
Smartphone as a Disease Screening Tool: A Systematic Review

 ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
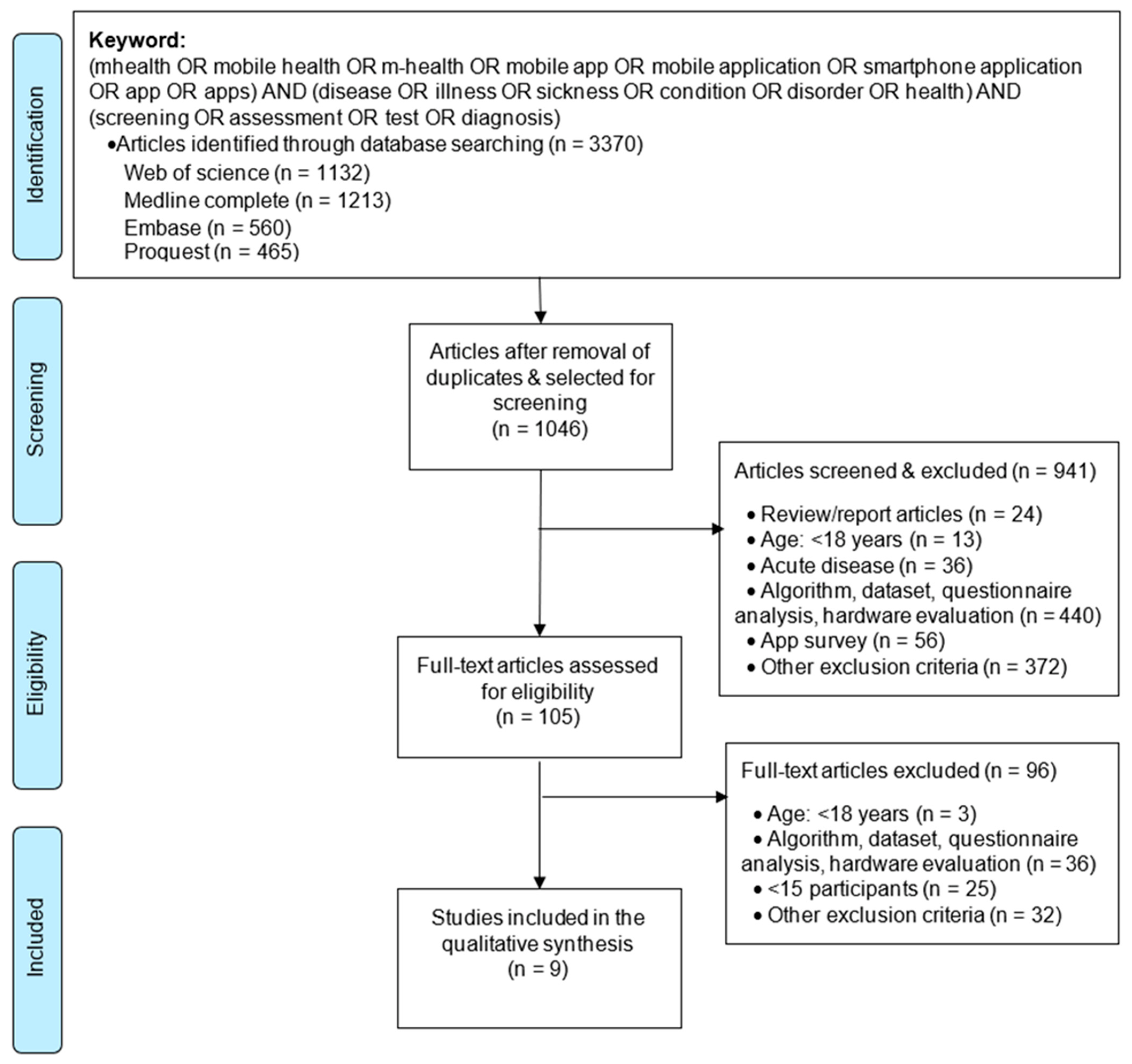
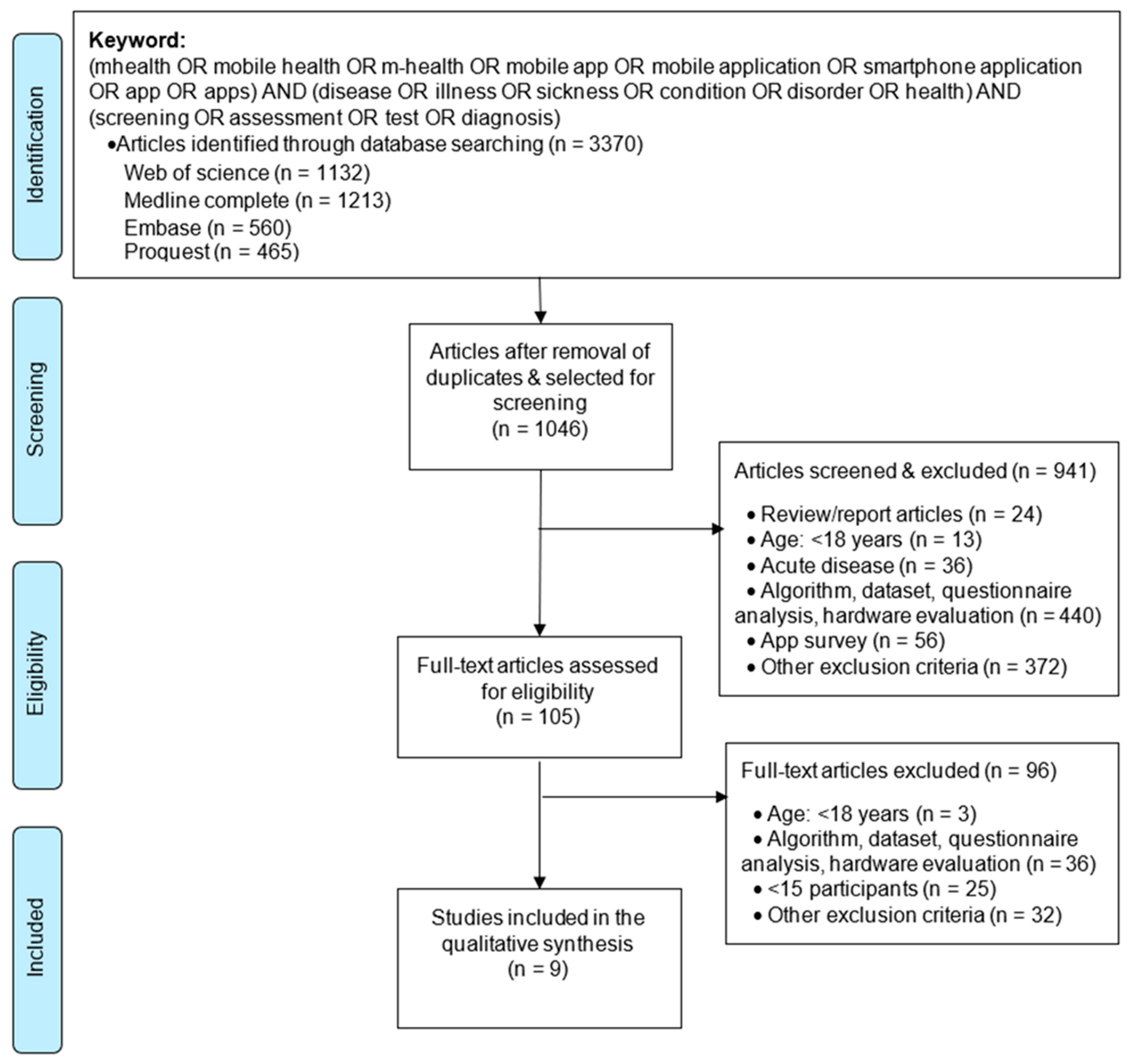
2.1. Data Sources and Search Strategy
2.2. Study Selection Criteria
2.3. Study Selection Process
2.4. Data Extraction and Analysis of Selected Studies
3. Results
3.1. An Overview of the Literature Reviewed
3.2. Participant Characteristics
Age
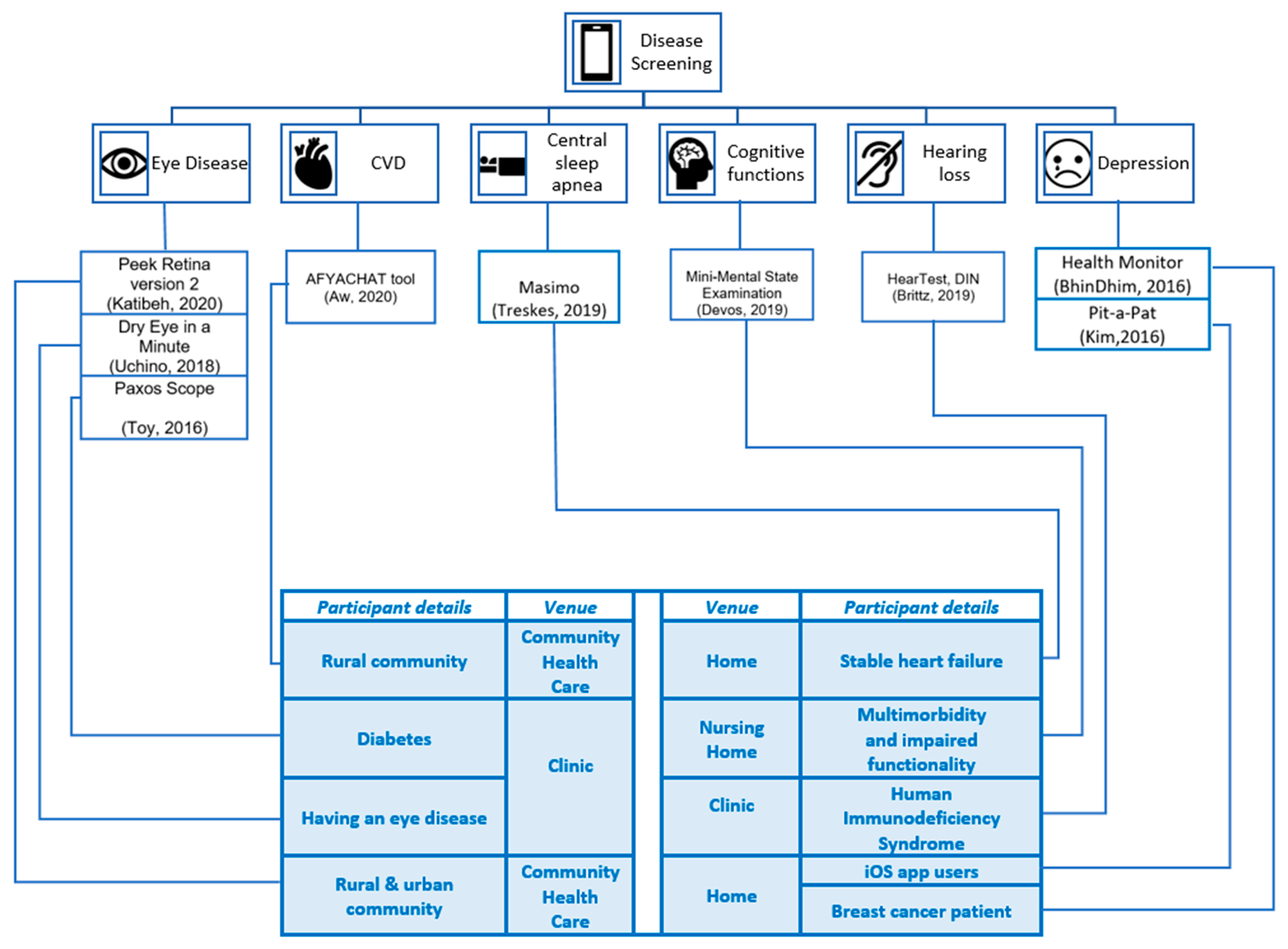
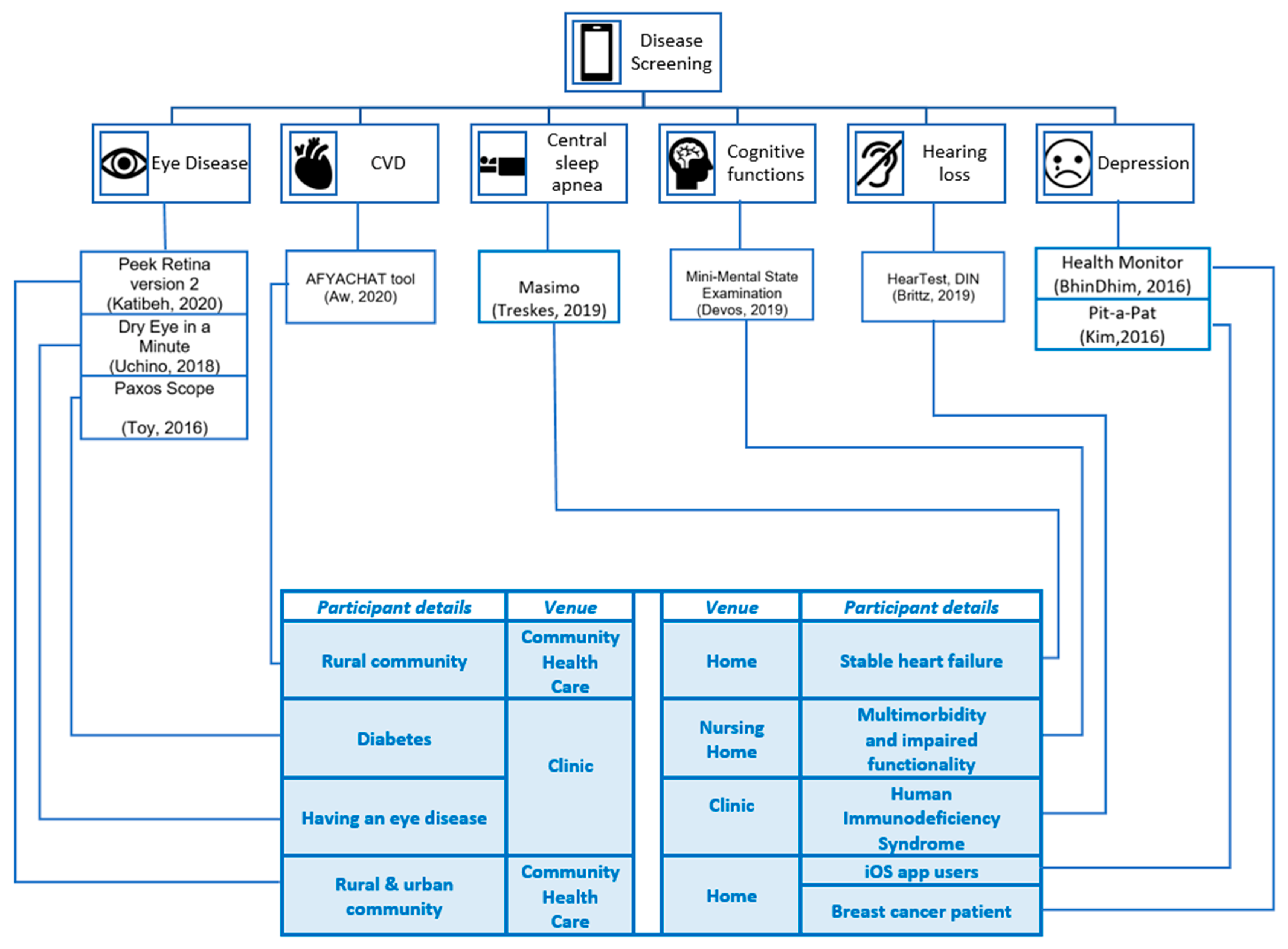
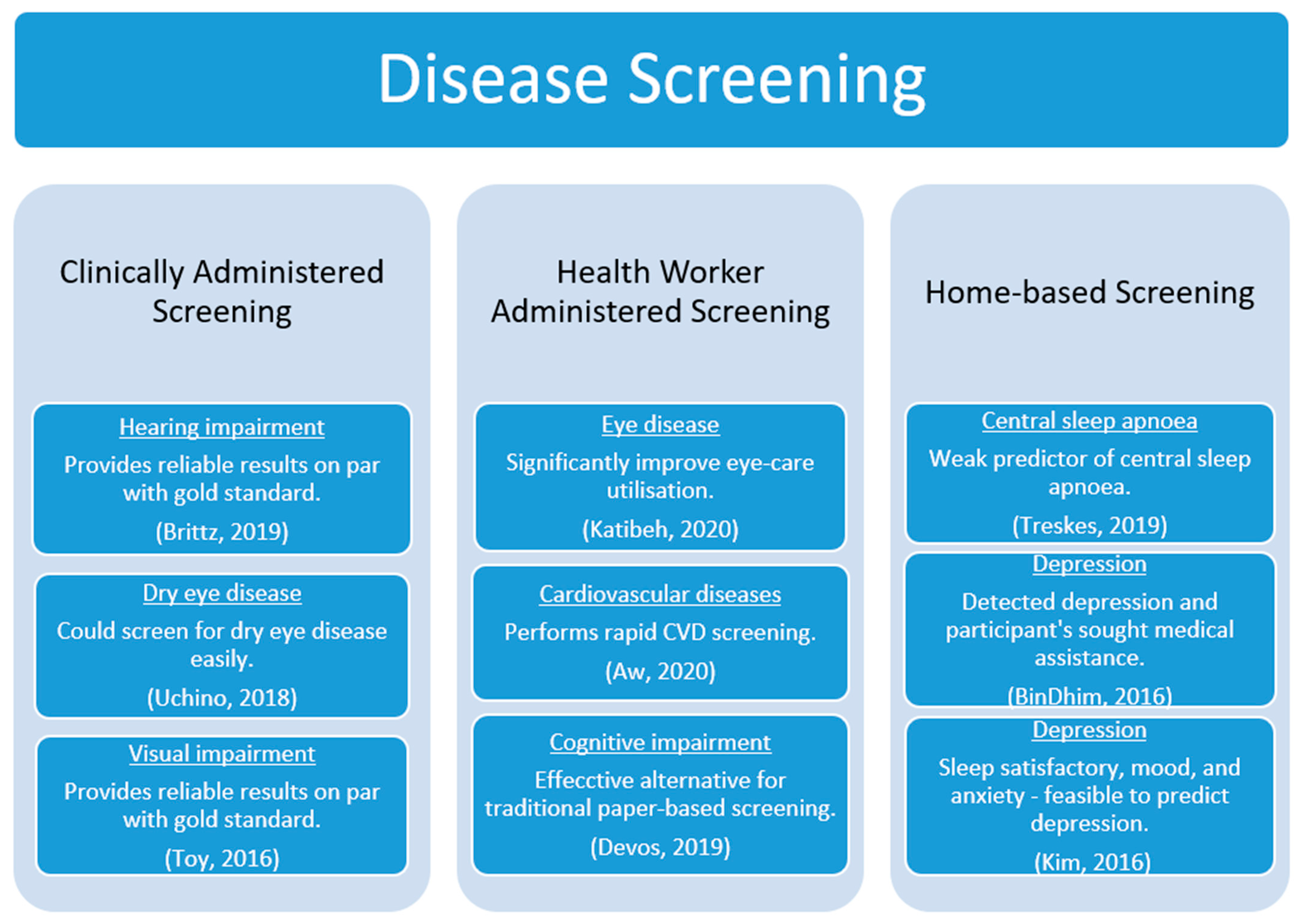
3.3. Disease Screening
3.3.1. Clinically Administered Screening
3.3.2. Health-Worker-Administered Screening
3.3.3. Home-Based Screening
3.4. Technology Acceptance
4. Discussion
4.1. Implications for Practice
4.2. Implications for Research
- It is premature to precisely predict the sequelae of COVID-19 on physical, psychological and neuropsychological outcomes, and social behaviour [38]. Hence, a literature search to find the potential consequences of the virus and screening technologies currently available for the consequences would be of assistance to the healthcare community and COVID-19 infected/recovered patients to identify symptoms at an initial stage.
- Our future work is focused on exploring and realising the potential of artificial intelligence (AI), such as predictive analytics/machine learning and image recognition in disease screening and national language processing and conversational AI in disease-screening literacy.
Future Research Directions
4.3. Limitations of This Survey
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wickramasinghe, N.; John, B.; George, J.; Vogel, D. Achieving Value-Based Care in Chronic Disease Management: Intervention Study. JMIR Diabetes 2019, 4, e10368. [Google Scholar] [CrossRef] [Green Version]
- Wilson, J.M.G.; Jungner, G.; World Health Organization. Principles and Practice of Screening for Disease; World Health Organization: Geneva, Switzerland, 1968. [Google Scholar]
- Iragorri, N.; Spackman, E. Assessing the value of screening tools: Reviewing the challenges and opportunities of cost-effectiveness analysis. Public Health Rev. 2018, 39, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adibi, S. (Ed.) Introduction. In Mobile Health; Springer Series in Bio-Neuroinformatics; Springer: Berlin/Heidelberg, Germany, 2015; pp. 1–7. [Google Scholar]
- Jeffery, M.M.; D’Onofrio, G.; Paek, H.; Platts-Mills, T.F.; Soares, W.E.; Hoppe, J.A.; Genes, N.; Nath, B.; Melnick, E.R. Trends in Emergency Department Visits and Hospital Admissions in Health Care Systems in 5 States in the First Months of the COVID-19 Pandemic in the US. JAMA Intern. Med. 2020, 180, 1328–1333. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.; Neal, R.D.; Duffy, S.R.G.; Scott, S.E.; Whitaker, K.L.; Brain, K. Impact of the COVID-19 pandemic on the symptomatic diagnosis of cancer: The view from primary care. Lancet Oncol. 2020, 21, 748–750. [Google Scholar] [CrossRef]
- Wright, A.; Salazar, A.; Mirica, M.; Volk, L.A.; Schiff, G.D. The Invisible Epidemic: Neglected Chronic Disease Management During COVID-19. J. Gen. Intern. Med. 2020, 35, 2816–2817. [Google Scholar] [CrossRef] [PubMed]
- Moses, J.; Adibi, S.; Islam, S.S.; Wickramasinghe, N.; Nguyen, L. Application of Smartphone Technologies in Disease Monitoring: A Systematic Review. Healthcare 2021, 9, 889. [Google Scholar] [CrossRef] [PubMed]
- Pérez, Y.I.V.; Medlow, S.; Ho, J.; Steinbeck, K. Mobile and Web-Based Apps That Support Self-Management and Transition in Young People with Chronic Illness: Systematic Review. J. Med Internet Res. 2019, 21, e13579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donevant, S.B.; Estrada, R.D.; Culley, J.M.; Habing, B.; Adams, S.A. Exploring app features with outcomes in mHealth studies involving chronic respiratory diseases, diabetes, and hypertension: A targeted exploration of the literature. J. Am. Med. Inform. Assoc. 2018, 25, 1407–1418. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Ioannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA Statement for Reporting Systematic Reviews and Meta-Analyses of Studies That Evaluate Health Care Interventions: Explanation and Elaboration. PLoS Med. 2009, 6, e1000100. [Google Scholar] [CrossRef]
- Jandoo, T. WHO guidance for digital health: What it means for researchers. Digit. Health 2020, 6, 2055207619898984. [Google Scholar] [CrossRef]
- Institute of Medicine; National Research Council. Investing in the Health and Well-Being of Young Adults; Bonnie, R.J., Stroud, C., Breiner, H., Eds.; The National Academies Press: Washington, DC, USA, 2015; p. 502. [Google Scholar]
- Sharma, S.; Mudgal, S.; Thakur, K.; Gaur, R. How to calculate sample size for observational and experiential nursing research studies? Natl. J. Physiol. Pharm. Pharmacol. 2019, 10, 1–8. [Google Scholar] [CrossRef]
- Katibeh, M.; Sabbaghi, H.; Kalantarion, M.; Nikkhah, H.; Mousavi, B.; Beiranvand, R.; Ahmadieh, H.; Kallestrup, P. Eye Care Utilization in A Community-oriented Mobile Screening Programme for Improving Eye Health in Iran: A Cluster Randomized Trial. Ophthalmic Epidemiol. 2020, 27, 417–428. [Google Scholar] [CrossRef] [PubMed]
- Aw, M.; Ochieng, B.O.; Attambo, D.; Opot, D.; Aw, J.; Francis, S.; Hawkes, M.T. Critical appraisal of a mHealth-assisted community-based cardiovascular disease risk screening program in rural Kenya: An operational research study. Pathog. Glob. Health 2020, 114, 379–387. [Google Scholar] [CrossRef] [PubMed]
- Treskes, R.W.; Maan, A.C.; Verwey, H.F.; Schot, R.; Beeres, S.L.M.A.; Tops, L.F.; Van Der Velde, E.T.; Schalij, M.J.; Slats, A.M. Mobile Health for Central Sleep Apnea Screening Among Patients with Stable Heart Failure: Single-Cohort, Open, Prospective Trial. JMIR Cardio 2019, 3, e9894. [Google Scholar] [CrossRef]
- Devos, P.; Debeer, J.; Ophals, J.; Petrovic, M. Cognitive impairment screening using m-health: An android implementation of the mini-mental state examination (MMSE) using speech recognition. Eur. Geriatr. Med. 2019, 10, 501–509. [Google Scholar] [CrossRef] [Green Version]
- Brittz, M.; Heinze, B.; Mahomed-Asmail, F.; Swanepoel, D.W.; Stoltz, A. Monitoring Hearing in an Infectious Disease Clinic with mHealth Technologies. J. Am. Acad. Audiol. 2019, 30, 482–492. [Google Scholar] [CrossRef]
- Uchino, M.; Kawashima, M.; Uchino, Y.; Suzuki, N.; Mitamura, H.; Mizuno, M.; Hori, Y.; Yokoi, N.; Tsubota, K. The evaluation of dry eye mobile apps for screening of dry eye disease and educational tear event in Japan. Ocul. Surf. 2018, 16, 430–435. [Google Scholar] [CrossRef]
- Toy, B.C.; Myung, D.J.; He, L.; Pan, C.K.; Chang, R.T.; Polkinhorne, A.; Merrell, D.; Foster, D.; Blumenkranz, M.S. Smartphone-Based Dilated Fundus Photography and Near Visual Acuity Testing As Inexpensive Screening Tools To Detect Referral Warranted Diabetic Eye Disease. Retina 2016, 36, 1000–1008. [Google Scholar] [CrossRef]
- BinDhim, N.F.; Alanazi, E.M.; Aljadhey, H.; Basyouni, M.H.; Kowalski, S.R.; Pont, L.G.; Shaman, A.M.; Trevena, L.; Alhawassi, T.M.; Zaidan, S.; et al. Does a Mobile Phone Depression-Screening App Motivate Mobile Phone Users with High Depressive Symptoms to Seek a Health Care Professional’s Help? J. Med. Internet Res. 2016, 18, e156. [Google Scholar] [CrossRef]
- Kim, J.; Lim, S.; Min, Y.H.; Shin, Y.-W.; Lee, B.; Sohn, G.; Jung, K.H.; Lee, J.-H.; Son, B.H.; Ahn, S.H.; et al. Depression Screening Using Daily Mental-Health Ratings from a Smartphone Application for Breast Cancer Patients. J. Med. Internet Res. 2016, 18, e216. [Google Scholar] [CrossRef]
- World Bank Group. Available online: https://databank.worldbank.org/reports.aspx?source=2&series=IT.CEL.SETS.P2 (accessed on 20 September 2020).
- Fantom, N.J.; Serajuddin, U. The World Bank’s Classification of Countries by Income; World Bank Group: Washington, DC, USA, 2016. [Google Scholar]
- Kahn, J.G.; Yang, J.S.; Kahn, J.S. ‘Mobile’ Health Needs and Opportunities In Developing Countries. Health Aff. 2010, 29, 254–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Majumder, S.; Deen, M.J. Smartphone Sensors for Health Monitoring and Diagnosis. Sensors 2019, 19, 2164. [Google Scholar] [CrossRef] [Green Version]
- Ericsson. Ericsson Mobility Report: COVID-19 Impact Shows Networks’ Crucial Role in Society. Available online: https://www.ericsson.com/en/press-releases/2020/6/ericsson-mobility-report---june-2020 (accessed on 13 August 2020).
- Li, D. 5G and intelligence medicine—How the next generation of wireless technology will reconstruct healthcare? Precis. Clin. Med. 2019, 2, 205–208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morak, J.; Schreier, G. Design and Evaluation of Near Field Communication (NFC) Technology Based Solutions for mHealth Challenges. In Mobile Health; Adibi, S., Ed.; Springer Series in Bio-Neuroinformatics; Springer: Berlin/Heidelberg, Germany, 2015; Volume 5, pp. 813–838. [Google Scholar] [CrossRef]
- Davis, F.D. Perceived Usefulness, Perceived Ease of Use, and User Acceptance of Information Technology. MIS Q. 1989, 13, 319–340. [Google Scholar] [CrossRef] [Green Version]
- Portz, J.D.; Bayliss, E.A.; Bull, S.; Boxer, R.S.; Bekelman, D.B.; Gleason, K.; Czaja, S. Using the Technology Acceptance Model to Explore User Experience, Intent to Use, and Use Behavior of a Patient Portal Among Older Adults with Multiple Chronic Conditions: Descriptive Qualitative Study. J. Med. Internet Res. 2019, 21, e11604. [Google Scholar] [CrossRef]
- Cohen, B.E.; Durstenfeld, A.; Roehm, P.C. Viral Causes of Hearing Loss: A Review for Hearing Health Professionals. Trends Hear. 2014, 18, 2331216514541361. [Google Scholar] [CrossRef]
- Currie, G.; Delles, C. Vascular biomedicine in an era of chronic disease and multimorbidity. Clin. Sci. 2019, 133, 1137–1143. [Google Scholar] [CrossRef]
- Do, A.N.L.; Dagogo-Jack, S. Comorbidities of Diabetes and Hypertension: Mechanisms and Approach to Target Organ Protection. J. Clin. Hypertens. 2011, 13, 244–251. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, L.; Adibi, S.; Wickramasinghe, N. Towards a Better Life for Diabetic Patients: Developing and Integrating a Non-invasive Self-Management Support Tool Within a Smart Digital Companion. In Delivering Superior Health and Wellness Management with IoT and Analytics; Wickramasinghe, N., Bodendorf, F., Eds.; Healthcare Delivery in the Information Age; ProQuest Ebook Central: Hong Kong, China, 2020; pp. 207–222. [Google Scholar] [CrossRef]
- Rajkumar, R.P. COVID-19 and mental health: A review of the existing literature. Asian J. Psychiatry 2020, 52, 102066. [Google Scholar] [CrossRef]
- Coronavirus Disease 2019 (COVID-19). BMJ. 2020. Available online: https://bestpractice.bmj.com/topics/en-us/3000168 (accessed on 13 August 2020).
- Dash, S.; Shakyawar, S.K.; Sharma, M.; Kaushik, S. Big data in healthcare: Management, analysis and future prospects. J. Big Data 2019, 6, 54. [Google Scholar] [CrossRef] [Green Version]
- Madanian, S.; Parry, D.T.; Airehrour, D.; Cherrington, M. mHealth and big-data integration: Promises for healthcare system in India. BMJ Health Care Inform. 2019, 26, e100071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venkatesh, V.; Thong, J.Y.L.; Xu, X. Consumer Acceptance and Use of Information Technology: Extending the Unified Theory of Acceptance and Use of Technology. MIS Q. 2012, 36, 157–178. [Google Scholar] [CrossRef] [Green Version]
- Delone, W.H.; McLean, E.R. The DeLone and McLean Model of Information Systems Success: A Ten-Year Update. J. Manag. Inf. Syst. 2003, 19, 9–30. [Google Scholar] [CrossRef]
- Burton-Jones, A.; Volkoff, O. How Can We Develop Contextualized Theories of Effective Use? A Demonstration in the Context of Community-Care Electronic Health Records. Inf. Syst. Res. 2017, 28, 468–489. [Google Scholar] [CrossRef]
- Singh, N.; Moneghetti, K.J.; Christle, J.W.; Hadley, D.; Froelicher, V.; Plews, D. Heart Rate Variability: An Old Metric with New Meaning in the Era of Using mHealth technologies for Health and Exercise Training Guidance. Part Two: Prognosis and Training. Arrhythm. Electrophysiol. Rev. 2018, 7, 247–255. [Google Scholar] [CrossRef]
- Fang, S.-C.; Wu, Y.-L.; Tsai, P.-S. Heart Rate Variability and Risk of All-Cause Death and Cardiovascular Events in Patients with Cardiovascular Disease: A Meta-Analysis of Cohort Studies. Biol. Res. Nurs. 2019, 22, 45–56. [Google Scholar] [CrossRef]
- Liu, G.; Wang, L.; Wang, Q.; Zhou, G.; Wang, Y.; Jiang, Q. A New Approach to Detect Congestive Heart Failure Using Short-Term Heart Rate Variability Measures. PLoS ONE 2014, 9, e93399. [Google Scholar] [CrossRef]
- Lees, T.; Shad-Kaneez, F.; Simpson, A.M.; Nassif, N.; Lin, Y.; Lal, S. Heart Rate Variability as a Biomarker for Predicting Stroke, Post-stroke Complications and Functionality. Biomark. Insights 2018, 13, 1177271918786931. [Google Scholar] [CrossRef]
- Saito, I.; Takata, Y.; Maruyama, K.; Eguchi, E.; Kato, T.; Shirahama, R.; Tomooka, K.; Kawamura, R.; Sano, M.; Tabara, Y.; et al. Association Between Heart Rate Variability and Home Blood Pressure: The Toon Health Study. Am. J. Hypertens. 2018, 31, 1120–1126. [Google Scholar] [CrossRef] [Green Version]
- Goldenberg, I.; Goldkorn, R.; Shlomo, N.; Einhorn, M.; Levitan, J.; Kuperstein, R.; Klempfner, R.; Johnson, B. Heart Rate Variability for Risk Assessment of Myocardial Ischemia in Patients Without Known Coronary Artery Disease: The HRV-DETECT (Heart Rate Variability for the Detection of Myocardial Ischemia) Study. J. Am. Heart Assoc. 2019, 8, e014540. [Google Scholar] [CrossRef]
- Mol, M.B.A.; Strous, M.T.A.; van Osch, F.H.M.; Vogelaar, F.J.; Barten, D.G.; Farchi, M.; Foudraine, N.A.; Gidron, Y. Heart-rate-variability (HRV), predicts outcomes in COVID-19. PLoS ONE 2021, 16, e0258841. [Google Scholar] [CrossRef] [PubMed]
- Owens, A.P. The Role of Heart Rate Variability in the Future of Remote Digital Biomarkers. Front. Neurosci. 2020, 14, 582145. [Google Scholar] [CrossRef] [PubMed]
- Pastorino, R.; De Vito, C.; Migliara, G.; Glocker, K.; Binenbaum, I.; Ricciardi, W.; Boccia, S. Benefits and challenges of Big Data in healthcare: An overview of the European initiatives. Eur. J. Public Health 2019, 29 (Suppl. 3), 23–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria: |
|---|
|
|
|
|
|
|
|
| Exclusion Criteria: |
|
|
|
|
|
|
|
|
|
| Articles | Study Type | Country | Count | Age | Male (%) | Female (%) |
|---|---|---|---|---|---|---|
| (Katibeh, 2020) [15] | Exp | Iran | 2520 | 61.7 ± 9.5 | 51.5 | 48.5 |
| (Aw, 2020) [16] | Obs | Kenya | 1650 | 43–59 | 37 | 63 |
| (Treskes, 2019) [17] | Obs | Netherlands | 26 | 62–71 | 92 | 8 |
| (Devos, 2019) [18] | Obs | Belgium | 15 | 86.5 ± 5.95 | 40 | 60 |
| (Brittz, 2019) [19] | Exp | SA | 200 | 18–55 | 27 | 73 |
| (Uchino, 2018) [20] | Obs | Japan | 63 | 24–84 | 40 | 60 |
| (Toy, 2016) [21] | Obs | US | 50 | 60.5 ± 10.6 | 42 | 58 |
| (BinDhim, 2016) [22] | Obs | AU, Canada, UK, US, NZ | 2538 | 18–75 | 55 | 45 |
| (Kim, 2016) [23] | Obs | South Korea | 78 | 44.35 ± 7 | - | 100 |
| # | Country | Economic Status | Year-Wise Subscription Details | ||
|---|---|---|---|---|---|
| 2015 | 2017 | 2019 | |||
| 1 | Australia | Developed | 107.7 | 108.4 | 110.6 |
| 2 | Belgium | Developed | 113.2 | 99.5 | 99.7 |
| 3 | Canada | Developed | 82.6 | 86.3 | 92.5 |
| 4 | Iran | Developing | 94.6 | 107.9 | 142.4 |
| 5 | Japan | Developed | 125.5 | 135.5 | Not available |
| 6 | Kenya | Developing | 78.8 | 85.3 | 103.8 |
| 7 | Netherlands | Developed | 122.9 | 120.6 | 127.3 |
| 8 | New Zealand | Developed | 121.4 | 136.1 | Not available |
| 9 | South Africa | Developing | 158.9 | 155.2 | 165.6 |
| 10 | South Korea | Developing | 116.0 | 124.6 | 134.5 |
| 11 | United Kingdom | Developed | 120.3 | 118.5 | Not available |
| 12 | United States | Developed | 119.1 | 123.0 | Not available |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moses, J.C.; Adibi, S.; Wickramasinghe, N.; Nguyen, L.; Angelova, M.; Islam, S.M.S. Smartphone as a Disease Screening Tool: A Systematic Review. Sensors 2022, 22, 3787. https://doi.org/10.3390/s22103787
Moses JC, Adibi S, Wickramasinghe N, Nguyen L, Angelova M, Islam SMS. Smartphone as a Disease Screening Tool: A Systematic Review. Sensors. 2022; 22(10):3787. https://doi.org/10.3390/s22103787
Chicago/Turabian StyleMoses, Jeban Chandir, Sasan Adibi, Nilmini Wickramasinghe, Lemai Nguyen, Maia Angelova, and Sheikh Mohammed Shariful Islam. 2022. "Smartphone as a Disease Screening Tool: A Systematic Review" Sensors 22, no. 10: 3787. https://doi.org/10.3390/s22103787
APA StyleMoses, J. C., Adibi, S., Wickramasinghe, N., Nguyen, L., Angelova, M., & Islam, S. M. S. (2022). Smartphone as a Disease Screening Tool: A Systematic Review. Sensors, 22(10), 3787. https://doi.org/10.3390/s22103787