
Smart Diagnostics: Combining Artificial Intelligence and In Vitro Diagnostics



Abstract
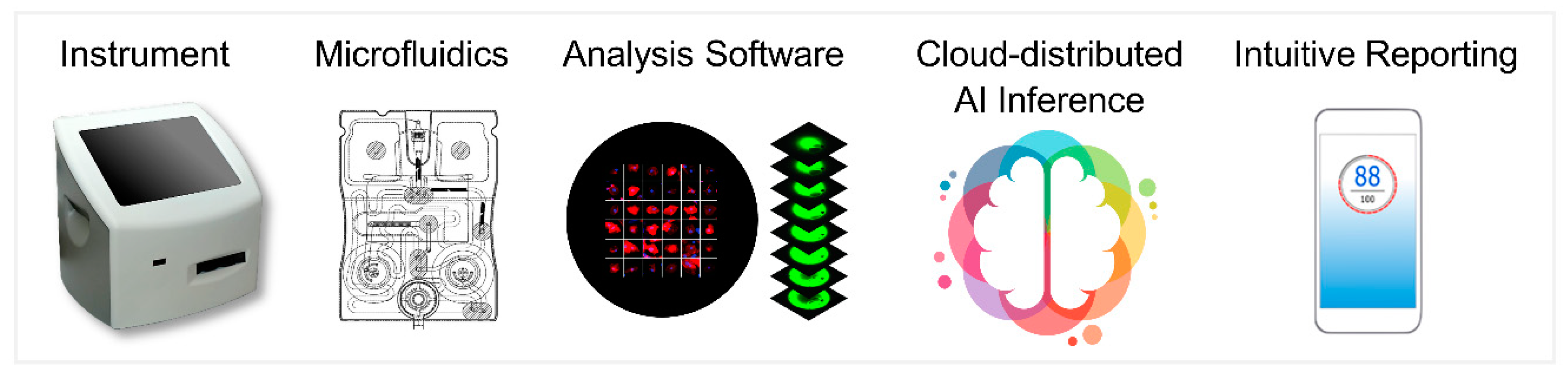
:1. Introduction
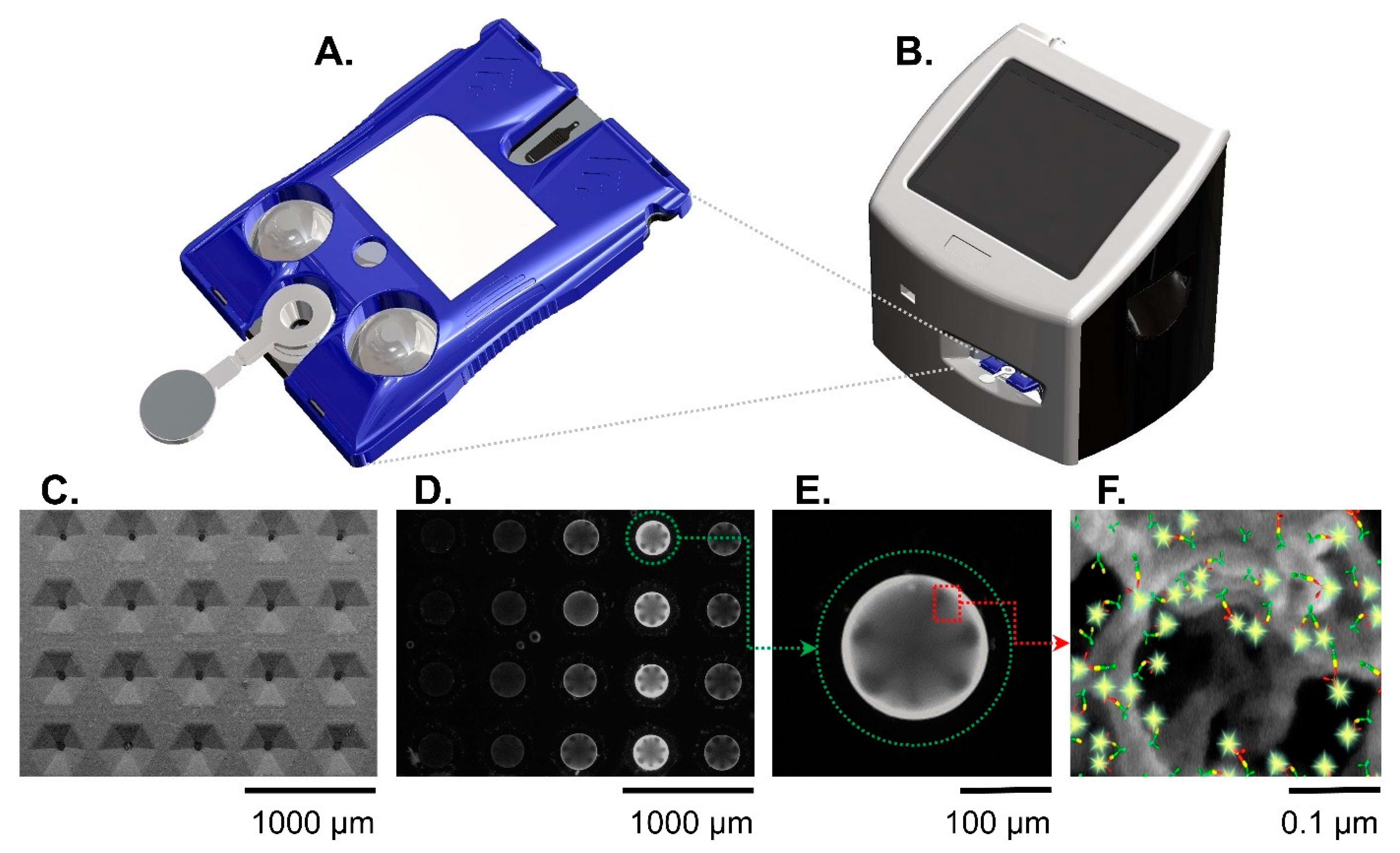
- A universal instrumentation platform that can facilitate a multitude of diagnostic tests;
- Highly scalable biosensors supported by microfluidics for assay processing;
- Analysis software for digitizing chemistry/biology;
- AI inference and clinical decision support;
- Intuitive reporting and integration with electronic health records.
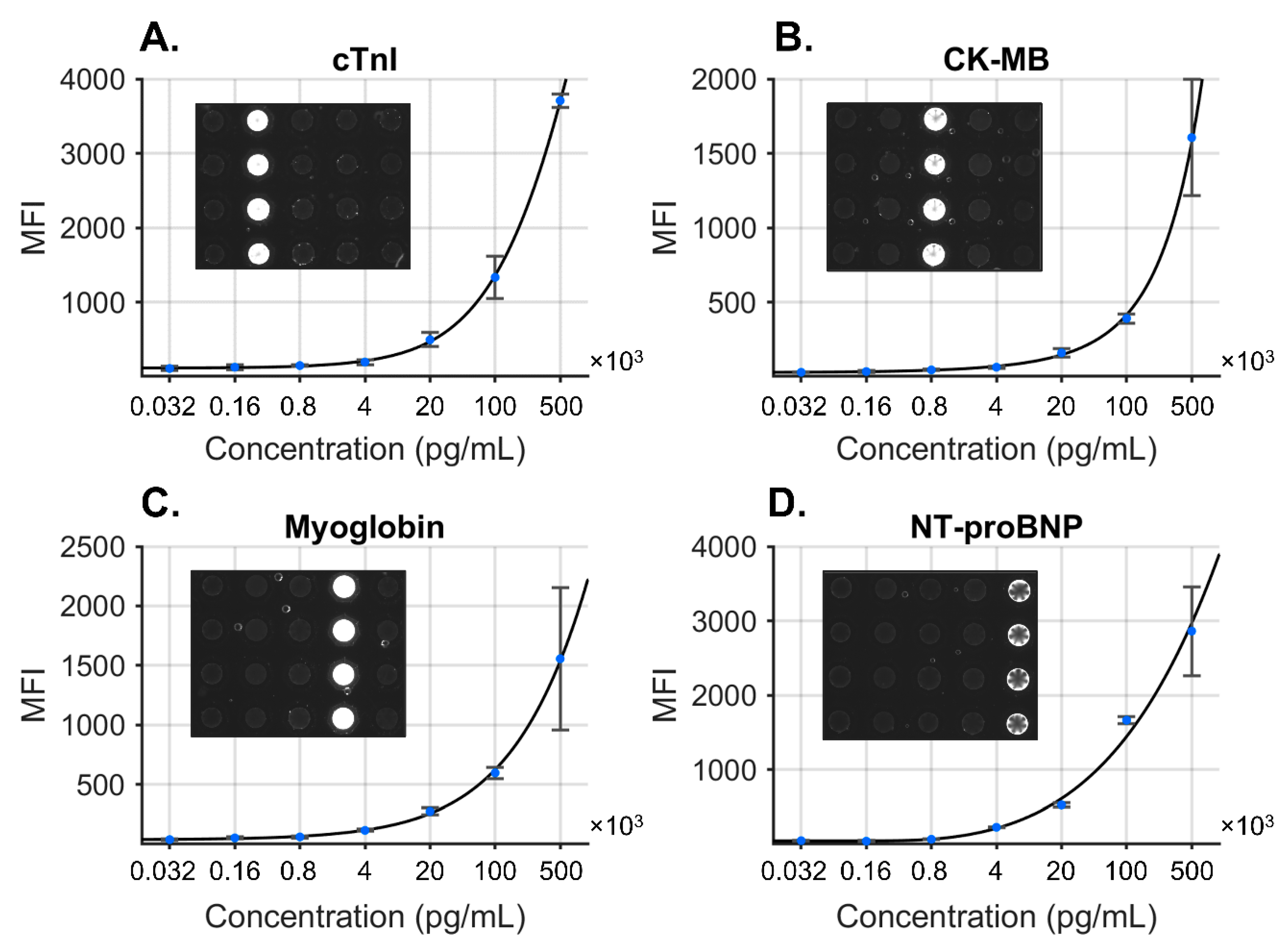
2. Smart Diagnostics for Cardiovascular Disease
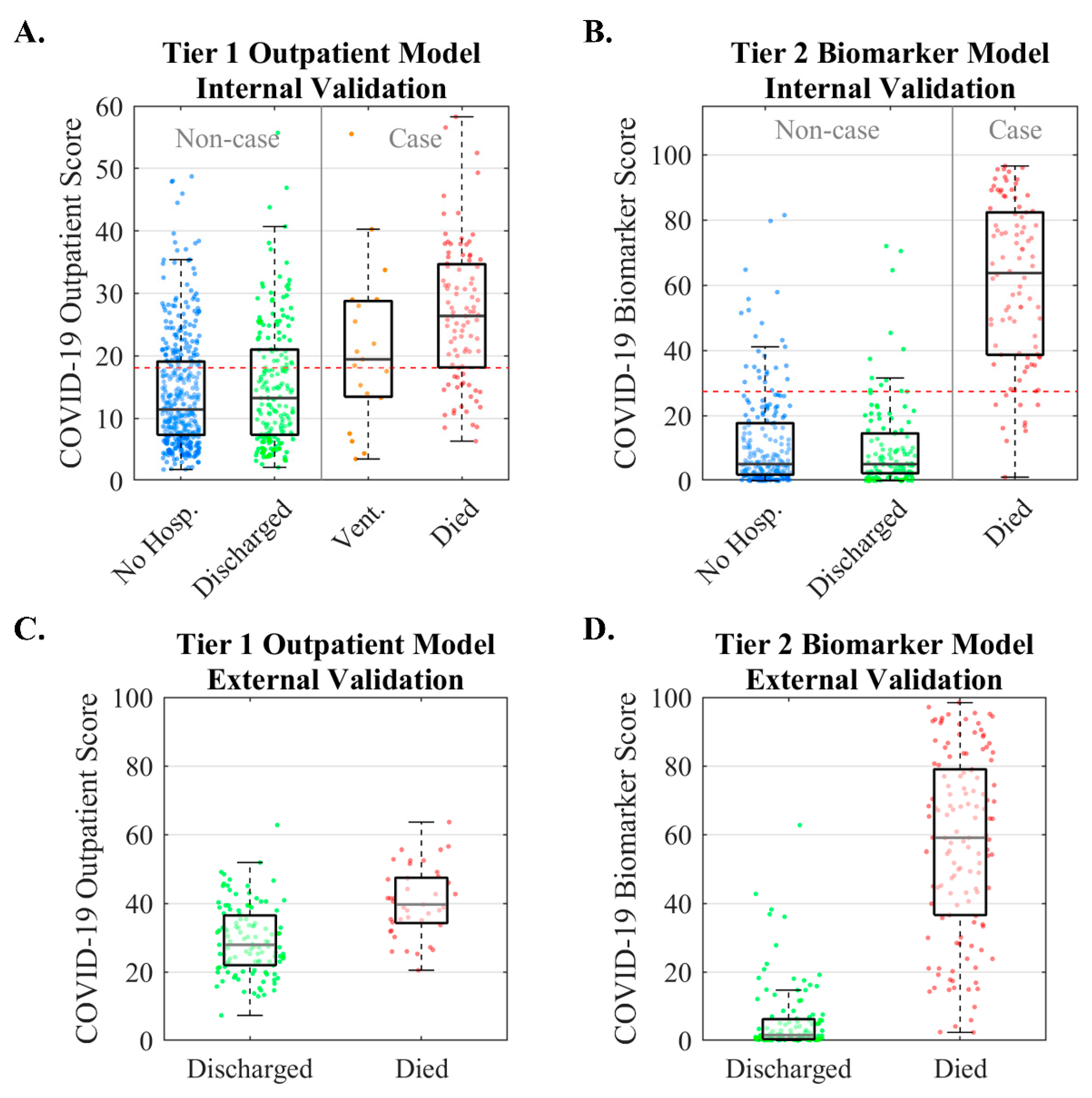
3. Smart Diagnostics for COVID-19
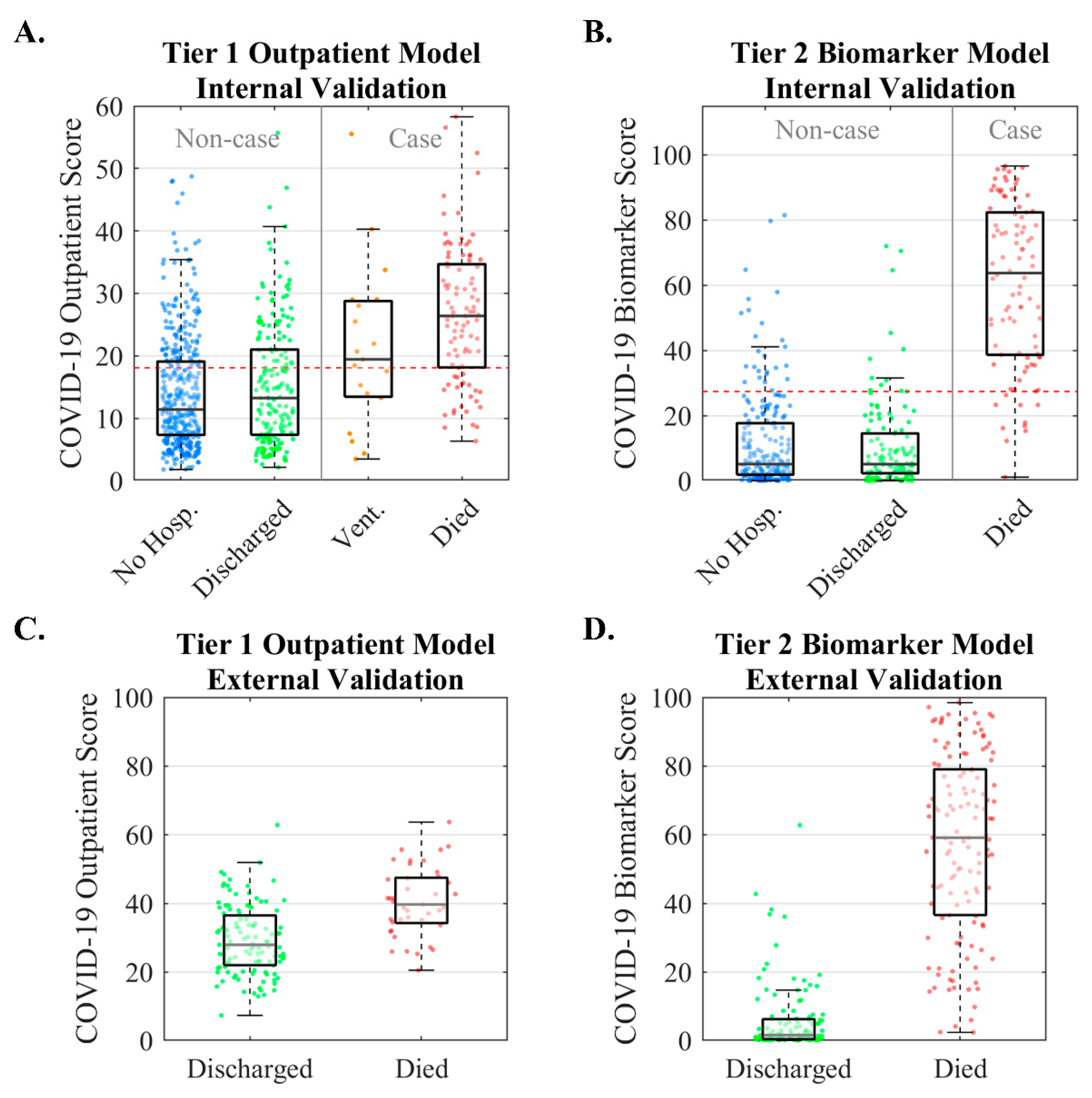
3.1. Predicting COVID-19 Severity in Patients with Cardiac Comorbidities
3.2. Managing COVID-19 in a Community Health Network
4. Smart Diagnostics for Cancer Cytopathology
4.1. Oral Cancer Cytopathology
4.2. Training and Validation Data
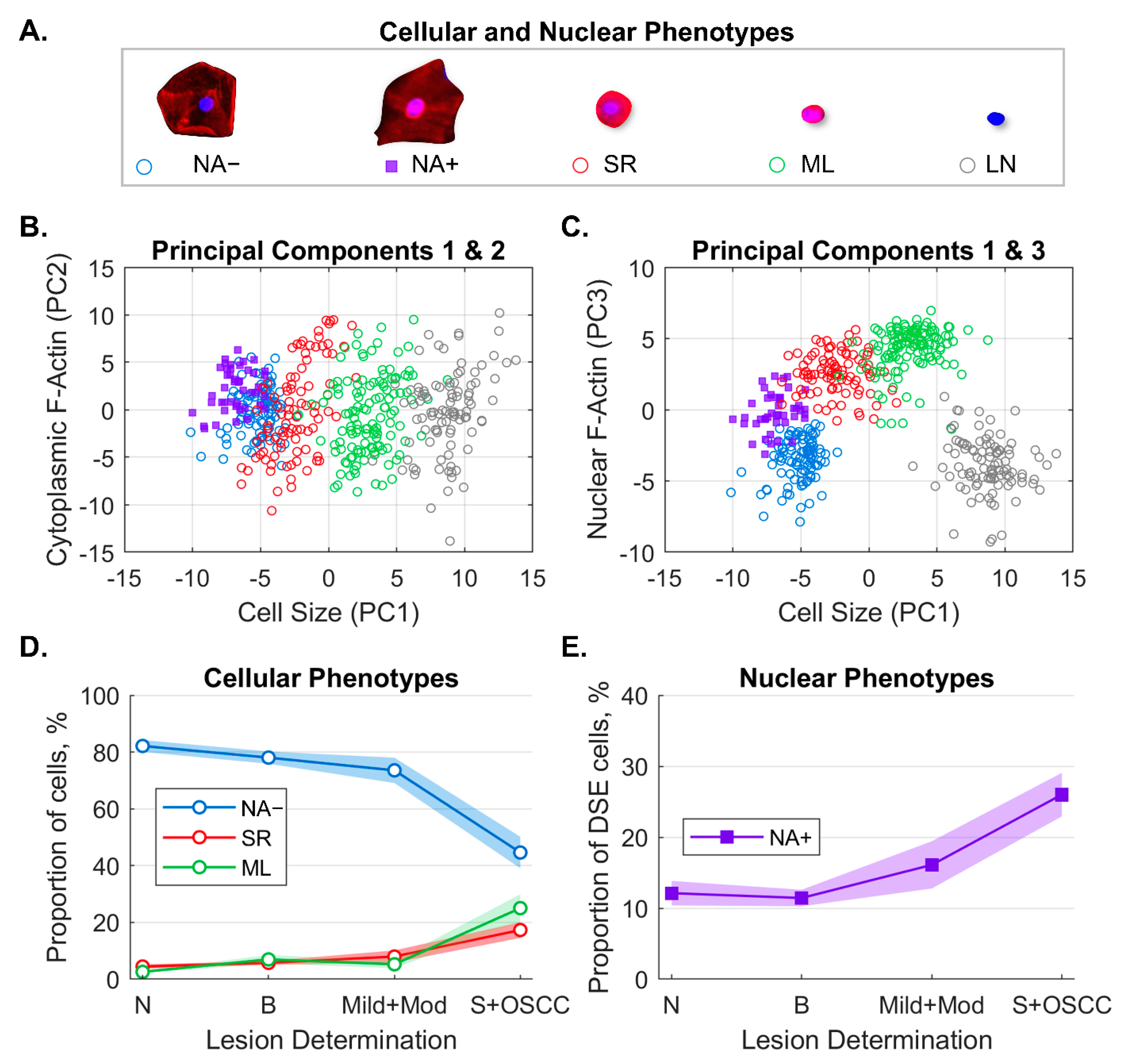
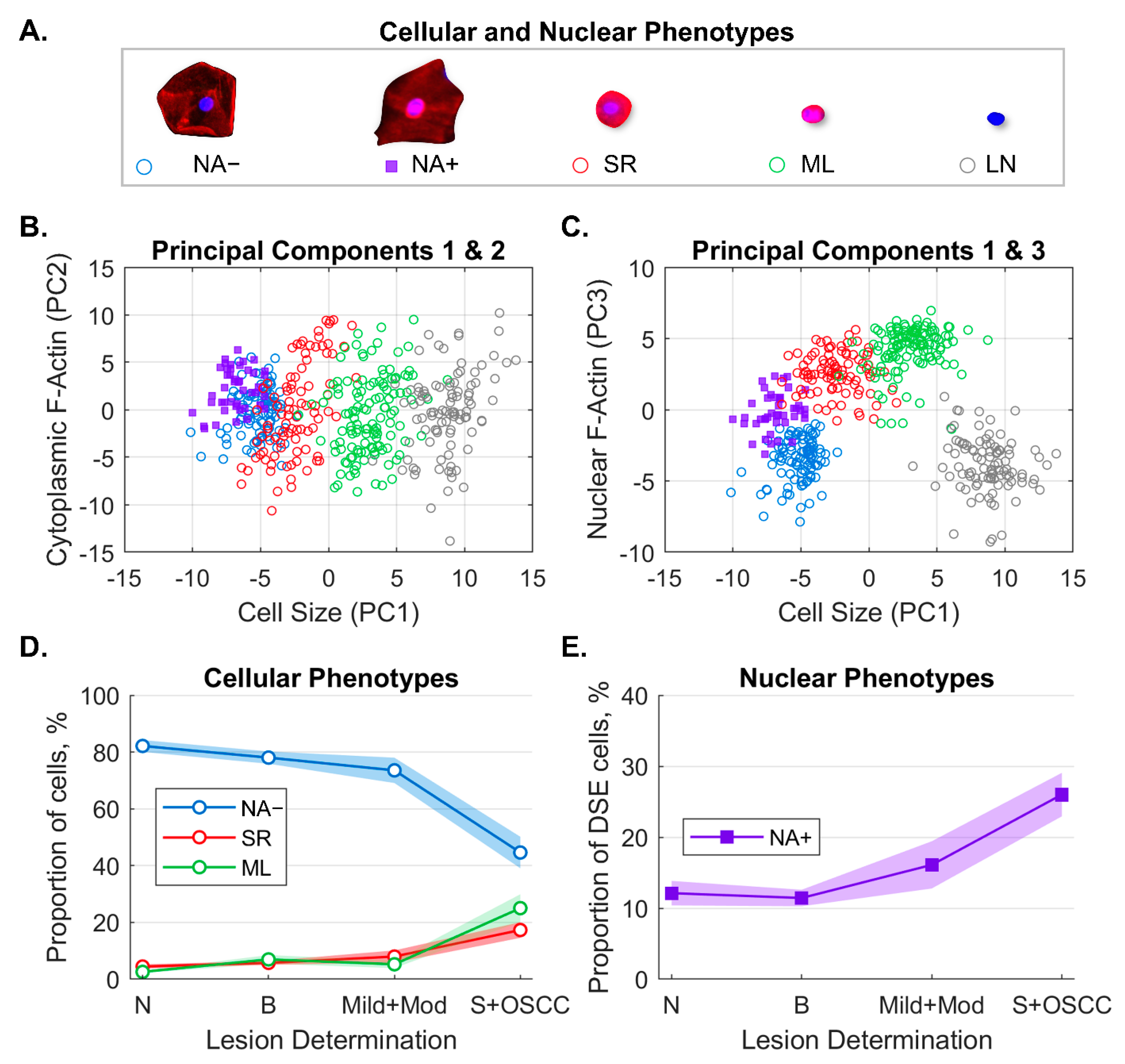
4.3. Machine-Learning-Based Cell Phenotype Classifier
- Immature basaloid keratinocytes or small round (SR) cells appearing as small, circular cells 12–30 µm in diameter;
- Mononuclear leukocytes (MLs) appearing as brightly stained pink cells 6–23 µm in diameter;
- Lone nuclei (LN) appearing as cell objects 5–12 µm in diameter with DAPI counterstaining but no cytoplasmic F-actin staining;
- Differentiated squamous epithelial cells (DSE) or mature keratinocytes appearing as broad/flat cells 50–100 µm in diameter;
- ○
- DSE cells with nuclear actin (NA+);
- ○
- DSE cells without nuclear actin (NA−).
4.4. Predicting a Spectrum of OED/OSCC
5. Discussion and Outlook
5.1. Considerations for Detection Methods
5.2. Considerations for AI Methods
5.3. The Future of Smart Cytology
5.4. Smart Diagnostics for Longitudinal Monitoring
5.5. Future of Smart Diagnostics
Author Contributions
Funding
Conflicts of Interest
References
- Forsman, R.W. Why is the laboratory an afterthought for managed care organizations? Clin. Chem. 1996, 42, 813–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mohammed, M.I.; Haswell, S.; Gibson, I. Lab-on-a-chip or chip-in-a-lab: Challenges of commercialization lost in translation. Procedia. Technol. 2015, 20, 54–59. [Google Scholar] [CrossRef] [Green Version]
- Chin, C.D.; Linder, V.; Sia, S.K. Commercialization of microfluidic point-of-care diagnostic devices. Lab. Chip 2012, 12, 2118–2134. [Google Scholar] [CrossRef] [PubMed]
- Becker, H. Lost in translation. Lab. Chip 2010, 10, 813–815. [Google Scholar] [CrossRef]
- American Hospital Association. Fact Sheet: Strengthening the Health Care Workforce. Available online: https://www.aha.org/fact-sheets/2021-05-26-fact-sheet-strengthening-health-care-workforce (accessed on 28 May 2022).
- CB Insights. Healthcare Remains the Hottest AI Category for Deals. Available online: www.cbinsights.com/research/artificial-intelligence-healthcare-startups-investors (accessed on 24 May 2022).
- Zhang, Z. An in vitro diagnostic multivariate index assay (IVDMIA) for ovarian cancer: Harvesting the power of multiple biomarkers. Rev. Obstet. Gynecol. 2012, 5, 35–41. [Google Scholar]
- U.S. Food and Drug Administration. Guidances with Digital Health Content. Available online: https://www.fda.gov/medical-devices/digital-health-center-excellence/guidances-digital-health-content (accessed on 15 June 2022).
- Patel, V.L.; Shortliffe, E.H.; Stefanelli, M.; Szolovits, P.; Berthold, M.R.; Bellazzi, R.; Abu-Hanna, A. The coming of age of artificial intelligence in medicine. Artif. Intell. Med. 2009, 46, 5–17. [Google Scholar] [CrossRef] [Green Version]
- McRae, M.P.; Simmons, G.; Wong, J.; McDevitt, J.T. Programmable bio-nanochip platform: A point-of-care biosensor system with the capacity to learn. Acc. Chem. Res. 2016, 49, 1359–1368. [Google Scholar] [CrossRef]
- McRae, M.P.; Simmons, G.W.; Wong, J.; Shadfan, B.; Gopalkrishnan, S.; Christodoulides, N.; McDevitt, J.T. Programmable bio-nano-chip system: A flexible point-of-care platform for bioscience and clinical measurements. Lab. Chip 2015, 15, 4020–4031. [Google Scholar] [CrossRef] [Green Version]
- Abram, T.J.; Floriano, P.N.; Christodoulides, N.; James, R.; Kerr, A.R.; Thornhill, M.H.; Redding, S.W.; Vigneswaran, N.; Speight, P.M.; Vick, J.; et al. ‘Cytology-on-a-chip’ based sensors for monitoring of potentially malignant oral lesions. Oral Oncol. 2016, 60, 103–111. [Google Scholar] [CrossRef] [Green Version]
- McRae, M.P.; Kerr, A.R.; Janal, M.N.; Thornhill, M.H.; Redding, S.W.; Vigneswaran, N.; Kang, S.K.; Niederman, R.; Christodoulides, N.J.; Trochesset, D.A.; et al. Nuclear F-actin Cytology in Oral Epithelial Dysplasia and Oral Squamous Cell Carcinoma. J. Dent. Res. 2020, 100, 479–486. [Google Scholar] [CrossRef]
- McRae, M.P.; Modak, S.S.; Simmons, G.W.; Trochesset, D.A.; Kerr, A.R.; Thornhill, M.H.; Redding, S.W.; Vigneswaran, N.; Kang, S.K.; Christodoulides, N.J.; et al. Point-of-care oral cytology tool for the screening and assessment of potentially malignant oral lesions. Cancer Cytopathol. 2020, 128, 207–220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shadfan, B.H.; Simmons, A.R.; Simmons, G.W.; Ho, A.; Wong, J.; Lu, K.H.; Bast, R.C., Jr.; McDevitt, J.T. A multiplexable, microfluidic platform for the rapid quantitation of a biomarker panel for early ovarian cancer detection at the point-of-care. Cancer Prev. Res. 2015, 8, 37–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McRae, M.P.; Bozkurt, B.; Ballantyne, C.M.; Sanchez, X.; Christodoulides, N.; Simmons, G.; Nambi, V.; Misra, A.; Miller, C.S.; Ebersole, J.L.; et al. Cardiac ScoreCard: A diagnostic multivariate index assay system for predicting a spectrum of cardiovascular disease. Expert Syst. Appl. 2016, 54, 136–147. [Google Scholar] [CrossRef]
- Christodoulides, N.; De La Garza, R., II; Simmons, G.W.; McRae, M.P.; Wong, J.; Newton, T.F.; Smith, R.; Mahoney Iii, J.J.; Hohenstein, J.; Gomez, S.; et al. Application of programmable bio-nano-chip system for the quantitative detection of drugs of abuse in oral fluids. Drug Alcohol Depend. 2015, 153, 306–313. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christodoulides, N.; De La Garza, R., II; Simmons, G.W.; McRae, M.P.; Wong, J.; Newton, T.F.; Kosten, T.R.; Haque, A.; McDevitt, J.T. Next generation programmable bio-nano-chip system for on-site quantitative drug detection in oral fluids. J. Drug Abus. 2015, 1, 1–6. [Google Scholar]
- McRae, M.P.; Dapkins, I.P.; Sharif, I.; Anderman, J.; Fenyo, D.; Sinokrot, O.; Kang, S.K.; Christodoulides, N.J.; Vurmaz, D.; Simmons, G.W.; et al. Managing COVID-19 With a Clinical Decision Support Tool in a Community Health Network: Algorithm Development and Validation. J. Med. Internet Res. 2020, 22, e22033. [Google Scholar] [CrossRef] [PubMed]
- McRae, M.P.; Simmons, G.W.; Christodoulides, N.J.; Lu, Z.; Kang, S.K.; Fenyo, D.; Alcorn, T.; Dapkins, I.P.; Sharif, I.; Vurmaz, D.; et al. Clinical decision support tool and rapid point-of-care platform for determining disease severity in patients with COVID-19. Lab. Chip 2020, 20, 2075–2085. [Google Scholar] [CrossRef]
- Rajkomar, A.; Dean, J.; Kohane, I. Machine Learning in Medicine. N. Engl. J. Med. 2019, 380, 1347–1358. [Google Scholar] [CrossRef]
- World Health Organization. The Top 10 Causes of Death. Available online: https://www.who.int/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 24 May 2022).
- Kawamoto, K.; Houlihan, C.A.; Balas, E.A.; Lobach, D.F. Improving clinical practice using clinical decision support systems: A systematic review of trials to identify features critical to success. BMJ 2005, 330, 765. [Google Scholar] [CrossRef] [Green Version]
- Baxt, W.G. Use of an artificial neural network for the diagnosis of myocardial infarction. Ann. Intern. Med. 1991, 115, 843–848. [Google Scholar] [CrossRef]
- Furlong, J.W.; Dupuy, M.E.; Heinsimer, J.A. Neural network analysis of serial cardiac enzyme data. A Clin. Appl. Artif. Mach. Intell. Am. J. Clin. Pathol. 1991, 96, 134–141. [Google Scholar]
- Yan, H.; Jiang, Y.; Zheng, J.; Peng, C.; Li, Q. A multilayer perceptron-based medical decision support system for heart disease diagnosis. Expert Syst. Appl. 2006, 30, 272–281. [Google Scholar] [CrossRef]
- Mehrabi, S.; Maghsoudloo, M.; Arabalibeik, H.; Noormand, R.; Nozari, Y. Application of multilayer perceptron and radial basis function neural networks in differentiating between chronic obstructive pulmonary and congestive heart failure diseases. Expert Syst. Appl. 2009, 36, 6956–6959. [Google Scholar] [CrossRef]
- Conforti, D.; Guido, R. Kernel-based Support Vector Machine classifiers for early detection of myocardial infarction. Optim. Methods Softw. 2005, 20, 395–407. [Google Scholar] [CrossRef]
- Ion Titapiccolo, J.; Ferrario, M.; Cerutti, S.; Barbieri, C.; Mari, F.; Gatti, E.; Signorini, M.G. Artificial intelligence models to stratify cardiovascular risk in incident hemodialysis patients. Expert Syst. Appl. 2013, 40, 4679–4686. [Google Scholar] [CrossRef]
- Vila-Francés, J.; Sanchís, J.; Soria-Olivas, E.; Serrano, A.J.; Martínez-Sober, M.; Bonanad, C.; Ventura, S. Expert system for predicting unstable angina based on Bayesian networks. Expert Syst. Appl. 2013, 40, 5004–5010. [Google Scholar] [CrossRef]
- Das, R.; Turkoglu, I.; Sengur, A. Effective diagnosis of heart disease through neural networks ensembles. Expert Syst. Appl. 2009, 36, 7675–7680. [Google Scholar] [CrossRef]
- Wang, A.; An, N.; Chen, G.; Li, L.; Alterovitz, G. Predicting hypertension without measurement: A non-invasive, questionnaire-based approach. Expert Syst. Appl. 2015, 42, 7601–7609. [Google Scholar] [CrossRef]
- Eom, J.-H.; Kim, S.-C.; Zhang, B.-T. AptaCDSS-E: A classifier ensemble-based clinical decision support system for cardiovascular disease level prediction. Expert Syst. Appl. 2008, 34, 2465–2479. [Google Scholar] [CrossRef] [Green Version]
- Blankenberg, S.; Zeller, T.; Saarela, O.; Havulinna, A.S.; Kee, F.; Tunstall-Pedoe, H.; Kuulasmaa, K.; Yarnell, J.; Schnabel, R.B.; Wild, P.S.; et al. Contribution of 30 biomarkers to 10-year cardiovascular risk estimation in 2 population cohorts: The MONICA, Risk, Genetics, Archiving, and Monograph (MORGAM) Biomarker Project. Circulation 2010, 121, 2388–2397. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morrow, D.A.; Braunwald, E. Future of biomarkers in acute coronary syndromes: Moving toward a multimarker strategy. Circulation 2003, 108, 250–252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sabatine, M.S.; Morrow, D.A.; de Lemos, J.A.; Gibson, C.M.; Murphy, S.A.; Rifai, N.; McCabe, C.; Antman, E.M.; Cannon, C.P.; Braunwald, E. Multimarker approach to risk stratification in non-ST elevation acute coronary syndromes: Simultaneous assessment of troponin I, C-reactive protein, and B-type natriuretic peptide. Circulation 2002, 105, 1760–1763. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Christodoulides, N.; Pierre, F.N.; Sanchez, X.; Li, L.; Hocquard, K.; Patton, A.; Muldoon, R.; Miller, C.S.; Ebersole, J.L.; Redding, S.; et al. Programmable bio-nanochip technology for the diagnosis of cardiovascular disease at the point-of-care. Methodist DeBakey Cardiovasc. J. 2012, 8, 6–12. [Google Scholar] [CrossRef] [Green Version]
- Floriano, P.N.; Christodoulides, N.; Miller, C.S.; Ebersole, J.L.; Spertus, J.; Rose, B.G.; Kinane, D.F.; Novak, M.J.; Steinhubl, S.; Acosta, S.; et al. Use of saliva-based nano-biochip tests for acute myocardial infarction at the point of care: A feasibility study. Clin. Chem. 2009, 55, 1530–1538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, N.; Zhou, M.; Dong, X.; Qu, J.; Gong, F.; Han, Y.; Qiu, Y.; Wang, J.; Liu, Y.; Wei, Y.; et al. Epidemiological and clinical characteristics of 99 cases of 2019 novel coronavirus pneumonia in Wuhan, China: A descriptive study. Lancet 2020, 395, 507–513. [Google Scholar] [CrossRef] [Green Version]
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China, 2019. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Available online: https://www.who.int/ (accessed on 1 April 2020).
- Bai, T.; Tu, S.; Wei, Y.; Xiao, L.; Jin, Y.; Zhang, L.; Song, J.; Liu, W.; Zhu, Q.; Yang, L.; et al. Clinical and Laboratory Factors Predicting the Prognosis of Patients with COVID-19: An Analysis of 127 Patients in Wuhan, China. SSRN 2020, 1–17. [Google Scholar] [CrossRef]
- Zhang, B.; Zhou, X.; Qiu, Y.; Feng, F.; Feng, J.; Jia, Y.; Zhu, H.; Hu, K.; Liu, J.; Liu, Z.; et al. Clinical characteristics of 82 death cases with COVID-19. medRxiv 2020, 15, e0235458. [Google Scholar] [CrossRef] [Green Version]
- Shi, S.; Qin, M.; Shen, B.; Cai, Y.; Liu, T.; Yang, F.; Gong, W.; Liu, X.; Liang, J.; Zhao, Q.; et al. Association of Cardiac Injury With Mortality in Hospitalized Patients With COVID-19 in Wuhan, China. JAMA Cardiol. 2020, 5, 802–810. [Google Scholar] [CrossRef] [Green Version]
- Guo, T.; Fan, Y.; Chen, M.; Wu, X.; Zhang, L.; He, T.; Wang, H.; Wan, J.; Wang, X.; Lu, Z. Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020, 5, 811–818. [Google Scholar] [CrossRef] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Clerkin, K.J.; Fried, J.A.; Raikhelkar, J.; Sayer, G.; Griffin, J.M.; Masoumi, A.; Jain, S.S.; Burkhoff, D.; Kumaraiah, D.; Rabbani, L.; et al. Coronavirus Disease 2019 (COVID-19) and Cardiovascular Disease. Circulation 2020, 1, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Singh, K.; Valley, T.S.; Tang, S.; Li, B.Y.; Kamran, F.; Sjoding, M.W.; Wiens, J.; Otles, E.; Donnelly, J.P.; Wei, M.Y.; et al. Evaluating a Widely Implemented Proprietary Deterioration Index Model among Hospitalized Patients with COVID-19. Ann. Am. Thorac. Soc. 2020, 18, 1129–1137. [Google Scholar] [CrossRef] [PubMed]
- The ARDS Definition Task Force. Acute respiratory distress syndrome: The Berlin Definition. JAMA 2012, 307, 2526–2533. [Google Scholar] [CrossRef]
- Fan, E.; Brodie, D.; Slutsky, A.S. Acute respiratory distress syndrome: Advances in diagnosis and treatment. JAMA 2018, 319, 698–710. [Google Scholar] [CrossRef]
- Wallis, L.A. African Federation for Emergency Medicine resources for managing COVID-19 in low resourced settings. Afr. J. Emerg. Med. 2020, 10, 49. [Google Scholar] [CrossRef]
- Duca, A.; Piva, S.; Focà, E.; Latronico, N.; Rizzi, M. Calculated Decisions: Brescia-COVID Respiratory Severity Scale (BCRSS)/Algorithm. Emerg. Med. Pract. 2020, 22, Cd1–Cd2. [Google Scholar]
- Yan, L.; Zhang, H.-T.; Goncalves, J.; Xiao, Y.; Wang, M.; Guo, Y.; Sun, C.; Tang, X.; Jing, L.; Zhang, M.; et al. An interpretable mortality prediction model for COVID-19 patients. Nat. Mach. Intell. 2020, 2, 283–288. [Google Scholar] [CrossRef]
- Bleeker, S.E.; Moll, H.A.; Steyerberg, E.W.; Donders, A.R.T.; Derksen-Lubsen, G.; Grobbee, D.E.; Moons, K.G.M. External validation is necessary in prediction research:: A clinical example. J. Clin. Epidemiol. 2003, 56, 826–832. [Google Scholar] [CrossRef]
- Hambrecht, A.; Krowsoski, L.; DiMaggio, C.; Hong, C.; Medina, B.; McDevitt, J.T.; McRae, M.; Mukherjee, V.; Uppal, A.; Bukur, M. A Novel COVID-19 Severity Score Is Associated with Survival in Patients Undergoing Percutaneous Dilational Tracheostomy. J. Am. Coll. Surg. 2021, 233, S287. [Google Scholar] [CrossRef]
- Lingen, M.W.; Abt, E.; Agrawal, N.; Chaturvedi, A.K.; Cohen, E.; D’Souza, G.; Gurenlian, J.; Kalmar, J.R.; Kerr, A.R.; Lambert, P.M.; et al. Evidence-based clinical practice guideline for the evaluation of potentially malignant disorders in the oral cavity: A report of the American Dental Association. J. Am. Dent. Assoc. (1939) 2017, 148, 712–727. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huber, M.A. Adjunctive Diagnostic Techniques for Oral and Oropharyngeal Cancer Discovery. Dent. Clin. N. Am. 2018, 62, 59–75. [Google Scholar] [CrossRef] [PubMed]
- Rashid, A.; Warnakulasuriya, S. The use of light-based (optical) detection systems as adjuncts in the detection of oral cancer and oral potentially malignant disorders: A systematic review. J. Oral Pathol. Med. 2015, 44, 307–328. [Google Scholar] [CrossRef]
- CDx Diagnostics: The Painless Test for Common Oral Spots. Available online: https://www.cdxdiagnostics.com/brushtest/ (accessed on 10 May 2019).
- Forward Science. CytID. Available online: https://forwardscience.com/cytid (accessed on 11 August 2022).
- Resolution Biomedical. Clear Prep. Available online: https://www.resolutionbiomedical.com/clearprep/ (accessed on 11 August 2022).
- Poate, T.W.J.; Buchanan, J.A.G.; Hodgson, T.A.; Speight, P.M.; Barrett, A.W.; Moles, D.R.; Scully, C.; Porter, S.R. An audit of the efficacy of the oral brush biopsy technique in a specialist Oral Medicine unit. Oral Oncol. 2004, 40, 829–834. [Google Scholar] [CrossRef] [PubMed]
- Svirsky, J.A.; Burns, J.C.; Carpenter, W.M.; Cohen, D.M.; Bhattacharyya, I.; Fantasia, J.E.; Lederman, D.A.; Lynch, D.P.; Sciubba, J.J.; Zunt, S.L. Comparison of computer-assisted brush biopsy results with follow up scalpel biopsy and histology. Gen. Dent. 2002, 50, 500–503. [Google Scholar]
- Weigum, S.E.; Floriano, P.N.; Redding, S.W.; Yeh, C.; Westbrook, S.D.; McGuff, H.S.; Lin, A.; Miller, F.R.; Villarreal, F.; Rowan, S.D.; et al. Nano-bio-chip sensor platform for examination of oral exfoliative cytology. Cancer Prev. Res. 2010, 3, 518–528. [Google Scholar] [CrossRef] [Green Version]
- Speight, P.M.; Abram, T.J.; Floriano, P.N.; James, R.; Vick, J.; Thornhill, M.H.; Murdoch, C.; Freeman, C.; Hegarty, A.M.; D’Apice, K.; et al. Interobserver agreement in dysplasia grading: Toward an enhanced gold standard for clinical pathology trials. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 120, 474–482. [Google Scholar] [CrossRef] [Green Version]
- El-Naggar, A.K.; Chan, J.K.; Grandis, J.R.; Takata, T.; Slootweg, P.J. (Eds.) WHO Classification of Tumours of the Head and Neck, 4th ed.; IARC Press: Lyon, France, 2017. [Google Scholar]
- Warnakulasuriya, S.; Reibel, J.; Bouquot, J.; Dabelsteen, E. Oral epithelial dysplasia classification systems: Predictive value, utility, weaknesses and scope for improvement. J. Oral Pathol. Med. 2008, 37, 127–133. [Google Scholar] [CrossRef]
- Babshet, M.; Nandimath, K.; Pervatikar, S.; Naikmasur, V. Efficacy of oral brush cytology in the evaluation of the oral premalignant and malignant lesions. J. Cytol. 2011, 28, 165–172. [Google Scholar] [CrossRef]
- Tampa, M.; Mitran, M.I.; Mitran, C.I.; Sarbu, M.I.; Matei, C.; Nicolae, I.; Caruntu, A.; Tocut, S.M.; Popa, M.I.; Caruntu, C.; et al. Mediators of Inflammation—A Potential Source of Biomarkers in Oral Squamous Cell Carcinoma. J. Immunol. Res. 2018, 2018, 12. [Google Scholar] [CrossRef] [Green Version]
- Kurien, B.T.; Scofield, R.H. Protein blotting: A review. J. Immunol. Methods 2003, 274, 1–15. [Google Scholar] [CrossRef]
- Obahiagbon, U.; Smith, J.T.; Zhu, M.; Katchman, B.A.; Arafa, H.; Anderson, K.S.; Blain Christen, J.M. A compact, low-cost, quantitative and multiplexed fluorescence detection platform for point-of-care applications. Biosens. Bioelectron. 2018, 117, 153–160. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.G.; Nordman, E.S.; Johnson, M.D.; Oldham, M.F. A Low-Cost, High-Performance System for Fluorescence Lateral Flow Assays. Biosensors 2013, 3, 360–373. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yetisen, A.K.; Akram, M.S.; Lowe, C.R. Paper-based microfluidic point-of-care diagnostic devices. Lab. Chip 2013, 13, 2210–2251. [Google Scholar] [CrossRef] [PubMed]
- Farrell, B. Lateral Flow Technology for Field-Based Applications—Basics and Advanced Developments. Top. Companion Anim. Med. 2015, 30, 139–147. [Google Scholar] [CrossRef]
- Banerjee, A.; Shuai, Y.; Dixit, R.; Papautsky, I.; Klotzkin, D. Concentration dependence of fluorescence signal in a microfluidic fluorescence detector. J. Lumin. 2010, 130, 1095–1100. [Google Scholar] [CrossRef]
- Bio-Rad Laboratories. Detection Methods. Available online: https://www.bio-rad.com/en-us/applications-technologies/detection-methods (accessed on 11 August 2022).
- Gunning, P.; O’Neill, G.; Hardeman, E. Tropomyosin-based regulation of the actin cytoskeleton in time and space. Physiol. Rev. 2008, 88, 1–35. [Google Scholar] [CrossRef] [Green Version]
- Stevenson, R.P.; Veltman, D.; Machesky, L.M. Actin-bundling proteins in cancer progression at a glance. J. Cell Sci. 2012, 125, 1073. [Google Scholar] [CrossRef] [Green Version]
- Olson, M.F.; Sahai, E. The actin cytoskeleton in cancer cell motility. Clin. Exp. Metastasis 2009, 26, 273–287. [Google Scholar] [CrossRef] [Green Version]
- Belin, B.J.; Cimini, B.A.; Blackburn, E.H.; Mullins, R.D. Visualization of actin filaments and monomers in somatic cell nuclei. Mol. Biol. Cell 2013, 24, 982–994. [Google Scholar] [CrossRef]
- Le, H.Q.; Ghatak, S.; Yeung, C.-Y.C.; Tellkamp, F.; Günschmann, C.; Dieterich, C.; Yeroslaviz, A.; Habermann, B.; Pombo, A.; Niessen, C.M.; et al. Mechanical regulation of transcription controls Polycomb-mediated gene silencing during lineage commitment. Nat. Cell Biol. 2016, 18, 864–875. [Google Scholar] [CrossRef]
- Moore, H.M.; Vartiainen, M.K. F-actin organizes the nucleus. Nat. Cell Biol. 2017, 19, 1386. [Google Scholar] [CrossRef] [PubMed]
- Miroshnikova, Y.A.; Nava, M.M.; Wickström, S.A. Emerging roles of mechanical forces in chromatin regulation. J. Cell Sci. 2017, 130, 2243. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hemstreet, G.P., 3rd; Rao, J.; Hurst, R.E.; Bonner, R.B.; Waliszewski, P.; Grossman, H.B.; Liebert, M.; Bane, B.L. G-actin as a risk factor and modulatable endpoint for cancer chemoprevention trials. J. Cell. Biochem. Suppl. 1996, 25, 197–204. [Google Scholar] [CrossRef]
- Drescher, C.W.; Shah, C.; Thorpe, J.; O’Briant, K.; Anderson, G.L.; Berg, C.D.; Urban, N.; McIntosh, M.W. Longitudinal Screening Algorithm that Incorporates Change over Time in CA125 Levels Identifies Ovarian Cancer Earlier than a Single-Threshold Rule. J. Clin. Oncol. 2012, 31, 387–392. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schork, N.J. Personalized medicine: Time for one-person trials. Nature 2015, 520, 609–611. [Google Scholar] [CrossRef]
- Goetz, L.H.; Schork, N.J. Personalized medicine: Motivation, challenges, and progress. Fertil. Steril. 2018, 109, 952–963. [Google Scholar] [CrossRef]
- Topol, E.J. High-performance medicine: The convergence of human and artificial intelligence. Nat. Med. 2019, 25, 44–56. [Google Scholar] [CrossRef]
- Benjamens, S.; Dhunnoo, P.; Meskó, B. The state of artificial intelligence-based FDA-approved medical devices and algorithms: An online database. NPJ Digit. Med. 2020, 3, 118. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sensitivity | Specificity | AUC | |
|---|---|---|---|
| Early Disease—2|3,4,5,6 | 0.72 (0.67–0.76) | 0.73 (0.69–0.78) | 0.82 (0.77–0.87) |
| 2,3|4,5,6 | 0.79 (0.74–0.83) | 0.85 (0.81–0.89) | 0.89 (0.84–0.93) |
| 2,3,4L|4H,5,6 | 0.80 (0.75–0.84) | 0.82 (0.78–0.86) | 0.89 (0.84–0.93) |
| Late Disease—2,3,4|5,6 | 0.86 (0.82–0.90) | 0.84 (0.80–0.88) | 0.93 (0.88–0.97) |
| 2 vs. 6 | 0.89 (0.85–0.92) | 0.90 (0.85–0.93) | 0.95 (0.91–0.98) |
| 1 vs. 6 | 0.94 (0.89–0.97) | 0.92 (0.87–0.95) | 0.97 (0.94–1.00) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
McRae, M.P.; Rajsri, K.S.; Alcorn, T.M.; McDevitt, J.T. Smart Diagnostics: Combining Artificial Intelligence and In Vitro Diagnostics. Sensors 2022, 22, 6355. https://doi.org/10.3390/s22176355
McRae MP, Rajsri KS, Alcorn TM, McDevitt JT. Smart Diagnostics: Combining Artificial Intelligence and In Vitro Diagnostics. Sensors. 2022; 22(17):6355. https://doi.org/10.3390/s22176355
Chicago/Turabian StyleMcRae, Michael P., Kritika S. Rajsri, Timothy M. Alcorn, and John T. McDevitt. 2022. "Smart Diagnostics: Combining Artificial Intelligence and In Vitro Diagnostics" Sensors 22, no. 17: 6355. https://doi.org/10.3390/s22176355
APA StyleMcRae, M. P., Rajsri, K. S., Alcorn, T. M., & McDevitt, J. T. (2022). Smart Diagnostics: Combining Artificial Intelligence and In Vitro Diagnostics. Sensors, 22(17), 6355. https://doi.org/10.3390/s22176355