
Whole-Body Adaptive Functional Electrical Stimulation Kinesitherapy Can Promote the Restoring of Physiological Muscle Synergies for Neurological Patients

 ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
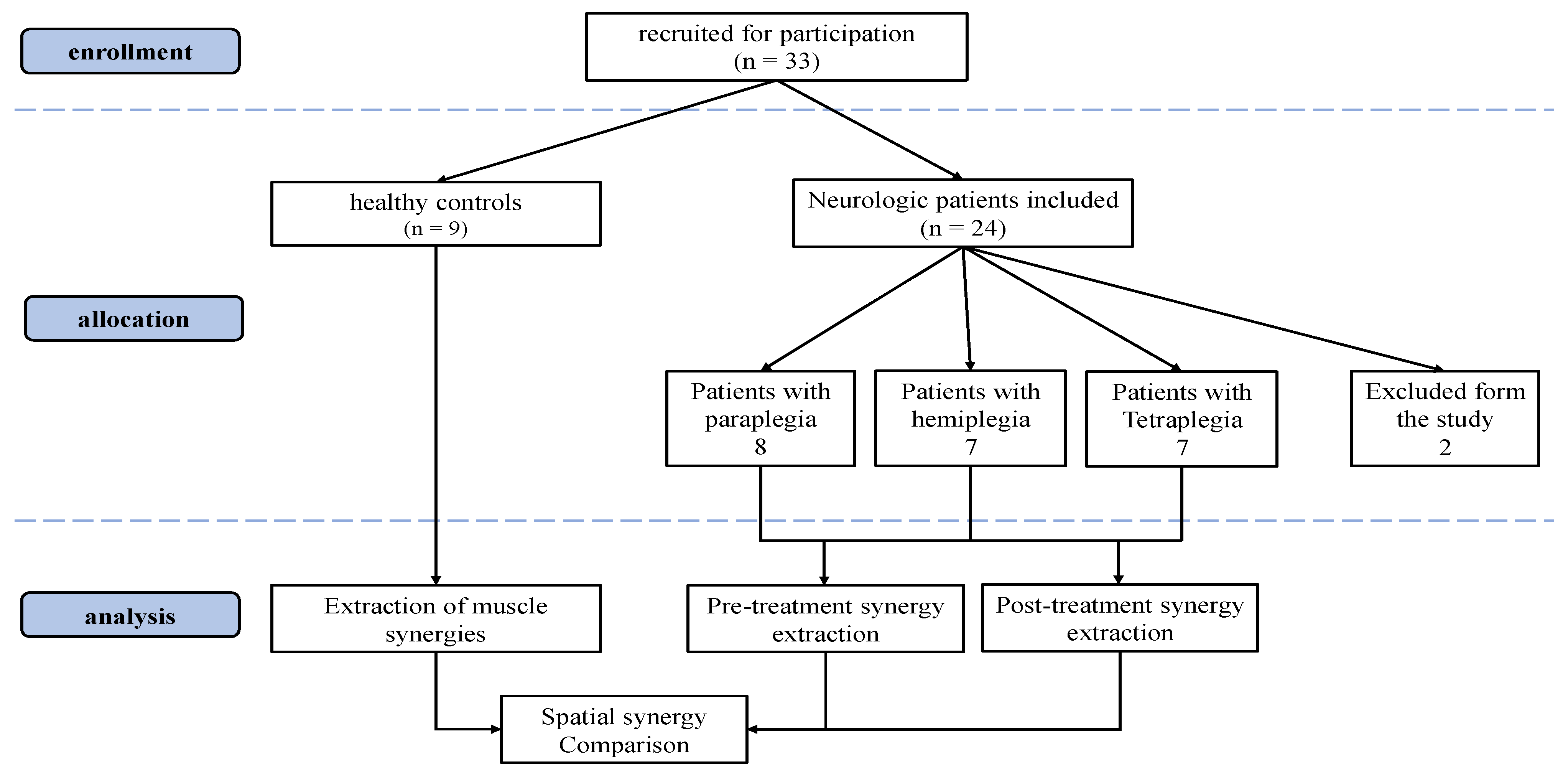
2.1. Participants
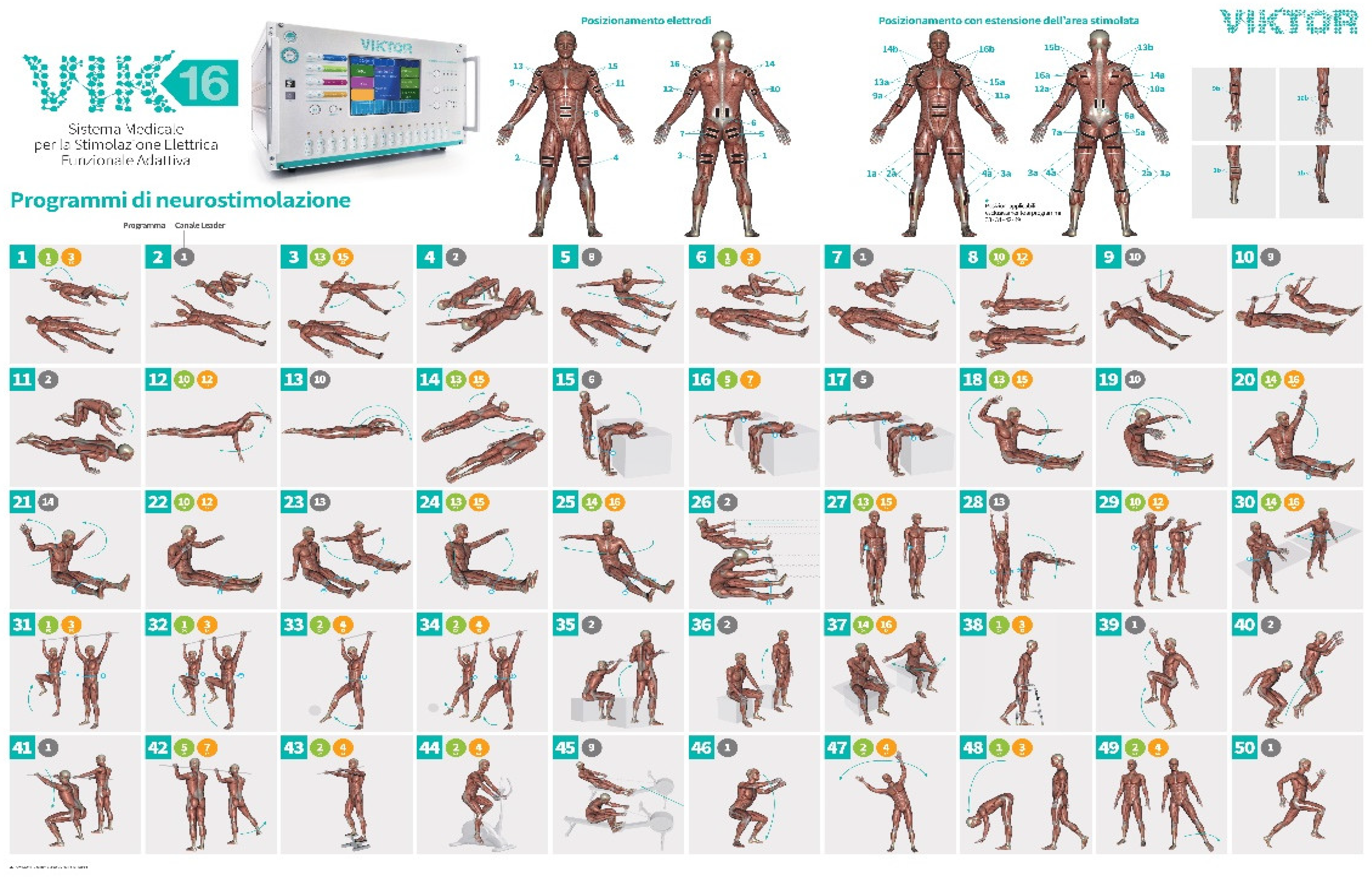
Treatment and Device: VIK16 Workstation AFESK™
2.2. Data Acquisition
2.2.1. Patients’ Protocol
- (1)
- Introductory, adaptation: 7–10 exercises—on average 3–5 min each
- (2)
- Restorative: 7–10 exercises—on average 3–5 min each
- (3)
- Postural correctional: 5–7 exercises of which 1–2 last for 10–15 min
- (4)
- Speed and endurance: 2–3 exercises of 15–20 min each
- (5)
- Increase the duration of basic exercises: 3–5 exercises according to the program for 10–20 min each
2.2.2. Control Group Protocol
2.3. Data Elaboration
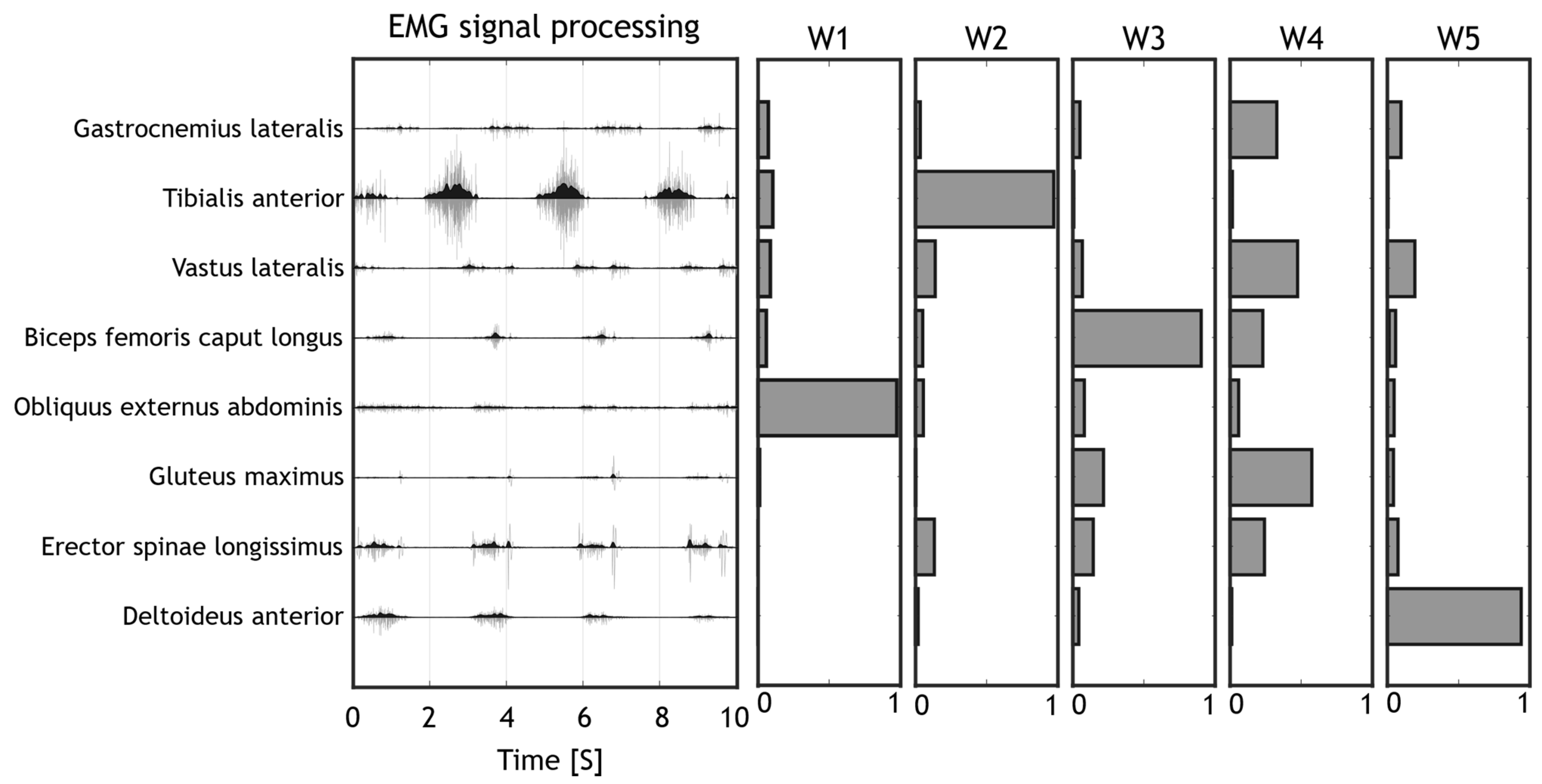
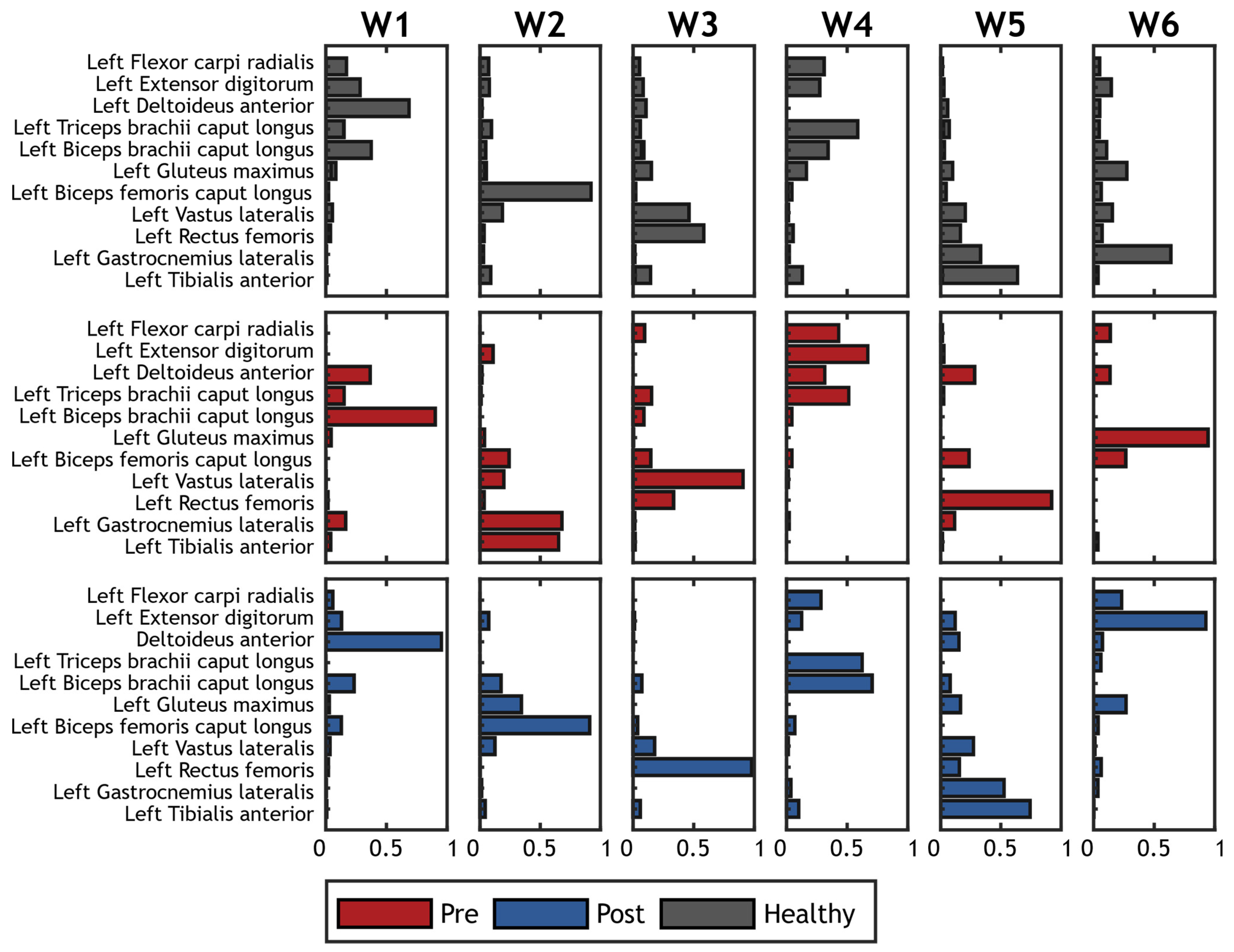
2.4. Synergy Extraction
Synergy Extraction: Control Group
2.5. Outcome Measures
2.6. Statistics
3. Results
4. Discussion
Limitations and Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ebels, P. EUObserver. 22 October 2012. Available online: https://euobserver.com/search?query=Disability+in+figures (accessed on 13 September 2021).
- Eurostat. Population Structure and Ageing. Statistics Explained. 2019. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Population_structure_and_ageing (accessed on 13 September 2021).
- World Health Organization. World Health Organization: Rehabilitation. 16 July 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/rehabilitation (accessed on 14 September 2021).
- Eurostat. Healthcare Expenditure Statistics. 2021. Available online: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Healthcare_expenditure_statistics#Healthcare_expenditure (accessed on 10 September 2021).
- Molteni, F.; Gasperini, G.; Cannaviello, G.; Guanziroli, E. Exoskeleton and End-Effector Robots for Upper and Lower Limbs Rehabilitation: Narrative Review. PM&R 2018, 10, S174–S188. [Google Scholar] [CrossRef]
- Ambrosini, E.; Ferrante, S.; Schauer, T.; Klauer, C.; Gaffuri, M.; Ferrigno, G.; Pedrocchi, A. A myocontrolled neuroprosthesis integrated with a passive exoskeleton to support upper limb activities. J. Electromyogr. Kinesiol. 2014, 24, 307–317. [Google Scholar] [CrossRef] [PubMed]
- Hamzaid, N.A.; Davis, G. Health and fitness benefits of functional electrical stimulation-evoked leg exercise for spinal cord–Injured individuals: A position review. Top. Spinal Cord Inj. Rehabil. 2009, 14, 88–121. [Google Scholar] [CrossRef]
- Jones, S.; Man, W.D.-C.; Gao, W.; Higginson, I.J.; Wilcock, A.; Maddocks, M. Neuromuscular electrical stimulation for muscle weakness in adults with advanced disease. Cochrane Database Syst. Rev. 2016, 2016, CD009419. [Google Scholar] [CrossRef]
- Sheffler, L.R.; Chae, J. Neuromuscular electrical stimulation in neurorehabilitation. Muscle Nerve Off. J. Am. Assoc. Electrodiagn. Med. 2007, 35, 562–590. [Google Scholar] [CrossRef] [PubMed]
- Van Griethuysen, C.M.; Paul, J.P.; Andrews, B.J.; Nicol, A.C. Biomechanics of functional electrical stimulation. Prosthet. Orthot. Int. 1982, 6, 152–156. [Google Scholar] [CrossRef]
- Sharif, F.; Ghulam, S.; Malik, A.N.; Saeed, Q. Effectiveness of Functional Electrical Stimulation (FES) versus Conventional Electrical Stimulation in Gait Rehabilitation of Patients with Stroke. J. Coll. Physicians Surg. Pak. 2017, 27, 703–706. [Google Scholar]
- Dujović, S.D.; Malešević, J.; Malešević, N.; Vidaković, A.S.; Bijelić, G.; Keller, T.; Konstantinović, L. Novel multi-pad functional electrical stimulation in stroke patients: A single-blind randomized study. NeuroRehabilitation 2017, 41, 791–800. [Google Scholar] [CrossRef]
- Knutson, J.S.; Harley, M.Y.; Hisel, T.Z.; Hogan, S.D.; Maloney, M.M.; Chae, J. Contralaterally controlled functional electrical stimulation for upper extremity hemiplegia: An early-phase randomized clinical trial in subacute stroke patients. Neurorehabilit. Neural Repair 2012, 26, 239–246. [Google Scholar] [CrossRef]
- Hara, Y.; Obayashi, S.; Tsujiuchi, K.; Muraoka, Y. The effects of electromyography-controlled functional electrical stimulation on upper extremity function and cortical perfusion in stroke patients. Clin. Neurophysiol. 2013, 124, 2008–2015. [Google Scholar] [CrossRef]
- Alon, G.; Levitt, A.F.; McCarthy, P.A. Functional Electrical Stimulation Enhancement of Upper Extremity Functional Recovery During Stroke Rehabilitation: A Pilot Study. Neurorehabilit. Neural Repair 2007, 21, 207–215. [Google Scholar] [CrossRef]
- Mazzoleni, S.; Battini, E.; Rustici, A.; Stampacchia, G. An integrated gait rehabilitation training based on Functional Electrical Stimulation cycling and overground robotic exoskeleton in complete spinal cord injury patients: Preliminary results. In Proceedings of the 2017 International Conference on Rehabilitation Robotics (ICORR), London, UK, 17–20 July 2017; pp. 289–293. [Google Scholar]
- Topçu, Ç.; Uysal, H.; Özkan, Ö.; Polat, Ö.; Bedeloğlu, M.; Akgül, A.; Döğer, E.N.; Sever, R.; Çolak, Ö.H. Recovery of facial expressions using functional electrical stimulation after full-face transplantation. J. Neuroeng. Rehabil. 2018, 15, 1–7. [Google Scholar] [CrossRef]
- Popovic, M.R.; Thrasher, T.A.; Adams, M.E.; Takes, V.; Zivanovic, V.; Tonack, M.I. Functional electrical therapy: Retraining grasping in spinal cord injury. Spinal Cord 2006, 44, 143–151. [Google Scholar] [CrossRef]
- McCabe, J.; Monkiewicz, M.; Holcomb, J.; Pundik, S.; Daly, J.J. Comparison of Robotics, Functional Electrical Stimulation, and Motor Learning Methods for Treatment of Persistent Upper Extremity Dysfunction after Stroke: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2015, 96, 981–990. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Zhu, K. Modeling biological motor control for human locomotion with functional electrical stimulation. Biol. Cybern. 2007, 96, 79–97. [Google Scholar] [CrossRef] [PubMed]
- Kimura, T.; Nakano, W. Repetition of a cognitive task promotes motor learning. Hum. Mov. Sci. 2019, 66, 109–116. [Google Scholar] [CrossRef] [PubMed]
- Dayan, E.; Cohen, L.G. Neuroplasticity Subserving Motor Skill Learning. Neuron 2011, 72, 443–454. [Google Scholar] [CrossRef]
- Doyon, J.; Benali, H. Reorganization and plasticity in the adult brain during learning of motor skills. Curr. Opin. Neurobiol. 2005, 15, 161–167. [Google Scholar] [CrossRef]
- He, K.; Liang, Y.; Abdollahi, F.; Bittmann, M.F.; Kording, K.; Wei, K. The Statistical Determinants of the Speed of Motor Learning. PLOS Comput. Biol. 2016, 12, e1005023. [Google Scholar] [CrossRef]
- Brushart, T. Motor axons preferentially reinnervate motor pathways. J. Neurosci. 1993, 13, 2730–2738. [Google Scholar] [CrossRef]
- Carmel, J.B.; Martin, J.H. Motor cortex electrical stimulation augments sprouting of the corticospinal tract and promotes recovery of motor function. Front. Integr. Neurosci. 2014, 8, 51. [Google Scholar] [CrossRef]
- Lee, W.A. Neuromotor Synergies as a Basis for Coordinated Intentional Action. J. Mot. Behav. 1984, 16, 135–170. [Google Scholar] [CrossRef]
- Bizzi, E.; Cheung, V.C.K.; D’Avella, A.; Saltiel, P.; Tresch, M. Combining modules for movement. Brain Res. Rev. 2008, 57, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Bizzi, E.; Cheung, V.C. The neural origin of muscle synergies. Front. Comput. Neurosci. 2013, 7, 51. [Google Scholar] [CrossRef] [PubMed]
- D’Avella, A.; Portone, A.; Fernandez, L.; Lacquaniti, F. Control of Fast-Reaching Movements by Muscle Synergy Combinations. J. Neurosci. 2006, 26, 7791–7810. [Google Scholar] [CrossRef]
- D’Avella, A.; Fernandez, L.; Portone, A.; Lacquaniti, F. Modulation of Phasic and Tonic Muscle Synergies with Reaching Direction and Speed. J. Neurophysiol. 2008, 100, 1433–1454. [Google Scholar] [CrossRef]
- Cheung, V.C.-K.; Piron, L.; Agostini, M.; Silvoni, S.; Turolla, A.; Bizzi, E. Stability of muscle synergies for voluntary actions after cortical stroke in humans. Proc. Natl. Acad. Sci. USA 2009, 106, 19563–19568. [Google Scholar] [CrossRef] [PubMed]
- Cheung, V.C.-K.; Turolla, A.; Agostini, M.; Silvoni, S.; Bennis, C.; Kasi, P.; Paganoni, S.; Bonato, P.; Bizzi, E. Muscle synergy patterns as physiological markers of motor cortical damage. Proc. Natl. Acad. Sci. USA 2012, 109, 14652–14656. [Google Scholar] [CrossRef]
- Banks, C.L.; Pai, M.M.; McGuirk, T.E.; Fregly, B.J.; Patten, C. Methodological Choices in Muscle Synergy Analysis Impact Differentiation of Physiological Characteristics Following Stroke. Front. Comput. Neurosci. 2017, 11, 78. [Google Scholar] [CrossRef]
- Ivanenko, Y.P.; Poppele, R.E.; Lacquaniti, F. Five basic muscle activation patterns account for muscle activity during human locomotion. J. Physiol. 2004, 556, 267–282. [Google Scholar] [CrossRef]
- Clark, D.J.; Ting, L.H.; Zajac, F.E.; Neptune, R.R.; Kautz, S.A. Merging of Healthy Motor Modules Predicts Reduced Locomotor Performance and Muscle Coordination Complexity Post-Stroke. J. Neurophysiol. 2010, 103, 844–857. [Google Scholar] [CrossRef] [PubMed]
- Dominici, N.; Ivanenko, Y.P.; Cappellini, G.; d’Avella, A.; Mondì, V.; Cicchese, M.; Fabiano, A.; Silei, T.; di Paolo, A.; Giannini, C.; et al. Locomotor primitives in newborn babies and their development. Science 2011, 334, 997–999. [Google Scholar] [CrossRef]
- Lencioni, T.; Jonsdottir, J.; Cattaneo, D.; Crippa, A.; Gervasoni, E.; Rovaris, M.; Bizzi, E.; Ferrarin, M. Are Modular Activations Altered in Lower Limb Muscles of Persons with Multiple Sclerosis during Walking? Evidence from Muscle Synergies and Biomechanical Analysis. Front. Hum. Neurosci. 2016, 10, 620. [Google Scholar] [CrossRef] [PubMed]
- Torres-Oviedo, G.; Ting, L.H. Muscle Synergies Characterizing Human Postural Responses. J. Neurophysiol. 2007, 98, 2144–2156. [Google Scholar] [CrossRef]
- Safavynia, S.A.; Ting, L.H. Task-level feedback can explain temporal recruitment of spatially fixed muscle synergies throughout postural perturbations. J. Neurophysiol. 2012, 107, 159–177. [Google Scholar] [CrossRef] [PubMed]
- Ambrosini, E.; Parati, M.; Peri, E.; De Marchis, C.; Nava, C.; Pedrocchi, A.; Ferriero, G.; Ferrante, S. Changes in leg cycling muscle synergies after training augmented by functional electrical stimulation in subacute stroke survivors: A pilot study. J. Neuroeng. Rehabil. 2020, 17, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Muceli, S.; Boye, A.T.; D’Avella, A.; Farina, D. Identifying Representative Synergy Matrices for Describing Muscular Activation Patterns During Multidirectional Reaching in the Horizontal Plane. J. Neurophysiol. 2010, 103, 1532–1542. [Google Scholar] [CrossRef] [PubMed]
- Denis, W.; Brunetti, F.; Piazza, S.; Torricelli, D.; Pons, J.L. Functional Electrical Stimulation Controller Based on Muscle Synergies. Converging Clin. Eng. Res. Neurorehabil. 2013, 283–287. [Google Scholar] [CrossRef]
- Ferrante, S.; Bejarano, N.C.; Ambrosini, E.; Nardone, A.; Turcato, A.M.; Monticone, M.; Ferrigno, G.; Pedrocchi, A. A Personalized Multi-Channel FES Controller Based on Muscle Synergies to Support Gait Rehabilitation after Stroke. Front. Neurosci. 2016, 10, 425. [Google Scholar] [CrossRef]
- Pano-Rodriguez, A.; Beltran-Garrido, J.V.; Hernández-González, V.; Reverter-Masia, J. Effects of whole-body ELECTROMYOSTIMULATION on health and performance: A systematic review. BMC Complement. Altern. Med. 2019, 19, 1–14. [Google Scholar] [CrossRef]
- Filipovic, A.; Kleinöder, H.; Dörmann, U.; Mester, J. Electromyostimulation—A Systematic Review of the Effects of Different Electromyostimulation Methods on Selected Strength Parameters in Trained and Elite Athletes. J. Strength Cond. Res. 2012, 26, 2600–2614. [Google Scholar] [CrossRef] [PubMed]
- Hashida, R.; Matsuse, H.; Takano, Y.; Omoto, M.; Nago, T.; Shiba, N. Walking exercise combined with neuromuscular electrical stimulation of antagonist resistance improved muscle strength and physical function for elderly people: A pilot study. J. Phys. Fit. Sports Med. 2016, 5, 195–203. [Google Scholar] [CrossRef]
- Bo, A.P.L.; da Fonseca, L.O.; de Sousa, A.C.C. FES-induced co-activation of antagonist muscles for upper limb control and disturbance rejection. Med. Eng. Phys. 2016, 38, 1176–1184. [Google Scholar] [CrossRef] [PubMed]
- Carson, R.G.; Buick, A.R. Neuromuscular electrical stimulation-promoted plasticity of the human brain. J. Physiol. 2019, 599, 2375–2399. [Google Scholar] [CrossRef] [PubMed]
- Rickham, P. Human experimentation. Code of ethics of the world medical association. Declaration of Helsinki. Br. Med. J. 1964, 2, 177. [Google Scholar]
- Ikuno, K.; Matsuo, A.; Shomoto, K. Sensory Electrical Stimulation for Recovery of Hand and Arm Function in Stroke Patients: A Review of the Literature. J. Nov. Physiother. 2012, 1, 7. [Google Scholar] [CrossRef]
- Karhu, J.; Tesche, C.D. Simultaneous early processing of sensory input in human primary (SI) and secondary (SII) somatosensory cortices. J. Neurophysiol. 1999, 81, 2017–2025. [Google Scholar] [CrossRef]
- del Vecchio, M.; Caruana, F.; Sartori, I.; Pelliccia, V.; Russo, G.L.; Rizzolatti, G.; Avanzini, P. Ipsilateral somatosensory responses in humans: The tonic activity of SII and posterior insular corte. Brain Struct. Funct. 2019, 224, 9–18. [Google Scholar] [CrossRef]
- Nas, K.; Yazmalar, L.; Şah, V.; Aydın, A.; Öneş, K. Rehabilitation of spinal cord injuries. World J. Orthop. 2015, 6, 8. [Google Scholar] [CrossRef]
- Klingner, C.M.; Huonker, R.; Flemming, S.; Hasler, C.; Brodoehl, S.; Preul, C.; Burmeister, H.; Kastrup, A.; Witte, O.W. Functional deactivations: Multiple ipsilateral brain areas engaged in the processing of somatosensory information. Hum. Brain Mapp. 2010, 32, 127–140. [Google Scholar] [CrossRef]
- Jovanovic, I.L.; Kapadia, N.; Lo, L.; Zivanovic, V.; Popovic, R.M.; Marquez-Chin, C. Restoration of Upper Limb Function After Chronic Severe Hemiplegia: A Case Report on the Feasibility of a Brain-Computer Interface-Triggered Functional Electrical Stimulation Therapy. Am. J. Phys. Med. Rehabil. 2020, 99, e35–e40. [Google Scholar] [CrossRef]
- Halonen, J.-P.; Jones, S.; Shawkat, F. Contribution of cutaneous and muscle afferent fibres to cortical SEPs following median and radial nerve stimulation in man. Electroencephalogr. Clin. Neurophysiol. Potentials Sect. 1988, 71, 331–335. [Google Scholar] [CrossRef]
- Avanzini, P.; Abdollahi, R.O.; Sartori, I.; Caruana, F.; Pelliccia, V.; Casaceli, G.; Mai, R.; Russo, G.L.; Rizzolatti, G.; Orban, G.A. Four-dimensional maps of the human somatosensory system. Proc. Natl. Acad. Sci. USA 2016, 113, E1936–E1943. [Google Scholar] [CrossRef]
- Kaas, J.; Pons, T. The somatosensory system of primates. In Neurosciences: Comparative Primate Biology; The Univeristy of Chicago Press Journals: Chicago, IL, USA, 1988; pp. 421–468. [Google Scholar]
- Hardy, S.G.P.; Spalding, T.B.; Liu, H.; Nick, T.G.; Pearson, R.H.; Hayes, A.V.; Stokic, D. The Effect of Transcutaneous Electrical Stimulation on Spinal Motor Neuron Excitability in People Without Known Neuromuscular Diseases: The Roles of Stimulus Intensity and Location. Phys. Ther. 2002, 82, 354–363. [Google Scholar] [CrossRef] [PubMed]
- Driver, J.; Noesselt, T. Review Multisensory Interplay Reveals Crossmodal Influences on ‘Sensory-Specific’ Brain Regions, Neural Responses, and Judgments. Neuron 2008, 57, 11–23. [Google Scholar] [CrossRef] [PubMed]
- Rath, M.; Vette, A.H.; Ramasubramaniam, S.; Li, K.; Burdick, J.; Edgerton, V.R.; Gerasimenko, Y.P.; Sayenko, D.G. Trunk Stability Enabled by Noninvasive Spinal Electrical Stimulation after Spinal Cord Injury. J. Neurotrauma 2018, 35, 2540–2553. [Google Scholar] [CrossRef] [PubMed]
- Tan, Z.; Liu, H.; Yan, T.; Jin, D.; He, X.; Zheng, X.; Xu, S.; Tan, C. The Effectiveness of Functional Electrical Stimulation Based on a Normal Gait Pattern on Subjects with Early Stroke: A Randomized Controlled Trial. BioMed Res. Int. 2014, 2014, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Arendsen, L.J.; Guggenberger, R.; Zimmer, M.; Weigl, T.; Gharabaghi, A. Peripheral Electrical Stimulation Modulates Cortical Beta-Band Activity. Front. Neurosci. 2021, 15, 339. [Google Scholar] [CrossRef] [PubMed]
- Cebolla, A.; Cheron, G. Sensorimotor and cognitive involvement of the beta–gamma oscillation in the frontal N30 component of somatosensory evoked potentials. Neuropsychologia 2015, 79, 215–222. [Google Scholar] [CrossRef]
- Cooke, S.F.; Bliss, T.V. Plasticity in the human central nervous system. Brain 2006, 129, 1659–1673. [Google Scholar] [CrossRef]
- Howlett, O.A.; Lannin, N.; Ada, L.; McKinstry, C. Functional Electrical Stimulation Improves Activity After Stroke: A Systematic Review with Meta-Analysis. Arch. Phys. Med. Rehabil. 2015, 96, 934–943. [Google Scholar] [CrossRef] [PubMed]
- Guertin, P.A. Central Pattern Generator for Locomotion: Anatomical, Physiological, and Pathophysiological Considerations. Front. Neurol. 2013, 3, 183. [Google Scholar] [CrossRef]
- Stegeman, D.; Hermens, H. Standards for surface electromyography: The European project Surface EMG for non-invasive assessment of muscles (SENIAM). Enschede Roessingh Res. Dev. 2007, 10, 108–112. [Google Scholar]
- Duthilleul, N.; Pirondini, E.; Coscia, M.; Micera, S. Effect of handedness on muscle synergies during upper limb planar movements. In Proceedings of the 2015 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milano, Italy, 25–29 August 2015; pp. 3452–3455. [Google Scholar]
- Steele, K.M.; Rozumalski, A.; Schwartz, M. Muscle synergies and complexity of neuromuscular control during gait in cerebral palsy. Dev. Med. Child Neurol. 2015, 57, 1176–1182. [Google Scholar] [CrossRef] [PubMed]
- Scano, A.; Dardari, L.; Molteni, F.; Giberti, H.; Tosatti, L.M.; D’Avella, A. A Comprehensive Spatial Mapping of Muscle Synergies in Highly Variable Upper-Limb Movements of Healthy Subjects. Front. Physiol. 2019, 10, 1231. [Google Scholar] [CrossRef] [PubMed]
- Torres-Oviedo, G.; MacPherson, J.M.; Ting, L.H. Muscle Synergy Organization Is Robust Across a Variety of Postural Perturbations. J. Neurophysiol. 2006, 96, 1530–1546. [Google Scholar] [CrossRef]
- Mayr, S.; Erdfelder, E.; Buchner, A.; Faul, F. A short tutorial of GPower. Tutor. Quant. Methods Psychol. 2007, 3, 51–59. [Google Scholar] [CrossRef]
- Niu, C.M.; Bao, Y.; Zhuang, C.; Li, S.; Wang, T.; Cui, L.; Xie, Q.; Lan, N. Synergy-Based FES for Post-Stroke Rehabilitation of Upper-Limb Motor Functions. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 256–264. [Google Scholar] [CrossRef]
- Galeano, D.; Brunetti, F.; Torricelli, D.; Piazza, S.; Pons, J.L. A Tool for Balance Control Training Using Muscle Synergies and Multimodal Interfaces. BioMed Res. Int. 2014, 2014, 1–13. [Google Scholar] [CrossRef]
- Li, S.; Zhuang, C.; Niu, C.M.; Bao, Y.; Xie, Q.; Lan, N. Evaluation of Functional Correlation of Task-Specific Muscle Synergies with Motor Performance in Patients Poststroke. Front. Neurol. 2017, 8, 337. [Google Scholar] [CrossRef]
- Cole, N.M.; Ajiboye, A.B. Muscle synergies for predicting non-isometric complex hand function for commanding FES neuroprosthetic hand systems. J. Neural Eng. 2019, 16, 56018. [Google Scholar] [CrossRef] [PubMed]
- Chou, C.-H.; Wang, T.; Sun, X.; Niu, C.M.; Hao, M.; Xie, Q.; Lan, N. Automated functional electrical stimulation training system for upper-limb function recovery in poststroke patients. Med. Eng. Phys. 2020, 84, 174–183. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.; Lim, T.; Lee, J.; Sim, J.; Chang, H.; Yoon, B.; Jung, H. Patient-specific functional electrical stimulation strategy based on muscle synergy and walking posture analysis for gait rehabilitation of stroke patients. J. Int. Med. Res. 2021, 49. [Google Scholar] [CrossRef] [PubMed]
- Matsui, K.; Hishii, Y.; Maegaki, K.; Yamashita, Y.; Uemura, M.; Hirai, H.; Miyazaki, F. Equilibrium-point control of human elbow-joint movement under isometric environment by using multichannel functional electrical stimulation. Front. Neurosci. 2014, 8, 164. [Google Scholar] [CrossRef] [PubMed]
- Lan, Y.; Yao, J.; Dewald, J.P. The impact of shoulder abduction loading on EMG-based intention detection of hand opening and closing after stroke. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; pp. 4136–4139. [Google Scholar]
- Williams, M.R. A pilot study into reaching performance after severe to moderate stroke using upper arm support. PLoS ONE 2018, 13, e0200787. [Google Scholar] [CrossRef] [PubMed]
- Scano, A.; Mira, R.M.; D’Avella, A. Mixed matrix factorization: A novel algorithm for the extraction of kinematic-muscular synergies. bioRxiv 2022. [Google Scholar] [CrossRef]
- Belfatto, A.; Scano, A.; Chiavenna, A.; Mastropietro, A.; Mrakic-Sposta, S.; Pittaccio, S.; Tosatti, L.M.; Molteni, F.; Rizzo, G. A Multiparameter Approach to Evaluate Post-Stroke Patients: An Application on Robotic Rehabilitation. Appl. Sci. 2018, 8, 2248. [Google Scholar] [CrossRef]
- Brambilla, C.; Pirovano, I.; Mira, R.M.; Rizzo, G.; Scano, A.; Mastropietro, A. Combined Use of EMG and EEG Techniques for Neuromotor Assessment in Rehabilitative Applications: A Systematic Review. Sensors 2021, 21, 7014. [Google Scholar] [CrossRef] [PubMed]
- Hofstoetter, U.S.; Krenn, M.; Danner, S.M.; Hofer, C.; Kern, H.; McKay, W.B.; Mayr, W.; Minassian, K. Augmentation of Voluntary Locomotor Activity by Transcutaneous Spinal Cord Stimulation in Motor-Incomplete Spinal Cord-Injured Individuals. Artif. Organs 2015, 39, E176–E186. [Google Scholar] [CrossRef]
- Kimura, T.; Kaneko, F.; Iwamoto, E.; Saitoh, S.; Yamada, T. Neuromuscular electrical stimulation increases serum brain-derived neurotrophic factor in humans. Exp. Brain Res. 2018, 237, 47–56. [Google Scholar] [CrossRef]
- Korvenoja, A.; Huttunen, J.; Salli, E.; Pohjonen, H.; Martinkauppi, S.; Palva, J.M.; Lauronen, L.; Virtanen, J.; And, R.J.I.; Aronen, H.J. Activation of multiple cortical areas in response to somatosensory stimulation: Combined magnetoencephalographic and functional magnetic resonance imaging. Hum. Brain Mapp. 1999, 8, 13–27. [Google Scholar] [CrossRef]
- McGie, S.C.; Zariffa, J.; Popovic, M.R.; Nagai, M.K. Short-Term Neuroplastic Effects of Brain-Controlled and Muscle-Controlled Electrical Stimulation. Neuromodul. Technol. Neural Interface 2015, 18, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Nascimento, L.; Michaelsen, S.M.; Ada, L.; Polese, J.C.; Teixeira-Salmela, L.F. Cyclical electrical stimulation increases strength and improves activity after stroke: A systematic review. J. Physiother. 2014, 60, 22–30. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Olsen, S.; Signal, N.; Niazi, I.K.; Christensen, T.; Jochumsen, M.; Taylor, D. Paired Associative Stimulation Delivered by Pairing Movement-Related Cortical Potentials with Peripheral Electrical Stimulation: An Investigation of the Duration of Neuromodulatory Effects. Neuromodul. Technol. Neural Interface 2018, 21, 362–367. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pulse Width (µs)/Pulse Frequency (Hz) | |||
|---|---|---|---|
| Hemiplegia | 200/100 | after adaptation | 500/50–100 |
| Hemiparesis | 100/50–100 | after adaptation | 200/100 |
| Paraplegia | 200/100 | after adaptation | 500/50–100 |
| Paraparesis | 100/50–100 | after adaptation | 200/100 |
| Tetraplegia | 200/100 | after adaptation | 500/50–100 |
| Tetraparesis | 200/50 | after adaptation | 200/100 |
| Hemiplegic | N° Sessions | Sessions/Week | Cycles Movements/Session | Total Movement Cycles |
|---|---|---|---|---|
| Hemiplegic | 71 | 2.25 | 813 | 57,720 |
| Paraplegic | 80 | 2.25 | 705 | 56,461 |
| Tetraplegic | 40 | 1.4 | 667 | 26,709 |
| Hemiplegic Patients | Tetraplegic Patients | Paraplegic Patients | |
|---|---|---|---|
| Biceps brachii caput longus | |||
| Biceps femoris caput longus | |||
| Deltoideus anterior | |||
| Deltoideus posterior | |||
| Erector spinae longissimus | |||
| Extensor carpi radialis longus | |||
| Extensor digitorum | |||
| Flexor carpi radialis | |||
| Gastrocnemius lateralis | |||
| Gluteus maximus | |||
| Latissimus Dorsi | |||
| Obliquus externus abdominis | |||
| Obliquus internus abdominis | |||
| Rectus abdominis | |||
| Rectus femoris | |||
| Tibialis anterior | |||
| Trapezius descendens | |||
| Triceps brachii caput lateralis | |||
| Triceps brachii caput longus | |||
| Vastus lateralis |
| Hemiplegic Patients | Tetraplegic Patients | Paraplegic Patients | |
|---|---|---|---|
| Walking | |||
| Crutch assisted walking | |||
| Lying down arm and contralateral knee adduction | |||
| Lying down Knees and arms abduction | |||
| Lying down Jumping jacks | |||
| Hip thrust | |||
| Torso Torsion | |||
| Knees adduction | |||
| Prone to cat pose | |||
| Sitting Punching | |||
| Shoulder abduction | |||
| Standing Punching | |||
| Standing Knee adduction | |||
| Sit to stand | |||
| March | |||
| Jump | |||
| Squat | |||
| Exoskeleton assisted movement | |||
| Push |
| Motricity Index | Hemiplegic Patients | Paraplegic Patients | Tetraplegic Patients | ||||
|---|---|---|---|---|---|---|---|
| Subject ID | Body Segment | PRE | POST | PRE | POST | PRE | POST |
| S1 | ARM | 10 | 34 | 100 | 100 | 40 | 73 |
| LEG | 70 | 76 | 29 | 67 | 38 | 53 | |
| TRUNK | 25 | 25 | 100 | 100 | 61 | 74 | |
| S2 | ARM | 50 | 73 | 100 | 100 | 29 | 29 |
| LEG | 91 | 100 | 76 | 100 | 1 | 1 | |
| TRUNK | 25 | 25 | 100 | 100 | 0 | 0 | |
| S3 | ARM | 34 | 41 | 100 | 100 | 29 | 29 |
| LEG | 76 | 76 | 1 | 10 | 24 | 24 | |
| TRUNK | 25 | 25 | 61 | 61 | 0 | 0 | |
| S4 | ARM | 1 | 18 | 100 | 100 | 19 | 40 |
| LEG | 24 | 29 | 28 | 28 | 19 | 39 | |
| TRUNK | 74 | 74 | 74 | 74 | 0 | 36 | |
| S5 | ARM | 10 | 15 | 100 | 100 | 29 | 29 |
| LEG | 29 | 39 | 1 | 10 | 29 | 29 | |
| TRUNK | 100 | 100 | 74 | 74 | 24 | 29 | |
| S6 | ARM | 10 | 29 | 100 | 100 | 29 | 34 |
| LEG | 19 | 29 | 1 | 10 | 29 | 29 | |
| TRUNK | 61 | 74 | 61 | 61 | 48 | 61 | |
| S7 | ARM | 19 | 29 | 100 | 100 | 92 | 100 |
| LEG | 28 | 38 | 58 | 76 | 92 | 100 | |
| TRUNK | 61 | 74 | 87 | 87 | 100 | 100 | |
| S8 | ARM | 34 | 39 | ||||
| LEG | 38 | 53 | |||||
| TRUNK | 87 | 100 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scano, A.; Mira, R.M.; Gabbrielli, G.; Molteni, F.; Terekhov, V. Whole-Body Adaptive Functional Electrical Stimulation Kinesitherapy Can Promote the Restoring of Physiological Muscle Synergies for Neurological Patients. Sensors 2022, 22, 1443. https://doi.org/10.3390/s22041443
Scano A, Mira RM, Gabbrielli G, Molteni F, Terekhov V. Whole-Body Adaptive Functional Electrical Stimulation Kinesitherapy Can Promote the Restoring of Physiological Muscle Synergies for Neurological Patients. Sensors. 2022; 22(4):1443. https://doi.org/10.3390/s22041443
Chicago/Turabian StyleScano, Alessandro, Robert Mihai Mira, Guido Gabbrielli, Franco Molteni, and Viktor Terekhov. 2022. "Whole-Body Adaptive Functional Electrical Stimulation Kinesitherapy Can Promote the Restoring of Physiological Muscle Synergies for Neurological Patients" Sensors 22, no. 4: 1443. https://doi.org/10.3390/s22041443
APA StyleScano, A., Mira, R. M., Gabbrielli, G., Molteni, F., & Terekhov, V. (2022). Whole-Body Adaptive Functional Electrical Stimulation Kinesitherapy Can Promote the Restoring of Physiological Muscle Synergies for Neurological Patients. Sensors, 22(4), 1443. https://doi.org/10.3390/s22041443