
Electromyographic Comparison of an Abdominal Rise on a Ball with a Traditional Crunch


Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Instruments
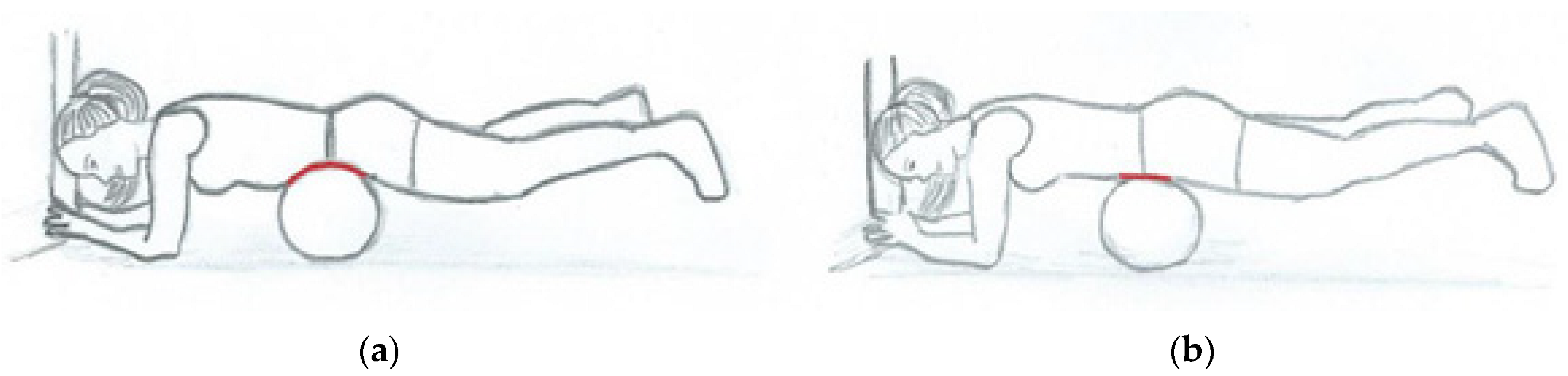
2.3. Exercises
2.4. Data Analyses
2.5. Statistical Analyses
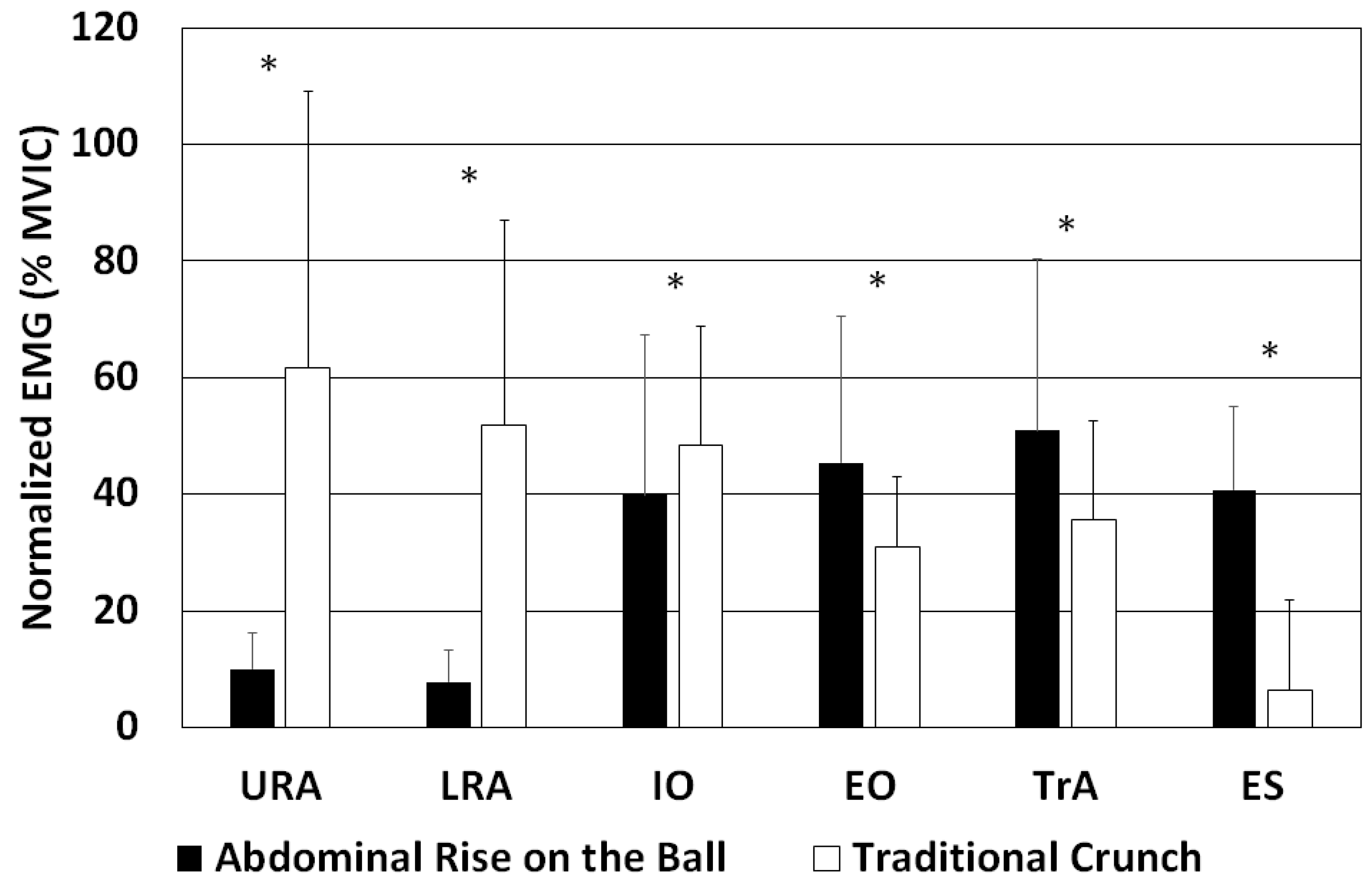
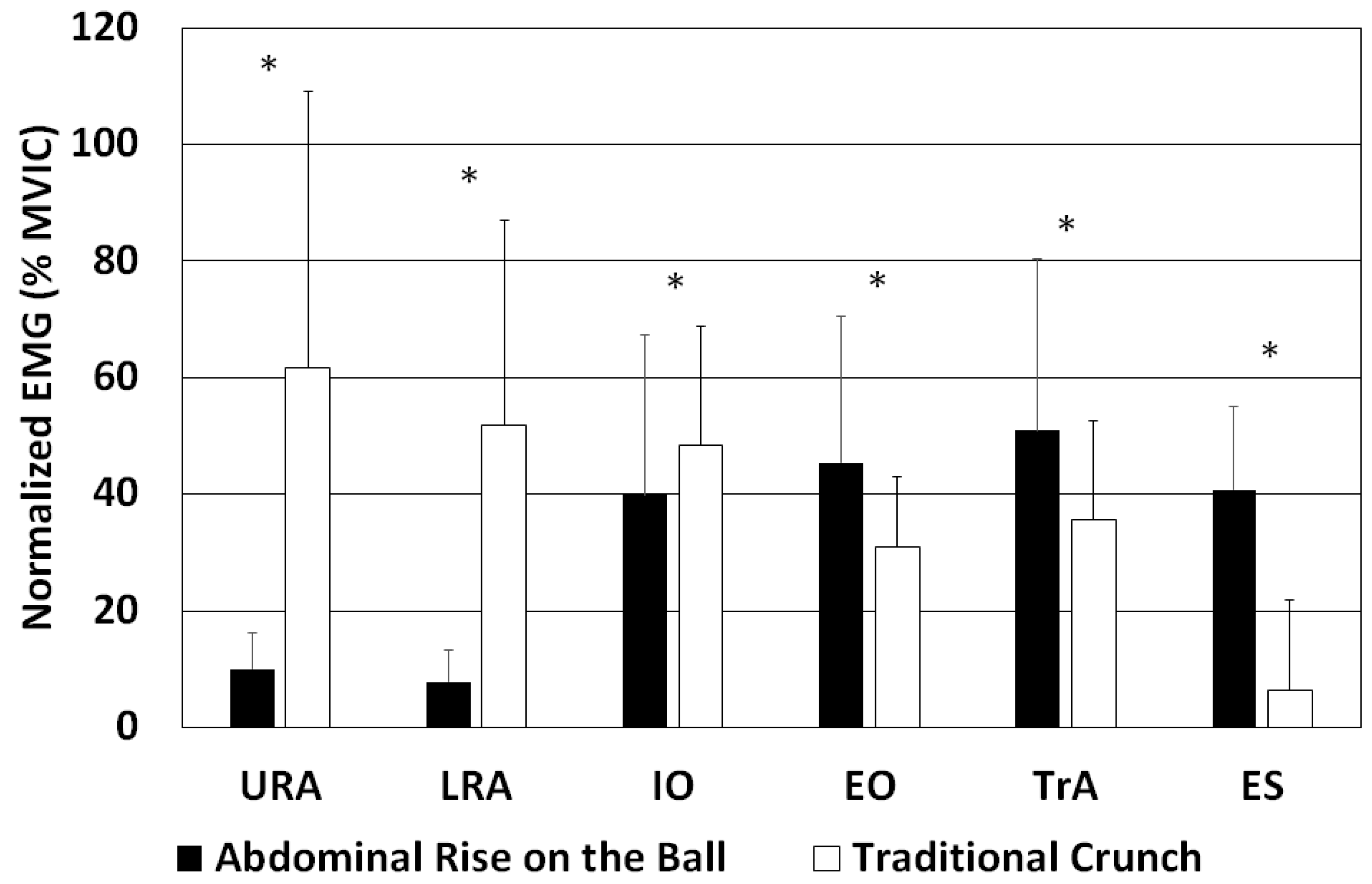
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Avedisian, L.; Kowalsky, D.S.; Albro, R.C.; Goldner, D.; Gill, R.C. Abdominal Strengthening Using the AbVice Machine as Measured by Surface Electromyographic Activation Levels. J. Strength Cond. Res. 2005, 19, 709–712. [Google Scholar] [CrossRef] [PubMed]
- Axler, C.T.; McGill, S.M. Low Back Loads over Abdominal Exercises: Searching for the Safest Abdominal Challenge. Med. Sci. Sport. Exerc. 1997, 29, 804–810. [Google Scholar] [CrossRef] [PubMed]
- Bird, M.; Fletcher, K.M.; Koch, A.J. Electromyographic Comparison of the Ab-Slide and Crunch Exercises. J. Strength Cond. Res. 2006, 20, 436–440. [Google Scholar] [CrossRef] [PubMed]
- Sternlicht, E.; Rugg, S.; Fujii, L.L.; Tomomitsu, K.F.; Seki, M.M.; Keri, T.F.; Seki, M.M. Electromyographic Comparison of a Stability Ball Crunch with a Traditional Crunch. J. Strength Cond. Res. 2007, 21, 506–509. [Google Scholar]
- Sternlicht, E.; Rugg, S.G.; Bernstein, M.D.; Armstrong, S.D. Electromyographical Analysis and Comparison of Selected Abdominal Training Devices with a Traditional Crunch. J. Strength Cond. Res. 2005, 19, 157–162. [Google Scholar] [CrossRef]
- Callaghan, J.P.; McGill, S.M. Intervertebral Disc Herniation: Studies on a Porcine Model Exposed to Highly Repetitive Flexion/Extension Motion with Compressive Force. Clin. Biomech. 2001, 16, 28–37. [Google Scholar] [CrossRef]
- Schoenfeld, B.J.; Kolber, M.J. Abdominal Crunches Are/Are Not a Safe and Effective Exercise. Strength Cond. J. 2016, 38, 61–64. [Google Scholar] [CrossRef]
- Ng, J.K.F.; Parnianpour, M.; Richardson, C.A.; Kippers, V. Functional Roles of Abdominal and Back Muscles during Isometric Axial Rotation of the Trunk. J. Orthop. Res. 2001, 19, 463–471. [Google Scholar] [CrossRef]
- Kavcic, N.; Grenier, S.; McGill, S.M. Determining the Stabilizing Role of Individual Torso Muscles during Rehabilitation Exercises. Spine 2004, 29, 1254–1265. [Google Scholar] [CrossRef]
- Hodges, P.W.; Eriksson, M.A.; Shirley, D.; Gandevia, S.C. Intra-Abdominal Pressure Increases Stiffness of the Lumbar Spine. J. Biomech. 2005, 38, 1873–1880. [Google Scholar] [CrossRef]
- Arjmand, N.; Shirazi-Adl, A. Role of Intra-Abdominal Pressure in the Unloading and Stabilization of the Human Spine during Static Lifting Tasks. Eur. Spine J. 2006, 15, 1265–1275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stokes, I.A.F.; Gardner-Morse, M.G.; Henry, S.M. Abdominal Muscle Activation Increases Lumbar Spinal Stability: Analysis of Contributions of Different Muscle Groups. Clin. Biomech. 2011, 26, 797–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guo, J.; Guo, W.; Ren, G. Embodiment of Intra-Abdominal Pressure in a Flexible Multibody Model of the Trunk and the Spinal Unloading Effects during Static Lifting Tasks. Biomech. Model. Mechanobiol. 2021, 20, 1599–1626. [Google Scholar] [CrossRef] [PubMed]
- Cresswell, A.G. Responses of Intra-Abdominal Pressure and Abdominal Muscle Activity during Dynamic Trunk Loading in Man. Eur. J. Appl. Physiol. Occup. Physiol. 1993, 66, 315–320. [Google Scholar] [CrossRef]
- Crommert, M.E.; Bjerkefors, A.; Tarassova, O.; Ekblom, M.M. Abdominal Muscle Activation During Common Modifications of the Trunk Curl-up Exercise. J. Strength Cond. Res. 2021, 35, 428–435. [Google Scholar] [CrossRef]
- El Ouaaid, Z.; Shirazi-Adl, A.; Plamondon, A.; Larivière, C. Trunk Strength, Muscle Activity and Spinal Loads in Maximum Isometric Flexion and Extension Exertions: A Combined in Vivo-Computational Study. J. Biomech. 2013, 46, 2228–2235. [Google Scholar] [CrossRef]
- Choi, J.-H.; Kim, D.-E.; Cynn, H.-S. Comparison of Trunk Muscle Activity Between Traditional Plank Exercise and Plank Exercise with Isometric Contraction of Ankle Muscles in Subjects with Chronic Low Back Pain. J. Strength Cond. Res. 2021, 35, 2407–2413. [Google Scholar] [CrossRef]
- Silva, F.H.O.; Arantes, F.J.; Gregorio, F.C.; Santos, F.R.A.; Fidale, T.M.; Bérzin, F.; Bigaton, D.R.; Lizardo, F.B. Comparison of the Electromyographic Activity of the Trunk and Rectus Femoris Muscles During Traditional Crunch and Exercise Using the 5-Minute Shaper Device. J. Strength Cond. Res. 2020, 34, 1–10. [Google Scholar] [CrossRef]
- Nakai, Y.; Kawada, M.; Miyazaki, T.; Araki, S.; Takeshita, Y.; Kiyama, R. A Self-Oblique Exercise That Activates the Coordinated Activity of Abdominal and Hip Muscles—A Pilot Study. PLoS ONE 2021, 16, e0255035. [Google Scholar] [CrossRef]
- Novak, J.; Jacisko, J.; Busch, A.; Cerny, P.; Stribrny, M.; Kovari, M.; Podskalska, P.; Kolar, P.; Kobesova, A. Intra-Abdominal Pressure Correlates with Abdominal Wall Tension during Clinical Evaluation Tests. Clin. Biomech. 2021, 88, 105426. [Google Scholar] [CrossRef]
- Mokhtarzadeh, H.; Anderson, D.E.; Allaire, B.T.; Bouxsein, M.L. Patterns of Load-to-Strength Ratios Along the Spine in a Population-Based Cohort to Evaluate the Contribution of Spinal Loading to Vertebral Fractures. J. Bone Miner. Res. 2021, 36, 704–711. [Google Scholar] [CrossRef] [PubMed]
- Beim, M.G.; Giraldo, L.J.; Pincivero, M.D.; Borror, J.M.; Fu, H.F. Abdominal Strengthening Exercises: A Comparative EMG Study. J. Sport Rehabil. 1997, 6, 11–20. [Google Scholar] [CrossRef]
- Escamilla, R.F.; Babb, E.; DeWitt, R.; Jew, P.; Kelleher, P.; Burnham, T.; Busch, J.; D’Anna, K.; Mowbray, R.; Imamura, R.T. Electromyographic Analysis of Traditional and Nontraditional Abdominal Exercises: Implications for Rehabilitation and Training. Phys. Ther. 2006, 86, 656–671. [Google Scholar] [CrossRef] [PubMed]
- Escamilla, R.F.; Lewis, C.; Bell, D.; Bramblet, G.; Daffron, J.; Lambert, S.; Pecson, A.; Imamura, R.; Paulos, L.; Dreanws, J.R. Core Muscle Activation during Swiss Ball and Traditional Abdominal Exercises. J. Orthop. Sports Phys. Ther. 2010, 40, 265–276. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NG, J.K.; Kippers, V.; Richardson, C.A. Muscle Fibre Orientation of Abdominal Muscles and Suggested Surface EMG Electrode Positions. Electromyogr. Clin. Neurophysiol. 1998, 31, 51–59. [Google Scholar]
- Stüpp, L.; Resende, A.; Petricelli, C.; Nakamura, M.; Alexandre, S.; Zanetti, M. Pelvic Floor Muscle and Transversus Abdominis Activation in Abdominal Hypopressive Technique Through Surface Electromyography. Neurourol. Urodyn. 2011, 30, 1518–1521. [Google Scholar] [CrossRef]
- Hermens, H.; Freriks, B. The State of the Art on Sensors and Sensor Placement Procedures for Surface Electromyography: A Proposal for Sensor Placement Procedures; Roessingh Research and Development: Enschede, The Netherlands, 1997. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences; Academic Press: New York, NY, USA, 1988. [Google Scholar]
- Sell, K.; Ghigiarelli, J.; Kitsos, J.; Burke, J.; Yeomans, S. Electromyographic Analysis of Abdominal and Lower Back Muscle Activation During Abdominal Exercises Using an Objective Biofeedback Device. J. Exerc. Physiol. 2011, 14, 54–66. [Google Scholar]
- Lee, N.; Kang, H.; Shin, G. Use of Antagonist Muscle EMG in the Assessment of Neuromuscular Health of the Low Back. J. Physiol. Anthropol. 2015, 34, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Daggfeldt, K. Extension Torque Production about the Lumbar Spine; Karolinska University Press: Stockholm, Sweden, 2002; ISBN 9173491071. [Google Scholar]
- McGill, S.M. Core Training: Evidence Translating to Better Performance and Injury Prevention. Strength Cond. J. 2010, 32, 33–46. [Google Scholar] [CrossRef] [Green Version]
- Kavcic, N.; Grenier, S.; McGill, S.M. Quantifying Tissue Loads and Spine Stability While Performing Commonly Prescribed Low Back Stabilization Exercises. Spine 2004, 29, 2319–2329. [Google Scholar] [CrossRef]
- Bojairami, I.; El Driscoll, M. Coordination Between Trunk Muscles, Thoracolumbar Fascia, and Intra-Abdominal Pressure Toward Static Spine Stability. Spine, 2021; Publish Ahead. [Google Scholar] [CrossRef]
- Stokes, I.A.F.; Gardner-Morse, M.G.; Henry, S.M. Intra-Abdominal Pressure and Abdominal Wall Muscular Function: Spinal Unloading Mechanism. Clin. Biomech. 2010, 25, 859–866. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daggfeldt, K.; Thorstensson, A.T. The Role of Intra-Abdominal Pressure in Spinal Unloading. J. Biomech. 1997, 30, 1149–1155. [Google Scholar] [CrossRef]
- McGill, S.M.; Norman, R.W. Reassessment of the Role of Intra-Abdominal Pressure in Spinal Compression. Ergonomics 1987, 30, 1565–1588. [Google Scholar] [CrossRef] [PubMed]
- Daggfeldt, K.; Thorstensson, A.T. The Mechanics of Back-Extensor Torque Production about the Lumbar Spine. J. Biomech. 2003, 36, 815–825. [Google Scholar] [CrossRef]
- Morris, J.M.; Lucas, D.B.; Bresler, B. Role of the Trunk in Stability of the Spine. J. Bone Jt. Surg. 1961, 43, 327–351. [Google Scholar] [CrossRef]
- Strongoli, L.M.; Gomez, C.L.; Coast, J.R. The Effect of Core Exercises on Transdiaphragmatic Pressure. J. Sport. Sci. Med. 2010, 9, 270–274. [Google Scholar]
- Ng, J.; Richardson, C. EMG Study of Erector Spinae and Multifidus in Two Isometric Back Extension Exercises. Aust. J. Physiother. 1994, 40, 115–121. [Google Scholar] [CrossRef] [Green Version]
- Konrad, P.; Schmitz, K.; Denner, A. Neuromuscular Evaluation of Trunk-Training Exercises. J. Athl. Train. 2001, 36, 109–118. [Google Scholar]
- De Troyer, A.; Sampson, M.; Sigrist, S.; Kelly, S. How the Abdominal Muscles Act on the Rib Cage. J. Appl. Physiol. 1983, 54, 465–469. [Google Scholar] [CrossRef]
- Hodges, P.W.; Cresswell, A.G.; Daggfeldt, K.; Thorstensson, A. In Vivo Measurement of the Effect of Intra-Abdominal Pressure on the Human Spine. J. Biomech. 2001, 34, 347–353. [Google Scholar] [CrossRef]
- Vuori, I.; Kannus, P. Exercise for Prevention of Osteoporotic Fractures. In Orthopeadic Issues in Osteoporosis; CRC Press: Boca Raton, FL, USA, 2002; pp. 543–555. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Muscle (%) | Abdominal Rise on the Ball | Traditional Crunch 1 | Effect Size |
|---|---|---|---|
| Upper rectus abdominis (URA) | 16 | 100 | 0.85 |
| Lower rectus abdominis (LRA) | 15 | 100 | 0.82 |
| Internal oblique (IO) | 82 | 100 | 0.67 |
| External oblique (EO) | 146 | 100 | 0.37 |
| Transversus abdominis (TrA) | 143 | 100 | 0.31 |
| Erector spinae (ES) | 641 2 | 100 | 0.77 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dolenec, A.; Svetina, M.; Strojnik, V. Electromyographic Comparison of an Abdominal Rise on a Ball with a Traditional Crunch. Sensors 2022, 22, 1979. https://doi.org/10.3390/s22051979
Dolenec A, Svetina M, Strojnik V. Electromyographic Comparison of an Abdominal Rise on a Ball with a Traditional Crunch. Sensors. 2022; 22(5):1979. https://doi.org/10.3390/s22051979
Chicago/Turabian StyleDolenec, Aleš, Mojca Svetina, and Vojko Strojnik. 2022. "Electromyographic Comparison of an Abdominal Rise on a Ball with a Traditional Crunch" Sensors 22, no. 5: 1979. https://doi.org/10.3390/s22051979
APA StyleDolenec, A., Svetina, M., & Strojnik, V. (2022). Electromyographic Comparison of an Abdominal Rise on a Ball with a Traditional Crunch. Sensors, 22(5), 1979. https://doi.org/10.3390/s22051979