
A Meta-Analysis on Remote HRI and In-Person HRI: What Is a Socially Assistive Robot to Do?


Abstract
:1. Introduction
2. Related Works
2.1. In-Person Robot Assistance
2.2. Remote Robot Assistance
2.3. Summary
3. Methodology
3.1. Meta-Analysis Criteria
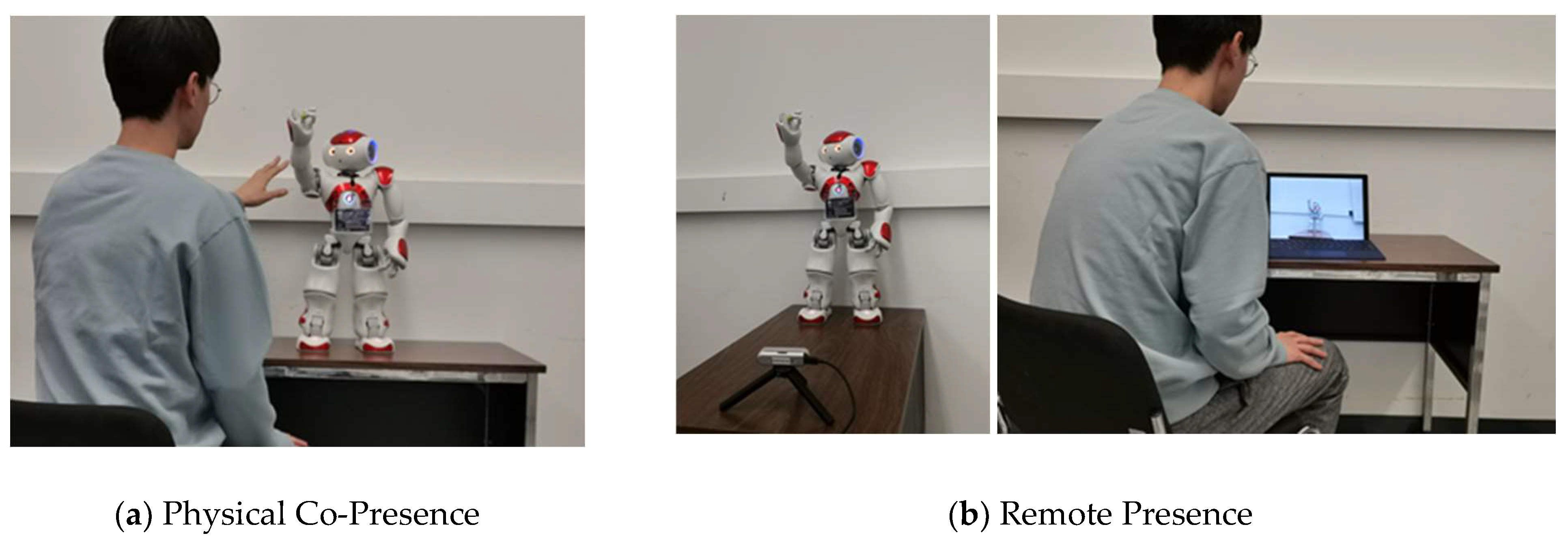
3.1.1. Studies with Differences between Outcomes for in-Person and Remote HRI
3.1.2. Studies without Differences between Outcomes for in-Person and Remote HRI
3.1.3. Summary
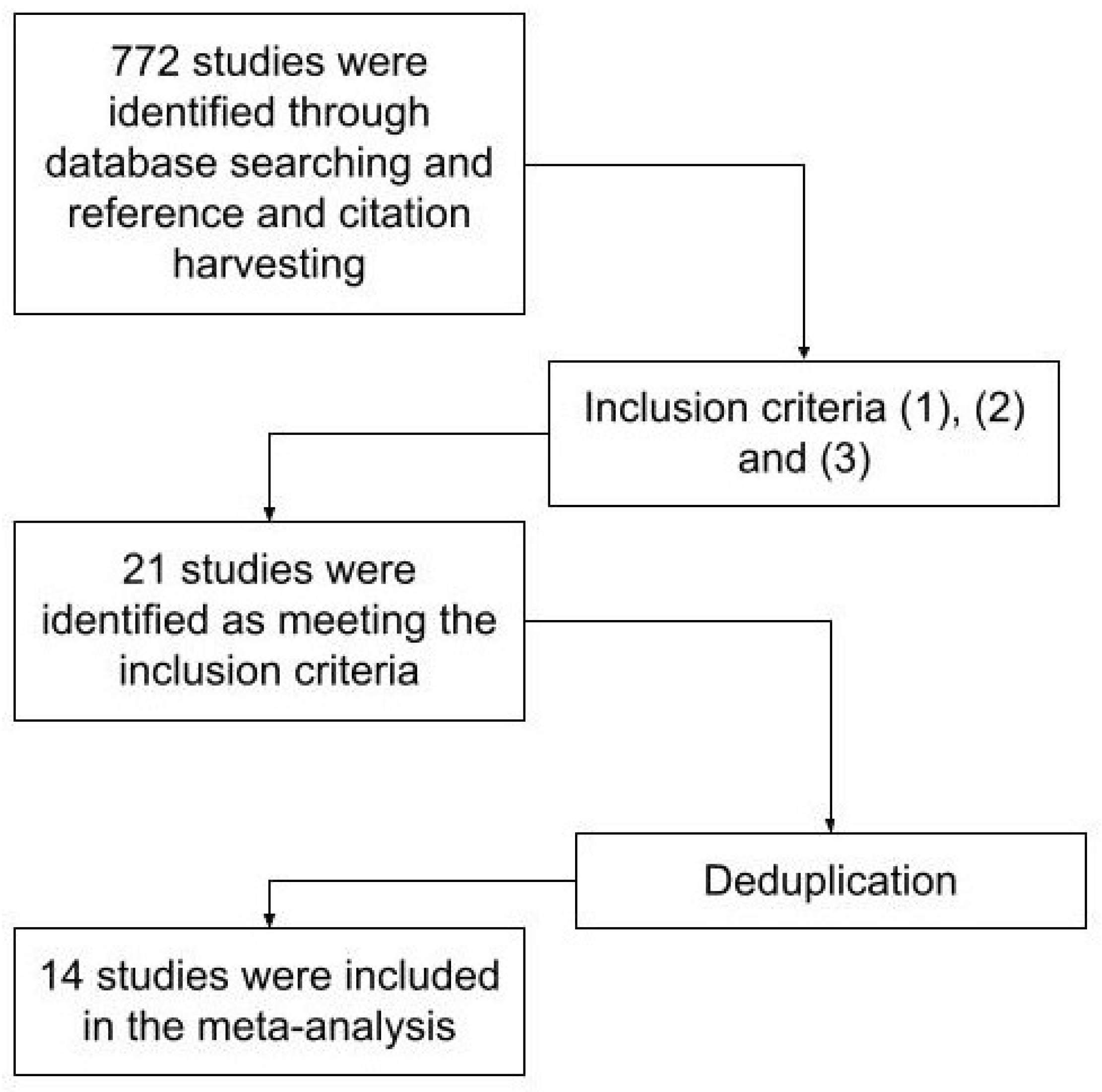
3.2. Meta-Analysis Procedure
- (1)
- Robot Type: humanoid or non-humanoid;
- (2)
- Participant Age Group: children or adults;
- (3)
- Assistive Activity Type: (a) information gathering (e.g., engaging in a conversation for the purpose of collecting information from participants), (b) prompting (e.g., providing verbal commands and asking participants to complete certain tasks), (c) facilitating (e.g., coaching and tutoring), (d) recognition (e.g., identifying information in the environment), and (e) answering (e.g., providing answers to the questions asked by the participants);
- (4)
- User Interaction Modes: (a) verbal (including spoken speech and speech-to-text input via a keyboard) and/or (b) non-verbal (e.g., object and/or touchscreen manipulation).
4. Meta-Analysis Results
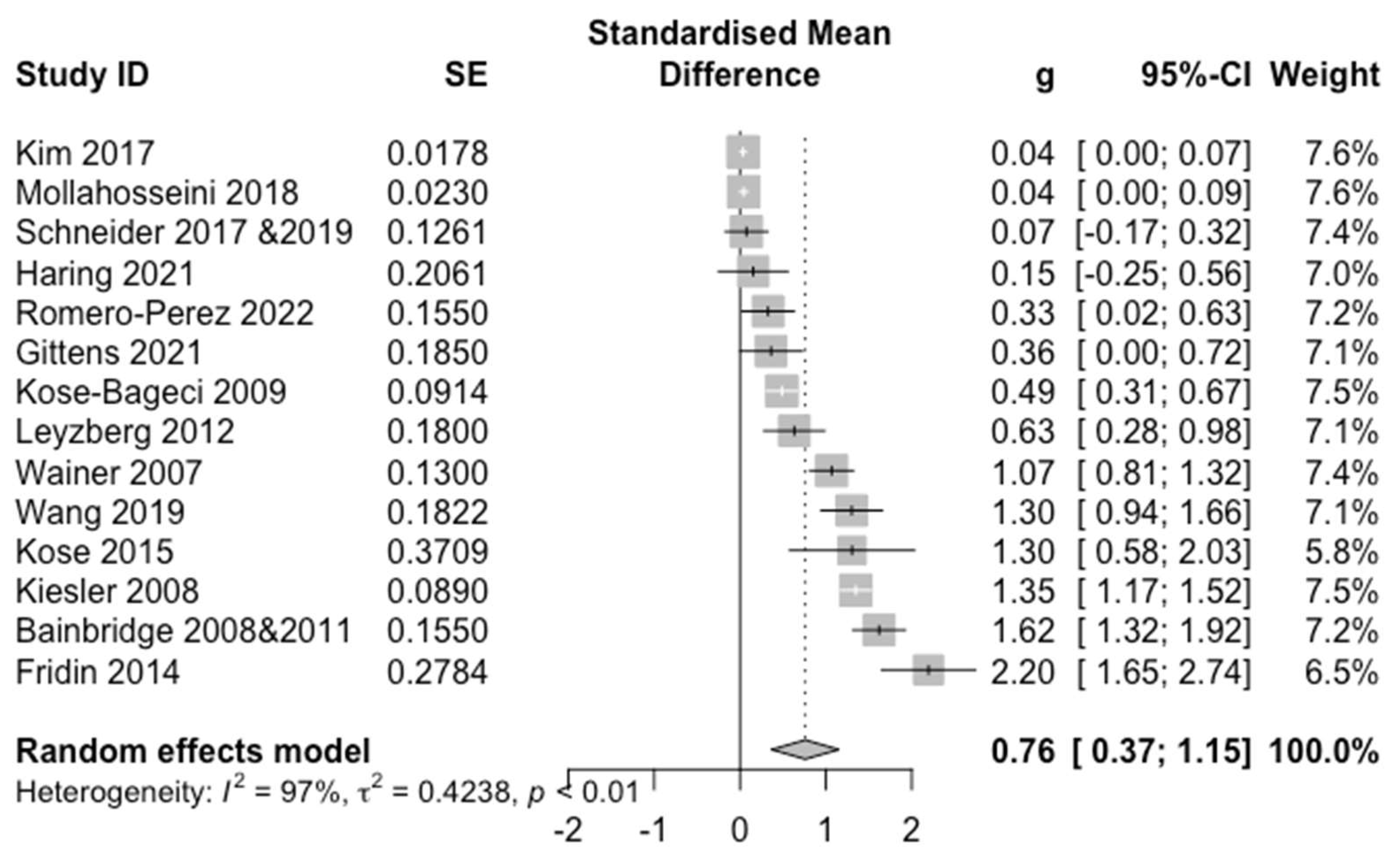
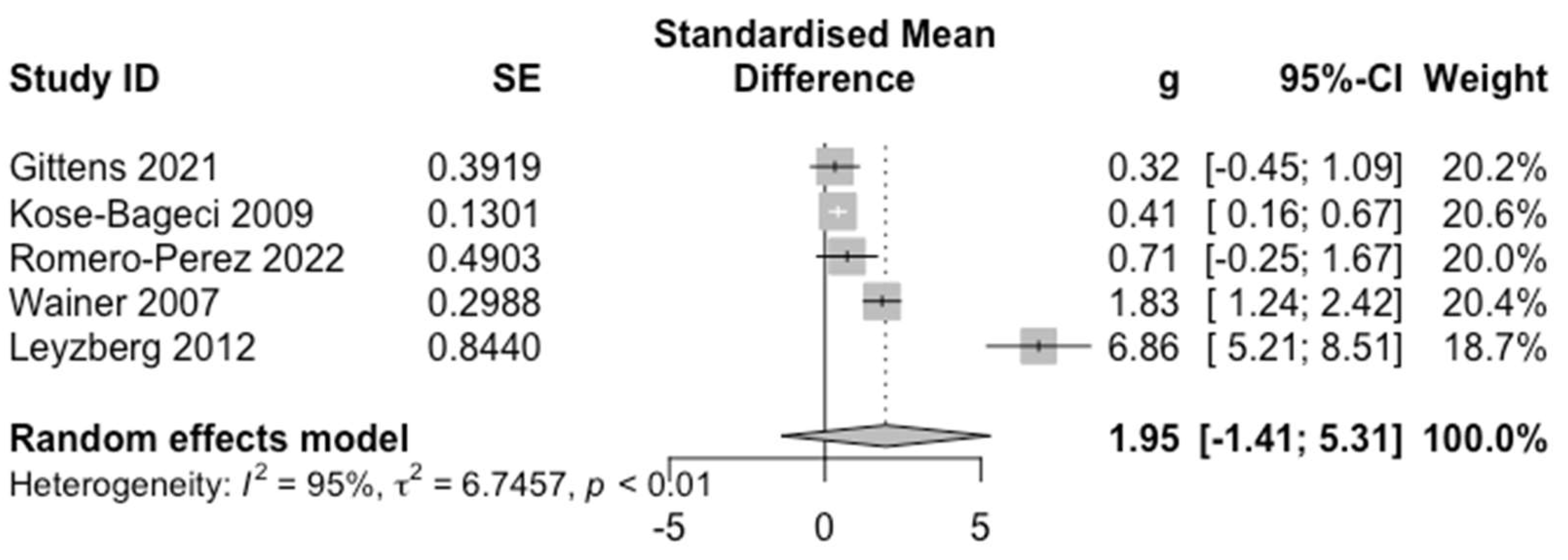
4.1. Overall Effect
4.2. Positive Experience
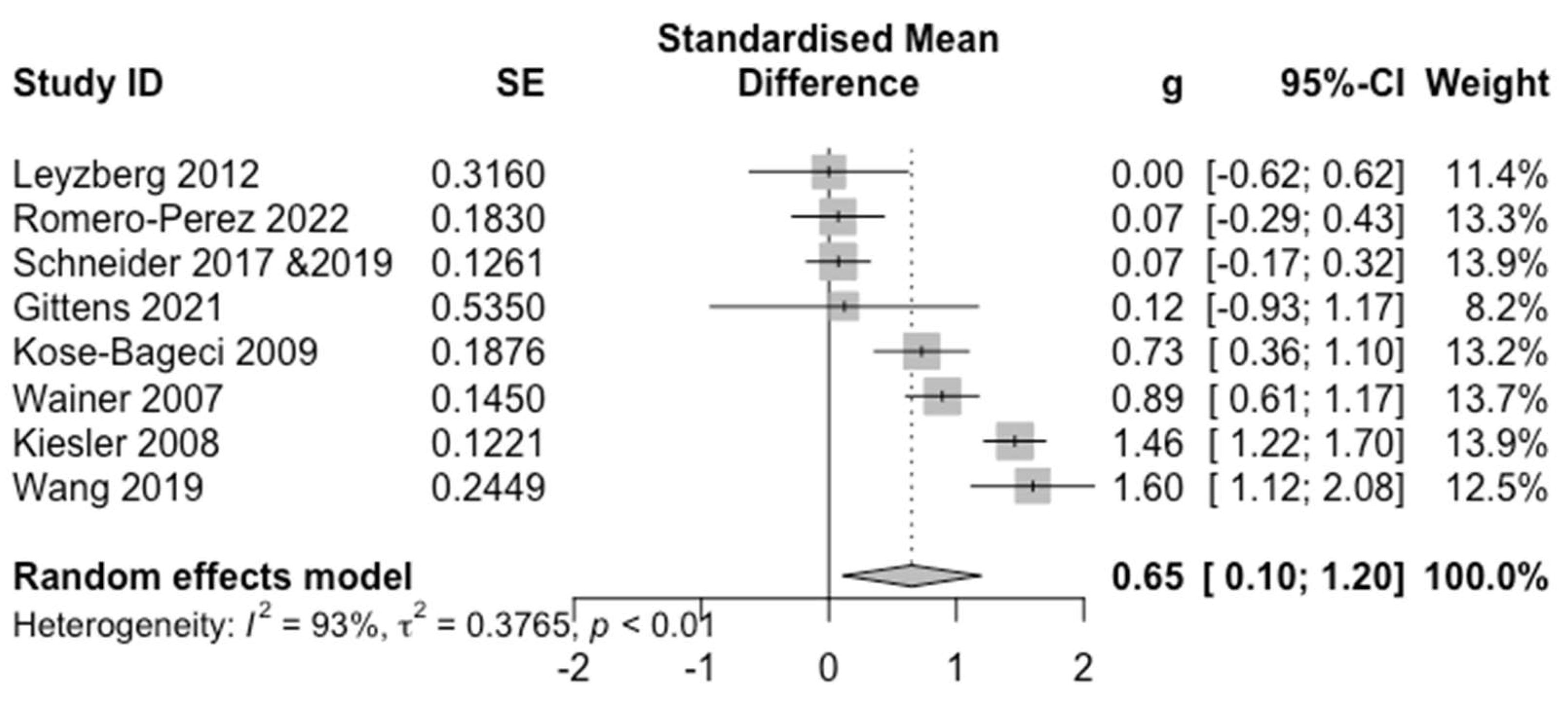
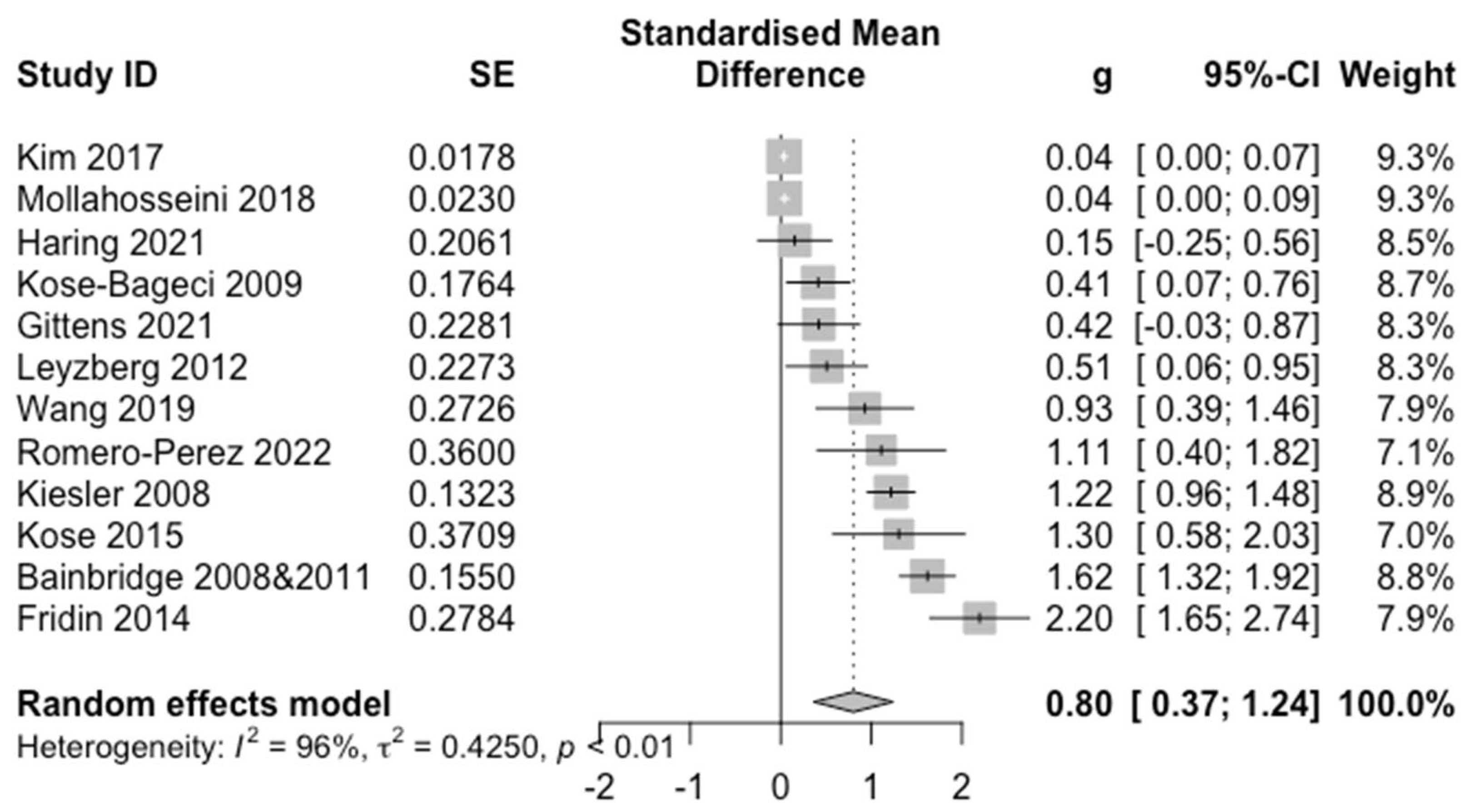
4.3. Perceptions and Attitudes
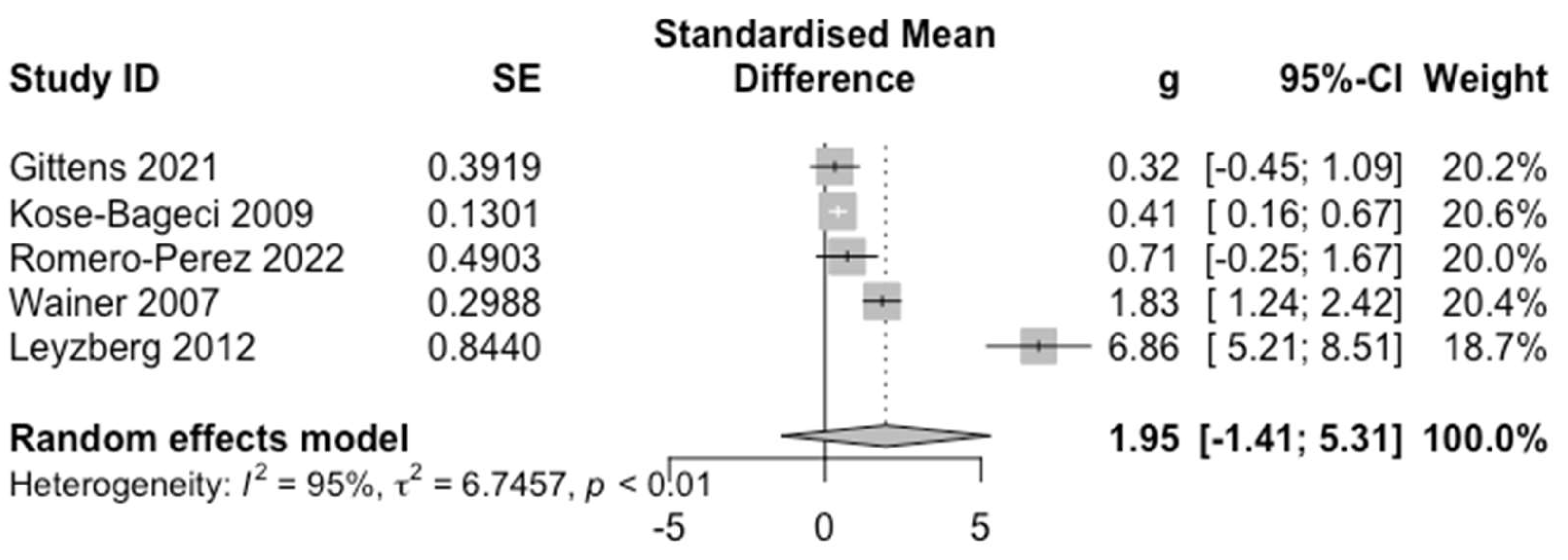
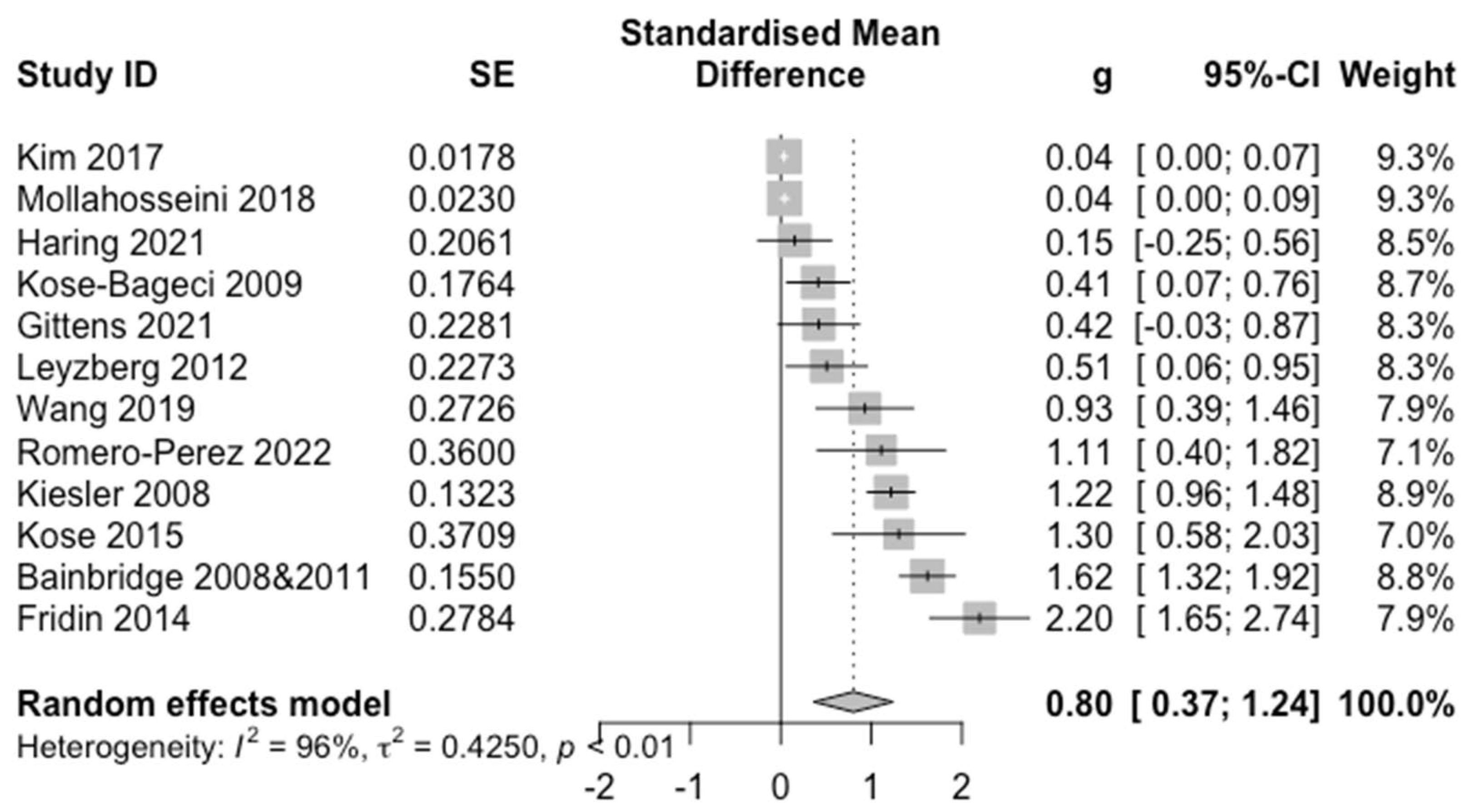
4.4. Efficacy
4.5. Quality of Evidence
5. Discussion
5.1. Insights
5.2. Considerations and Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sheridan, T.B. Human–Robot Interaction: Status and Challenges. Hum. Factors 2016, 58, 525–532. [Google Scholar] [CrossRef] [PubMed]
- Zacharaki, A.; Kostavelis, I.; Gasteratos, A.; Dokas, I. Safety Bounds in Human Robot Interaction: A Survey. Saf. Sci. 2020, 127, 104667. [Google Scholar] [CrossRef]
- Hancock, P.A.; Billings, D.R.; Schaefer, K.E.; Chen, J.Y.C.; de Visser, E.J.; Parasuraman, R. A Meta-Analysis of Factors Affecting Trust in Human-Robot Interaction. Hum. Factors 2011, 53, 517–527. [Google Scholar] [CrossRef]
- Broekens, J.; Heerink, M.; Rosendal, H. Assistive Social Robots in Elderly Care: A Review. Gerontechnology 2009, 8, 94–103. [Google Scholar] [CrossRef]
- Abdi, J.; Al-Hindawi, A.; Ng, T.; Vizcaychipi, M.P. Scoping Review on the Use of Socially Assistive Robot Technology in Elderly Care. BMJ Open 2018, 8, e018815. [Google Scholar] [CrossRef] [PubMed]
- Kachouie, R.; Sedighadeli, S.; Khosla, R.; Chu, M.-T. Socially Assistive Robots in Elderly Care: A Mixed-Method Systematic Literature Review. Int. J. Hum.–Comput. Interact. 2014, 30, 369–393. [Google Scholar] [CrossRef]
- Bovbel, P.; Nejat, G. Casper: An Assistive Kitchen Robot to Promote Aging in Place. J. Med. Device 2014, 8, 030945. [Google Scholar] [CrossRef]
- McColl, D.; Louie, W.-Y.G.; Nejat, G. Brian 2.1: A Socially Assistive Robot for the Elderly and Cognitively Impaired. IEEE Robot. Autom. Mag. 2013, 20, 74–83. [Google Scholar] [CrossRef]
- Moro, C.; Nejat, G.; Mihailidis, A. Learning and Personalizing Socially Assistive Robot Behaviors to Aid with Activities of Daily Living. J. Hum.-Robot Interact. 2018, 7, 1–25. [Google Scholar] [CrossRef]
- Robinson, F.; Cen, Z.; Naguib, H.; Nejat, G. Socially Assistive Robotics Using Wearable Sensors for User Dressing Assistance. In Proceedings of the IEEE International Symposium on Robot and Human Interactive Communication (RO-MAN), Naples, Italy, 29 August–2 September 2022. [Google Scholar]
- Abubshait, A.; Beatty, P.J.; McDonald, C.G.; Hassall, C.D.; Krigolson, O.E.; Wiese, E. A Win-Win Situation: Does Familiarity with a Social Robot Modulate Feedback Monitoring and Learning? Cogn. Affect. Behav. Neurosci. 2021, 21, 763–775. [Google Scholar] [CrossRef]
- Ribino, P.; Bonomolo, M.; Lodato, C.; Vitale, G. A Humanoid Social Robot Based Approach for Indoor Environment Quality Monitoring and Well-Being Improvement. Adv. Robot. 2021, 13, 277–296. [Google Scholar] [CrossRef]
- Wairagkar, M.; De Lima, M.R.; Harrison, M.; Batey, P.; Daniels, S.; Barnaghi, P.; Sharp, D.J.; Vaidyanathan, R. Conversational Artificial Intelligence and Affective Social Robot for Monitoring Health and Well-Being of People with Dementia. Alzheimers Dement. 2021, 17 (Suppl. S11), e053276. [Google Scholar] [CrossRef]
- Casaccia, S.; Revel, G.M.; Scalise, L.; Bevilacqua, R.; Rossi, L.; Paauwe, R.A.; Karkowsky, I.; Ercoli, I.; Artur Serrano, J.; Suijkerbuijk, S.; et al. Social Robot and Sensor Network in Support of Activity of Daily Living for People with Dementia. In Proceedings of the Dementia Lab 2019. Making Design Work: Engaging with Dementia in Context, Eindhoven, The Netherlands, 21–22 October 2019; Springer International Publishing: Berlin/Heidelberg, Germany, 2019; pp. 128–135. [Google Scholar]
- Cooper, S.; Lemaignan, S. Towards Using Behaviour Trees for Long-Term Social Robot Behaviour. In Proceedings of the HRI ’22: ACM/IEEE International Conference on Human-Robot Interaction, Sapporo, Hokkaido, Japan, 7–10 March 2022. [Google Scholar]
- Hsu, K.-H.; Tsai, W.-S.; Yang, H.-F.; Huang, L.-Y.; Zhuang, W.-H. On the Design of Cross-Platform Social Robots: A Multi-Purpose Reminder Robot as an Example. In Proceedings of the 2017 International Conference on Applied System Innovation (ICASI), Sapporo, Japan, 13–17 May 2017; IEEE: Piscataway, NJ, USA; pp. 256–259. [Google Scholar]
- Matarić, M.J.; Eriksson, J.; Feil-Seifer, D.J.; Winstein, C.J. Socially Assistive Robotics for Post-Stroke Rehabilitation. J. Neuroeng. Rehabil. 2007, 4, 5. [Google Scholar] [CrossRef] [PubMed]
- Malik, N.A.; Hanapiah, F.A.; Rahman, R.A.A.; Yussof, H. Emergence of Socially Assistive Robotics in Rehabilitation for Children with Cerebral Palsy: A Review. Int. J. Adv. Rob. Syst. 2016, 13, 135. [Google Scholar] [CrossRef]
- Céspedes, N.; Irfan, B.; Senft, E.; Cifuentes, C.A.; Gutierrez, L.F.; Rincon-Roncancio, M.; Belpaeme, T.; Múnera, M. A Socially Assistive Robot for Long-Term Cardiac Rehabilitation in the Real World. Front. Neurorobot. 2021, 15, 633248. [Google Scholar] [CrossRef]
- Cho, S.-J.; Ahn, D.H. Socially Assistive Robotics in Autism Spectrum Disorder. Hanyang Med. Rev. 2016, 36, 17. [Google Scholar] [CrossRef]
- Feil-Seifer, D.; Matarić, M.J. Toward Socially Assistive Robotics for Augmenting Interventions for Children with Autism Spectrum Disorders. In Proceedings of the Experimental Robotics; Springer: Berlin/Heidelberg, Germany, 2009; pp. 201–210. [Google Scholar]
- Dickstein-Fischer, L. Socially Assistive Robots: Current Status and Future Prospects for Autism Interventions. Innov. Impact 2018, 5, 15–25. [Google Scholar] [CrossRef]
- Getson, C.; Nejat, G. Socially Assistive Robots Helping Older Adults through the Pandemic and Life after COVID-19. Robotics 2021, 10, 106. [Google Scholar] [CrossRef]
- Kanero, J.; Tunalı, E.T.; Oranç, C.; Göksun, T.; Küntay, A.C. When Even a Robot Tutor Zooms: A Study of Embodiment, Attitudes, and Impressions. Front. Robot. AI 2021, 8, 679893. [Google Scholar] [CrossRef]
- Romero-Pérez, S.; Smith-Arias, K.; Corrales-Cortés, L.; Ramírez-Benavides, K.; Vega, A.; Mora, A. Evaluating Virtual and Local Pepper Presence in the Role of Communicator Interacting with Another Human Presenter at a Vocational Fair of Computer Sciences. In Proceedings of the Human-Computer Interaction. Technological Innovation; Springer International Publishing: Berlin/Heidelberg, Germany, 2022; pp. 580–589. [Google Scholar]
- Lytridis, C.; Bazinas, C.; Sidiropoulos, G.; Papakostas, G.A.; Kaburlasos, V.G.; Nikopoulou, V.-A.; Holeva, V.; Evangeliou, A. Distance Special Education Delivery by Social Robots. Electronics 2020, 9, 1034. [Google Scholar] [CrossRef]
- Urdanivia Alarcon, D.A.; Cano, S.; Paucar, F.H.R.; Quispe, R.F.P.; Talavera-Mendoza, F.; Zegarra, M.E.R. Exploring the Effect of Robot-Based Video Interventions for Children with Autism Spectrum Disorder as an Alternative to Remote Education. Electronics 2021, 10, 2577. [Google Scholar] [CrossRef]
- Philip, K.E.J.; Polkey, M.I.; Hopkinson, N.S.; Steptoe, A.; Fancourt, D. Social Isolation, Loneliness and Physical Performance in Older-Adults: Fixed Effects Analyses of a Cohort Study. Sci. Rep. 2020, 10, 13908. [Google Scholar] [CrossRef] [PubMed]
- Isabet, B.; Pino, M.; Lewis, M.; Benveniste, S.; Rigaud, A.-S. Social Telepresence Robots: A Narrative Review of Experiments Involving Older Adults before and during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 3597. [Google Scholar] [CrossRef] [PubMed]
- Li, J. The Benefit of Being Physically Present: A Survey of Experimental Works Comparing Copresent Robots, Telepresent Robots and Virtual Agents. Int. J. Hum. Comput. Stud. 2015, 77, 23–37. [Google Scholar] [CrossRef]
- Goodrich, M.A.; Schultz, A.C. Human-Robot Interaction: A Survey; Now Publishers Inc.: Delft, The Netherlands, 2008; ISBN 9781601980922. [Google Scholar]
- Kidd, C.D.; Breazeal, C. Effect of a Robot on User Perceptions. In Proceedings of the 2004 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS) (IEEE Cat. No.04CH37566), Sendai, Japan, 28 September–2 October 2004; Volume 4, pp. 3559–3564. [Google Scholar]
- Kose-Bagci, H.; Ferrari, E.; Dautenhahn, K.; Syrdal, D.S.; Nehaniv, C.L. Effects of Embodiment and Gestures on Social Interaction in Drumming Games with a Humanoid Robot. Adv. Robot. 2009, 23, 1951–1996. [Google Scholar] [CrossRef]
- Mollahosseini, A.; Abdollahi, H.; Sweeny, T.D.; Cole, R.; Mahoor, M.H. Role of Embodiment and Presence in Human Perception of Robots’ Facial Cues. Int. J. Hum. Comput. Stud. 2018, 116, 25–39. [Google Scholar] [CrossRef]
- Schneider, S.; Kummert, F. Does the User’s Evaluation of a Socially Assistive Robot Change Based on Presence and Companionship Type? In Proceedings of the Companion of the 2017 ACM/IEEE International Conference on Human-Robot Interaction, Vienna, Austria, 6–9 March 2017; Association for Computing Machinery: New York, NY, USA, 2017; pp. 277–278. [Google Scholar]
- Gittens, C.L. Remote HRI: A Methodology for Maintaining COVID-19 Physical Distancing and Human Interaction Requirements in HRI Studies. Inf. Syst. Front. 2021, 1–16. [Google Scholar] [CrossRef]
- Balasubramanian, S. The Healthcare Industry Is Crumbling Due to Staffing Shortages. Forbes Magazine, 22 December 2022. [Google Scholar]
- Hospitals Are under “unprecedented” Strain from Staff Shortages, Says Ontario Health VP. CBC News, 4 August 2022.
- Fox, C. Unions Say Hospital Staffing Shortages Are Impacting Patient Care. Available online: https://toronto.ctvnews.ca/unions-say-hospital-staffing-shortages-are-impacting-patient-care-1.6015905 (accessed on 1 September 2022).
- Rosella, L.C.; Fitzpatrick, T.; Wodchis, W.P.; Calzavara, A.; Manson, H.; Goel, V. High-Cost Health Care Users in Ontario, Canada: Demographic, Socio-Economic, and Health Status Characteristics. BMC Health Serv. Res. 2014, 14, 532. [Google Scholar] [CrossRef]
- Rais, S.; Nazerian, A.; Ardal, S.; Chechulin, Y.; Bains, N.; Malikov, K. High-Cost Users of Ontario’s Healthcare Services. Healthc. Policy 2013, 9, 44–51. [Google Scholar] [CrossRef]
- 4Understanding Why Health Care Costs in the U.S. Are so High. Available online: https://www.hsph.harvard.edu/news/hsph-in-the-news/understanding-why-health-care-costs-in-the-u-s-are-so-high/ (accessed on 9 September 2022).
- Hendry, L. Hospitals Facing Greater Workload amid Staff Shortage, Growing Fatigue. Available online: https://www.intelligencer.ca/news/hospitals-facing-greater-workload-amid-staff-shortage-growing-fatigue (accessed on 8 September 2022).
- Benchetrit, J. Heavy Workload, Fatigue Hit Pharmacists Like Never before in Rush for COVID Tests, Vaccines. CBC News, 23 December 2021. [Google Scholar]
- Sikaras, C.; Ilias, I.; Tselebis, A.; Pachi, A.; Zyga, S.; Tsironi, M.; Gil, A.P.R.; Panagiotou, A. Nursing Staff Fatigue and Burnout during the COVID-19 Pandemic in Greece. AIMS Public Health 2022, 9, 94–105. [Google Scholar] [CrossRef]
- Kim, K.; Nagendran, A.; Bailenson, J.N.; Raij, A.; Bruder, G.; Lee, M.; Schubert, R.; Yan, X.; Welch, G.F. A Large-Scale Study of Surrogate Physicality and Gesturing on Human–Surrogate Interactions in a Public Space. Front. Robot. AI 2017, 4, 32. [Google Scholar] [CrossRef]
- Van der Drift, E.J.G.; Beun, R.-J.; Looije, R.; Blanson Henkemans, O.A.; Neerincx, M.A. A Remote Social Robot to Motivate and Support Diabetic Children in Keeping a Diary. In Proceedings of the 2014 ACM/IEEE International Conference on Human-Robot Interaction, Bielefeld, Germany, 3–6 March 2014; Association for Computing Machinery: New York, NY, USA, 2014; pp. 463–470. [Google Scholar]
- Kiesler, S.; Powers, A.; Fussell, S.R.; Torrey, C. Anthropomorphic interactions with a robot and robot–like agent. Soc. Cogn. 2008, 26, 169–181. [Google Scholar] [CrossRef]
- Wainer, J.; Feil-Seifer, D.J.; Shell, D.A.; Mataric, M.J. Embodiment and Human-Robot Interaction: A Task-Based Perspective. In Proceedings of the RO-MAN 2007—The 16th IEEE International Symposium on Robot and Human Interactive Communication, Jeju, Korea, 26–29 August 2007; pp. 872–877. [Google Scholar]
- Leyzberg, D.; Spaulding, S.; Toneva, M.; Scassellati, B. The Physical Presence of a Robot Tutor Increases Cognitive Learning Gains. Proc. Annu. Meet. Cogn. Sci. Soc. 2012, 34, 1882–1887. [Google Scholar]
- Fridin, M.; Belokopytov, M. Embodied Robot versus Virtual Agent: Involvement of Preschool Children in Motor Task Performance. Int. J. Hum.–Comput. Interact. 2014, 30, 459–469. [Google Scholar] [CrossRef]
- Köse, H.; Uluer, P.; Akalın, N.; Yorgancı, R.; Özkul, A.; Ince, G. The Effect of Embodiment in Sign Language Tutoring with Assistive Humanoid Robots. Int. J. Soc. Robot. 2015, 7, 537–548. [Google Scholar] [CrossRef]
- Haring, K.S.; Satterfield, K.M.; Tossell, C.C.; de Visser, E.J.; Lyons, J.R.; Mancuso, V.F.; Finomore, V.S.; Funke, G.J. Robot Authority in Human-Robot Teaming: Effects of Human-Likeness and Physical Embodiment on Compliance. Front. Psychol. 2021, 12, 625713. [Google Scholar] [CrossRef]
- Bainbridge, W.A.; Hart, J.; Kim, E.S.; Scassellati, B. The Effect of Presence on Human-Robot Interaction. In Proceedings of the RO-MAN 2008—The 17th IEEE International Symposium on Robot and Human Interactive Communication, Munich, Germany, 1–3 August 2008; IEEE: Piscataway, NJ, USA, 2008; pp. 701–706. [Google Scholar]
- Wang, B.; Rau, P.-L.P. Influence of Embodiment and Substrate of Social Robots on Users’ Decision-Making and Attitude. Adv. Robot. 2019, 11, 411–421. [Google Scholar] [CrossRef]
- Van der Loos, H.F.M.; Reinkensmeyer, D.J.; Guglielmelli, E. Rehabilitation and Health Care Robotics. In Springer Handbook of Robotics; Siciliano, B., Khatib, O., Eds.; Springer International Publishing: Cham, Switzerland, 2016; pp. 1685–1728. ISBN 9783319325521. [Google Scholar]
- Robinson, N.L.; Connolly, J.; Hides, L.; Kavanagh, D.J. A Social Robot to Deliver an 8-Week Intervention for Diabetes Management: Initial Test of Feasibility in a Hospital Clinic. In Proceedings of the Social Robotics; Springer International Publishing: Berlin/Heidelberg, Germany, 2020; pp. 628–639. [Google Scholar]
- Ikeuchi, T.; Sakurai, R.; Furuta, K.; Kasahara, Y.; Imamura, Y.; Shinkai, S. Utilizing social robot to reduce workload of healthcare professionals in psychiatric hospital: A preliminary study. Innov. Aging 2018, 2, 695–696. [Google Scholar] [CrossRef]
- Begum, M.; Serna, R.W.; Yanco, H.A. Are Robots Ready to Deliver Autism Interventions? A Comprehensive Review. Adv. Robot. 2016, 8, 157–181. [Google Scholar] [CrossRef]
- Thompson, C.; Mohamed, S.; Louie, W.-Y.G.; He, J.C.; Li, J.; Nejat, G. The Robot Tangy Facilitating Trivia Games: A Team-Based User-Study with Long-Term Care Residents. In Proceedings of the 2017 IEEE International Symposium on Robotics and Intelligent Sensors (IRIS), Ottawa, ON, Canada, 5–7 October 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 173–178. [Google Scholar]
- Louie, W.-Y.G.; Nejat, G. A Social Robot Learning to Facilitate an Assistive Group-Based Activity from Non-Expert Caregivers. Int. J. Soc. Robot. 2020, 12, 1159–1176. [Google Scholar] [CrossRef]
- Rosenthal-von der Pütten, A.M.; Krämer, N.C.; Hoffmann, L.; Sobieraj, S.; Eimler, S.C. An Experimental Study on Emotional Reactions Towards a Robot. Int. J. Soc. Robot. 2013, 5, 17–34. [Google Scholar] [CrossRef]
- Bainbridge, W.A.; Hart, J.W.; Kim, E.S.; Scassellati, B. The Benefits of Interactions with Physically Present Robots over Video-Displayed Agents. Adv. Robot. 2011, 3, 41–52. [Google Scholar] [CrossRef]
- Schneider, S. Socially Assistive Robots for Exercising Scenarios. Studies on Group Effects, Feedback, Embodiment and Adaption. Ph.D. Thesis, Bielefeld University, Bielefeld, Germany, 2019. [Google Scholar]
- Lo, S.-Y.; Lai, Y.-Y.; Liu, J.-C.; Yeh, S.-L. Robots and Sustainability: Robots as Persuaders to Promote Recycling. Int. J. Soc. Robot. 2022, 14, 1261–1272. [Google Scholar] [CrossRef]
- Naneva, S.; Sarda Gou, M.; Webb, T.L.; Prescott, T.J. A Systematic Review of Attitudes, Anxiety, Acceptance, and Trust Towards Social Robots. Int. J. Soc. Robot. 2020, 12, 1179–1201. [Google Scholar] [CrossRef]
- Harrer, M.; Cuijpers, P.; Furukawa, T.A.; Ebert, D.D. Doing Meta-Analysis with R: A Hands-On Guide; Chapman and Hall/CRC: Boca Raton, FL, USA, 2021. [Google Scholar]
- Marín-Martínez, F.; Sánchez-Meca, J. Weighting by Inverse Variance or by Sample Size in Random-Effects Meta-Analysis. Educ. Psychol. Meas. 2010, 70, 56–73. [Google Scholar] [CrossRef]
- Balduzzi, S.; Rücker, G.; Schwarzer, G. How to Perform a Meta-Analysis with R: A Practical Tutorial. Evid. Based Ment. Health 2019, 22, 153–160. [Google Scholar] [CrossRef]
- Guyatt, G.; Oxman, A.D.; Akl, E.A.; Kunz, R.; Vist, G.; Brozek, J.; Norris, S.; Falck-Ytter, Y.; Glasziou, P.; deBeer, H.; et al. GRADE Guidelines: 1. Introduction—GRADE Evidence Profiles and Summary of Findings Tables. J. Clin. Epidemiol. 2011, 64, 383–394. [Google Scholar] [CrossRef]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in Meta-Analysis Detected by a Simple, Graphical Test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef]
- Esterwood, C.; Essenmacher, K.; Yang, H.; Zeng, F.; Robert, L.P. A Meta-Analysis of Human Personality and Robot Acceptance in Human-Robot Interaction. In Proceedings of the 2021 CHI Conference on Human Factors in Computing Systems, Yokohama, Japan, 8–13 May 2021; Association for Computing Machinery: New York, NY, USA, 2021; pp. 1–18. [Google Scholar]
- Roesler, E.; Manzey, D.; Onnasch, L. A Meta-Analysis on the Effectiveness of Anthropomorphism in Human-Robot Interaction. Sci. Robot. 2021, 6, eabj5425. [Google Scholar] [CrossRef]
- Matsusaka, Y.; Tojo, T.; Kobayashi, T. Conversation Robot Participating in Group Conversation. IEICE Trans. Inf. Syst. 2003, 86, 26–36. [Google Scholar]
- Robinson, H.; Macdonald, B.; Kerse, N.; Broadbent, E. The Psychosocial Effects of a Companion Robot: A Randomized Controlled Trial. J. Am. Med. Dir. Assoc. 2013, 14, 661–667. [Google Scholar] [CrossRef] [PubMed]
- Liu, O.; Rakita, D.; Mutlu, B.; Gleicher, M. Understanding Human-Robot Interaction in Virtual Reality. In Proceedings of the 2017 26th IEEE International Symposium on Robot and Human Interactive Communication (RO-MAN), Lisbon, Portugal, 28 August–1 September 2017; IEEE: Piscataway, NJ, USA, 2017; pp. 751–757. [Google Scholar]
- Mara, M.; Stein, J.-P.; Latoschik, M.E.; Lugrin, B.; Schreiner, C.; Hostettler, R.; Appel, M. User Responses to a Humanoid Robot Observed in Real Life, Virtual Reality, 3D and 2D. Front. Psychol. 2021, 12, 633178. [Google Scholar] [CrossRef] [PubMed]
- Moeyaert, M.; Ugille, M.; Natasha Beretvas, S.; Ferron, J.; Bunuan, R.; Van den Noortgate, W. Methods for Dealing with Multiple Outcomes in Meta-Analysis: A Comparison between Averaging Effect Sizes, Robust Variance Estimation and Multilevel Meta-Analysis. Int. J. Soc. Res. Methodol. 2017, 20, 559–572. [Google Scholar] [CrossRef]
- Hancock, P.A.; Kessler, T.T.; Kaplan, A.D.; Brill, J.C.; Szalma, J.L. Evolving Trust in Robots: Specification Through Sequential and Comparative Meta-Analyses. Hum. Factors 2021, 63, 1196–1229. [Google Scholar] [CrossRef]
- Esterwood, C.; Essenmacher, K.; Yang, H.; Zeng, F.; Robert, L.P. A Personable Robot: Meta-Analysis of Robot Personality and Human Acceptance. IEEE Robot. Autom. Lett. 2022, 7, 6918–6925. [Google Scholar] [CrossRef]
- Weiss, A.; Bartneck, C. Meta Analysis of the Usage of the Godspeed Questionnaire Series. In Proceedings of the 2015 24th IEEE International Symposium on Robot and Human Interactive Communication (RO-MAN), Kobe, Japan, 31 August–4 September 2015; IEEE: Piscataway, NJ, USA, 2015; pp. 381–388. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study ID | Robot Type | # of Participants | Participant Age Group | Activity | User Interaction Modes |
|---|---|---|---|---|---|
| Wainer 2007 [49] | Non-humanoid ActivMedia Pioneer 2 DX, courtesy of Maja J. Matarić [49] | 21 | Adults | Facilitating | Non-verbal |
| Kiesler 2008 [48] | Humanoid Pearl robot, courtesy of National Science Foundation | 113 | Adults | Information gathering | Verbal |
| Bainbridge 2008 & 2011 [54,63] | Humanoid Nico robot, courtesy of Brian Scassellati [54] | 65 | Adults | Prompting | Non-verbal |
| Leyzberg 2012 [50] | Non-humanoid Keepon, courtesy of Brian Scassellati [50] | 100 | Adults | Facilitating | Non-verbal |
| Kose-Bageci 2009 [33] | Humanoid Kaspar robot, courtesy of Kose-Bageci et al. [33] | 100 | Children | Facilitating | Non-verbal |
| Fridin 2014 [51] | Humanoid NAO robot, courtesy of ASBLab | 9 | Children | Prompting | Non-verbal |
| Schneider 2017 & 2019 [35,64] | Humanoid NAO robot, courtesy of ASBLab | 90 | Adults | Prompting | Non-verbal |
| Kim 2017 [46] | Humanoid robot RoboThespian robot, courtesy of Kim et al. [46] | 7685 | Adults | Prompting | Verbal |
| Gittens 2021 [36] | Non-humanoid Zenbo robot [65], under a Creative Commons Attribution 4.0 International License | 10 | Adults | Information gathering | Verbal |
| Kose 2015 [52] | Humanoid Robovie R3 robot, courtesy of Kose et al. [52] | 31 | Children | Facilitating | Non-verbal |
| Haring 2021 [53] | Humanoid Nao robot, courtesy of ASBLab | 60 | Adults | Facilitating | Non-verbal |
| Wang 2019 [55] | Humanoid Nao robot, courtesy of ASBLab | 60 | Adults | Information gathering | Verbal |
| Mollahosseini 2018 [34] | Humanoid Ryan robot, courtesy of Mollahosseini et al. [34] | 17 | Adults | Recognition | Non-verbal |
| Romero-Perez 2022 [25] | Humanoid Pepper robot, Nao robot, courtesy of ASBLab | 18 | Children | Answering | Verbal |
| Outcome Classes | Related Research Question |
|---|---|
| Positive experience (PE): user experience during interactions including pleasure and enjoyment. | Do humans have a better experience with in-person HRI or remote HRI? |
| Perceptions and Attitudes towards the robots (PA): likeability and intelligence, helpfulness, human-likeness, trust, acceptance, respect and ease of use. | Do humans perceive robots differently under the in-person and remote conditions? |
| Efficacy (EF): user performance measures including task performance, activity level, workload, compliance, ability and robot influence. Robot performance measures including social presence and competence. | Does HRI performance differ under in-person and remote conditions? |
| Outcome | Risk of Bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Quality of Evidence |
|---|---|---|---|---|---|---|
| Overall | Not serious | Not serious | Not serious | Not serious | Serious | Moderate |
| PE | Not serious | Not serious | Not serious | Serious | Serious | Low |
| PA | Not serious | Not serious | Not serious | Not serious | Serious | Moderate |
| EF | Not serious | Not serious | Not serious | Not serious | Serious | Moderate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liang, N.; Nejat, G. A Meta-Analysis on Remote HRI and In-Person HRI: What Is a Socially Assistive Robot to Do? Sensors 2022, 22, 7155. https://doi.org/10.3390/s22197155
Liang N, Nejat G. A Meta-Analysis on Remote HRI and In-Person HRI: What Is a Socially Assistive Robot to Do? Sensors. 2022; 22(19):7155. https://doi.org/10.3390/s22197155
Chicago/Turabian StyleLiang, Nan, and Goldie Nejat. 2022. "A Meta-Analysis on Remote HRI and In-Person HRI: What Is a Socially Assistive Robot to Do?" Sensors 22, no. 19: 7155. https://doi.org/10.3390/s22197155
APA StyleLiang, N., & Nejat, G. (2022). A Meta-Analysis on Remote HRI and In-Person HRI: What Is a Socially Assistive Robot to Do? Sensors, 22(19), 7155. https://doi.org/10.3390/s22197155