
Structural Anomalies Detection from Electrocardiogram (ECG) with Spectrogram and Handcrafted Features



Abstract
:1. Introduction
1.1. Related Work
1.1.1. Feature Extraction
1.1.2. Classification Tool
2. Materials and Methods
2.1. Data Description
2.2. Methodology
2.2.1. Signal Pre-Processing
2.2.2. Rhythm and Heartbeat Signal Extraction
2.2.3. Spectrogram Using Short-Time Fourier Transform
2.2.4. Handcrafted Features Rhythm Classification
2.2.5. Detecting the Number of R Peaks
2.2.6. Statistics Features
2.2.7. ECG Intervals Measurement
2.2.8. Handcrafted Features for Heartbeat Classification
2.2.9. Network Architecture
3. Experimental Setup and Result Discussion
3.1. Dataset Setup
3.2. Model Training and Testing
3.2.1. Multilead Utilization
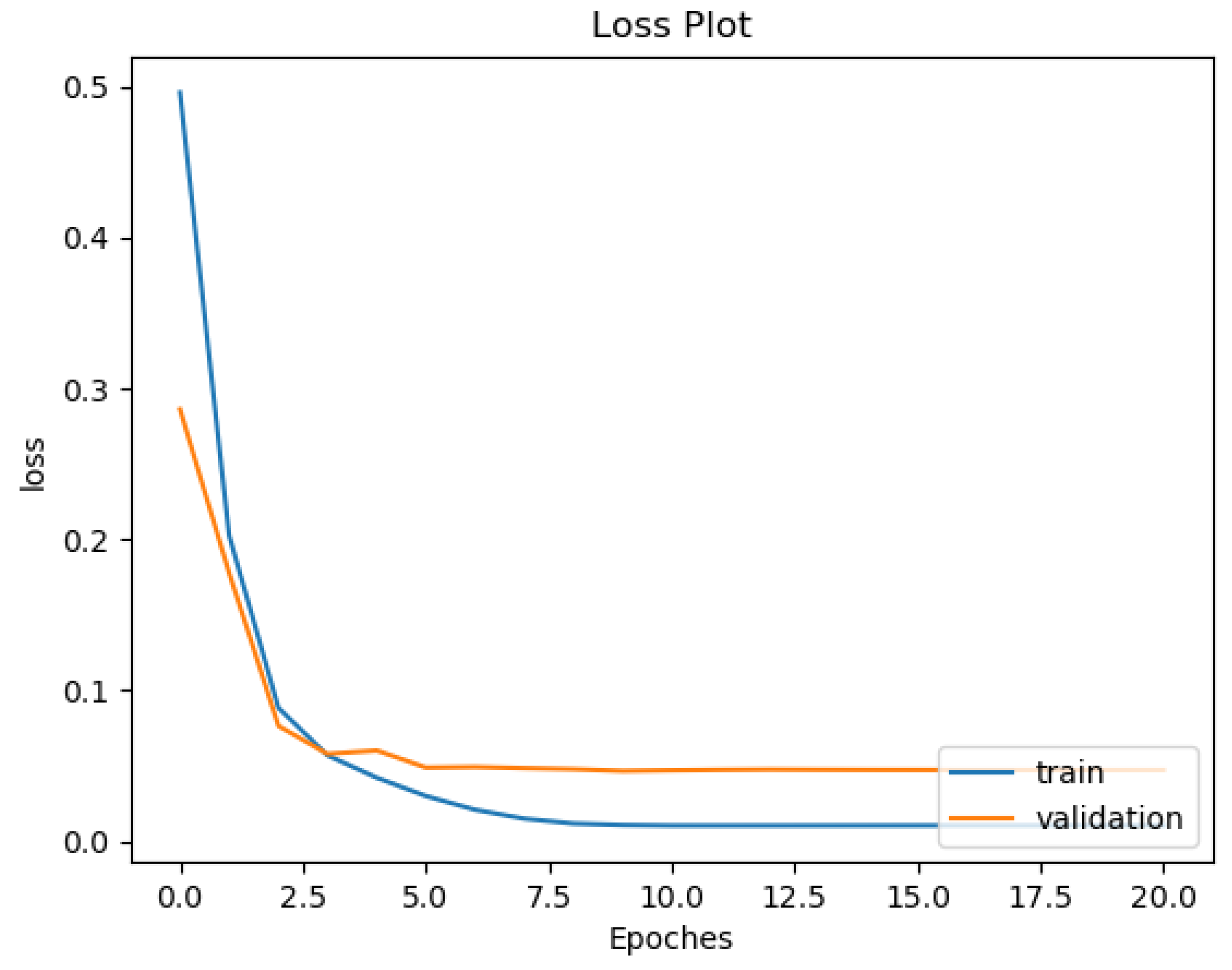
3.2.2. Over-Fitting Prevention
3.3. Evaluation Metrics
- TP: the number of successfully detected abnormal rhythms/heartbeats;
- FP: the number of wrongly detected abnormal rhythms/heartbeats;
- TN: the number of successfully detected normal rhythms/heartbeats;
- FN: the number of wrongly detected normal rhythms/heartbeats;
- Sensitivity (SEN) = TP/(TP + FN);
- False Alarm Rate (FAR)= 1 − Specificity = FP/(FP + TN);
- Positive Predictive Value (PPV) = TP/(TP + FP);
- Accuracy (ACC) = (TP + TN)/(TP + FP + TN + FN).
3.4. Comparison Results and Discussion
3.4.1. Rhythm Classification Result Discussion
3.4.2. Heartbeat Classification Result Comparison

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Method | A/N | Types | TP | FP | TN | FN | SEN | FAR | PPV | Accuracy | Time(s) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Christov [17]-morphology | 18,378/47,239 | 5 | 18,042 | 1604 | 45,635 | 336 | 98.17% | 3.40% | 91.84% | 97.04% | N/A |
| Christov [17]-frequency | 18,378/47,239 | 5 | 17,590 | 1459 | 45,780 | 788 | 95.71% | 3.09% | 92.34% | 96.58% | N/A |
| Chazal [18]-frequency | 4317/34,394 | 4 | 4108 | 1962 | 32,432 | 209 | 95.16% | 5.70% | 67.68% | 94.39% | N/A |
| Ubeyli [8] | 269/90 | 4 | 268 | 2 | 88 | 2 | 99.26% | 2.22% | 99.26% | 99.89% | N/A |
| Llamedo [38] | 5441/44,188 | 3 | 4752 | 2238 | 41,950 | 689 | 87.34% | 5.06% | 67.98% | 94.10% | N/A |
| Ye [12] | 20,745/65,264 | 16 | 20,557 | 286 | 64,978 | 188 | 99.09% | 0.44% | 98.63% | 99.32% | N/A |
| Zhang [11] | 5653/44,011 | 4 | 5248 | 4869 | 39,142 | 405 | 92.84% | 11.06% | 51.87% | 89.38% | N/A |
| Thomas [9] | 26,626/67,268 | 5 | 22,900 | 1300 | 65,968 | 3726 | 86.01% | 1.93% | 94.63% | 94.65% | N/A |
| Kiranyaz [23] | 7366/42,191 | 5 | 6539 | 1228 | 40,963 | 827 | 88.77% | 2.97% | 84.19% | 95.85% | N/A |
| Rajesh [10] | 8000/2000 | 5 | 7677 | 33 | 1967 | 323 | 95.96% | 1.65% | 99.57% | 96.44% | N/A |
| Sahoo [7] | 807/244 | 4 | 798 | 5 | 239 | 9 | 98.88% | 2.04% | 99.38% | 98.67% | N/A |
| Xia-VEB [37] | 300/- | 1 | - | - | - | - | 98.1% | 0.1% | 99.84% | 99.7% | N/A |
| Xia-SVEB [37] | 300/- | 1 | - | - | - | - | 97.2% | 0.1% | 99.57% | 99.8% | N/A |
| Sen [14] | 1154/1305 | 3 | 1149 | 39 | 1266 | 5 | 99.57% | 2.99% | 96.72% | 98.21% | N/A |
| Regular VGG16-RGB | 2425/2425 | 14 | 2196 | 75 | 2350 | 229 | 90.56% | 3.09% | 96.70% | 93.73% | 784 |
| Regular VGG19-RGB | 2425/2425 | 14 | 2171 | 58 | 2367 | 254 | 89.53% | 2.39% | 97.40% | 93.57% | 862 |
| Regular VGG16-Gray | 2425/2425 | 14 | 2276 | 45 | 2380 | 149 | 93.86% | 1.86% | 98.06% | 96% | 613 |
| Regular VGG19-Gray | 2425/2425 | 14 | 2359 | 22 | 2403 | 66 | 97.28% | 0.91% | 99.08% | 98.19% | 701 |
| Proposed VGG16-RGB | 2425/2425 | 14 | 2324 | 49 | 2376 | 101 | 95.84% | 2.02% | 97.94% | 96.91% | 774 |
| Proposed VGG19-RGB | 2425/2425 | 14 | 2188 | 57 | 2368 | 237 | 90.23% | 2.35% | 97.46% | 93.94% | 861 |
| Proposed VGG16-Gray | 2425/2425 | 14 | 2366 | 28 | 2397 | 59 | 97.57% | 1.15% | 98.83% | 98.21% | 612 |
| Proposed VGG19-Gray | 2425/2425 | 14 | 2367 | 28 | 2397 | 58 | 97.61% | 1.15% | 98.83% | 98.23% | 707 |
| Regular ResNet18-RGB | 2425/2425 | 14 | 2338 | 53 | 2372 | 87 | 96.41% | 2.19% | 97.78% | 97.11% | 388 |
| Regular ResNet34-RGB | 2425/2425 | 14 | 2354 | 60 | 2365 | 71 | 97.07% | 2.47% | 97.51% | 97.30% | 453 |
| Regular ResNet18-Gray | 2425/2425 | 14 | 2373 | 22 | 2403 | 52 | 97.66% | 0.91% | 98.47% | 99.08% | 212 |
| Regular ResNet34-Gray | 2425/2425 | 14 | 2377 | 19 | 2406 | 48 | 98.02% | 0.78% | 99.21% | 98.62% | 272 |
| Proposed ResNet18-RGB | 2425/2425 | 14 | 2390 | 26 | 2399 | 35 | 98.56% | 1.07% | 98.92% | 98.74% | 381 |
| Proposed ResNet34-RGB | 2425/2425 | 14 | 2394 | 32 | 2393 | 31 | 98.72% | 1.32% | 98.68% | 98.70% | 444 |
| Proposed ResNet18-Gray | 2425/2425 | 14 | 2402 | 18 | 2407 | 23 | 99.05% | 0.74% | 99.26% | 99.15% | 209 |
| Proposed ResNet34-Gray | 2425/2425 | 14 | 2396 | 11 | 2414 | 29 | 98.80% | 0.45% | 99.54% | 99.18% | 279 |
3.4.3. Discussion and Future Work
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roth, G.A.; Mensah, G.A.; Johnson, C.O.; Addolorato, G.; Ammirati, E.; Baddour, L.M.; Barengo, N.C.; Beaton, A.Z.; Benjamin, E.J.; Benziger, C.P.; et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: Update from the GBD 2019 study. J. Am. Coll. Cardiol. 2020, 76, 2982–3021. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Cardiovascular Diseases. 2017. Available online: https://www.who.int/health-topics/cardiovascular-diseases/#tab=tab_3 (accessed on 10 January 2022).
- Li, H.; Boulanger, P. An Automatic Method to Reduce Baseline Wander and Motion Artifacts on Ambulatory Electrocardiogram Signals. Sensors 2021, 21, 8169. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Boulanger, P. A Survey of Heart Anomaly Detection Using Ambulatory Electrocardiogram (ECG). Sensors 2020, 20, 1461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ge, D.; Srinivasan, N.; Krishnan, S.M. Cardiac arrhythmia classification using autoregressive modeling. Biomed. Eng. Online 2002, 1, 5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Özbay, Y.; Ceylan, R.; Karlik, B. Integration of type-2 fuzzy clustering and wavelet transform in a neural network based ECG classifier. Expert Syst. Appl. 2011, 38, 1004–1010. [Google Scholar] [CrossRef]
- Sahoo, S.; Kanungo, B.; Behera, S.; Sabut, S. Multiresolution wavelet transform based feature extraction and ECG classification to detect cardiac abnormalities. Measurement 2017, 108, 55–66. [Google Scholar] [CrossRef]
- Übeyli, E.D. Combining recurrent neural networks with eigenvector methods for classification of ECG beats. Digit. Signal Process. 2009, 19, 320–329. [Google Scholar] [CrossRef]
- Thomas, M.; Das, M.K.; Ari, S. Automatic ECG arrhythmia classification using dual tree complex wavelet based features. AEU-Int. J. Electron. Commun. 2015, 69, 715–721. [Google Scholar] [CrossRef]
- Rajesh, K.N.; Dhuli, R. Classification of ECG heartbeats using nonlinear decomposition methods and support vector machine. Comput. Biol. Med. 2017, 87, 271–284. [Google Scholar] [CrossRef]
- Zhang, Z.; Dong, J.; Luo, X.; Choi, K.S.; Wu, X. Heartbeat classification using disease-specific feature selection. Comput. Biol. Med. 2014, 46, 79–89. [Google Scholar] [CrossRef]
- Ye, C.; Kumar, B.V.; Coimbra, M.T. Heartbeat classification using morphological and dynamic features of ECG signals. IEEE Trans. Biomed. Eng. 2012, 59, 2930–2941. [Google Scholar] [PubMed]
- Zihlmann, M.; Perekrestenko, D.; Tschannen, M. Convolutional recurrent neural networks for electrocardiogram classification. In Proceedings of the 2017 Computing in Cardiology (CinC), Rennes, France, 24–27 September 2017; pp. 1–4. [Google Scholar]
- Şen, S.Y.; Özkurt, N. ECG arrhythmia classification by using convolutional neural network and spectrogram. In Proceedings of the 2019 Innovations in Intelligent Systems and Applications Conference (ASYU), Izmir, Turkey, 31 October–2 November 2019; pp. 1–6. [Google Scholar]
- Chuah, M.C.; Fu, F. ECG anomaly detection via time series analysis. In International Symposium on Parallel and Distributed Processing and Applications; Springer: Berlin/Heidelberg, Germany, 2007; pp. 123–135. [Google Scholar]
- Veeravalli, B.; Deepu, C.J.; Ngo, D. Real-time, personalized anomaly detection in streaming data for wearable healthcare devices. In Handbook of Large-Scale Distributed Computing in Smart Healthcare; Springer: Cham, Switzerland, 2017; pp. 403–426. [Google Scholar]
- Christov, I.; Gómez-Herrero, G.; Krasteva, V.; Jekova, I.; Gotchev, A.; Egiazarian, K. Comparative study of morphological and time-frequency ECG descriptors for heartbeat classification. Med. Eng. Phys. 2006, 28, 876–887. [Google Scholar] [CrossRef] [PubMed]
- De Chazal, P.; Reilly, R.B. A patient-adapting heartbeat classifier using ECG morphology and heartbeat interval features. IEEE Trans. Biomed. Eng. 2006, 53, 2535–2543. [Google Scholar] [CrossRef] [PubMed]
- O’Shea, K.; Nash, R. An introduction to convolutional neural networks. arXiv 2015, arXiv:1511.08458. [Google Scholar]
- Albawi, S.; Mohammed, T.A.; Al-Zawi, S. Understanding of a convolutional neural network. In Proceedings of the 2017 International Conference on Engineering and Technology (ICET), Antalya, Turkey, 21–23 August 2017; pp. 1–6. [Google Scholar]
- Rajpurkar, P.; Hannun, A.Y.; Haghpanahi, M.; Bourn, C.; Ng, A.Y. Cardiologist-level arrhythmia detection with convolutional neural networks. arXiv 2017, arXiv:1707.01836. [Google Scholar]
- Acharya, U.R.; Fujita, H.; Lih, O.S.; Hagiwara, Y.; Tan, J.H.; Adam, M. Automated detection of arrhythmias using different intervals of tachycardia ECG segments with convolutional neural network. Inf. Sci. 2017, 405, 81–90. [Google Scholar] [CrossRef]
- Kiranyaz, S.; Ince, T.; Gabbouj, M. Real-time patient-specific ECG classification by 1-D convolutional neural networks. IEEE Trans. Biomed. Eng. 2015, 63, 664–675. [Google Scholar] [CrossRef]
- Hochreiter, S.; Schmidhuber, J. Long short-term memory. Neural Comput. 1997, 9, 1735–1780. [Google Scholar] [CrossRef]
- Chauhan, S.; Vig, L. Anomaly detection in ECG time signals via deep long short-term memory networks. In Proceedings of the 2015 IEEE International Conference on Data Science and Advanced Analytics (DSAA), Paris, France, 19–21 October 2015; pp. 1–7. [Google Scholar]
- Moody, G.B.; Mark, R.G. The impact of the MIT-BIH arrhythmia database. IEEE Eng. Med. Biol. Mag. 2001, 20, 45–50. [Google Scholar] [CrossRef]
- Taddei, A.; Distante, G.; Emdin, M.; Pisani, P.; Moody, G.; Zeelenberg, C.; Marchesi, C. The European ST-T database: Standard for evaluating systems for the analysis of ST-T changes in ambulatory electrocardiography. Eur. Heart J. 1992, 13, 1164–1172. [Google Scholar] [CrossRef]
- Goldberger, A.L.; Amaral, L.A.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet: Components of a new research resource for complex physiologic signals. Circulation 2000, 101, e215–e220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MATLAB, Version 9.11.0 (R2021b); The MathWorks Inc.: Natick, MA, USA, 2021.
- Sejdić, E.; Djurović, I.; Jiang, J. Time–frequency feature representation using energy concentration: An overview of recent advances. Digit. Signal Process. 2009, 19, 153–183. [Google Scholar] [CrossRef]
- Mitra, S.K.; Kuo, Y. Digital Signal Processing: A Computer-Based Approach; McGraw-Hill: New York, NY, USA, 2006; Volume 2. [Google Scholar]
- Pan, J.; Tompkins, W.J. A real-time QRS detection algorithm. IEEE Trans. Biomed. Eng 1985, 32, 230–236. [Google Scholar] [CrossRef] [PubMed]
- Manikandan, M.S.; Soman, K. A novel method for detecting R-peaks in electrocardiogram (ECG) signal. Biomed. Signal Process. Control 2012, 7, 118–128. [Google Scholar] [CrossRef]
- Kim, H.Y. Statistical notes for clinical researchers: Assessing normal distribution (2) using skewness and kurtosis. Restor. Dent. Endod. 2013, 38, 52–54. [Google Scholar]
- You, K.; Long, M.; Wang, J.; Jordan, M.I. How does learning rate decay help modern neural networks? arXiv 2019, arXiv:1908.01878. [Google Scholar]
- Prechelt, L. Early stopping-but when? In Neural Networks: Tricks of the Trade; Springer: Berlin/Heidelberg, Germany, 1998; pp. 55–69. [Google Scholar]
- Xia, Y.; Zhang, H.; Xu, L.; Gao, Z.; Zhang, H.; Liu, H.; Li, S. An automatic cardiac arrhythmia classification system with wearable electrocardiogram. IEEE Access 2018, 6, 16529–16538. [Google Scholar] [CrossRef]
- Llamedo, M.; Martínez, J.P. Heartbeat classification using feature selection driven by database generalization criteria. IEEE Trans. Biomed. Eng. 2010, 58, 616–625. [Google Scholar] [CrossRef] [PubMed]
- Addabbo, P.; Besson, O.; Orlando, D.; Ricci, G. Adaptive detection of coherent radar targets in the presence of noise jamming. IEEE Trans. Signal Process. 2019, 67, 6498–6510. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.; Liu, W.; Hao, C.; Orlando, D. Persymmetric subspace detectors with multiple observations in homogeneous environments. IEEE Trans. Aerosp. Electron. Syst. 2020, 56, 3276–3284. [Google Scholar] [CrossRef]
- Hua, X.; Ono, Y.; Peng, L.; Cheng, Y.; Wang, H. Target detection within nonhomogeneous clutter via total Bregman divergence-based matrix information geometry detectors. IEEE Trans. Signal Process. 2021, 69, 4326–4340. [Google Scholar] [CrossRef]








| Symbol | Meaning | Database |
|---|---|---|
| NSR | Normal sinus rhythm | M, E |
| AB | Atrial bigeminy | M, E |
| AFIB | Atrial fibrillation | M, E |
| AFL | Atrial flutter | M |
| B | Ventricular bigeminy | M, E |
| BII | 2 heart block | M |
| B3 | 3 heart block | E |
| IVR | Idioventricular rhythm | M |
| NOD | Nodal (A-V junctional) rhythm | M |
| P | Paced rhythm | M |
| PREX | Pre-excitation (WPW) | M |
| SAB | Sino-atrial block | E |
| SBR | Sinus bradycardia | M, E |
| SVTA | Supraventricular tachyarrhythmia | M, E |
| T | Ventricular trigeminy | M, E |
| VFL | Ventricular flutter | M |
| VT | Ventricular tachycardia | M, E |
| Symbol | Meaning | Database |
|---|---|---|
| N | Normal | M, E |
| LBBB | Left bundle branch block beat | M |
| RBBB | Right bundle branch block beat | M |
| PAC | Atrial premature beat | M |
| a | Aberrated atrial premature beat | M, E |
| J | Nodal (junctional) premature beat | M, E |
| S | Supraventricular premature beat | M, E |
| PVC | Premature ventricular contraction | M, E |
| F | Fusion of ventricular and normal beat | M, E |
| e | Atrial escape beat | M |
| j | Nodal (junctional) escape beat | M, E |
| E | Ventricular escape beat | M, E |
| P | Paced beat | M |
| f | Fusion of paced and normal beat | M, E |
| Q | Unclassified beat | M |
| Method | A/N | Types | TP | FP | TN | FN | SEN | FAR | PPV | ACC | Time(s) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| AR modeling [5] | 713/143 | 6 | 706 | 10 | 133 | 7 | 99.02% | 6.99% | 98.60% | 98.01% | N/A |
| Acharya Net A [22] | 20,807/902 | 4 | 19,160 | 62 | 840 | 1647 | 92.08% | 6.87% | 99.68% | 92.13% | N/A |
| Acharya Net B [22] | 8322/361 | 4 | 7946 | 376 | 294 | 67 | 99.16% | 56.12% | 95.48% | 94.90% | N/A |
| Zihlmann [13] | - | 4 | - | - | - | - | - | - | - | 82.3% | N/A |
| Regular VGG16-RGB | 2653/2653 | 17 | 2522 | 185 | 2468 | 131 | 95.06% | 6.97% | 93.17% | 94.04% | 433 |
| Regular VGG19-RGB | 2653/2653 | 17 | 2436 | 235 | 2418 | 217 | 91.82% | 8.86% | 91.20% | 91.48% | 452 |
| Regular VGG16-Gray | 2653/2653 | 17 | 2554 | 215 | 2438 | 99 | 96.27% | 8.10% | 92.24% | 94.08% | 332 |
| Regular VGG19-Gray | 2653/2653 | 17 | 2544 | 116 | 2537 | 109 | 95.89% | 4.37% | 95.64% | 95.76% | 349 |
| Regular ResNet18-RGB | 2653/2653 | 17 | 2536 | 121 | 2532 | 117 | 95.59% | 4.56% | 95.45% | 95.51% | 117 |
| Regular ResNet34-RGB | 2653/2653 | 17 | 2550 | 131 | 2522 | 103 | 96.12% | 4.94% | 95.11% | 95.59% | 152 |
| Regular ResNet18-Gray | 2653/2653 | 17 | 2599 | 155 | 2498 | 54 | 97.96% | 5.84% | 94.37% | 96.06% | 61 |
| Regular ResNet34-Gray | 2653/2653 | 17 | 2635 | 150 | 2503 | 18 | 99.32% | 5.65% | 94.61% | 96.83% | 96 |
| Proposed VGG16-RGB | 2653/2653 | 17 | 2433 | 173 | 2480 | 220 | 91.71% | 6.52% | 93.36% | 92.59% | 425 |
| Proposed VGG19-RGB | 2653/2653 | 17 | 2476 | 199 | 2454 | 177 | 93.33% | 7.50% | 92.56% | 92.91% | 446 |
| Proposed VGG16-Gray | 2653/2653 | 17 | 2567 | 172 | 2481 | 86 | 96.76% | 6.48% | 93.72% | 95.14% | 319 |
| Proposed VGG19-Gray | 2653/2653 | 17 | 2572 | 134 | 2519 | 81 | 96.95% | 5.05% | 95.05% | 95.95% | 345 |
| Proposed ResNet18-RGB | 2653/2653 | 17 | 2648 | 15 | 2638 | 5 | 99.81% | 0.57% | 99.44% | 99.62% | 110 |
| Proposed ResNet34-RGB | 2653/2653 | 17 | 2646 | 10 | 2643 | 7 | 99.74% | 0.38% | 99.62% | 99.68% | 144 |
| Proposed ResNet18-Gray | 2653/2653 | 17 | 2646 | 4 | 2649 | 7 | 99.74% | 0.15% | 99.85% | 99.79% | 55 |
| Proposed ResNet34-Gray | 2653/2653 | 17 | 2649 | 8 | 2645 | 4 | 99.85% | 0.30% | 99.70% | 99.77% | 90 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, H.; Boulanger, P. Structural Anomalies Detection from Electrocardiogram (ECG) with Spectrogram and Handcrafted Features. Sensors 2022, 22, 2467. https://doi.org/10.3390/s22072467
Li H, Boulanger P. Structural Anomalies Detection from Electrocardiogram (ECG) with Spectrogram and Handcrafted Features. Sensors. 2022; 22(7):2467. https://doi.org/10.3390/s22072467
Chicago/Turabian StyleLi, Hongzu, and Pierre Boulanger. 2022. "Structural Anomalies Detection from Electrocardiogram (ECG) with Spectrogram and Handcrafted Features" Sensors 22, no. 7: 2467. https://doi.org/10.3390/s22072467
APA StyleLi, H., & Boulanger, P. (2022). Structural Anomalies Detection from Electrocardiogram (ECG) with Spectrogram and Handcrafted Features. Sensors, 22(7), 2467. https://doi.org/10.3390/s22072467