retraining exercises for shoulder impingement: Effects on function, muscle activation, and biomechanics in young adults. J. Shoulder Elb. Surg. 2013, 22, e11–e19. [Google Scholar] [CrossRef]
- Castelein, B.; Cagnie, B.; Parlevliet, T.; Cools, A. Superficial and Deep Scapulothoracic Muscle Electromyographic Activity During Elevation Exercises in the Scapular Plane. J. Orthop. Sports Phys. Ther. 2016, 46, 184–193. [Google Scholar] [CrossRef]
- Pizzari, T.; Wickham, J.; Balster, S.; Ganderton, C.; Watson, L. Modifying a shrug exercise can facilitate the upward rotator muscles of the scapula. Clin. Biomech. 2014, 29, 201–205. [Google Scholar] [CrossRef]
- Cole, A.K.; McGrath, M.L.; Harrington, S.E.; Padua, D.A.; Rucinski, T.J.; Prentice, W.E. Scapular bracing and alteration of posture and muscle activity in overhead athletes with poor posture. J. Athl. Train. 2013, 48, 12–24. [Google Scholar] [CrossRef]
- Moezy, A. The effects of scapular stabilization based exercise therapy on pain, posture, flexibility and shoulder mobility in patients with shoulder impingement syndrome: A controlled randomized clinical trial. Med J. Islam. Repub. Iran 2014, 28, 87. [Google Scholar]
- Phadke, V.; Camargo, P.; Ludewig, P. Scapular and rotator cuff muscle activity during arm elevation: A review of normal function and alterations with shoulder impingement. Rev. Bras. De Fisioter. 2009, 13, 1–9. [Google Scholar] [CrossRef]
- Tsuruike, M.; Ellenbecker, T.S. Serratus anterior and lower trapezius muscle activities during multi-joint isotonic scapular exercises and isometric contractions. J. Athl. Train. 2015, 50, 199–210. [Google Scholar] [CrossRef]
- Magarey, M.E.; Jones, M.A. Dynamic evaluation and early management of altered motor control around the shoulder complex. Man. Ther. 2003, 8, 195–206. [Google Scholar] [CrossRef]
- Watson, L.A.; Pizzari, T.; Balster, S. Thoracic outlet syndrome part 2: Conservative management of thoracic outlet. Man. Ther. 2010, 15, 305–314. [Google Scholar] [CrossRef]
- Lin, J.-J.; Hanten, W.P.; Olson, S.L.; Roddey, T.S.; Soto-quijano, D.A.; Lim, H.K.; Sherwood, A.M. Functional activity characteristics of individuals with shoulder dysfunctions. J. Electromyogr. Kinesiol. 2005, 15, 576–586. [Google Scholar] [CrossRef]
- Wadsworth, D.J.; Bullock-Saxton, J.E. Recruitment patterns of the scapular rotator muscles in freestyle swimmers with subacromial impingement. Int. J. Sports Med. 1997, 18, 618–624. [Google Scholar] [CrossRef]
- Camargo, P.R.; Neumann, D.A. Kinesiologic considerations for targeting activation of scapulothoracic muscles—Part 2: Trapezius. Braz. J. Phys. Ther. 2019, 23, 467–475. [Google Scholar] [CrossRef]
- Johnson, G.; Bogduk, N.; Nowitzke, A.; House, D. Anatomy and actions of the trapezius muscle. Clin. Biomech. 1994, 9, 44–50. [Google Scholar] [CrossRef] [PubMed]
- Alexander, C.M. Altered control of the trapezius muscle in subjects with non-traumatic shoulder instability. Clin. Neurophysiol. 2007, 118, 2664–2671. [Google Scholar] [CrossRef] [PubMed]
- Alexander, C.; Miley, R.; Stynes, S.; Harrison, P.J. Differential control of the scapulothoracic muscles in humans. J. Physiol. 2007, 580, 777–786. [Google Scholar] [CrossRef]
- Vangsgaard, S.; Hansen, E.A.; Madeleine, P. Between-day reliability of the trapezius muscle H-reflex and M-wave. Muscle Nerve 2015, 52, 1066–1071. [Google Scholar] [CrossRef] [PubMed]
- Heckman, C.J.; Mottram, C.; Quinlan, K.; Theiss, R.; Schuster, J. Motoneuron excitability: The importance of neuromodulatory inputs. Clin. Neurophysiol. 2009, 120, 2040–2054. [Google Scholar] [CrossRef] [PubMed]
- Misiaszek, J.E. The H-reflex as a tool in neurophysiology: Its limitations and uses in understanding nervous system function. Muscle Nerve 2003, 28, 144–160. [Google Scholar] [CrossRef] [PubMed]
- Palmieri, R.M.; Ingersoll, C.D.; Hoffman, M.A. The hoffmann reflex: Methodologic considerations and applications for use in sports medicine and athletic training research. J. Athl. Train. 2004, 39, 268–277. [Google Scholar] [PubMed]
- Alexander, C.M.; Stynes, S.; Thomas, A.; Lewis, J.; Harrison, P.J. Does tape facilitate or inhibit the lower fibres of trapezius? Man. Ther. 2003, 8, 37–41. [Google Scholar] [CrossRef]
- Ge, H.Y.; Serrao, M.; Andersen, O.K.; Graven-Nielsen, T.; Arendt-Nielsen, L. Increased H-reflex response induced by intramuscular electrical stimulation of latent myofascial trigger points. Acupunct. Med. 2009, 27, 150–154. [Google Scholar] [CrossRef]
- Mazzocchio, R.; Scarfò, G.B.; Mariottini, A.; Muzii, V.F.; Palma, L. Recruitment curve of the soleus H-reflex in chronic back pain and lumbosacral radiculopathy. BMC Musculoskelet. Disord. 2001, 2, 4. [Google Scholar] [CrossRef]
- Ginanneschi, F.; Dominici, F.; Milani, P.; Biasella, A.; Rossi, A.; Mazzocchio, R. Changes in the recruitment curve of the soleus H-reflex associated with chronic low back pain. Clin. Neurophysiol. 2007, 118, 111–118. [Google Scholar] [CrossRef]
- Vangsgaard, S.; Nørgaard, L.T.; Flaskager, B.K.; Søgaard, K.; Taylor, J.L.; Madeleine, P. Eccentric exercise inhibits the H reflex in the middle part of the trapezius muscle. Eur. J. Appl. Physiol. 2013, 113, 77–87. [Google Scholar] [CrossRef]
- Johal, J.; Iwanaga, J.; Tubbs, K.; Loukas, M.; Oskouian, R.J.; Tubbs, R.S. The Accessory Nerve: A Comprehensive Review of its Anatomy, Development, Variations, Landmarks and Clinical Considerations. Anat. Rec. 2019, 302, 620–629. [Google Scholar] [CrossRef]
- Alexander, C.M.; Harrison, P.J. The bilateral reflex control of the trapezius muscle in humans. Exp. Brain Res. 2002, 142, 418–424. [Google Scholar] [CrossRef]
- Feng, Y.N.; Li, Y.P.; Liu, C.L.; Zhang, Z.J. Assessing the elastic properties of skeletal muscle and tendon using shearwave ultrasound elastography and MyotonPRO. Sci. Rep. 2018, 8, 17064. [Google Scholar] [CrossRef] [PubMed]
- Kelly, J.P.; Koppenhaver, S.L.; Michener, L.A.; Proulx, L.; Bisagni, F.; Cleland, J.A. Characterization of tissue stiffness of the infraspinatus, erector spinae, and gastrocnemius muscle using ultrasound shear wave elastography and superficial mechanical deformation. J. Electromyogr. Kinesiol. 2018, 38, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Kocur, P.; Wilski, M.; Lewandowski, J.; Łochyński, D. Female Office Workers With Moderate Neck Pain Have Increased Anterior Positioning of the Cervical Spine and Stiffness of Upper Trapezius Myofascial Tissue in Sitting Posture. PM R 2019, 11, 476–482. [Google Scholar] [CrossRef] [PubMed]
- Kamonseki, D.H.; Haik, M.N.; Ribeiro, L.P.; Almeida, R.F.d.; Almeida, L.A.d.; Fonseca, C.L.; Camargo, P.R. Measurement properties of the Brazilian versions of Fear-Avoidance Beliefs Questionnaire and Tampa Scale of Kinesiophobia in individuals with shoulder pain. PLoS ONE 2021, 16, e0260452. [Google Scholar] [CrossRef]
- Boonstra, A.M.; Stewart, R.E.; Köke, A.J.A.; Oosterwijk, R.F.A.; Swaan, J.L.; Schreurs, K.M.G.; Schiphorst Preuper, H.R. Cut-Off Points for Mild, Moderate, and Severe Pain on the Numeric Rating Scale for Pain in Patients with Chronic Musculoskeletal Pain: Variability and Influence of Sex and Catastrophizing. Front. Psychol. 2016, 7, 1466. [Google Scholar] [CrossRef]
- Duarte, A. Validação Intercultural do Shoulder Pain and Disability Index—SPADI; [monography]—Escola Superior de Tecnologia da Saúde de Coimbra: Coimbra, Portugal, 2002. [Google Scholar]
- Leal, S. Constant Score e Shoulder Pain and Disability Index (SPADI)—Adaptação Cultural e Linguística; [monography]—Escola Superior de Tecnologia da Saúde de Coimbra: Coimbra, Portugal, 2001. [Google Scholar]
- Roy, J.S.; MacDermid, J.C.; Woodhouse, L.J. Measuring shoulder function: A systematic review of four questionnaires. Arthritis Rheum. 2009, 61, 623–632. [Google Scholar] [CrossRef] [PubMed]
- Kamonseki, D.H.; Haik, M.N.; Camargo, P.R. Scapular movement training versus standardized exercises for individuals with chronic shoulder pain: Protocol for a randomized controlled trial. Braz. J. Phys. Ther. 2021, 25, 221–229. [Google Scholar] [CrossRef]
- Kibler, W.B.; Uhl, T.L.; Maddux, J.W.; Brooks, P.V.; Zeller, B.; McMullen, J. Qualitative clinical evaluation of scapular dysfunction: A reliability study. J. Shoulder Elb. Surg. 2002, 11, 550–556. [Google Scholar] [CrossRef]
- Huang, T.-S.; Huang, H.-Y.; Wang, T.-G.; Tsai, Y.-S.; Lin, J.-J. Comprehensive classification test of scapular dyskinesis: A reliability study. Man. Ther. 2015, 20, 427–432. [Google Scholar] [CrossRef]
- Heick, J.; Haggerty, J.; Manske, R. A Comparison of Resting Scapular Posture and the Davies Closed Kinetic Chain Upper Extremity Stability Test. Int. J. Sports Phys. Ther. 2021, 16, 835–843. [Google Scholar] [CrossRef]
- Struyf, F.; Nijs, J.; Mottram, S.; Roussel, N.A.; Cools, A.M.; Meeusen, R. Clinical assessment of the scapula: A review of the literature. Br. J. Sports Med. 2014, 48, 883–890. [Google Scholar] [CrossRef] [PubMed]
- Cools, A.M.; Dewitte, V.; Lanszweert, F.; Notebaert, D.; Roets, A.; Soetens, B.; Cagnie, B.; Witvrouw, E.E. Rehabilitation of scapular muscle balance: Which exercises to prescribe? Am. J. Sports Med. 2007, 35, 1744–1751. [Google Scholar] [CrossRef] [PubMed]
- Hermens, H.J.; Freriks, B.; Merletti, R.; Stegeman, D.; Blok, J.; Rau, G.; Disselhorst-Klug, C.; Hägg, G. European recommendations for surface electromyography. Roessingh Res. Dev. 1999, 8, 13–54. [Google Scholar]
- Heuberer, P.; Kranzl, A.; Laky, B.; Anderl, W.; Wurnig, C. Electromyographic analysis: Shoulder muscle activity revisited. Arch. Orthop. Trauma Surg. 2015, 135, 549–563. [Google Scholar] [CrossRef]
- Vangsgaard, S.; Nørgaard, L.T.; Madeleine, P.; Taylor, J.L. Crossed responses found in human trapezius muscles are not H-reflexes. Muscle Nerve 2014, 49, 362–369. [Google Scholar] [CrossRef]
- Pierrot-Deseilligny, E.; Burke, D. The Circuitry of the Human Spinal Cord: Its Role in Motor Control and Movement Disorders; Cambridge University Press: Cambridge, UK, 2005. [Google Scholar]
- Burke, D. Clinical uses of H reflexes of upper and lower limb muscles. Clin. Neurophysiol. Pract. 2016, 1, 9–17. [Google Scholar] [CrossRef]
- Ekstrom, R.A.; Soderberg, G.L.; Donatelli, R.A. Normalization procedures using maximum voluntary isometric contractions for the serratus anterior and trapezius muscles during surface EMG analysis. J. Electromyogr. Kinesiol. 2005, 15, 418–428. [Google Scholar] [CrossRef]
- Kibler, W.B.; Sciascia, A.D.; Uhl, T.L.; Tambay, N.; Cunningham, T. Electromyographic analysis of specific exercises for scapular control in early phases of shoulder rehabilitation. Am. J. Sports Med. 2008, 36, 1789–1798. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Cynn, H.S.; Yoon, T.L.; Ko, C.H.; Choi, W.J.; Choi, S.A.; Choi, B.S. The effect of scapular posterior tilt exercise, pectoralis minor stretching, and shoulder brace on scapular alignment and muscles activity in subjects with round-shoulder posture. J. Electromyogr. Kinesiol. 2015, 25, 107–114. [Google Scholar] [CrossRef]
- Field, A. Descobrindo a Estatística Usando o SPSS-2: Artmed Editora; Porto Alegre, Brasil, 2009. [Google Scholar]
- Haik, M.N.; Alburquerque-Sendín, F.; Silva, C.Z.; Siqueira-Junior, A.L.; Ribeiro, I.L.; Camargo, P.R. Scapular kinematics pre–and post–thoracic thrust manipulation in individuals with and without shoulder impingement symptoms: A randomized controlled study. J. Orthop. Sport. Phys. Ther. 2014, 44, 475–487. [Google Scholar] [CrossRef]
- Clark, J.; Nijs, J.; Yeowell, G.; Goodwin, P.C. What Are the Predictors of Altered Central Pain Modulation in Chronic Musculoskeletal Pain Populations? A Systematic Review. Pain Physician 2017, 20, 487–500. [Google Scholar] [CrossRef]
- Den Boer, C.; Dries, L.; Terluin, B.; van der Wouden, J.C.; Blankenstein, A.H.; van Wilgen, C.P.; Lucassen, P.; van der Horst, H.E. Central sensitization in chronic pain and medically unexplained symptom research: A systematic review of definitions, operationalizations and measurement instruments. J. Psychosom. Res. 2019, 117, 32–40. [Google Scholar] [CrossRef]
- Martinez-Calderon, J.; Meeus, M.; Struyf, F.; Miguel Morales-Asencio, J.; Gijon-Nogueron, G.; Luque-Suarez, A. The role of psychological factors in the perpetuation of pain intensity and disability in people with chronic shoulder pain: A systematic review. BMJ Open 2018, 8, e020703. [Google Scholar] [CrossRef] [PubMed]
- Walankar, P.P.; Panhale, V.P.; Patil, M.M. Psychosocial factors, disability and quality of life in chronic shoulder pain patients with central sensitization. Health Psychol. Res. 2020, 8, 8874. [Google Scholar] [CrossRef]
- Madeleine, P.; Mathiassen, S.E.; Arendt-Nielsen, L. Changes in the degree of motor variability associated with experimental and chronic neck-shoulder pain during a standardised repetitive arm movement. Exp. Brain Res. 2008, 185, 689–698. [Google Scholar] [CrossRef]
- Mario, P. The Epidemiology of Shoulder Pain: A Narrative Review of the Literature. In Pain in Perspective; Subhamay, G., Ed.; IntechOpen: Rijeka, Croatia, 2012; p. Ch. 7. [Google Scholar]
- Nieto, F.R.; Vuckovic, S.M.; Prostran, M.S. Editorial: Mechanisms and New Targets for the Treatment of Chronic Pain. Front. Pharmacol. 2020, 11, 600037. [Google Scholar] [CrossRef]
- Schulte, E.; Ciubotariu, A.; Arendt-Nielsen, L.; Disselhorst-Klug, C.; Rau, G.; Graven-Nielsen, T. Experimental muscle pain increases trapezius muscle activity during sustained isometric contractions of arm muscles. Clin. Neurophysiol. 2004, 115, 1767–1778. [Google Scholar] [CrossRef]
- Alexander, C.M.; Miley, R.; Harrison, P.J. Functional modulation of shoulder girdle stability. Exp. Brain Res. 2005, 161, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.M.; Hart, J.M.; Saliba, S.A.; Hertel, J. Modulation of the Fibularis Longus Hoffmann Reflex and Postural Instability Associated With Chronic Ankle Instability. J. Athl. Train. 2016, 51, 637–643. [Google Scholar] [CrossRef] [PubMed]
- Yamauchi, T.; Hasegawa, S.; Matsumura, A.; Nakamura, M.; Ibuki, S.; Ichihashi, N. The effect of trunk rotation during shoulder exercises on the activity of the scapular muscle and scapular kinematics. J. Shoulder Elb. Surg. 2015, 24, 955–964. [Google Scholar] [CrossRef]
- Moeller, C.R.; Bliven, K.C.; Valier, A.R. Scapular muscle-activation ratios in patients with shoulder injuries during functional shoulder exercises. J. Athl. Train. 2014, 49, 345–355. [Google Scholar] [CrossRef] [PubMed]
- Castelein, B.; Cagnie, B.; Cools, A. Scapular muscle dysfunction associated with subacromial pain syndrome. J. Hand Ther. 2017, 30, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.; Abbod, M.; Shieh, J.S. Pain and Stress Detection Using Wearable Sensors and Devices-A Review. Sensors 2021, 21, 1030. [Google Scholar] [CrossRef]
- Mendez-Rebolledo, G.; Guzman-Muňoz, E.; Concha-Araya, J.; Aravena-Falcon, M.; Galvez-Gonzalez, V.; de la Rosa, F.B. Relationship between anthropometric and electromyographic variables of the scapular muscles. Hum. Mov. 2020, 21, 1–6. [Google Scholar] [CrossRef]
- Zhu, J.; Yi, C.; Wei, B.; Yang, C.; Ding, Z.; Jiang, F. The Muscle Fatigue’s Effects on the sEMG-Based Gait Phase Classification: An Experimental Study and a Novel Training Strategy. Appl. Sci. 2021, 11, 3821. [Google Scholar] [CrossRef]
- Stutzig, N.; Siebert, T. Assessment of the H-reflex at two contraction levels before and after fatigue. Scand. J. Med. Sci. Sports 2017, 27, 399–407. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Asymptomatic Group (n = 12) | Symptomatic Group (n = 12) | Comparison between Groups | |||
|---|---|---|---|---|---|
| Parameter | mean ± SD | mean ± SD | t | p-value | |
| Height (m) | 1.7 ± 0.09 | 1.7 ± 0.08 | 0.345 | 0.733 | |
| Weight (kg) | 69.8 ± 14.02 | 68.3 ± 14.10 | 0.269 | 0.791 | |
| BMI (kg/m2) | 23.0 ± 3.12 | 22.9 ± 3.50 | 0.127 | 0.900 | |
| median ± IR | median ± IR | U | p-value | ||
| Age (years) | 23.0 ± 9.00 | 22.0 ± 2.75 | 58.00 | 0.443 | |
| frequency (n) | frequency (n) | Pearson X2 | p-value | ||
| Scapular positioning | Without changes | 67% (n = 8) | 0% (n = 0) | 12.000 | 0.001 * |
| Presenting a dyskinesis type | 33% (n = 4): Two subjects with type II and two with type III | 100% (n = 12): Three subjects with type I, two with type II, four with type III and two with type II + III | |||
| H reflex—frequency of responses identified | UT | 75% (n = 9) | 58% (n = 7) | 0.750 | 0.386 |
| MT | 75% (n = 9) | 58% (n = 7) | 0.750 | 0.386 | |
| LT | 58% (n = 7) | 42% (n = 5) | 0.667 | 0.414 | |
| M-wave—frequency of responses identified | UT | 100% (n = 12) | 100% (n = 12) | - | - |
| MT | 92% (n = 11) | 100% (n = 12) | 1.043 | 1.000 | |
| LT | 100% (n = 12) | 100% (n = 12) | - | - | |
| Asymptomatic Group | Symptomatic Group | Comparison between Groups | Effect Size | ||||
|---|---|---|---|---|---|---|---|
| Parameter | Muscle | mean ± SD | mean ± SD | t | p-value | ||
| Current at Hmax (mA) | UT | 5.83 ± 1.28 | 4.75 ± 2.41 | 1.163 | 0.264 | 0.586 | |
| MT | 5.50 ± 1.34 | 6.79 ± 5.90 | 0.448 | 0.661 | 0.226 | ||
| LT | 4.79 ± 1.85 | 5.68 ± 2.95 | −0.648 | 0.532 | −0.379 | ||
| Hmax (mV) | UT | 0.34 ± 0.28 | 0.13 ± 0.10 | 1.628 | 0.060 | 0.957 | |
| MT | 0.14 ± 0.21 | 0.15 ± 0.17 | −0.053 | 0.959 | −0.027 | ||
| LT | 0.12 ± 0.16 | 0.04 ± 0.02 | 0.503 | 0.630 | 0.252 | ||
| Mmax (mV) | UT | 1.64 ± 0.99 | 2.20 ± 1.48 | −1.076 | 0.293 | −0.439 | |
| MT | 1.83 ± 1.38 | 1.90 ± 0.93 | −0.159 | 0.875 | −0.066 | ||
| LT | 2.02 ± 1.10 | 1.84 ± 0.66 | 0.494 | 0.626 | 0.202 | ||
| % Hmax/Mmax | UT | 18.58 ± 11.61 | 6.20 ± 5.05 | 2.619 | 0.020 * | 1.320 | |
| MT | 10.86 ± 10.95 | 7.10 ± 8.28 | 0.741 | 0.472 | 0.383 | ||
| LT | 6.33 ± 8.25 | 2.32 ± 0.96 | 0.701 | 0.503 | 0.357 | ||
| Hmax latency (ms) | UT | 8.94 ± 0.39 | 10.50 ± 2.55 | −1.600 | 0.159 | −0.918 | |
| MT | 10.50 ± 1.66 | 11.50 ± 2.35 | −1.001 | 0. 334 | −0.505 | ||
| LT | 10.71 ± 1.04 | 14.10 ± 3.15 | −2.692 | 0.023 * | −1.576 | ||
| U | p-value | ||||||
| Mmax latency (ms) | UT | 3.62 ± 1.80 | 3.00 ± 0.43 | 57.000 | 0.343 | - | |
| MT | 4.18 ± 1.08 | 4.04 ± 0.66 | 66.500 | 0.974 | - | ||
| LT | 5.42 ± 1.86 | 5.21 ± 0.86 | 75.500 | 0.835 | - | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Melo, A.S.C.; Taylor, J.L.; Ferreira, R.; Cunha, B.; Ascenção, M.; Fernandes, M.; Sousa, V.; Cruz, E.B.; Vilas-Boas, J.P.; Sousa, A.S.P. Differences in Trapezius Muscle H-Reflex between Asymptomatic Subjects and Symptomatic Shoulder Pain Subjects. Sensors 2023, 23, 4217. https://doi.org/10.3390/s23094217
Melo ASC, Taylor JL, Ferreira R, Cunha B, Ascenção M, Fernandes M, Sousa V, Cruz EB, Vilas-Boas JP, Sousa ASP. Differences in Trapezius Muscle H-Reflex between Asymptomatic Subjects and Symptomatic Shoulder Pain Subjects. Sensors. 2023; 23(9):4217. https://doi.org/10.3390/s23094217
Chicago/Turabian StyleMelo, Ana S. C., Janet L. Taylor, Ricardo Ferreira, Bruno Cunha, Manuel Ascenção, Mathieu Fernandes, Vítor Sousa, Eduardo B. Cruz, J. Paulo Vilas-Boas, and Andreia S. P. Sousa. 2023. "Differences in Trapezius Muscle H-Reflex between Asymptomatic Subjects and Symptomatic Shoulder Pain Subjects" Sensors 23, no. 9: 4217. https://doi.org/10.3390/s23094217
APA StyleMelo, A. S. C., Taylor, J. L., Ferreira, R., Cunha, B., Ascenção, M., Fernandes, M., Sousa, V., Cruz, E. B., Vilas-Boas, J. P., & Sousa, A. S. P. (2023). Differences in Trapezius Muscle H-Reflex between Asymptomatic Subjects and Symptomatic Shoulder Pain Subjects. Sensors, 23(9), 4217. https://doi.org/10.3390/s23094217