
Home-Based Measurements of Dystonia in Cerebral Palsy Using Smartphone-Coupled Inertial Sensor Technology and Machine Learning: A Proof-of-Concept Study

 , , , and
, , , and
Abstract
:1. Introduction
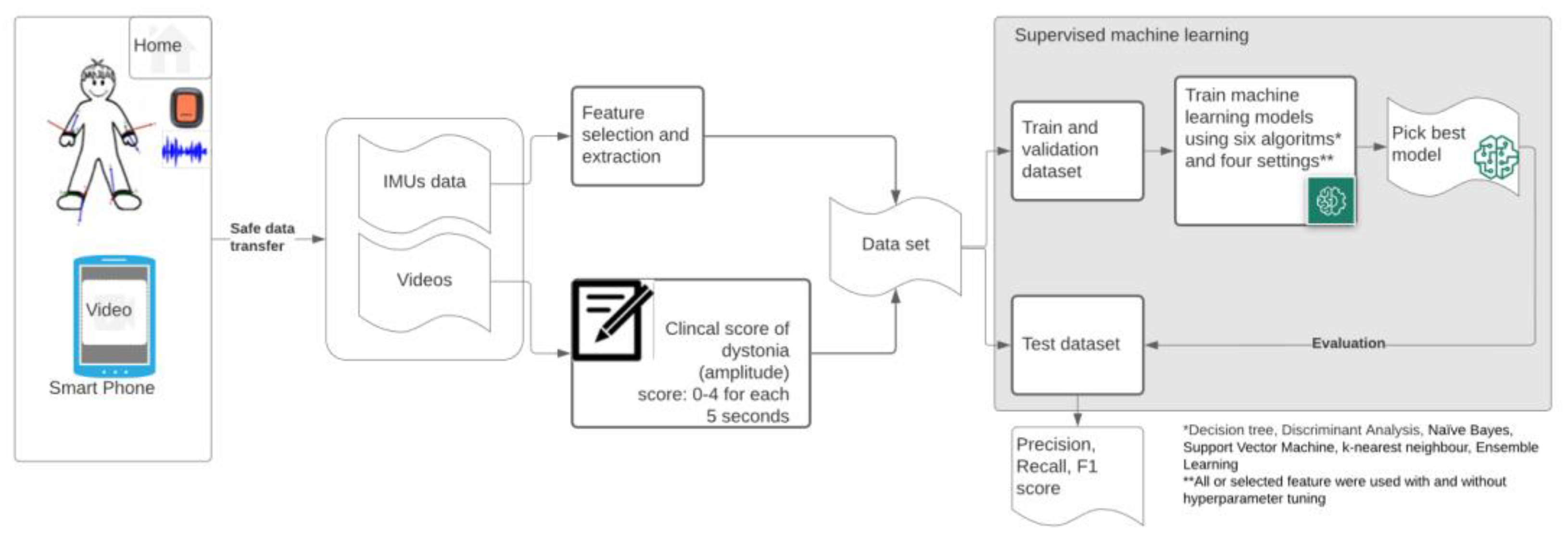
2. Materials and Methods
2.1. Participants
- Age 14.9 ± 4.4 (10.2–21.4) years;
- Weight: 37.3 ± 17.2 (21.7–76.9) kg;
- Height: 145.41 ± 23.5 (116–190) cm;
- 4 females/8 males;
- Gross Motor Function Classification System (GMFCS): II (n= 2), IV (n = 5) or V (n = 5);
- Manual Ability Classification System (MACS): II (n = 1), III (n = 3), IV (n = 2), V (n = 6).
2.2. Measurements
2.2.1. Materials
- (1)
- Mobile phone: Samsung A71 (Samsung Electronics, Daegu, South-Korea), with;
- (2)
- MODYS@home app (developed by Rutgers Engineering, Norg, The Netherlands): a custom mobile application for Android, using the Xsens DOT Software Development Kit (SDK). The app automatically links recorded videos with corresponding time stamps in the sensor data;
- (3)
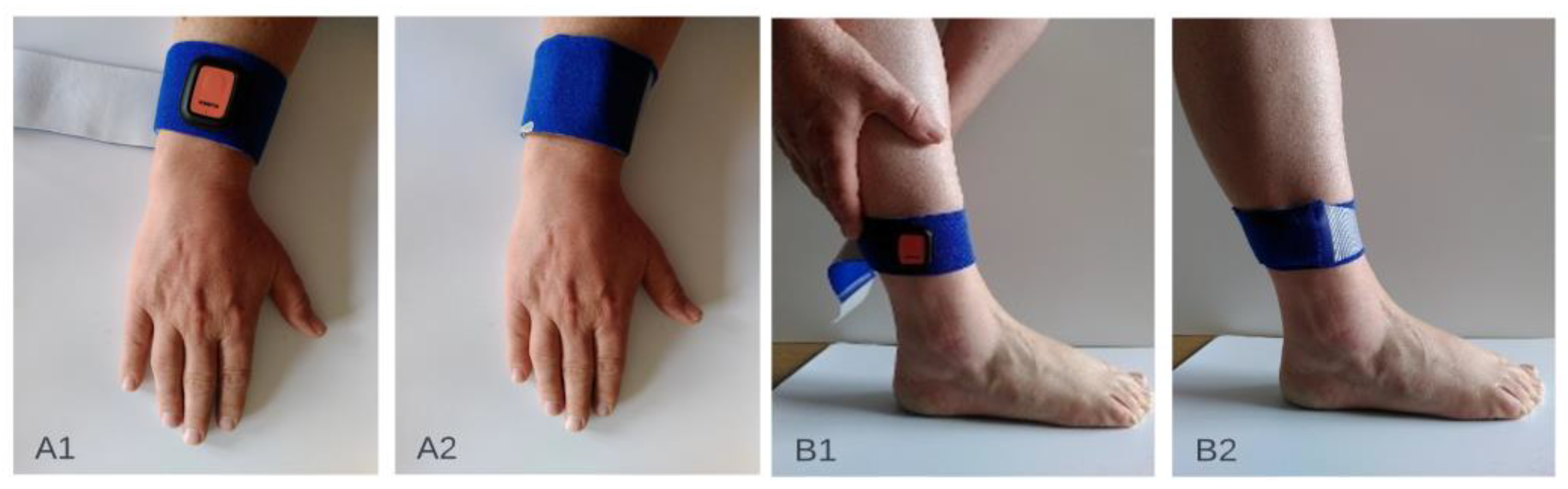
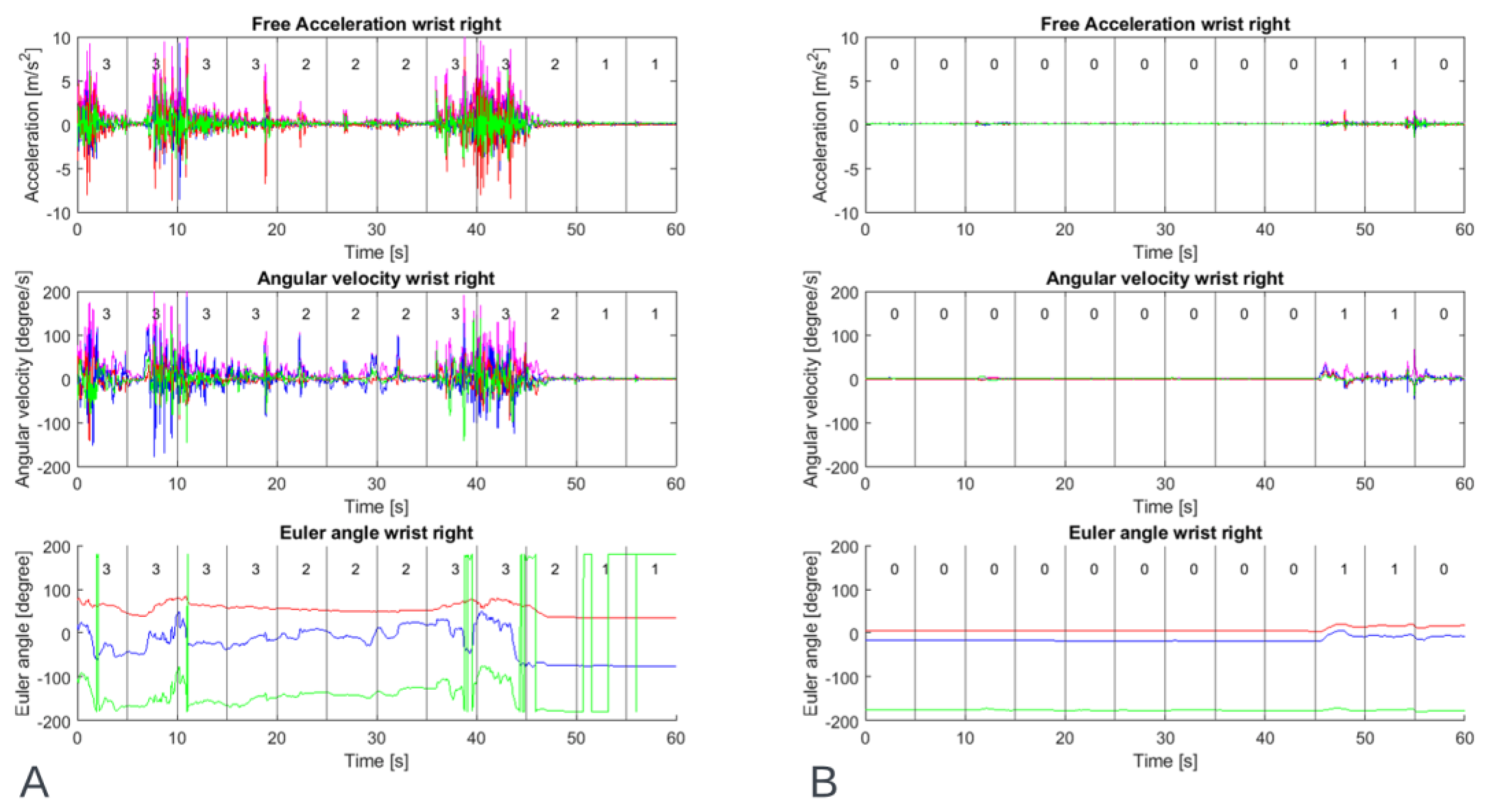
- Four IMUs (Xsens DOT, Xsens Technologies B.V., Enschede, The Netherlands). Xsens DOT is a wearable sensor incorporating 3D accelerometers, gyroscopes and magnetometers to provide acceleration, angular velocity, and the Earth’s magnetic field. Combined with Xsens, sensor fusion algorithms, 3D orientation and free acceleration are provided [10]. Inertial and orientation data outputs of the Xsens DOT sensor are presented in Table 1. The Xsens DOT sensors were set to measure with a sampling frequency of 60 Hz with an accelerometer range of ±16 g and a gyroscope range of ±2000 dps;
- (4)
- Fixation material (Xsens DOT Adhesive patches (Xsens DOT, Xsens Technologies B.V., Enschede, The Netherlands), FabriFoam NuStim Wrap (Fabrifoam, Exton, PA, USA), 3m Coban self-adherent wrap (3M, St. Paul, MN, USA).
2.2.2. Procedure
2.3. Software
2.4. Clinical Scoring
2.5. Data Pre-Processing
2.6. Feature Selection and Extraction
2.7. Machine Learning and Algorithms
2.8. Training, Validating and Testing
3. Results
3.1. Datasets
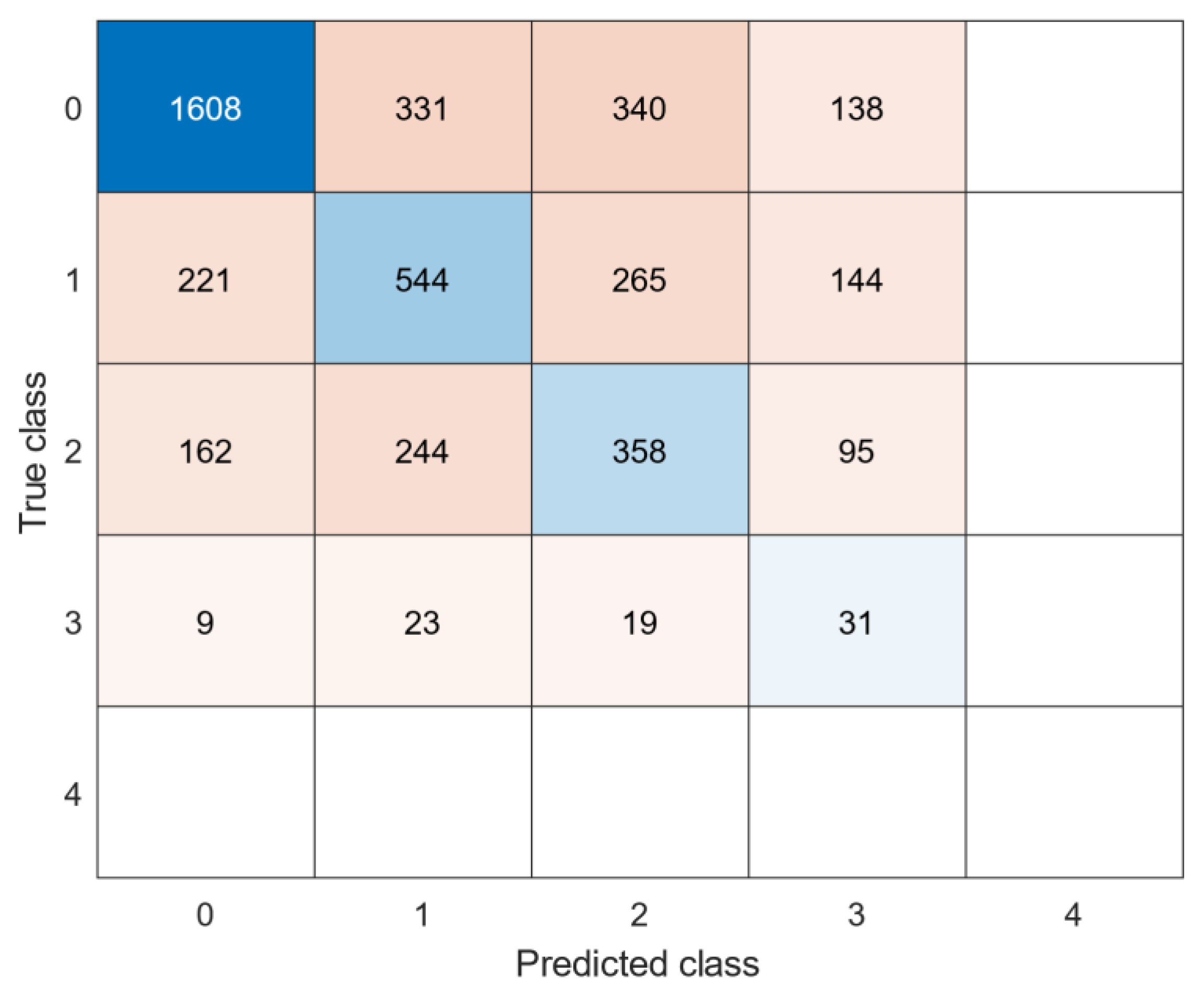
3.2. Individual Clinical Scores Classification
3.3. Generalized Clinical Scores Classification
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Graham, H.K.; Rosenbaum, P.; Paneth, N.; Dan, B.; Lin, J.P.; Damiano, D.L.; Becher, J.G.; Gaebler-Spira, D.; Colver, A.; Reddihough, D.S.; et al. Cerebral Palsy. Nat. Rev. Dis. Primers 2016, 2, 15082. [Google Scholar] [CrossRef] [PubMed]
- Himmelmann, K.; McManus, V.; Hagberg, G.; Uvebrant, P.; Krägeloh-Mann, I.; Cans, C.; on behalf of the SCPE Collaboration. Dyskinetic Cerebral Palsy in Europe: Trends in Prevalence and Severity. Arch. Dis. Child. 2009, 94, 921–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monbaliu, E.; Himmelmann, K.; Lin, J.P.; Ortibus, E.; Bonouvrié, L.; Feys, H.; Vermeulen, R.J.; Dan, B. Clinical Presentation and Management of Dyskinetic Cerebral Palsy. Lancet. Neurol. 2017, 16, 741–749. [Google Scholar] [CrossRef]
- Bohn, E.; Goren, K.; Switzer, L.; Falck-Ytter, Y.; Fehlings, D. Pharmacological and Neurosurgical Interventions for Individuals with Cerebral Palsy and Dystonia: A Systematic Review Update and Meta-Analysis. Dev. Med. Child. Neurol. 2021, 63, 1038–1050. [Google Scholar] [CrossRef] [PubMed]
- Bonouvrié, L.A.; Becher, J.G.; Vles, J.S.; Vermeulen, R.J.; Buizer, A.I.; Idys Study Group. The Effect of Intrathecal Baclofen in Dyskinetic Cerebral Palsy: The Idys Trial. Ann. Neurol. 2019, 86, 79–90. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonouvrié, L.A.; Haberfehlner, H.; Becher, J.G.; Vles, J.S.; Vermeulen, R.J.; Buizer, A.I.; Idys Study Group. Attainment of Personal Goals in the First Year of Intrathecal Baclofen Treatment in Dyskinetic Cerebral Palsy: A Prospective Cohort Study. Disabil. Rehabil. 2022, 1–8. [Google Scholar] [CrossRef]
- Sanger, T.D. Deep Brain Stimulation for Cerebral Palsy: Where Are We Now? Dev. Med. Child. Neurol. 2020, 62, 28–33. [Google Scholar]
- Stewart, K.; Harvey, A.; Johnston, L.M. A Systematic Review of Scales to Measure Dystonia and Choreoathetosis in Children with Dyskinetic Cerebral Palsy. Dev. Med. Child. Neurol. 2017, 59, 786–795. [Google Scholar] [CrossRef] [Green Version]
- Sanger, T.D.; Delgado, M.R.; Gaebler-Spira, D.; Hallett, M.; Mink, J.W.; Task Force on Childhood Motor Disorders. Classification and Definition of Disorders Causing Hypertonia in Childhood. Pediatrics 2003, 111, e89–e97. [Google Scholar] [CrossRef] [Green Version]
- States, R.A.; Krzak, J.J.; Salem, Y.; Godwin, E.M.; Bodkin, A.W.; McMulkin, M.L. Instrumented Gait Analysis for Management of Gait Disorders in Children with Cerebral Palsy: A Scoping Review. Gait Posture 2021, 90, 1–8. [Google Scholar] [CrossRef]
- Francisco-Martínez, C.; Prado-Olivarez, J.; Padilla-Medina, J.A.; Díaz-Carmona, J.; Pérez-Pinal, F.J.; Barranco-Gutiérrez, A.I.; Martínez-Nolasco, J.J. Upper Limb Movement Measurement Systems for Cerebral Palsy: A Systematic Literature Review. Sensors 2021, 21, 7884. [Google Scholar] [CrossRef] [PubMed]
- Kidzinski, L.; Yang, B.; Hicks, J.L.; Rajagopal, A.; Delp, S.L.; Schwartz, M.H. Deep neural networks enable quantitative movement analysis using single-camera videos. Nat. Commun. 2020, 11, 4054. [Google Scholar] [CrossRef] [PubMed]
- Khaksar, S.; Pan, H.; Borazjani, B.; Murray, I.; Agrawal, H.; Liu, W.; Elliott, C.; Imms, C.; Campbell, A.; Walmsley, C. Application of Inertial Measurement Units and Machine Learning Classification in Cerebral Palsy: Randomized Controlled Trial. JMIR Rehabil. Assist. Technol. 2021, 8, e29769. [Google Scholar] [CrossRef] [PubMed]
- Vanmechelen, I.; Bekteshi, S.; Konings, M.; Feys, H.; Desloovere, K.; Aerts, J.M.; Monbaliu, E. Upper limb movement characteristics of children and youth with dyskinetic cerebral palsy—A sensor approach. Gait Posture 2020, 81, 377–378. [Google Scholar] [CrossRef]
- Silva, N.; Zhang, D.; Kulvicius, T.; Gail, A.; Barreiros, C.; Lindstaedt, S.; Kraft, M.; Bolte, S.; Poustka, L.; Nielsen-Saines, K.; et al. The future of General Movement Assessment: The role of computer vision and machine learning—A scoping review. Res. Dev. Disabil. 2021, 110, 103854. [Google Scholar] [CrossRef] [PubMed]
- Ancona, S.; Faraci, F.D.; Khatab, E.; Fiorillo, L.; Gnarra, O.; Nef, T.; Bassetti, C.L.A.; Bargiotas, P. Wearables in the home-based assessment of abnormal movements in Parkinson’s disease: A systematic review of the literature. J. Neurol. 2022, 269, 100–110. [Google Scholar] [CrossRef]
- Pulliam, C.L.; Heldman, D.A.; Brokaw, E.B.; Mera, T.O.; Mari, Z.K.; Burack, M.A. Continuous Assessment of Levodopa Response in Parkinson’s Disease Using Wearable Motion Sensors. IEEE Trans. Biomed. Eng. 2018, 65, 159–164. [Google Scholar] [CrossRef]
- Del Din, S.; Kirk, C.; Yarnall, A.J.; Rochester, L.; Hausdorff, J.M. Body-Worn Sensors for Remote Monitoring of Parkinson’s Disease Motor Symptoms: Vision, State of the Art, and Challenges Ahead. J. Parkinsons Dis. 2021, 11, S35–S47. [Google Scholar] [CrossRef]
- Bennasar, M.; Hicks, Y.A.; Clinch, S.P.; Jones, P.; Holt, C.; Rosser, A.; Busse, M. Automated Assessment of Movement Impairment in Huntington’s Disease. IEEE Trans. Neural. Syst. Rehabil. Eng. 2018, 26, 2062–2069. [Google Scholar] [CrossRef]
- Sanger, T.D. Arm trajectories in dyskinetic cerebral palsy have increased random variability. J. Child. Neurol. 2006, 21, 551–557. [Google Scholar] [CrossRef]
- Monbaliu, E.; de Cock, P.; Ortibus, E.; Heyrman, L.; Klingels, K.; Feys, H. Clinical patterns of dystonia and choreoathetosis in participants with dyskinetic cerebral palsy. Dev. Med. Child. Neurol. 2016, 58, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Vanmechelen, I.; Bekteshi, S.; Konings, M.; Feys, H.; Desloovere, K.; Aerts, J.-M.; Monbaliu, E. Psychometric properties of upper limb kinematics during functional tasks in children and adolescents with dyskinetic cerebral palsy. medRxiv 2022. [Google Scholar] [CrossRef]
- Rosenbaum, P.; Paneth, N.; Leviton, A.; Goldstein, M.; Bax, M.; Damiano, D.; Dan, B.; Jacobsson, B. A report: The definition and classification of cerebral palsy April 2006. Dev. Med. Child. Neurol. 2007, 109, 8–14. [Google Scholar]
- SCPE. Prevalence and characteristics of children with cerebral palsy in Europe. Dev. Med. Child. Neurol. 2002, 44, 633–640. [Google Scholar]
- Monbaliu, E.; Ortibus, E.; de Cat, J.; Dan, B.; Heyrman, L.; Prinzie, P.; De Cock, P.; Feys, H. The dyskinesia Impairment Scale: A new instrument to measure dystonia and choreoathetosis in dyskinetic cerebral palsy. Dev. Med. Child. Neurol. 2012, 54, 278–283. [Google Scholar] [CrossRef]
- Patel, S.; Lorincz, K.; Hughes, R.; Huggins, N.; Growdon, J.; Standaert, D.; Akay, M.; Dy, J.; Welsh, M.; Bonato, P. Monitoring motor fluctuations in patients with Parkinson’s disease using wearable sensors. IEEE Trans. Inf. Technol. Biomed. 2009, 13, 864–873. [Google Scholar] [CrossRef] [Green Version]
- Kuhn, M.; Johnson, K. An Introduction to Feature Selection. In Applied Predictive Modeling; Kuhn, M., Johnson, K., Eds.; Springer: New York, NY, USA, 2013; pp. 487–519. [Google Scholar]
- Hartog, D.D.; Harlaar, J.; Smit, G. The Stumblemeter: Design and Validation of a System That Detects and Classifies Stumbles during Gait. Sensors 2021, 21, 6636. [Google Scholar] [CrossRef]
- Halilaj, E.; Rajagopal, A.; Fiterau, M.; Hicks, J.L.; Hastie, T.J.; Delp, S.L. Machine learning in human movement biomechanics: Best practices, common pitfalls, and new opportunities. J. Biomech. 2018, 81, 1–11. [Google Scholar] [CrossRef]
- Keijsers, N.L.; Horstink, M.W.; Gielen, S.C. Automatic assessment of levodopa-induced dyskinesias in daily life by neural networks. Mov. Disord. 2003, 18, 70–80. [Google Scholar] [CrossRef]
- Tsipouras, M.G.; Tzallas, A.T.; Rigas, G.; Tsouli, S.; Fotiadis, D.I.; Konitsiotis, S. An automated methodology for levodopa-induced dyskinesia: Assessment based on gyroscope and accelerometer signals. Artif. Intell. Med. 2012, 55, 127–135. [Google Scholar] [CrossRef]
- Rodriguez-Molinero, A.; Perez-Lopez, C.; Sama, A.; Rodriguez-Martin, D.; Alcaine, S.; Mestre, B.; Quispe, P.; Giuliani, B.; Vainstein, G.; Browne, P.; et al. Estimating dyskinesia severity in Parkinson’s disease by using a waist-worn sensor: Concurrent validity study. Sci. Rep. 2019, 9, 13434. [Google Scholar] [PubMed] [Green Version]
- Hssayeni, M.D.; Jimenez-Shahed, J.; Burack, M.A.; Ghoraani, B. Dyskinesia estimation during activities of daily living using wearable motion sensors and deep recurrent networks. Sci. Rep. 2021, 11, 7865. [Google Scholar] [CrossRef] [PubMed]
- Haberfehlner, H.; Goudriaan, M.; Bonouvrie, L.A.; Jansma, E.P.; Harlaar, J.; Vermeulen, R.J.; Van der Krogt, M.M.; Buizer, A.I. Instrumented assessment of motor function in dyskinetic cerebral palsy: A systematic review. J. Neuroeng. Rehabil. 2020, 17, 39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sanger, T.D.; Ferman, D. Similarity of Involuntary Postures between Different Children with Dystonia. Mov. Disord. Clin. Pract. 2017, 4, 870–874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yeomans, J.; Thwaites, S.; Robertson, W.S.P.; Booth, D.; Ng, B.; Thewlis, D. Simulating Time-Series Data for Improved Deep Neural Network Performance. IEEE Access 2019, 7, 131248–131255. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Output | Unit |
|---|---|
| Free acceleration | m/s2 |
| Angular velocity | degree/s |
| Euler angles | degree. Roll, pitch, yaw (ZYX Euler Sequence. Earth fixed type, also known as Cardan or aerospace sequence) |
| Nr | Feature Class |
|---|---|
| 1 | Absolute harmonic mean |
| 2 | Absolute maximum |
| 3 | Bandpower |
| 4 | Geometric mean |
| 5 | Maximum |
| 6 | Median |
| 7 | Minimum |
| 8 | Root-mean-square |
| 9 | Root-sum-of-squares |
| 10 | Shannon entropy |
| Model | Features | Hyperparameter Tuning |
|---|---|---|
| ML model (ALL) | All features | no |
| ML model (ALL + HYP) | All features | yes |
| ML model (SFS) | Selected features with SFS | no |
| ML model (SFS + HYP) | Selected features with SFS | yes |
| Subject | Dataset | Samples | Best Algorithm | Model | F1 Score Validation | F1 Score Test | Precision Test | Recall Test |
|---|---|---|---|---|---|---|---|---|
| Subject 1 | dys lower | 720 | KNN | ALL + HYP | 1 | 0.50 | 0.98 | 0.33 |
| dys upper | 726 | KNN | SFS | 0.92 | 0.74 | 0.74 | 0.75 | |
| Subject 2 | dys lower | 189 | KNN | ALL | 0.94 | 0.93 | 0.93 | 0.93 |
| dys upper | 186 | KNN | SFS + HYP | 0.88 | 0.75 | 0.73 | 0.77 | |
| Subject 4 | dys lower | 120 | KNN | ALL | 1 | 0.74 | 0.87 | 0.64 |
| dys upper | 125 | KNN | SFS | 0.97 | 0.70 | 0.85 | 0.60 | |
| Subject 5 | dys lower | 338 | KNN | ALL | 1 | 0.66 | 0.96 | 0.50 |
| dys upper | 441 | KNN | SFS | 0.98 | 0.96 | 0.95 | 0.98 | |
| Subject 6 | dys lower | 66 | n/a | n/a | n/a | n/a | n/a | n/a |
| dys upper | 66 | KNN | ALL + HYP | 0.96 | 0.60 | 0.65 | 0.73 | |
| Subject 7 | dys lower | 334 | KNN | ALL | 0.95 | 0.82 | 0.81 | 0.83 |
| dys upper | 336 | NB | ALL + HYP | 0.97 | 0.59 | 0.73 | 0.50 | |
| Subject 8 | dys lower | 336 | NB | ALL + HYP | 1 | 0.62 | 0.81 | 0.50 |
| dys upper | 298 | KNN | SFS | 0.93 | 0.64 | 0.73 | 0.58 | |
| Subject 9 | dys lower | 588 | KNN | ALL + HYP | 0.93 | 0.85 | 0.84 | 0.85 |
| dys upper | 583 | KNN | ALL | 0.97 | 0.75 | 0.86 | 0.66 | |
| Subject 10 | dys lower | 514 | n/a | n/a | n/a | n/a | 1 | 1 |
| dys upper | 510 | KNN | SFS | 0.97 | 0.53 | 0.53 | 0.54 | |
| Subject 11 | dys lower | 478 | KNN | ALL + HYP | 0.97 | 0.37 | 0.43 | 0.33 |
| dys upper | 444 | ENS | ALL | 0.84 | 0.76 | 0.75 | 0.77 | |
| Subject 12 | dys lower | 775 | KNN | SFS | 0.93 | 0.51 | 0.61 | 0.44 |
| dys upper | 1237 | ENS | ALL | 0.85 | 0.46 | 0.54 | 0.41 |
| Dataset | Mean F1 Score Validation | Mean F1 Score Test | Mean Precision Test | Mean Recall Test |
|---|---|---|---|---|
| dys lower | 0.97 ± 0.03 | 0.67 ± 0.19 | 0.82 ± 0.18 | 0.66 ± 0.26 |
| dys upper | 0.93 ± 0.06 | 0.68± 0.14 | 0.73 ± 0.13 | 0.66 ± 0.16 |
| Dataset | Samples | Best Algorithm | Model | F1 Score Validation | F1 Score Test | Precision Test | Recall Test |
|---|---|---|---|---|---|---|---|
| dys lower | 4533 | ENS | SFS | 0.93 | 0.45 | 0.43 | 0.48 |
| dys upper | 4976 | KNN | SFS | 0.91 | 0.34 | 0.32 | 0.36 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
den Hartog, D.; van der Krogt, M.M.; van der Burg, S.; Aleo, I.; Gijsbers, J.; Bonouvrié, L.A.; Harlaar, J.; Buizer, A.I.; Haberfehlner, H. Home-Based Measurements of Dystonia in Cerebral Palsy Using Smartphone-Coupled Inertial Sensor Technology and Machine Learning: A Proof-of-Concept Study. Sensors 2022, 22, 4386. https://doi.org/10.3390/s22124386
den Hartog D, van der Krogt MM, van der Burg S, Aleo I, Gijsbers J, Bonouvrié LA, Harlaar J, Buizer AI, Haberfehlner H. Home-Based Measurements of Dystonia in Cerebral Palsy Using Smartphone-Coupled Inertial Sensor Technology and Machine Learning: A Proof-of-Concept Study. Sensors. 2022; 22(12):4386. https://doi.org/10.3390/s22124386
Chicago/Turabian Styleden Hartog, Dylan, Marjolein M. van der Krogt, Sven van der Burg, Ignazio Aleo, Johannes Gijsbers, Laura A. Bonouvrié, Jaap Harlaar, Annemieke I. Buizer, and Helga Haberfehlner. 2022. "Home-Based Measurements of Dystonia in Cerebral Palsy Using Smartphone-Coupled Inertial Sensor Technology and Machine Learning: A Proof-of-Concept Study" Sensors 22, no. 12: 4386. https://doi.org/10.3390/s22124386
APA Styleden Hartog, D., van der Krogt, M. M., van der Burg, S., Aleo, I., Gijsbers, J., Bonouvrié, L. A., Harlaar, J., Buizer, A. I., & Haberfehlner, H. (2022). Home-Based Measurements of Dystonia in Cerebral Palsy Using Smartphone-Coupled Inertial Sensor Technology and Machine Learning: A Proof-of-Concept Study. Sensors, 22(12), 4386. https://doi.org/10.3390/s22124386