
Fluctuations in Upper and Lower Body Movement during Walking in Normal Pressure Hydrocephalus and Parkinson’s Disease Assessed by Motion Capture with a Smartphone Application, TDPT-GT

 ,
, 
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Approvals
2.2. Study Population
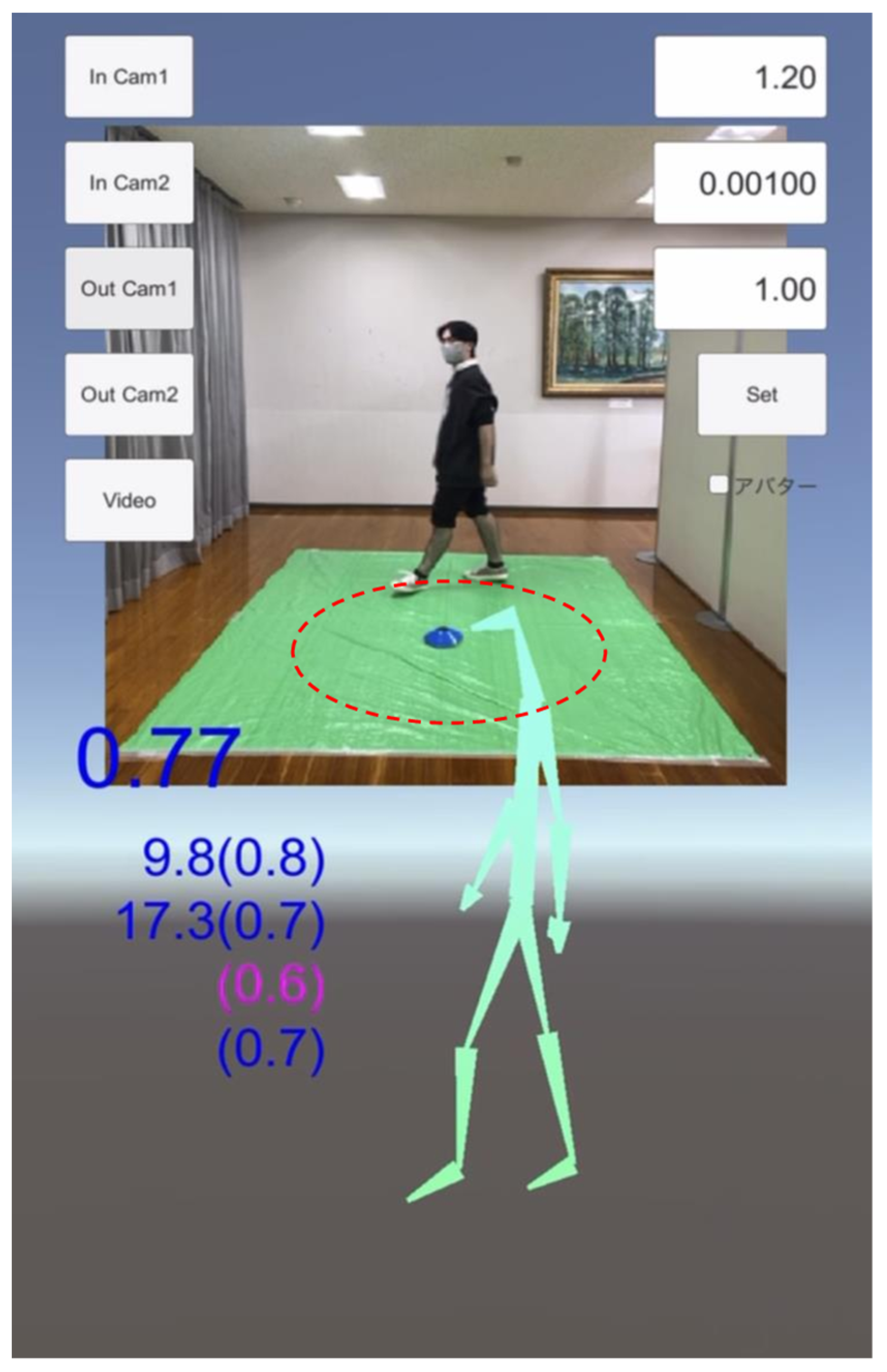
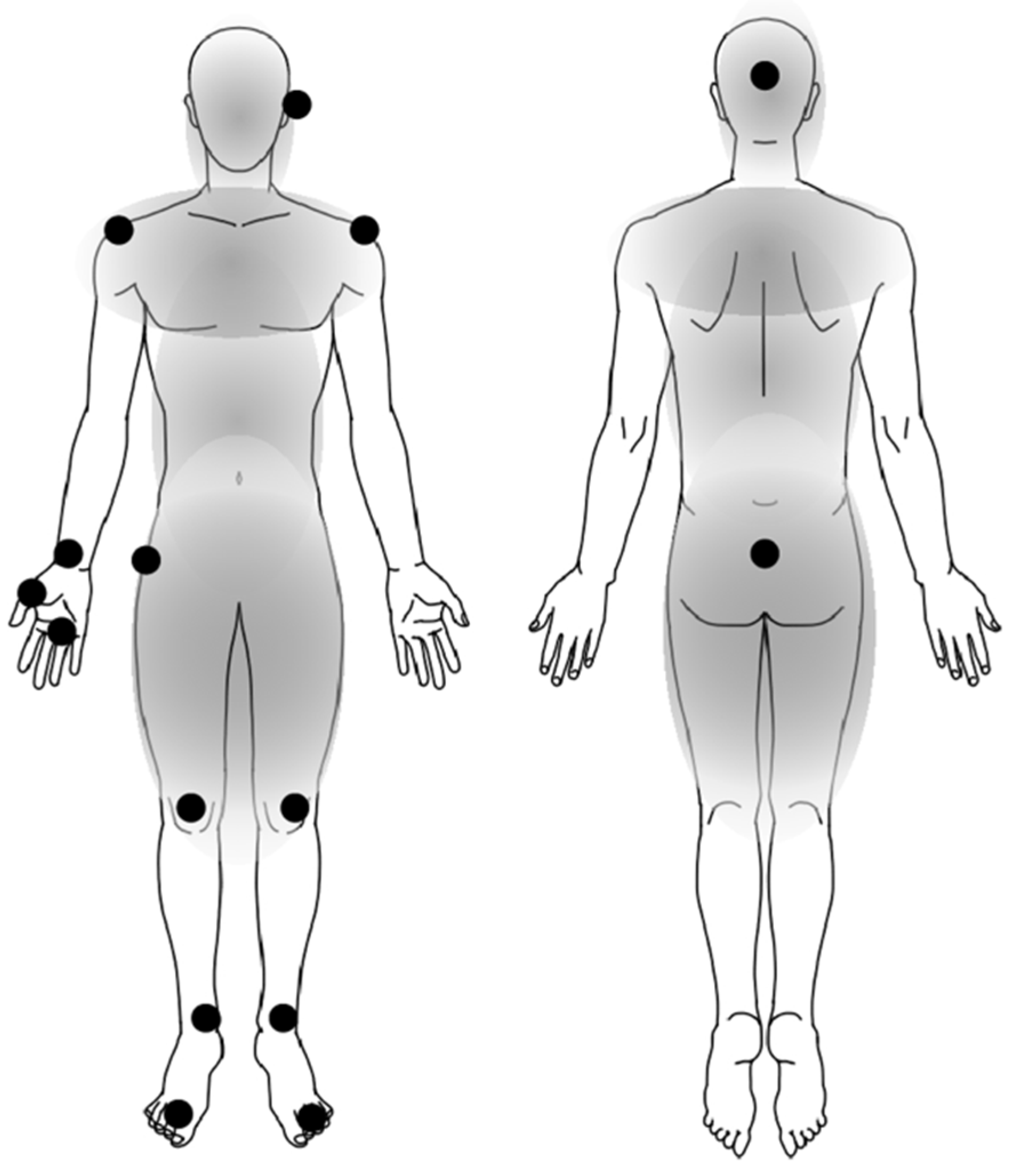
2.3. Data Acquisition of Estimated Three-Dimensional Relative Coordinates during 1 m Circle Walking
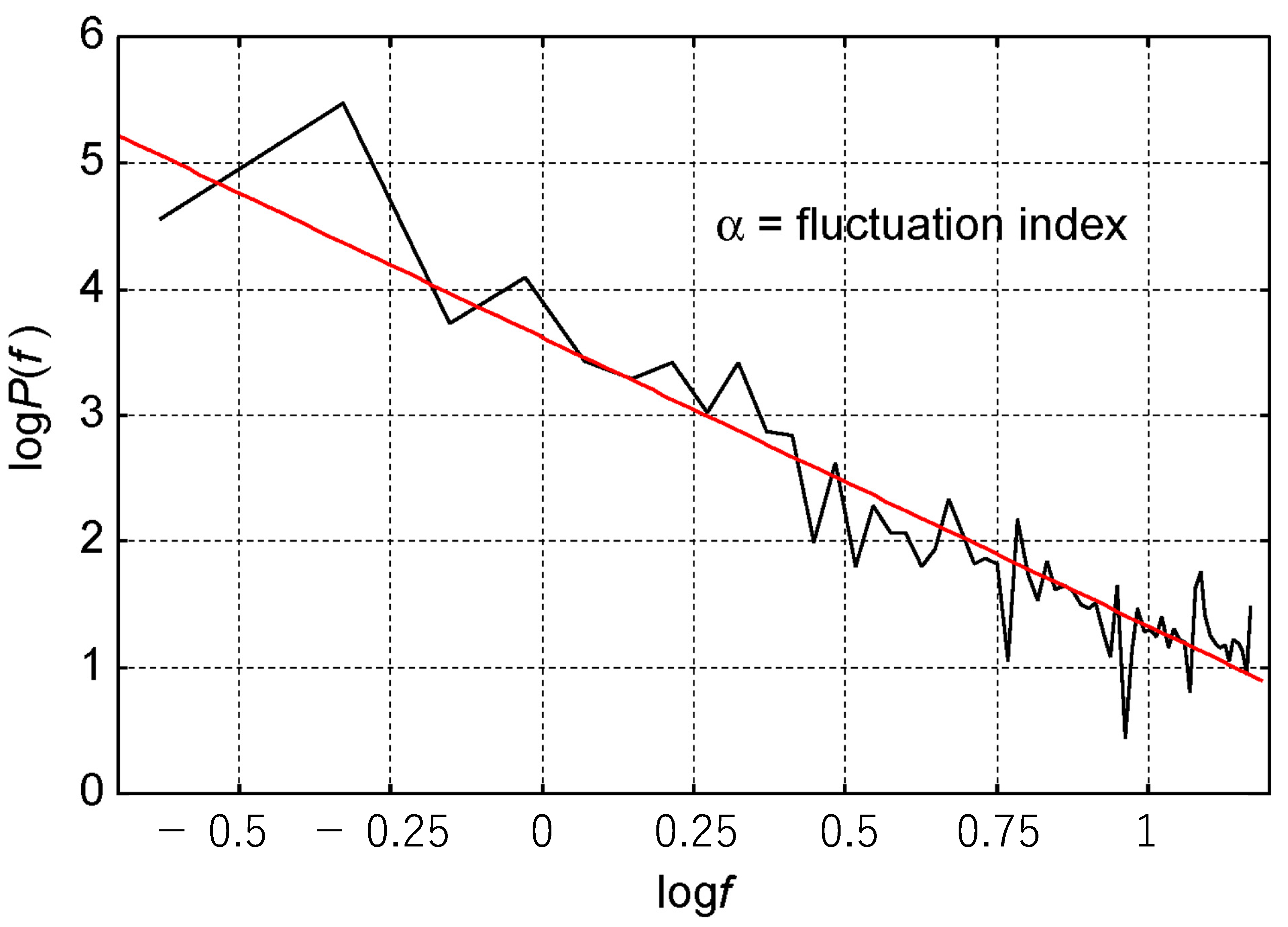
2.4. Fluctuation in Body Positions during Walking
2.5. Statistical Analysis
3. Results
3.1. Clinical Characteristics
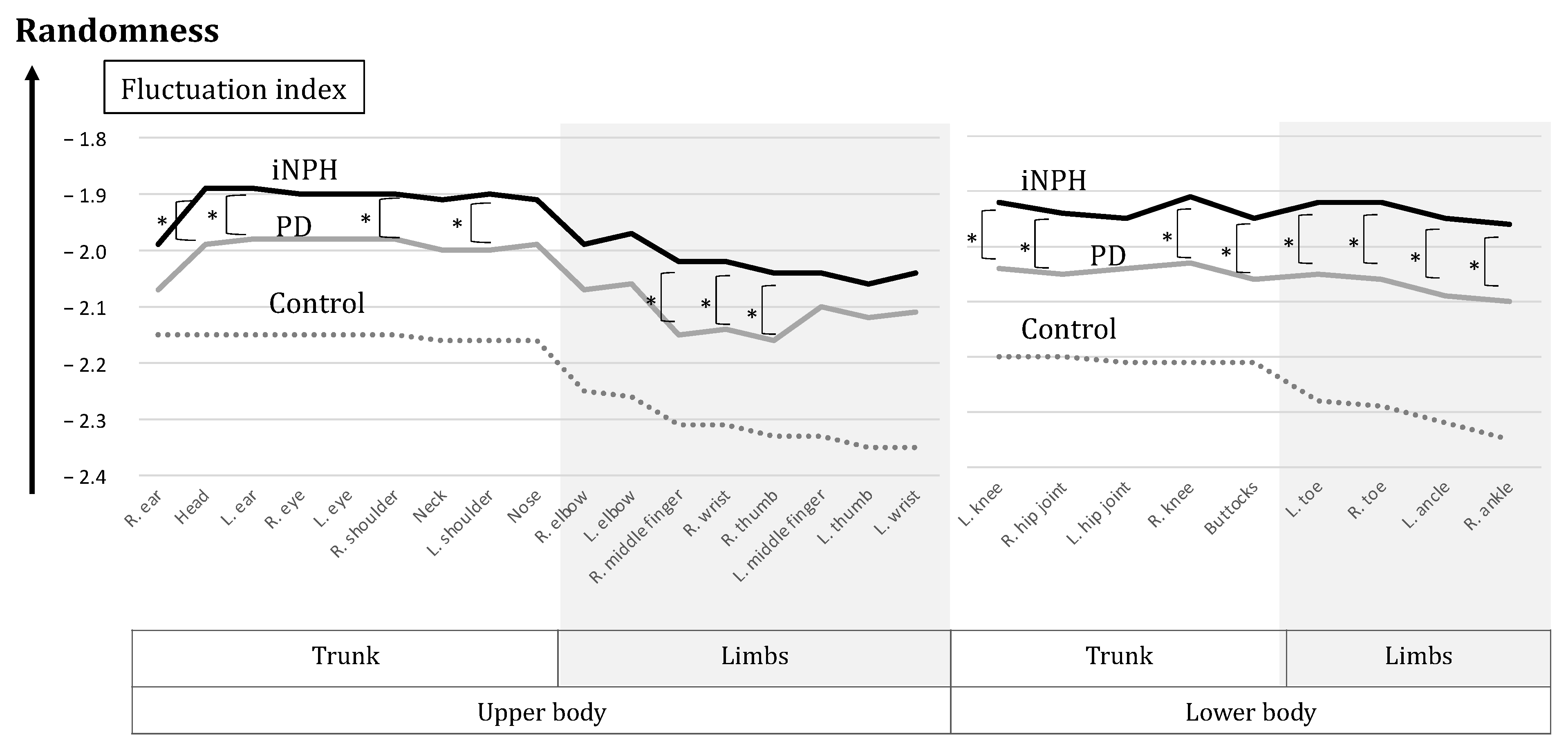
3.2. Fluctuation Index for Each Body Position
4. Discussion
4.1. Analysis of Gait by the System of TDPT-GT
4.2. Fluctuation during Walking in Patients with iNPH and PD
4.3. Prospects for Using the Technology
4.4. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stolze, H.; Kuhtz-Buschbeck, J.P.; Drücke, H.; Jöhnk, K.; Illert, M.; Deuschl, G. Comparative analysis of the gait disorder of normal pressure hydrocephalus and Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 2001, 70, 289–297. [Google Scholar] [CrossRef] [PubMed]
- Bugalho, P.; Alves, L.; Miguel, R. Gait dysfunction in Parkinson’s disease and normal pressure hydrocephalus: A comparative study. J. Neural Transm. 2013, 120, 1201–1207. [Google Scholar] [CrossRef]
- Silva de Lima, A.L.; Evers, L.J.W.; Hahn, T.; Bataille, L.; Hamilton, J.L.; Little, M.A.; Okuma, Y.; Bloem, B.R.; Faber, M.J. Freezing of gait and fall detection in Parkinson’s disease using wearable sensors: A systematic review. J. Neurol. 2017, 264, 1642–1654. [Google Scholar] [CrossRef]
- Raccagni, C.; Nonnekes, J.; Bloem, B.R.; Peball, M.; Boehme, C.; Seppi, K.; Wenning, G.K. Gait and postural disorders in parkinsonism: A clinical approach. J. Neurol. 2020, 267, 3169–3176. [Google Scholar] [CrossRef] [PubMed]
- Gouelle, A.; Megrot, F.; Presedo, A.; Husson, I.; Yelnik, A.; Pennecot, G.F. The gait variability index: A new way to quantify fluctuation magnitude of spatiotemporal parameters during gait. Gait Posture 2013, 38, 461–465. [Google Scholar] [CrossRef] [PubMed]
- Buckley, E.; Mazza, C.; McNeill, A. A systematic review of the gait characteristics associated with Cerebellar Ataxia. Gait Posture 2018, 60, 154–163. [Google Scholar] [CrossRef]
- Debu, B.; De Oliveira Godeiro, C.; Lino, J.C.; Moro, E. Managing Gait, Balance, and Posture in Parkinson’s Disease. Curr. Neurol. Neurosci. Rep. 2018, 18, 23. [Google Scholar] [CrossRef]
- Ishikawa, M.; Yamada, S.; Yamamoto, K. Agreement study on gait assessment using a video-assisted rating method in patients with idiopathic normal-pressure hydrocephalus. PLoS ONE 2019, 14, e0224202. [Google Scholar] [CrossRef]
- Nakajima, M.; Yamada, S.; Miyajima, M.; Ishii, K.; Kuriyama, N.; Kazui, H.; Kanemoto, H.; Suehiro, T.; Yoshiyama, K.; Kameda, M.; et al. Guidelines for Management of Idiopathic Normal Pressure Hydrocephalus (Third Edition): Endorsed by the Japanese Society of Normal Pressure Hydrocephalus. Neurol. Med. Chir. 2021, 61, 63–97. [Google Scholar] [CrossRef]
- Milletti, D.; Randi, F.T.; Lanzino, G.; Hakim, F.; Palandri, G. Gait Apraxia and Hakim’s Disease: A Historical Review. Biomedicines 2023, 11, 1086. [Google Scholar] [CrossRef]
- Milne, S.C.; Hocking, D.R.; Georgiou-Karistianis, N.; Murphy, A.; Delatycki, M.B.; Corben, L.A. Sensitivity of spatiotemporal gait parameters in measuring disease severity in Friedreich ataxia. Cerebellum 2014, 13, 677–688. [Google Scholar] [CrossRef] [PubMed]
- Yamada, S.; Aoyagi, Y.; Yamamoto, K.; Ishikawa, M. Quantitative Evaluation of Gait Disturbance on an Instrumented Timed Up-and-go Test. Aging Dis. 2019, 10, 23–36. [Google Scholar] [CrossRef] [PubMed]
- Yamada, S.; Aoyagi, Y.; Ishikawa, M.; Yamaguchi, M.; Yamamoto, K.; Nozaki, K. Gait Assessment Using Three-Dimensional Acceleration of the Trunk in Idiopathic Normal Pressure Hydrocephalus. Front. Aging Neurosci. 2021, 13, 653964. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, Y.; Hobara, H.; Matsushita, S.; Mochimaru, M. Key joint kinematic characteristics of the gait of fallers identified by principal component analysis. J. Biomech. 2014, 47, 2424–2429. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, Y.; Hobara, H.; Heldoorn, T.A.; Kouchi, M.; Mochimaru, M. Age-independent and age-dependent sex differences in gait pattern determined by principal component analysis. Gait Posture 2016, 46, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Hardstone, R.; Poil, S.S.; Schiavone, G.; Jansen, R.; Nikulin, V.V.; Mansvelder, H.D.; Linkenkaer-Hansen, K. Detrended fluctuation analysis: A scale-free view on neuronal oscillations. Front. Physiol. 2012, 3, 450. [Google Scholar] [CrossRef]
- Neumcke, B. 1/f noise in membranes. Eur. Biophys. J. 1978, 4, 179–199. [Google Scholar] [CrossRef]
- Gilden, D.L.; Thornton, T.; Mallon, M.W. 1/f noise in human cognition. Science 1995, 267, 1837–1839. [Google Scholar] [CrossRef]
- Diniz, A.; Wijnants, M.L.; Torre, K.; Barreiros, J.; Crato, N.; Bosman, A.M.; Hasselman, F.; Cox, R.F.; Van Orden, G.C.; Delignieres, D. Contemporary theories of 1/f noise in motor control. Hum. Mov. Sci. 2011, 30, 889–905. [Google Scholar] [CrossRef]
- Yamada, N. Chaotic swaying of the upright posture. Hum. Mov. Sci. 1995, 14, 711–726. [Google Scholar] [CrossRef]
- Hausdorff, J.M. Gait variability: Methods, modeling and meaning. J. Neuroeng. Rehabil. 2005, 2, 19. [Google Scholar] [CrossRef] [PubMed]
- Hove, M.J.; Suzuki, K.; Uchitomi, H.; Orimo, S.; Miyake, Y. Interactive rhythmic auditory stimulation reinstates natural 1/f timing in gait of Parkinson’s patients. PLoS ONE 2012, 7, e32600. [Google Scholar] [CrossRef]
- Huisinga, J.M.; Mancini, M.; St George, R.J.; Horak, F.B. Accelerometry reveals differences in gait variability between patients with multiple sclerosis and healthy controls. Ann. Biomed. Eng. 2013, 41, 1670–1679. [Google Scholar] [CrossRef] [PubMed]
- Herman, T.; Weiss, A.; Brozgol, M.; Giladi, N.; Hausdorff, J.M. Gait and balance in Parkinson’s disease subtypes: Objective measures and classification considerations. J. Neurol. 2014, 261, 2401–2410. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, A.; Brach, J.S.; Perera, S.; Sejdic, E. A comparative analysis of spectral exponent estimation techniques for 1/f(beta) processes with applications to the analysis of stride interval time series. J. Neurosci. Methods 2014, 222, 118–130. [Google Scholar] [CrossRef] [PubMed]
- Uchitomi, H.; Ogawa, K.-i.; Orimo, S.; Wada, Y.; Miyake, Y. Effect of Interpersonal Interaction on Festinating Gait Rehabilitation in Patients with Parkinson’s Disease. PLoS ONE 2016, 11, e0155540. [Google Scholar] [CrossRef]
- Fu, C.; Suzuki, Y.; Morasso, P.; Nomura, T. Phase resetting and intermittent control at the edge of stability in a simple biped model generates 1/f-like gait cycle variability. Biol. Cybern. 2020, 114, 95–111. [Google Scholar] [CrossRef]
- Sidoroff, V.; Raccagni, C.; Kaindlstorfer, C.; Eschlboeck, S.; Fanciulli, A.; Granata, R.; Eskofier, B.; Seppi, K.; Poewe, W.; Willeit, J.; et al. Characterization of gait variability in multiple system atrophy and Parkinson’s disease. J. Neurol. 2021, 268, 1770–1779. [Google Scholar] [CrossRef]
- Dingwell, J.B.; Salinas, M.M.; Cusumano, J.P. Increased gait variability may not imply impaired stride-to-stride control of walking in healthy older adults: Winner: 2013 Gait and Clinical Movement Analysis Society Best Paper Award. Gait Posture 2017, 55, 131–137. [Google Scholar] [CrossRef]
- Hausdorff, J.M. Gait dynamics, fractals and falls: Finding meaning in the stride-to-stride fluctuations of human walking. Hum. Mov. Sci. 2007, 26, 555–589. [Google Scholar] [CrossRef]
- Hausdorff, J.M. Gait dynamics in Parkinson’s disease: Common and distinct behavior among stride length, gait variability, and fractal-like scaling. Chaos 2009, 19, 026113. [Google Scholar] [CrossRef] [PubMed]
- Aoyagi, Y.; Yamada, S.; Ueda, S.; Iseki, C.; Kondo, T.; Mori, K.; Kobayashi, Y.; Fukami, T.; Hoshimaru, M.; Ishikawa, M.; et al. Development of Smartphone Application for Markerless Three-Dimensional Motion Capture Based on Deep Learning Model. Sensors 2022, 22, 5282. [Google Scholar] [CrossRef] [PubMed]
- Yamada, S.; Aoyagi, Y.; Iseki, C.; Kondo, T.; Kobayashi, Y.; Ueda, S.; Mori, K.; Fukami, T.; Tanikawa, M.; Mase, M.; et al. Quantitative Gait Feature Assessment on Two-Dimensional Body Axis Projection Planes Converted from Three-Dimensional Coordinates Estimated with a Deep Learning Smartphone App. Sensors 2023, 23, 617. [Google Scholar] [CrossRef] [PubMed]
- Iseki, C.; Hayasaka, T.; Yanagawa, H.; Komoriya, Y.; Kondo, T.; Hoshi, M.; Fukami, T.; Kobayashi, Y.; Ueda, S.; Kawamae, K.; et al. Artificial Intelligence Distinguishes Pathological Gait: The Analysis of Markerless Motion Capture Gait Data Acquired by an iOS Application (TDPT-GT). Sensors 2023, 23, 6217. [Google Scholar] [CrossRef] [PubMed]
- Clark, R.A.; Pua, Y.H.; Bryant, A.L.; Hunt, M.A. Validity of the Microsoft Kinect for providing lateral trunk lean feedback during gait retraining. Gait Posture 2013, 38, 1064–1066. [Google Scholar] [CrossRef] [PubMed]
- Macpherson, T.W.; Taylor, J.; McBain, T.; Weston, M.; Spears, I.R. Real-time measurement of pelvis and trunk kinematics during treadmill locomotion using a low-cost depth-sensing camera: A concurrent validity study. J. Biomech. 2016, 49, 474–478. [Google Scholar] [CrossRef] [PubMed]
- Merchant, R.A.; Banerji, S.; Singh, G.; Chew, E.; Poh, C.L.; Tapawan, S.C.; Guo, Y.R.; Pang, Y.W.; Sharma, M.; Kambadur, R.; et al. Is Trunk Posture in Walking a Better Marker than Gait Speed in Predicting Decline in Function and Subsequent Frailty? J. Am. Med. Dir. Assoc. 2016, 17, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Jehu, D.; Nantel, J. Fallers with Parkinson’s disease exhibit restrictive trunk control during walking. Gait Posture 2018, 65, 246–250. [Google Scholar] [CrossRef]
- Clark, R.A.; Mentiplay, B.F.; Pua, Y.-H.; Bower, K.J. Reliability and validity of the Wii Balance Board for assessment of standing balance: A systematic review. Gait Posture 2018, 61, 40–54. [Google Scholar] [CrossRef]
- Jeon, E.T.; Cho, H.Y. A Novel Method for Gait Analysis on Center of Pressure Excursion Based on a Pressure-Sensitive Mat. Int. J. Environ. Res. Public Health 2020, 17, 7845. [Google Scholar] [CrossRef]
- Granacher, U.; Gollhofer, A.; Hortobágyi, T.; Kressig, R.W.; Muehlbauer, T. The Importance of Trunk Muscle Strength for Balance, Functional Performance, and Fall Prevention in Seniors: A Systematic Review. Sports Med. 2013, 43, 627–641. [Google Scholar] [CrossRef] [PubMed]
- Ueda, N.; Hakii, Y.; Koyano, S.; Higashiyama, Y.; Joki, H.; Baba, Y.; Suzuki, Y.; Kuroiwa, Y.; Tanaka, F. Quantitative analysis of upper-limb ataxia in patients with spinocerebellar degeneration. J. Neurol. 2014, 261, 1381–1386. [Google Scholar] [CrossRef]
- Coghe, G.; Corona, F.; Pilloni, G.; Porta, M.; Frau, J.; Lorefice, L.; Fenu, G.; Cocco, E.; Pau, M. Is There Any Relationship between Upper and Lower Limb Impairments in People with Multiple Sclerosis? A Kinematic Quantitative Analysis. Mult. Scler. Int. 2019, 2019, 9149201. [Google Scholar] [CrossRef] [PubMed]
- Heremans, E.; Broeder, S.; Nieuwboer, A.; Bekkers, E.M.; Ginis, P.; Janssens, L.; Nackaerts, E. When motor control gets out of hand: Speeding up triggers freezing in the upper limb in Parkinson’s disease. Parkinsonism Relat. Disord. 2019, 64, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Bonnefoy-Mazure, A.; Sagawa, Y., Jr.; Lascombes, P.; De Coulon, G.; Armand, S. A descriptive analysis of the upper limb patterns during gait in individuals with cerebral palsy. Res. Dev. Disabil. 2014, 35, 2756–2765. [Google Scholar] [CrossRef] [PubMed]
- Elsworth-Edelsten, C.; Bonnefoy-Mazure, A.; Laidet, M.; Armand, S.; Assal, F.; Lalive, P.; Allali, G. Upper limb movement analysis during gait in multiple sclerosis patients. Hum. Mov. Sci. 2017, 54, 248–252. [Google Scholar] [CrossRef] [PubMed]
- Marmarou, A.; Bergsneider, M.; Relkin, N.; Klinge, P.; Black, P.M. Development of guidelines for idiopathic normal-pressure hydrocephalus: Introduction. Neurosurgery 2005, 57, S1–S3. [Google Scholar] [CrossRef] [PubMed]
- Stolze, H.; Kuhtz-Buschbeck, J.P.; Drucke, H.; Johnk, K.; Diercks, C.; Palmie, S.; Mehdorn, H.M.; Illert, M.; Deuschl, G. Gait analysis in idiopathic normal pressure hydrocephalus-which parameters respond to the CSF tap test? Clin. Neurophysiol. 2000, 111, 1678–1686. [Google Scholar] [CrossRef] [PubMed]
- Postuma, R.B.; Berg, D.; Stern, M.; Poewe, W.; Olanow, C.W.; Oertel, W.; Obeso, J.; Marek, K.; Litvan, I.; Lang, A.E.; et al. MDS clinical diagnostic criteria for Parkinson’s disease. Mov. Disord. 2015, 30, 1591–1601. [Google Scholar] [CrossRef]
- Peng, C.K.; Buldyrev, S.V.; Havlin, S.; Simons, M.; Stanley, H.E.; Goldberger, A.L. Mosaic organization of DNA nucleotides. Phys. Rev. E 1994, 49, 1685–1689. [Google Scholar] [CrossRef]
- Hausdorff, J.M.; Peng, C.K.; Ladin, Z.; Wei, J.Y.; Goldberger, A.L. Is walking a random walk? Evidence for long-range correlations in stride interval of human gait. J. Appl. Physiol. 1995, 78, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Goldberger, A.L.; Amaral, L.A.; Hausdorff, J.M.; Ivanov, P.C.; Peng, C.K.; Stanley, H.E. Fractal dynamics in physiology: Alterations with disease and aging. Proc. Natl. Acad. Sci. USA 2002, 99 (Suppl. S1), 2466–2472. [Google Scholar] [CrossRef] [PubMed]
- McIntosh, G.C.; Brown, S.H.; Rice, R.R.; Thaut, M.H. Rhythmic auditory-motor facilitation of gait patterns in patients with Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 1997, 62, 22–26. [Google Scholar] [CrossRef] [PubMed]
- Grosu, G.F.; Hopp, A.V.; Moca, V.V.; Barzan, H.; Ciuparu, A.; Ercsey-Ravasz, M.; Winkel, M.; Linde, H.; Muresan, R.C. The fractal brain: Scale-invariance in structure and dynamics. Cereb. Cortex 2023, 33, 4574–4605. [Google Scholar] [CrossRef] [PubMed]
- O’Donnell, L.J.; Westin, C.F. An introduction to diffusion tensor image analysis. Neurosurg. Clin. N. Am. 2011, 22, 185–196. [Google Scholar] [CrossRef] [PubMed]
- Nunez, P.L.; Srinivasan, R. Electric Fields of the Brain: The Neurophysics of EEG, 2nd ed.; Oxford University Press: Oxford, UK, 2006. [Google Scholar] [CrossRef]
- Uhlhaas, P.J.; Pipa, G.; Lima, B.; Melloni, L.; Neuenschwander, S.; Nikolic, D.; Singer, W. Neural synchrony in cortical networks: History, concept and current status. Front. Integr. Neurosci. 2009, 3, 17. [Google Scholar] [CrossRef] [PubMed]
- Pirici, D.; Mogoantă, L.; Mărgăritescu, O.; Pirici, I.; Tudorică, V.; Coconu, M. Fractal analysis of astrocytes in stroke and dementia. Rom. J. Morphol. Embryol. 2009, 50, 381–390. [Google Scholar]
- Gallagher, R.M.; Marquez, J.; Osmotherly, P. Cognitive and upper limb symptom changes from a tap test in Idiopathic Normal Pressure Hydrocephalus. Clin. Neurol. Neurosurg. 2018, 174, 92–96. [Google Scholar] [CrossRef]
- Sirkka, J.; Parviainen, M.; Jyrkkanen, H.K.; Koivisto, A.M.; Saisanen, L.; Rauramaa, T.; Leinonen, V.; Danner, N. Upper limb dysfunction and activities in daily living in idiopathic normal pressure hydrocephalus. Acta Neurochir. 2021, 163, 2675–2683. [Google Scholar] [CrossRef]
- Takakusaki, K. Functional Neuroanatomy for Posture and Gait Control. J. Mov. Disord. 2017, 10, 1–17. [Google Scholar] [CrossRef]
- Mikami, K.; Shiraishi, M.; Kamo, T. Subjective Vertical Position Allows Prediction of Postural Deterioration in Patients with Parkinson’s Disease. Parkinson’s Dis. 2019, 2019, 1875435. [Google Scholar] [CrossRef]
- Kaminishi, K.; Chiba, R.; Takakusaki, K.; Ota, J. Increase in muscle tone promotes the use of ankle strategies during perturbed stance. Gait Posture 2021, 90, 67–72. [Google Scholar] [CrossRef]
- Pickering, R.M.; Grimbergen, Y.A.; Rigney, U.; Ashburn, A.; Mazibrada, G.; Wood, B.; Gray, P.; Kerr, G.; Bloem, B.R. A meta-analysis of six prospective studies of falling in Parkinson’s disease. Mov. Disord. 2007, 22, 1892–1900. [Google Scholar] [CrossRef]
- Kwon, K.Y.; Lee, M.; Ju, H.; Im, K. Risk Factors for Falls in Patients with de novo Parkinson’s Disease: A Focus on Motor and Non-Motor Symptoms. J. Mov. Disord. 2020, 13, 142–145. [Google Scholar] [CrossRef]
- Thomas, J.C.; Odonkor, C.; Griffith, L.; Holt, N.; Percac-Lima, S.; Leveille, S.; Ni, P.; Latham, N.K.; Jette, A.M.; Bean, J.F. Reconceptualizing balance: Attributes associated with balance performance. Exp. Gerontol. 2014, 57, 218–223. [Google Scholar] [CrossRef]
- Weiss, A.; Brozgol, M.; Dorfman, M.; Herman, T.; Shema, S.; Giladi, N.; Hausdorff, J.M. Does the evaluation of gait quality during daily life provide insight into fall risk? A novel approach using 3-day accelerometer recordings. Neurorehabilit. Neural Repair 2013, 27, 742–752. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| iNPH | PD | Control | |
|---|---|---|---|
| Number | 23 | 23 | 92 |
| Sex (male/female) | 16/7 | 13/10 | 36/56 |
| Number of gait trials | 117 | 56 | 184 |
| Age (average ± SD) | 77.0 ± 6.4 | 70.1 ± 6.0 | 72.3 ± 6.3 |
| Controls | PD | iNPH | p | |||
|---|---|---|---|---|---|---|
| Upper body | Trunk | R. ear | −2.15 | −2.07 | −1.99 | 0.101 |
| Head | −2.15 | −1.99 | −1.89 | 0.036 * | ||
| L. ear | −2.15 | −1.98 | −1.89 | 0.044 * | ||
| R. eye | −2.15 | −1.98 | −1.90 | 0.094 | ||
| L. eye | −2.15 | −1.98 | −1.90 | 0.089 | ||
| R. shoulder | −2.15 | −1.98 | −1.90 | 0.044 * | ||
| Neck | −2.16 | −2.00 | −1.91 | 0.059 | ||
| L. shoulder | −2.16 | −2.00 | −1.90 | 0.024 * | ||
| Nose | −2.16 | −1.99 | −1.91 | 0.118 | ||
| Limbs | R. elbow | −2.25 | −2.07 | −1.99 | 0.196 | |
| L. elbow | −2.26 | −2.06 | −1.97 | 0.102 | ||
| R. middle finger | −2.31 | −2.15 | −2.02 | 0.035 * | ||
| R. wrist | −2.31 | −2.14 | −2.02 | 0.049 * | ||
| R. thumb | −2.33 | −2.16 | −2.04 | 0.045 * | ||
| L. middle finger | −2.33 | −2.10 | −2.04 | 0.408 | ||
| L. thumb | −2.35 | −2.12 | −2.06 | 0.494 | ||
| L. wrist | −2.35 | −2.11 | −2.04 | 0.272 | ||
| Lower body | Trunk | L. knee | −2.20 | −2.04 | −1.92 | 0.023 * |
| R. hip joint | −2.20 | −2.05 | −1.94 | 0.019 * | ||
| L. hip joint | −2.21 | −2.04 | −1.95 | 0.093 | ||
| R. knee | −2.21 | −2.03 | −1.91 | 0.015 * | ||
| Buttocks | −2.21 | −2.06 | −1.95 | 0.019 * | ||
| Limbs | L. toe | −2.28 | −2.05 | −1.92 | 0.038 * | |
| R. toe | −2.29 | −2.06 | −1.92 | 0.012 * | ||
| L. ankle | −2.32 | −2.09 | −1.95 | 0.018 * | ||
| R. ankle | −2.35 | −2.10 | −1.96 | 0.015 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iseki, C.; Suzuki, S.; Fukami, T.; Yamada, S.; Hayasaka, T.; Kondo, T.; Hoshi, M.; Ueda, S.; Kobayashi, Y.; Ishikawa, M.; et al. Fluctuations in Upper and Lower Body Movement during Walking in Normal Pressure Hydrocephalus and Parkinson’s Disease Assessed by Motion Capture with a Smartphone Application, TDPT-GT. Sensors 2023, 23, 9263. https://doi.org/10.3390/s23229263
Iseki C, Suzuki S, Fukami T, Yamada S, Hayasaka T, Kondo T, Hoshi M, Ueda S, Kobayashi Y, Ishikawa M, et al. Fluctuations in Upper and Lower Body Movement during Walking in Normal Pressure Hydrocephalus and Parkinson’s Disease Assessed by Motion Capture with a Smartphone Application, TDPT-GT. Sensors. 2023; 23(22):9263. https://doi.org/10.3390/s23229263
Chicago/Turabian StyleIseki, Chifumi, Shou Suzuki, Tadanori Fukami, Shigeki Yamada, Tatsuya Hayasaka, Toshiyuki Kondo, Masayuki Hoshi, Shigeo Ueda, Yoshiyuki Kobayashi, Masatsune Ishikawa, and et al. 2023. "Fluctuations in Upper and Lower Body Movement during Walking in Normal Pressure Hydrocephalus and Parkinson’s Disease Assessed by Motion Capture with a Smartphone Application, TDPT-GT" Sensors 23, no. 22: 9263. https://doi.org/10.3390/s23229263
APA StyleIseki, C., Suzuki, S., Fukami, T., Yamada, S., Hayasaka, T., Kondo, T., Hoshi, M., Ueda, S., Kobayashi, Y., Ishikawa, M., Kanno, S., Suzuki, K., Aoyagi, Y., & Ohta, Y. (2023). Fluctuations in Upper and Lower Body Movement during Walking in Normal Pressure Hydrocephalus and Parkinson’s Disease Assessed by Motion Capture with a Smartphone Application, TDPT-GT. Sensors, 23(22), 9263. https://doi.org/10.3390/s23229263