

Ultra-Wideband Radar for Simultaneous and Unobtrusive Monitoring of Respiratory and Heart Rates in Early Childhood: A Deep Transfer Learning Approach

 , , , ,
, , , , 
Abstract
:1. Introduction
2. Latest Literature Survey
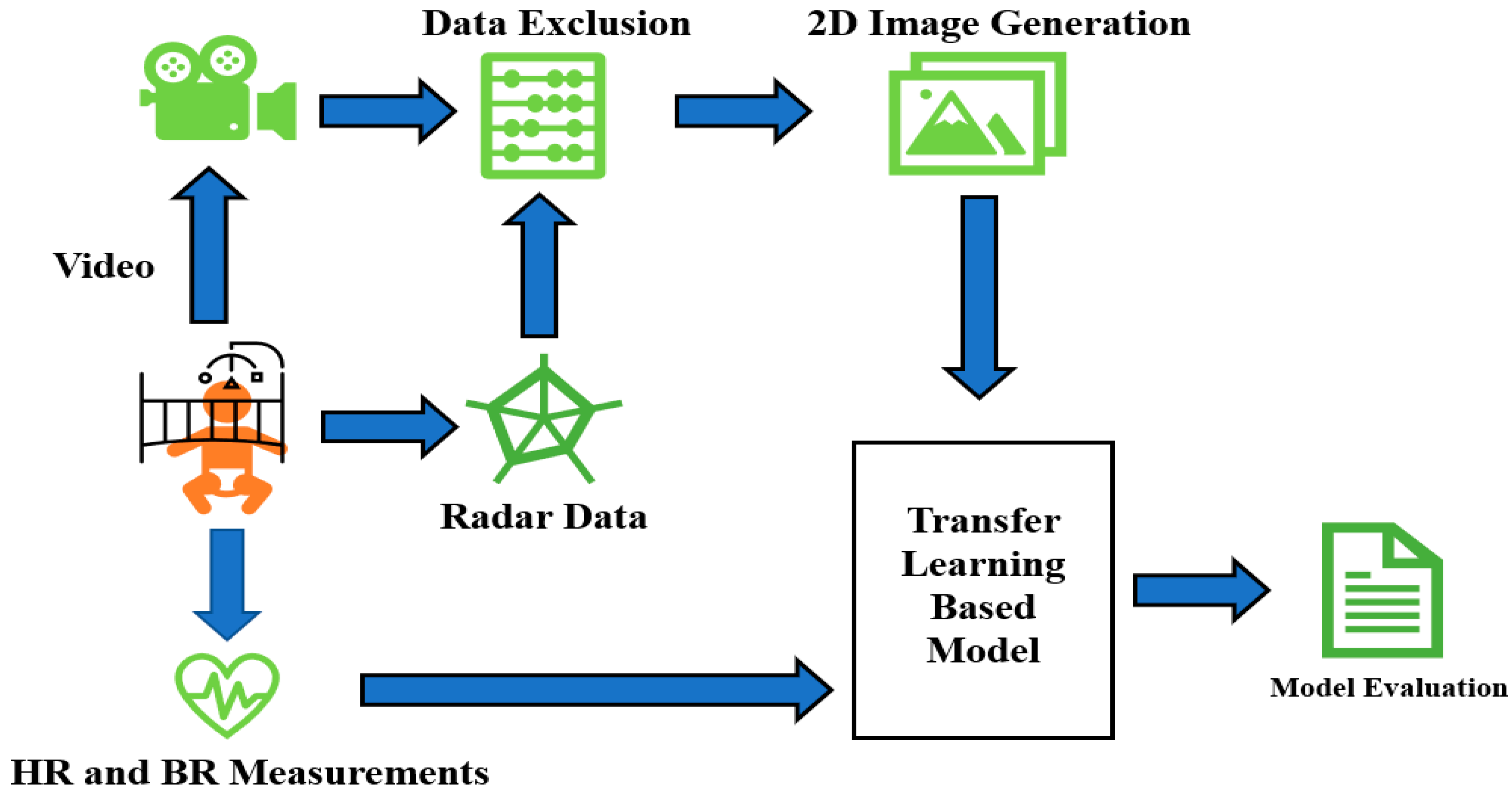
3. Materials and Method
3.1. Study Population
3.2. Radar Data Acquisition
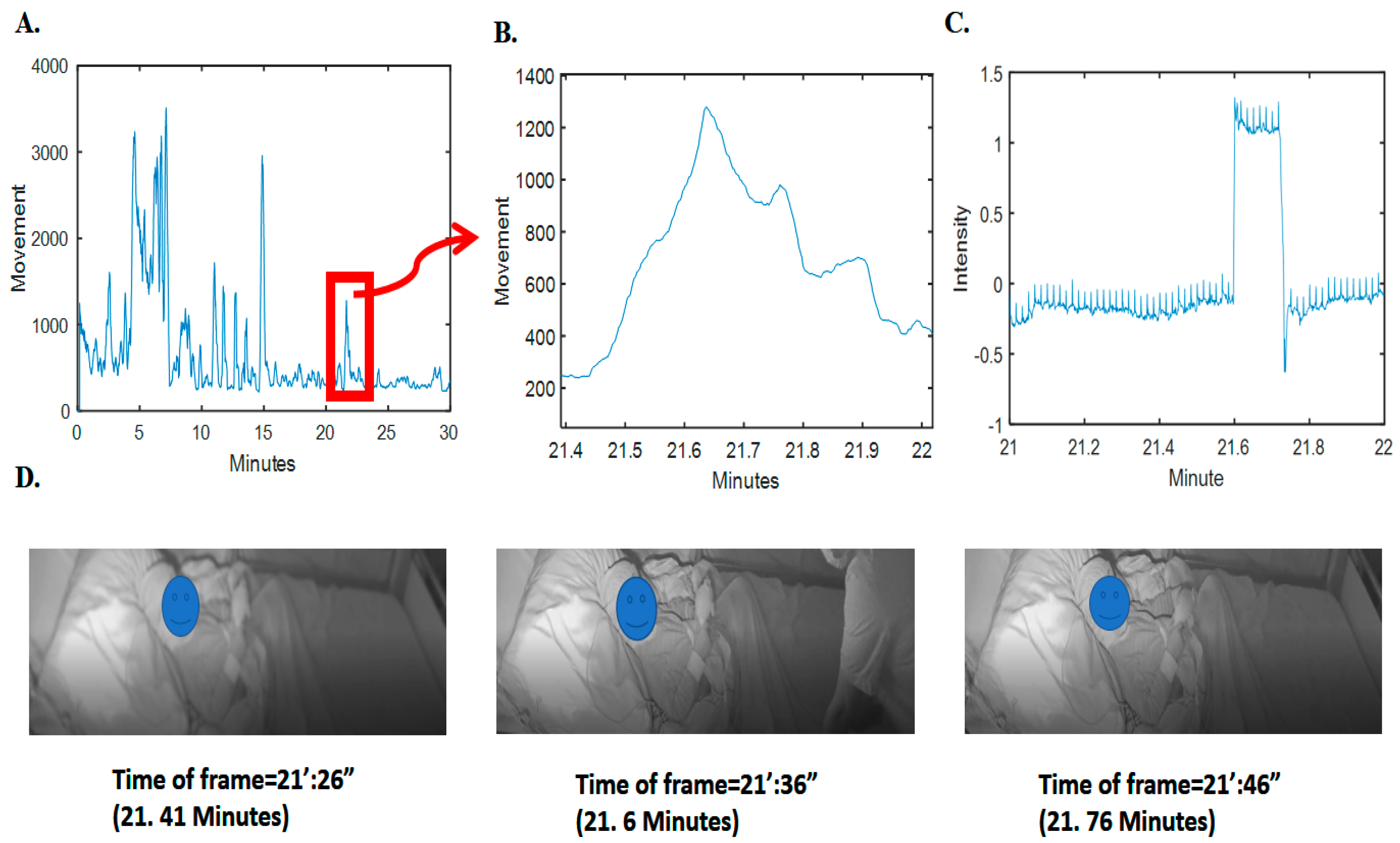
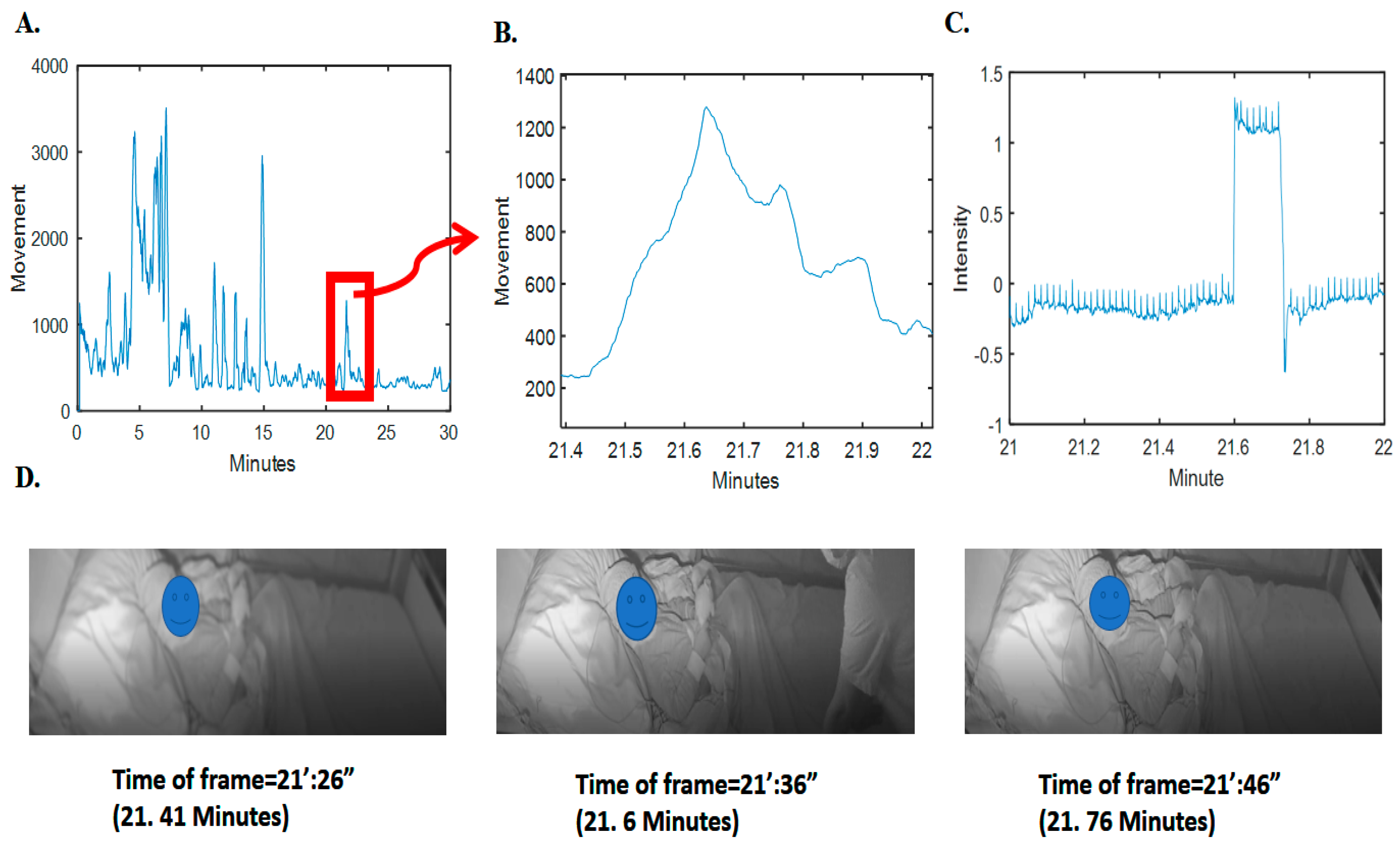
3.3. Data Inclusion
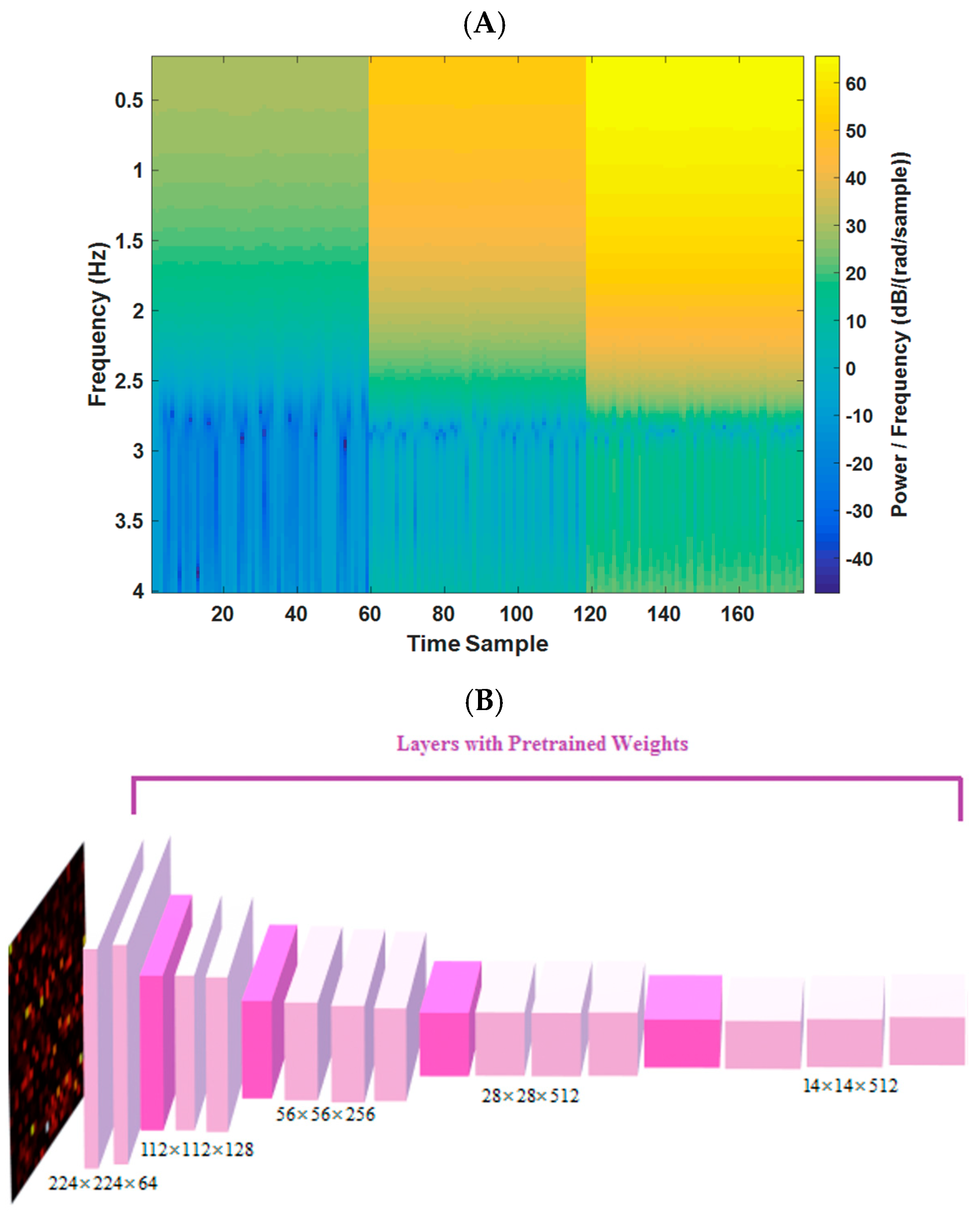
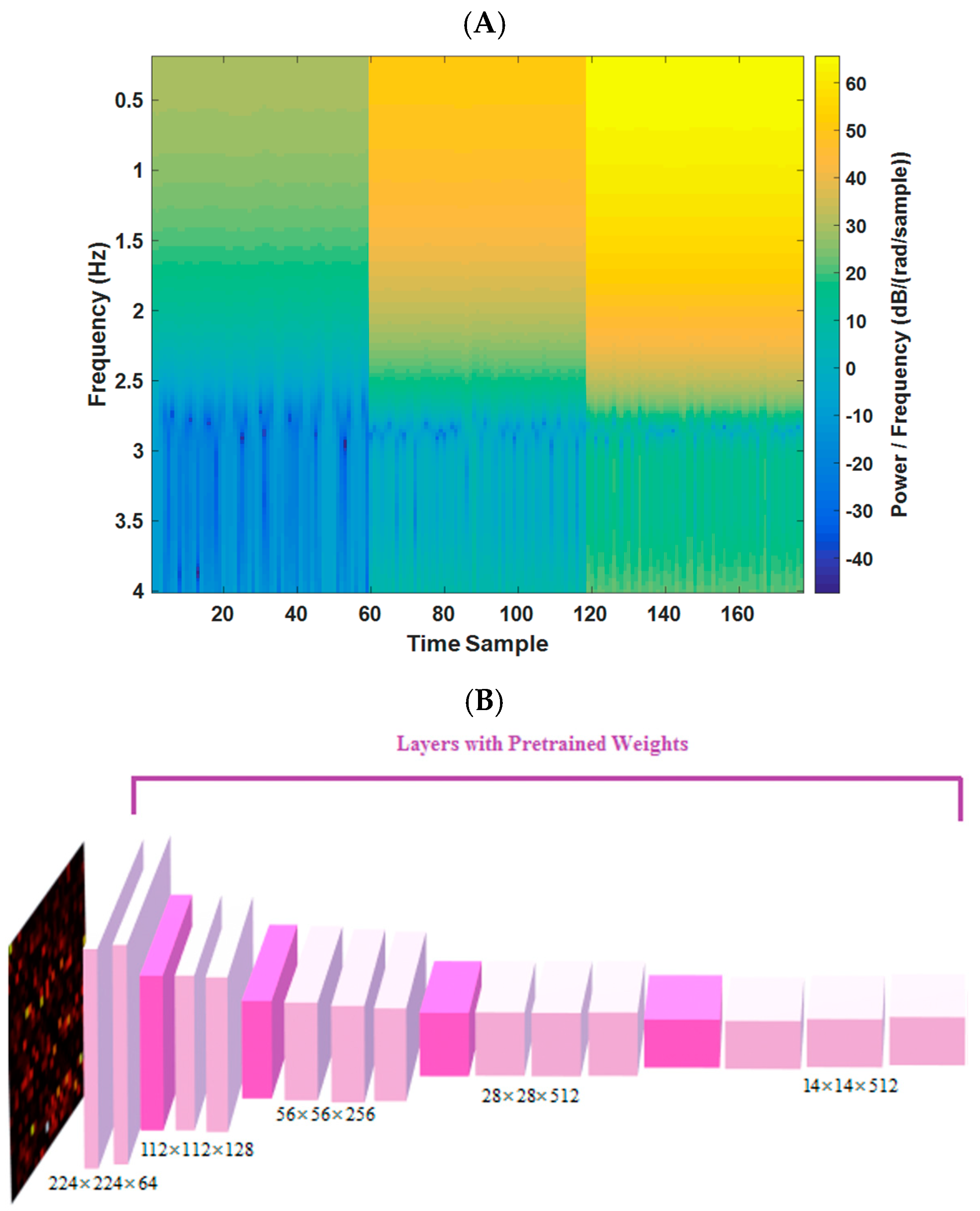
3.4. Pre-Processing and 2D Image Generation from Radar Data
3.5. Transfer Learning and Model Definition
- (A)
- adding 2D convolutional layer ((filter width × filter height) × number of neurons) of ((3 × 3)× 16) and a max-pooling layer (filter width × filter height)× of (3 × 3).
- (B)
- developing a fully connected layer (width × height × depth) of (1 × 1 × 8) with the activation function of “Relu” and another one with (1 × 1 × 4) with the activation function of “Relu”.
- (C)
- applying the fully connected layer (1 × 1 × 1) with the activation function of the “linear” type for the regression task for each branch of HR/RR estimation.
- (D)
- model compiled (for Keras model in Python) by Adam optimizer (learning rate = 0.005 and decay = 0.001).
- (E)
- loss function is mean square error and the batch size is 32.
- (F)
- for the fine-tuning, we only updated the last 5 convolutional layers’ weights (mentioned in A and B).
3.6. Model Evaluation Strategies and Statistics
4. Results
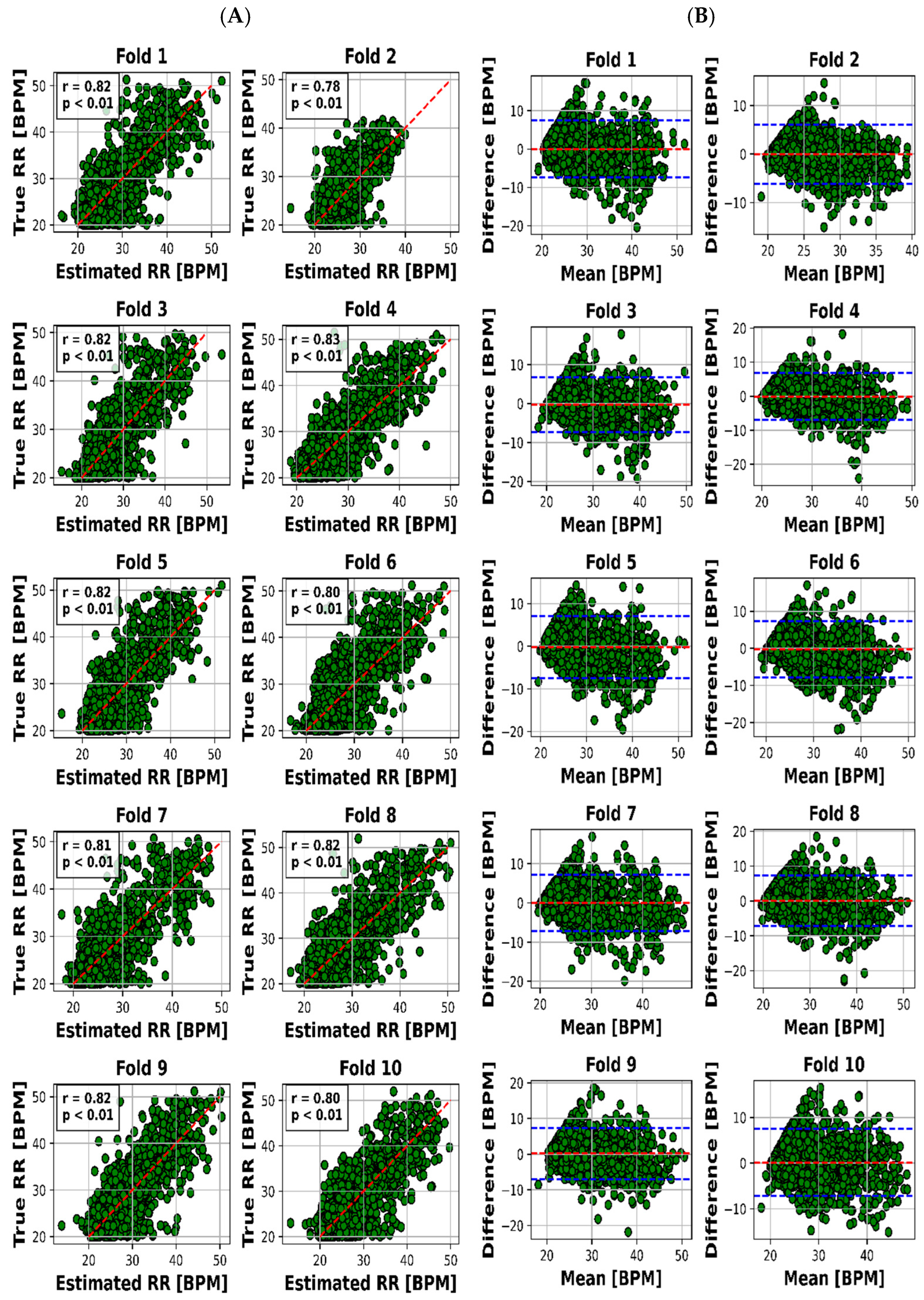
4.1. Analysis of the Results
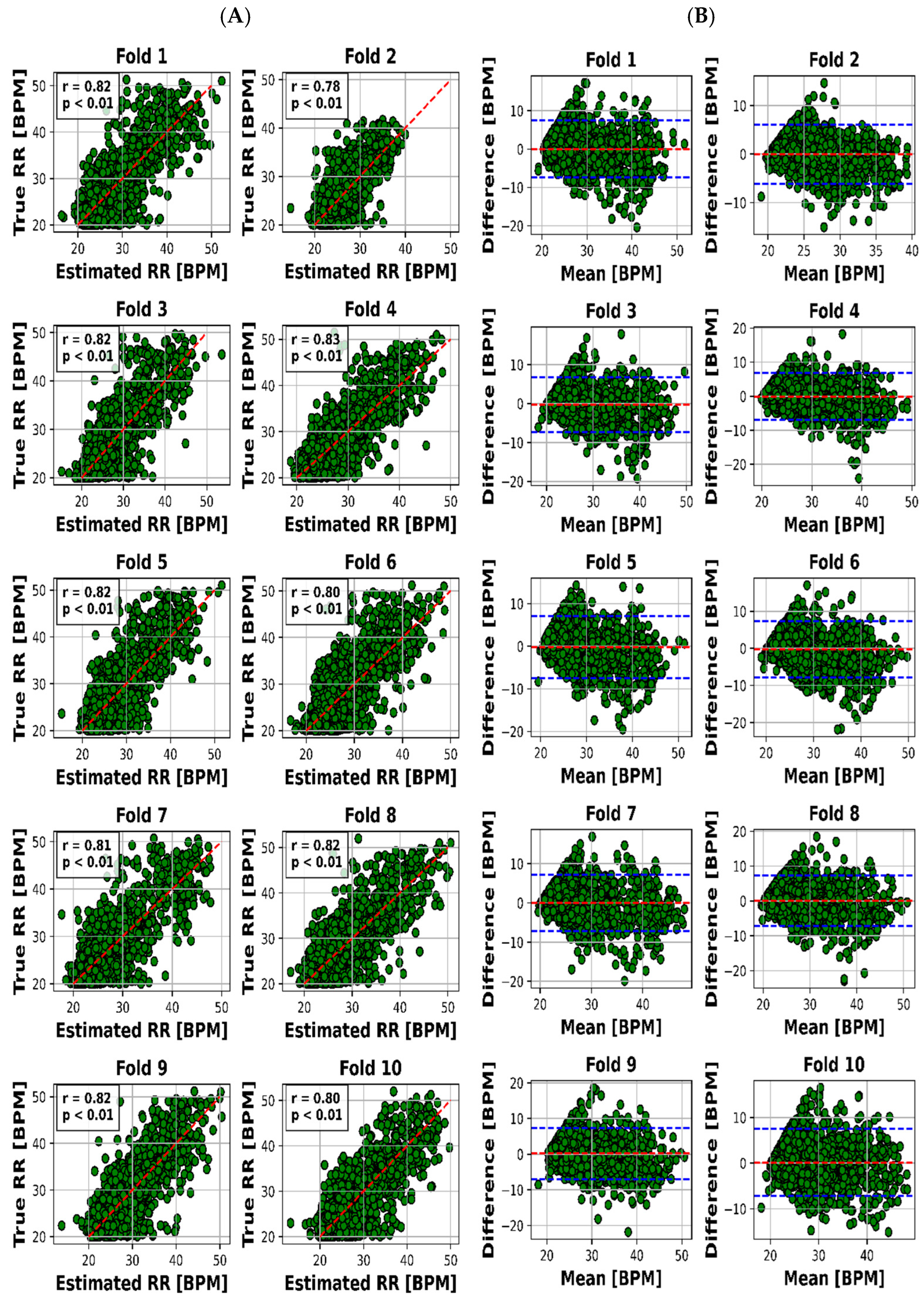
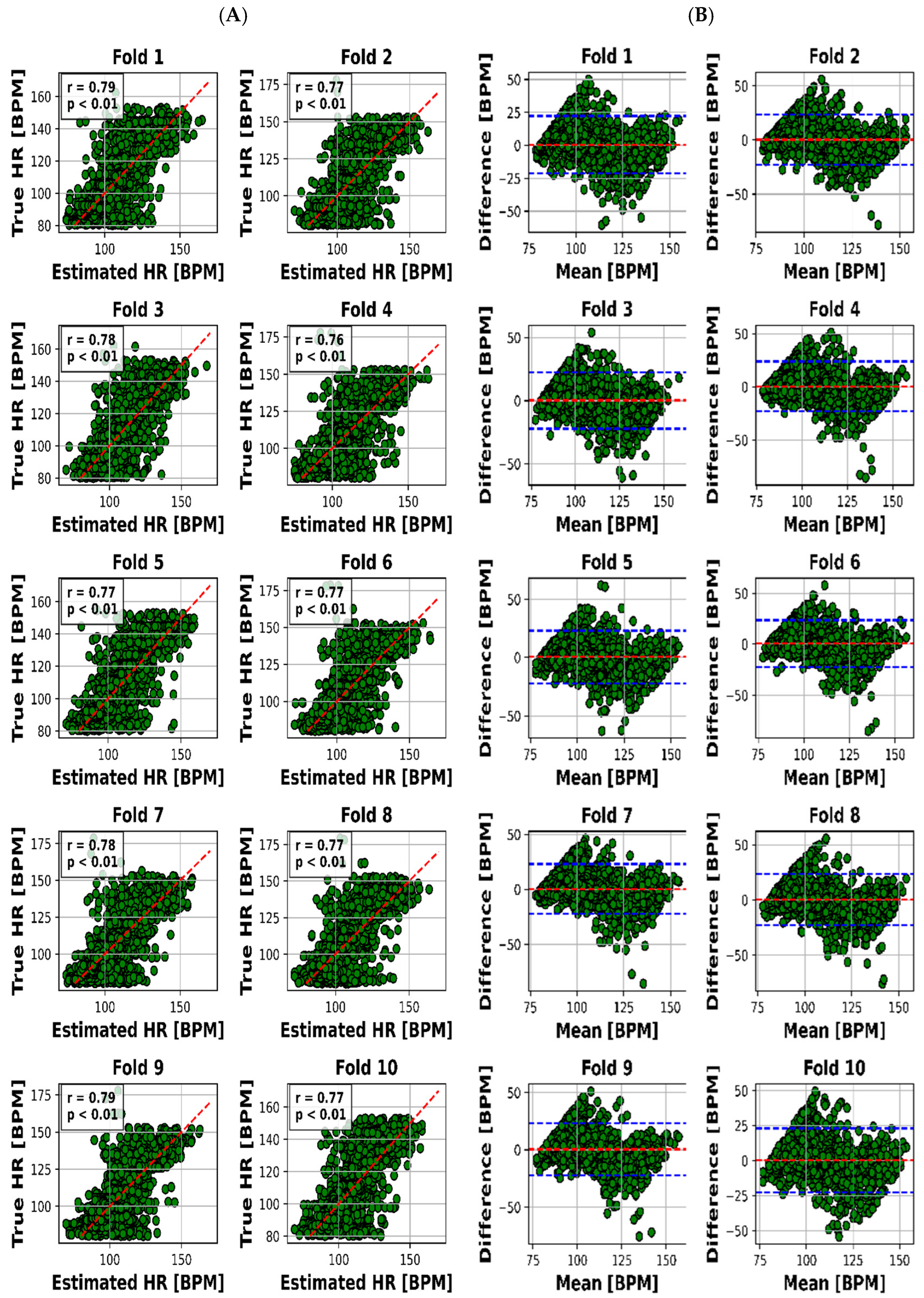
4.1.1. Visual Representation: Insights through Visuals
4.1.2. Quantitative Summary: Key Metrics at a Glance
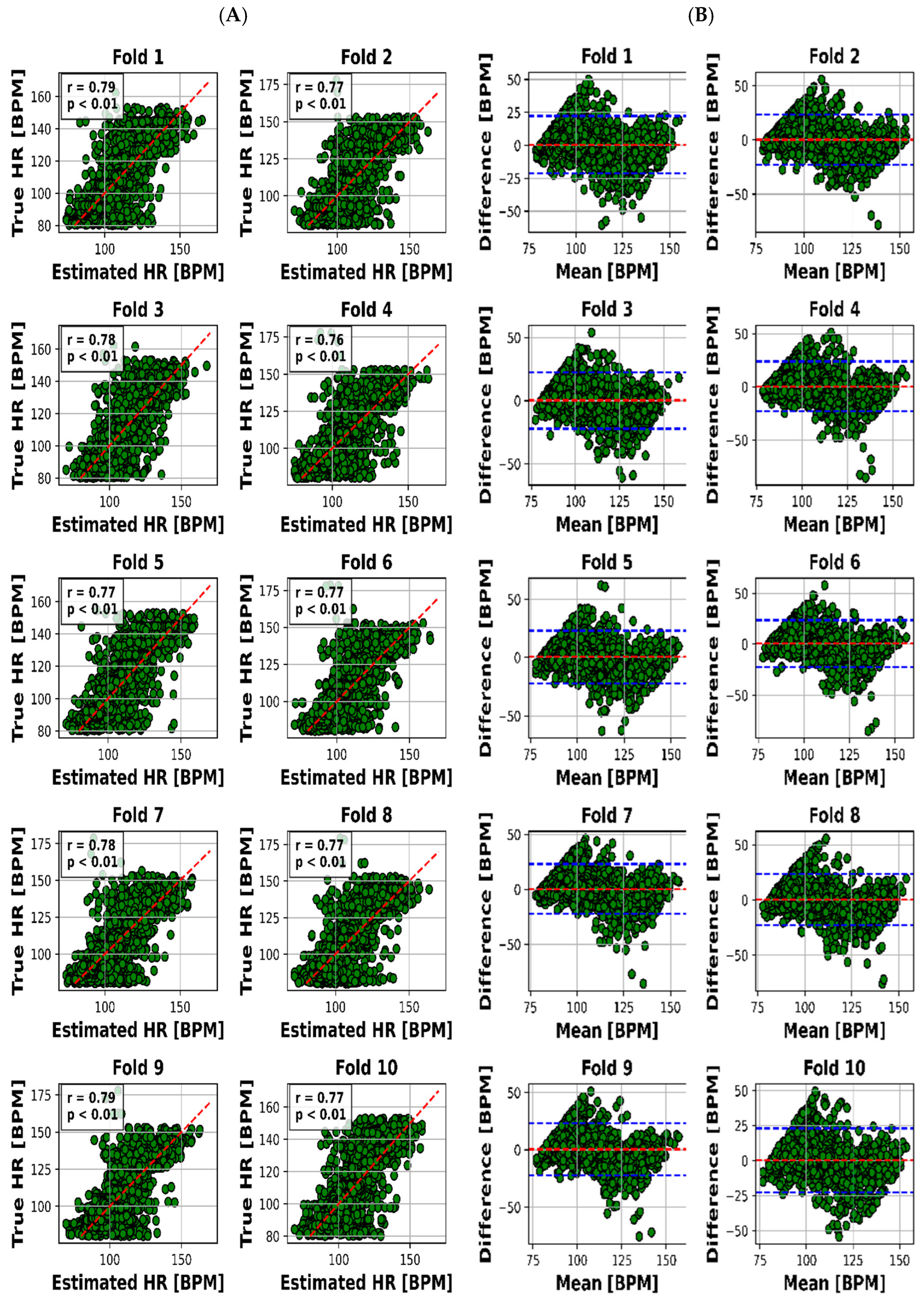
4.1.3. Robust Dependencies: Pearson’s Correlation Coefficients
4.1.4. Addressing Systematic Errors: Mean Biases Examination
4.1.5. Limits of Agreement: Gauging Practical Reliability
4.1.6. Methodology: Integrating Data for Model Performance
5. Discussion
5.1. Limitations
5.2. Future Perspectives
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Maurya, L.; Kaur, P.; Chawla, D.; Mahapatra, P. Non-contact breathing rate monitoring in newborns: A review. Comput. Biol. Med. 2021, 132, 104321. [Google Scholar] [CrossRef] [PubMed]
- Serra, A.; Cocuzza, S.; Maiolino, L.; Abramo, A.; Spinato, G.; Tonoli, G.; Amadori, M.; Politi, D.; Tirelli, G.; Spinato, R. The watch-pat in pediatrics sleep disordered breathing: Pilot study on children with negative nocturnal pulse oximetry. Int. J. Pediatr. Otorhinolaryngol. 2017, 97, 245–250. [Google Scholar] [CrossRef] [PubMed]
- Aarts, L.A.; Jeanne, V.; Cleary, J.P.; Lieber, C.; Nelson, J.S.; Oetomo, S.B.; Verkruysse, W. Non-contact heart rate monitoring utilizing camera photoplethysmography in the neonatal intensive care unit—A pilot study. Early Hum. Dev. 2013, 89, 943–948. [Google Scholar] [CrossRef] [PubMed]
- Abbas, A.K.; Heimann, K.; Jergus, K.; Orlikowsky, T.; Leonhardt, S. Neonatal non-contact respiratory monitoring based on real-time infrared thermography. Biomed. Eng. Online 2011, 10, 93. [Google Scholar] [CrossRef]
- Villarroel, M.; Guazzi, A.; Jorge, J.; Davis, S.; Watkinson, P.; Green, G.; Shenvi, A.; McCormick, K.; Tarassenko, L. Continuous non-contact vital sign monitoring in neonatal intensive care unit. Healthc. Technol. Lett. 2014, 1, 87–91. [Google Scholar] [CrossRef]
- Faragli, A.; Abawi, D.; Quinn, C.; Cvetkovic, M.; Schlabs, T.; Tahirovic, E.; Düngen, H.-D.; Pieske, B.; Kelle, S.; Edelmann, F. The role of non-invasive devices for the telemonitoring of heart failure patients. Heart Fail. Rev. 2021, 26, 1063–1080. [Google Scholar] [CrossRef]
- O’Neill, R.; Dempsey, E.M.; Garvey, A.A.; Schwarz, C.E. Non-invasive cardiac output monitoring in neonates. Front. Pediatr. 2021, 8, 614585. [Google Scholar] [CrossRef]
- Chan, K.C.-C.; Au, C.T.; Hui, L.L.; Wing, Y.K.; Li, A.M. Childhood OSA is an independent determinant of blood pressure in adulthood: Longitudinal follow-up study. Thorax 2020, 75, 422–431. [Google Scholar] [CrossRef]
- Paulson, C.N.; Chang, J.T.; Romero, C.E.; Watson, J.; Pearce, F.J.; Levin, N. Ultra-wideband radar methods and techniques of medical sensing and imaging. In Proceedings of the Smart Medical and Biomedical Sensor Technology III, Boston, MA, USA, 24–26 October 2005; pp. 96–107. [Google Scholar]
- Hu, X.; Jin, T. Short-range vital signs sensing based on EEMD and CWT using IR-UWB radar. Sensors 2016, 16, 2025. [Google Scholar] [CrossRef]
- Lauteslager, T.; Maslik, M.; Siddiqui, F.; Marfani, S.; Leschziner, G.D.; Williams, A.J. Validation of a new contactless and continuous respiratory rate monitoring device based on ultra-wideband radar technology. Sensors 2021, 21, 4027. [Google Scholar] [CrossRef]
- Wang, P.; Ma, Y.; Liang, F.; Zhang, Y.; Yu, X.; Li, Z.; An, Q.; Lv, H.; Wang, J. Non-contact vital signs monitoring of dog and cat using a UWB radar. Animals 2020, 10, 205. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Yang, X.; Ding, Y.; Wang, Y.; Zhou, J.; Zhang, L. Contactless simultaneous breathing and heart rate detections in physical activity using ir-uwb radars. Sensors 2021, 21, 5503. [Google Scholar] [CrossRef]
- Liang, X.; Deng, J.; Zhang, H.; Gulliver, T.A. Ultra-wideband impulse radar through-wall detection of vital signs. Sci. Rep. 2018, 8, 13367. [Google Scholar] [CrossRef] [PubMed]
- Arasteh, E.; de Groot, E.R.; Van den Ende, D.; Alderliesten, T.; Long, X.; de Goederen, R.; Benders, M.; Dudink, J. Unobtrusive Cot Side Sleep Stage Classification in Preterm Infants Using Ultra-Wideband Radar. Front. Sleep 2023, 2, 1150962. [Google Scholar] [CrossRef]
- Siriwardhana, L.S.; Yee, A.K.; Mann, D.L.; Dawadi, S.; Nixon, G.M.; Wong, F.Y.; Edwards, B.A.; Horne, R.S. Ventilatory control instability as a predictor of persistent periodic breathing in preterm infants. Pediatr. Res. 2022, 92, 513–519. [Google Scholar] [CrossRef]
- Sundermeyer, M.; Schlüter, R.; Ney, H. LSTM neural networks for language modeling. In Proceedings of the Thirteenth Annual Conference of the International Speech Communication Association, Portland, ON, USA, 9–13 September 2012. [Google Scholar]
- Pappy, G.A.; Aczon, M.D.; Wetzel, R.C.; Ledbetter, D.R. Predicting High-Flow Nasal Cannula Failure in an ICU Using a Recurrent Neural Network with Transfer Learning and Input Data Perseveration: A Retrospective Analysis. arXiv 2021, arXiv:2111.11846. [Google Scholar]
- Tan, C.; Sun, F.; Kong, T.; Zhang, W.; Yang, C.; Liu, C. A survey on deep transfer learning. In Proceedings of the Artificial Neural Networks and Machine Learning–ICANN 2018: 27th International Conference on Artificial Neural Networks, Rhodes, Greece, 4–7 October 2018; Proceedings, Part III 27. pp. 270–279. [Google Scholar]
- Al-Naji, A.; Gibson, K.; Lee, S.-H.; Chahl, J. Real time apnoea monitoring of children using the Microsoft Kinect sensor: A pilot study. Sensors 2017, 17, 286. [Google Scholar] [CrossRef]
- Al-Naji, A.; Perera, A.G.; Chahl, J. Remote monitoring of cardiorespiratory signals from a hovering unmanned aerial vehicle. Biomed. Eng. Online 2017, 16, 1–20. [Google Scholar] [CrossRef]
- Simonyan, K.; Zisserman, A. Very deep convolutional networks for large-scale image recognition. arXiv 2014, arXiv:1409.1556. [Google Scholar]
- Arasteh, E.; Mahdizadeh, A.; Mirian, M.S.; Lee, S.; McKeown, M.J. Deep transfer learning for parkinson’s disease monitoring by image-based representation of resting-state EEG using directional connectivity. Algorithms 2022, 15, 5. [Google Scholar] [CrossRef]
- Hsu, G.-S.J.; Xie, R.-C.; Ambikapathi, A.; Chou, K.-J. A deep learning framework for heart rate estimation from facial videos. Neurocomputing 2020, 417, 155–166. [Google Scholar] [CrossRef]
- Wu, S.; Sakamoto, T.; Oishi, K.; Sato, T.; Inoue, K.; Fukuda, T.; Mizutani, K.; Sakai, H. Person-specific heart rate estimation with ultra-wideband radar using convolutional neural networks. IEEE Access 2019, 7, 168484–168494. [Google Scholar] [CrossRef]
- Han-Trong, T.; Nguyen Viet, H. An Efficient Heart Rate Measurement System Using Medical Radar and LSTM Neural Network. J. Electr. Comput. Eng. 2022, 2022, 4696163. [Google Scholar] [CrossRef]
- Ennett, C.M.; Frize, M. Investigation into the strengths and limitations of artificial neural networks: An application to an adult ICU patient database. In Proceedings of the AMIA Symposium 1998, Lake Buena Vista, FL, USA, 7–11 November 1998; p. 998. [Google Scholar]
- Katoh, M.; Kanazawa, T.; Abe, Y.; Sun, G.; Matsui, T. Development of a non-contact 15-s paediatric respiratory rate monitor using microwave radar and its clinical application. Acta Paediatr. 2023, 112, 493–495. [Google Scholar] [CrossRef] [PubMed]
- Zhao, P.; Lu, C.X.; Wang, B.; Chen, C.; Xie, L.; Wang, M.; Trigoni, N.; Markham, A. Heart rate sensing with a robot mounted mmwave radar. Proceedings of 2020 IEEE International Conference on Robotics and Automation (ICRA), Paris, France, 31 May–31 August 2020; pp. 2812–2818. [Google Scholar]
- Jung, D.; Cheon, S.; Kim, D.; Yoon, J.; Kim, B. Short Time Remote Heart Rate Measurement based on mmWave FMCW Radar Frame Structure. IEEE Antennas Wirel. Propag. Lett. 2023, 22, 1301–1305. [Google Scholar] [CrossRef]
- Shi, Q.; Hu, B.; Tian, F.; Zhao, Q. Noncontact Doppler Radar-based Heart Rate Detection on the SVD and ANC. In Proceedings of the 2022 IEEE International Conference on Bioinformatics and Biomedicine (BIBM), Las Vegas, NV, USA, 6–8 December 2022; pp. 1710–1713. [Google Scholar]
- Bhagat Bhagyashri, B.; Bazil Raj, A.A. Detection of human presence using UWB radar. In Proceedings of the 2021 International Conference on System, Computation, Automation and Networking (ICSCAN), Puducherry, India, 30–31 July 2021. [Google Scholar]
- de Goederen, R.; Pu, S.; Viu, M.S.; Doan, D.; Overeem, S.; Serdijn, W.A.; Joosten, K.F.; Long, X.; Dudink, J. Radar-based sleep stage classification in children undergoing polysomnography: A pilot-study. Sleep Med. 2021, 82, 1–8. [Google Scholar] [CrossRef]
- Massagram, W.; Lubecke, V.M.; HØst-Madsen, A.; Boric-Lubecke, O. Assessment of heart rate variability and respiratory sinus arrhythmia via Doppler radar. IEEE Trans. Microw. Theory Tech. 2009, 57, 2542–2549. [Google Scholar] [CrossRef]
- Yoo, S.; Ahmed, S.; Kang, S.; Hwang, D.; Lee, J.; Son, J.; Cho, S.H. Radar recorded child vital sign public dataset and deep learning-based age group classification framework for vehicular application. Sensors 2021, 21, 2412. [Google Scholar] [CrossRef]
- Kim, J.D.; Lee, W.H.; Lee, Y.; Lee, H.J.; Cha, T.; Kim, S.H.; Song, K.-M.; Lim, Y.-H.; Cho, S.H.; Cho, S.H. Non-contact respiration monitoring using impulse radio ultrawideband radar in neonates. R. Soc. Open Sci. 2019, 6, 190149. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Outputs | Outcomes | Limitations |
|---|---|---|---|
| Wu et al. [25] | Individualized skin displacement for HR estimation | Estimation of HR using skin displacement | Movement-sensitive; limited to certain states of subjects |
| Han-Trong et al. [26] | HR estimation through LSTM network. Incorporates Eclipse Fit method for motion and distortion correction. Incorporates spectrogram analysis for enhanced accuracy | Improved HR estimation via deep transfer learning and incorporation of spectrogram analysis | Motion correction degrades in high noise; vanishing gradients limit generalizability and reliability |
| Katoh et al. [28] | Respiratory waveform and HR in 15 s intervals captured via radar. Effective use of “Alternate Distinguishing Inhalation from Exhalation” algorithm | Non-contact measurement of RR and HR in pediatriccare; accurate estimation of RR and HR | Susceptible to motion artifacts during measurements; requires careful consideration |
| Zhao et al. [29] | Heart rate changes tracked based on daily activity poses and movements. Incorporates mmWave radar on robot | Heart rate variations monitored through neural network weight updates; applicability in hospital and home environments | Demands substantial training dataset; infeasible for hospitals and home monitoring |
| Jung et al. [30] | Remote heart rate measurement using frame structure of FMCW radar systems | Improved heart rate measurement resolution within short timeframe; potential limitations in dynamic scenarios | Assumes minimal movement for stable phase changes; trade-off between accuracy and computational complexity |
| Shi et al. [31] | Heartbeat information extracted from weak thoracic mechanical motion via Doppler-radar-based applications | Detection and variability of heart rate through Doppler-radar-based methods; potential for non-contact vital sign measurement | Sliding window introduces time delay; not tested in pediatric data; may lack efficiency in scenarios with high delay; demands |
| N | 55 |
|---|---|
| Mean age (range) | 6.1 year (10 day–18 year) |
| <1 year, N (%) | 18 (33) |
| 1–12 year, N (%) | 29 (53) |
| >12 year, N (%) | 8 (15) |
| Male gender (%) | 32 (58) |
| Mean birth weight in kg (range) | 3.1 (1.1–4.3) |
| Apgar (appearance, pulse, grimace, activity, and respiration) score 1/5/10 min (N at 1 min/N at 5 min/N at 10 min) | 7.8/8.9/8.9 (21/22/9) |
| Medication 24 h before or during observation, N (%) | 39 (71) |
| Caffeine | 1 |
| Doxapram | 0 |
| Hydrocortison (systemic) | 1 |
| Syndromes/diagnosis | |
| Spinal muscular atrophy type II | 1 |
| Central nervous system | 7 |
| Spina bifida aperta with Chiari malformation | 2 |
| Epilepsy | 2 |
| West syndrome | 1 |
| Joubert syndrome | 1 |
| Hydrocephalus | 1 |
| Skeletal abnormalities | 15 |
| Achondroplasia | 12 |
| Brachycephalia | 1 |
| Craniosynostoses | 1 |
| Arthrogryposis multiplex congenita | 1 |
| Upper airway abnormalities | 17 |
| Pierre Robin sequence | 4 |
| Palatoschisis | 3 |
| Laryngomalacia | 2 |
| Cheilognathopalatoschisis | 2 |
| Treacher Collins hypoplastic mandible | 1 |
| Midline facial cleft | 1 |
| Bifide uvula | 1 |
| Bronchomalacia | 1 |
| Tracheobronchomalacia | 1 |
| Laryngobronchomalacia | 1 |
| Other syndromes | 10 |
| Down syndrome | 3 |
| 22q11.2 deletion syndrome | 2 |
| ROHHADNET (Rapid onset Obesity, Hypothalamic dysfunction, Hypoventilation, Autonomic Dysregulation and Neuroendocrine Tumor) syndrome | 1 |
| Carey Fineman Ziter syndrome | 1 |
| Kabuki syndrome | 1 |
| Leri Weill syndrome | 1 |
| Coffin Siris syndrome | 1 |
| Premature/dysmature | 9 |
| No syndrome/unknown | 13 |
| Fold No. | MAE for RR (BPM) | MAE for RR (BPM) | Corr for RR | Corr for HR | Mean Bias for RR (BPM) | Mean Bias for HR (BPM) | LOA for RR (BPM) | LOA for HR (BPM) |
|---|---|---|---|---|---|---|---|---|
| 1 | 2.65 | 7.81 | 0.82 | 0.79 | 0.02 | 0.55 | 7.40 | 21.8 |
| 2 | 2.28 | 8.23 | 0.78 | 0.77 | −0.04 | 0.30 | 6.03 | 23.4 |
| 3 | 2.55 | 7.94 | 0.82 | 0.78 | −0.26 | 0.21 | 7.00 | 22.3 |
| 4 | 2.54 | 8.19 | 0.83 | 0.76 | −0.06 | 0.52 | 6.93 | 23.4 |
| 5 | 2.72 | 8.04 | 0.81 | 0.77 | −0.20 | 0.46 | 7.30 | 22.5 |
| 6 | 2.79 | 8.00 | 0.79 | 0.77 | −0.24 | 0.54 | 7.65 | 22.8 |
| 7 | 2.61 | 8.05 | 0.80 | 0.78 | −0.04 | 0.32 | 7.20 | 22.5 |
| 8 | 2.65 | 8.09 | 0.82 | 0.77 | 0.08 | 0.48 | 7.24 | 23.0 |
| 9 | 2.63 | 8.02 | 0.82 | 0.79 | 0.18 | 0.55 | 7.17 | 22.6 |
| 10 | 2.73 | 8.07 | 0.80 | 0.77 | 0.14 | 0.24 | 7.34 | 22.87 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arasteh, E.; Veldhoen, E.S.; Long, X.; van Poppel, M.; van der Linden, M.; Alderliesten, T.; Nijman, J.; de Goederen, R.; Dudink, J. Ultra-Wideband Radar for Simultaneous and Unobtrusive Monitoring of Respiratory and Heart Rates in Early Childhood: A Deep Transfer Learning Approach. Sensors 2023, 23, 7665. https://doi.org/10.3390/s23187665
Arasteh E, Veldhoen ES, Long X, van Poppel M, van der Linden M, Alderliesten T, Nijman J, de Goederen R, Dudink J. Ultra-Wideband Radar for Simultaneous and Unobtrusive Monitoring of Respiratory and Heart Rates in Early Childhood: A Deep Transfer Learning Approach. Sensors. 2023; 23(18):7665. https://doi.org/10.3390/s23187665
Chicago/Turabian StyleArasteh, Emad, Esther S. Veldhoen, Xi Long, Maartje van Poppel, Marjolein van der Linden, Thomas Alderliesten, Joppe Nijman, Robbin de Goederen, and Jeroen Dudink. 2023. "Ultra-Wideband Radar for Simultaneous and Unobtrusive Monitoring of Respiratory and Heart Rates in Early Childhood: A Deep Transfer Learning Approach" Sensors 23, no. 18: 7665. https://doi.org/10.3390/s23187665
APA StyleArasteh, E., Veldhoen, E. S., Long, X., van Poppel, M., van der Linden, M., Alderliesten, T., Nijman, J., de Goederen, R., & Dudink, J. (2023). Ultra-Wideband Radar for Simultaneous and Unobtrusive Monitoring of Respiratory and Heart Rates in Early Childhood: A Deep Transfer Learning Approach. Sensors, 23(18), 7665. https://doi.org/10.3390/s23187665