
Heart Rate Modeling and Prediction Using Autoregressive Models and Deep Learning

 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Wearable Device
2.3. Heart Rate
2.4. Models
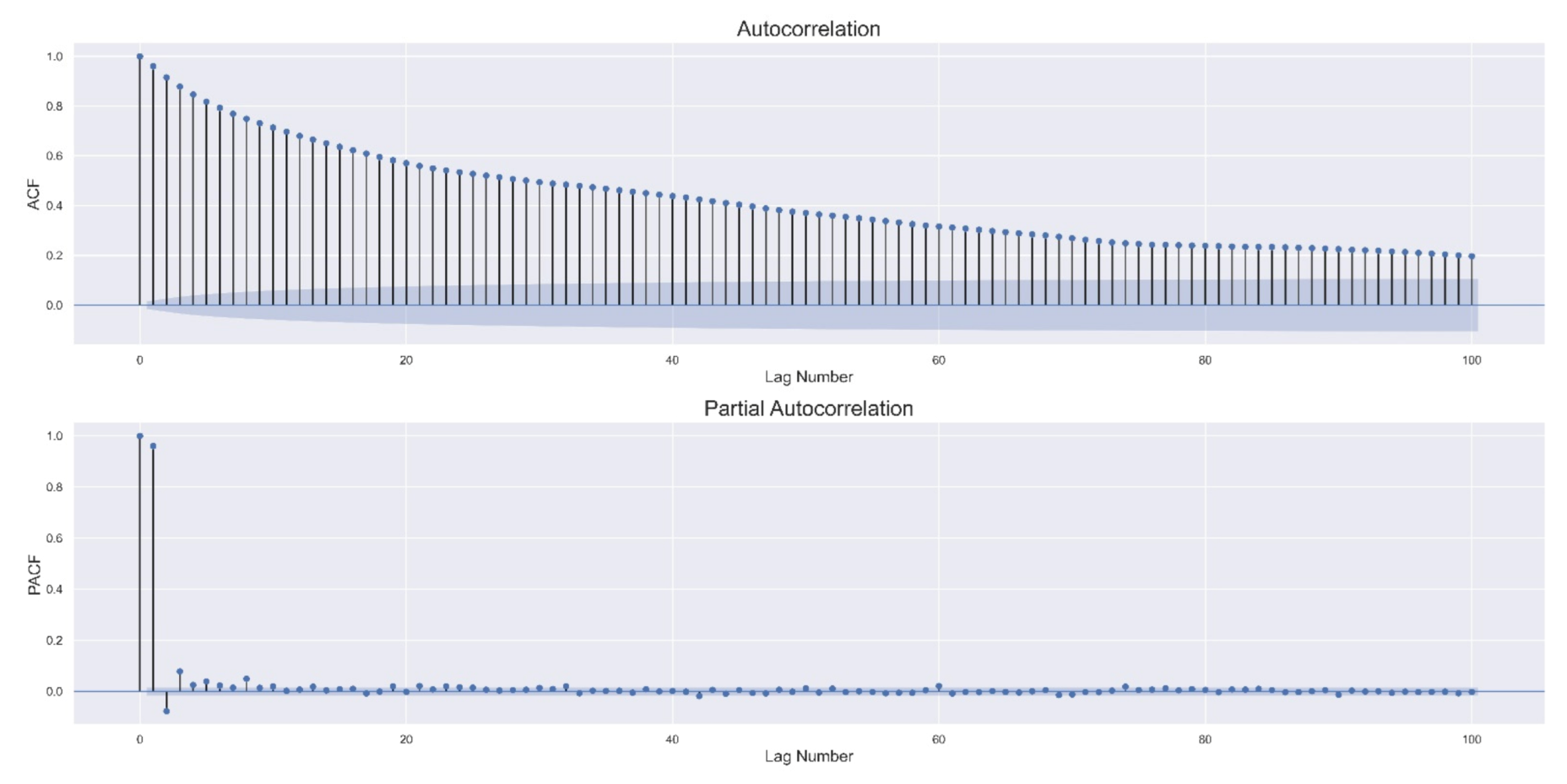
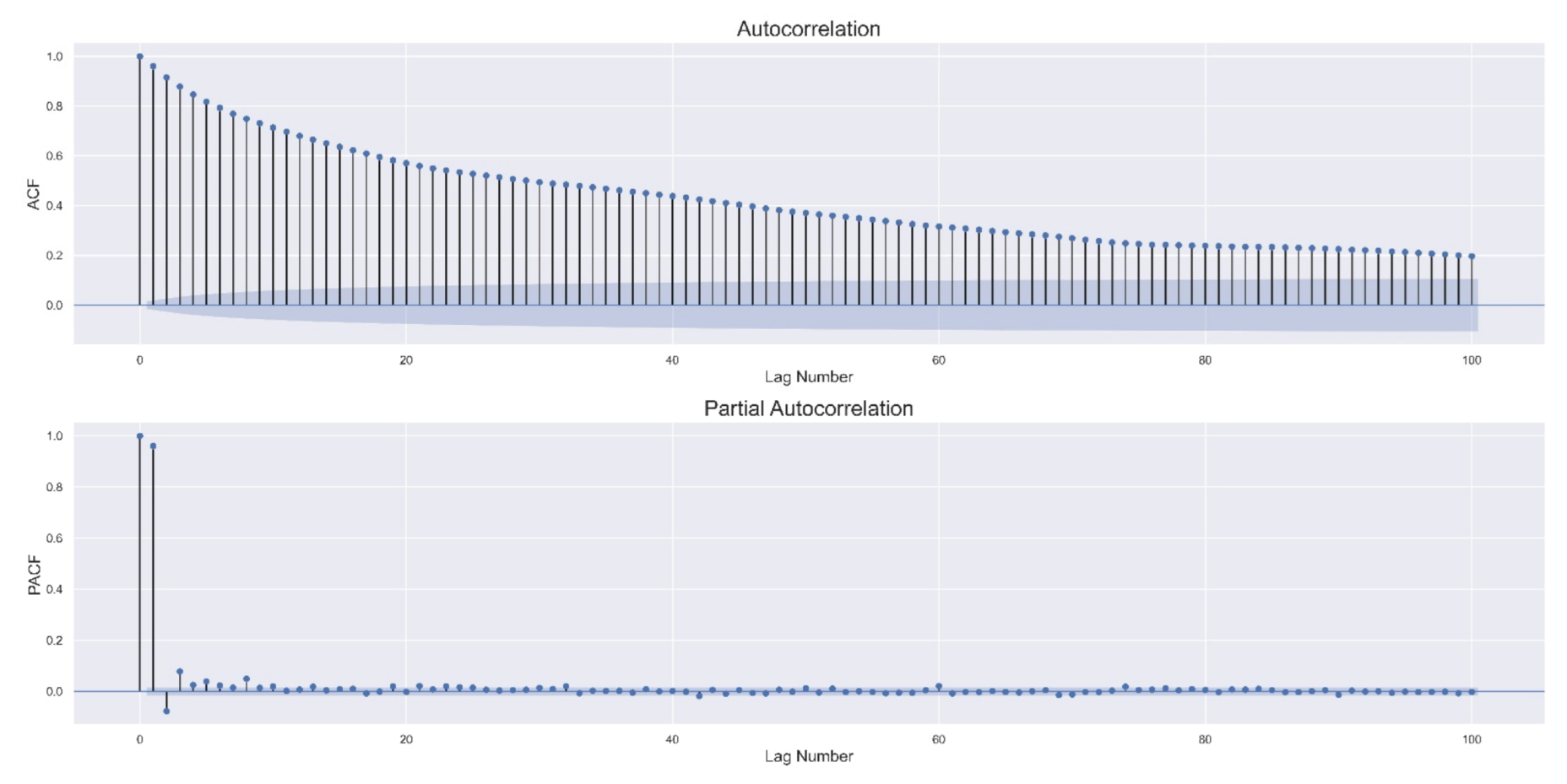
2.4.1. Autoregressive Process
2.4.2. Long Short-Term Memory Network (LSTM)
2.4.3. Convolutional Long Short-Term Memory Network (ConvLSTM)
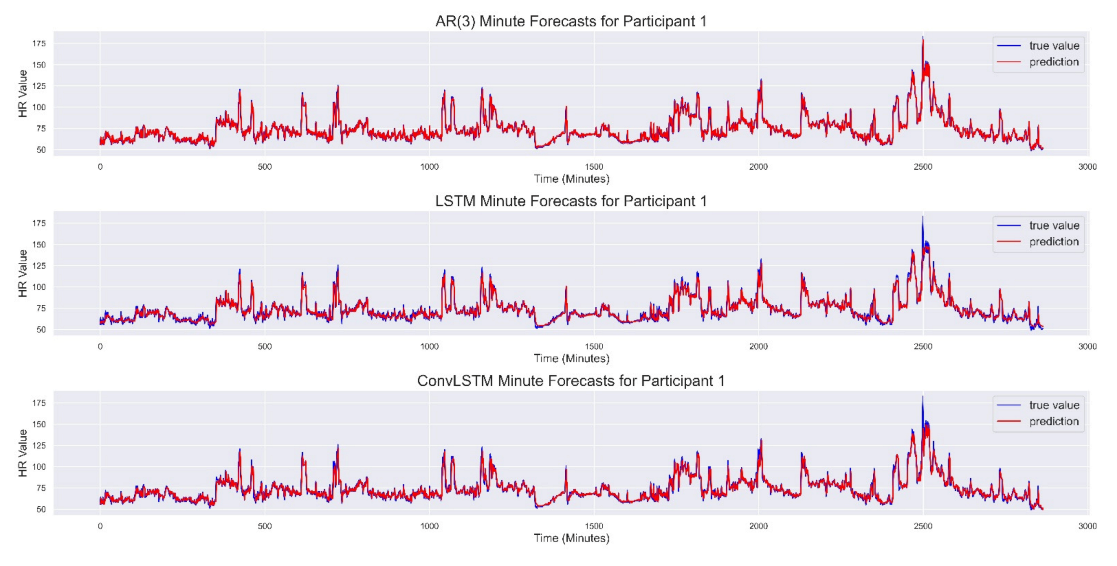
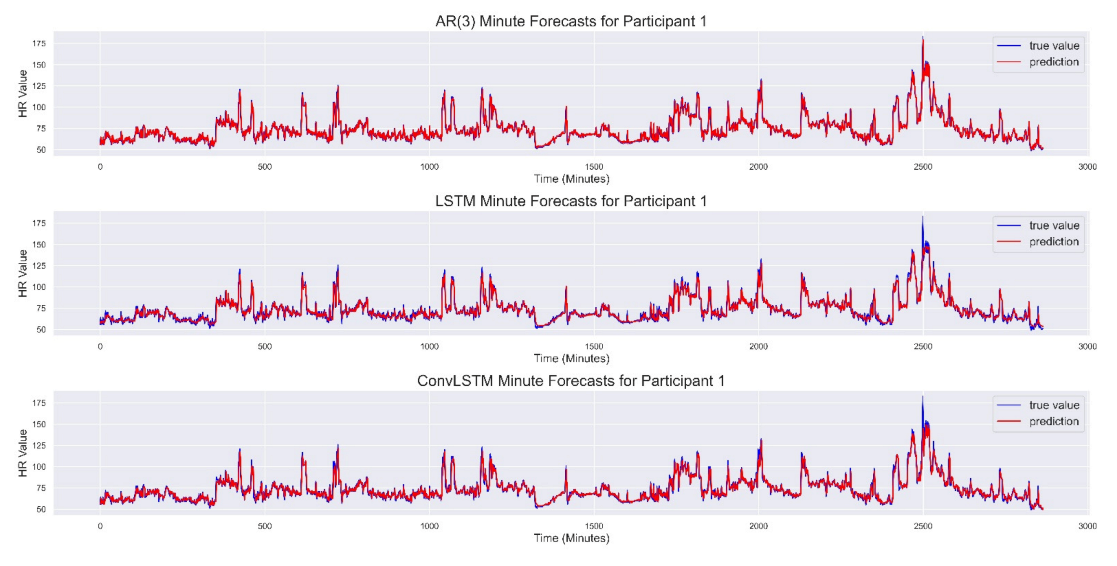
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Perret-Guillaume, C.; Joly, L.; Benetos, A. Heart rate as a risk factor for cardiovascular diseases. Prog. Cardiovasc. Dis. 2010, 52, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Dimietriev, D.A.; Saperova, E.V.; Dimietriev, A.D. State Anxiety and Nonlinear Dynamics of Heart Rate Variability in Students. PLoS ONE 2016, 11, e0146131. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nahshoni, E.; Aravot, D.; Aizenberg, D.; Sigler, M.; Zalsman, G.; Strasberg, B.; Imbar, S.; Adler, E.; Weizman, A. Heart rate variability in patients with major depression. Psychosomatics 2004, 45, 129–134. [Google Scholar] [CrossRef] [PubMed]
- Lutfi, M.F. Patterns of heart rate variability and cardiac autonomic modulations in controlled and uncontrolled asthmatic patients. BMC Pulm. Med. 2015, 15, 119. [Google Scholar] [CrossRef] [Green Version]
- Yun, S.; Son, C.S.; Lee, S.H.; Kang, W.S. Forecasting of heart rate variability using wrist-worn heart rate monitor based on hidden Markov model. In Proceedings of the 2018 International Conference on Electronics, Information and Communication (ICEIC), Honolulu, HI, USA, 24–27 January 2018. [Google Scholar] [CrossRef]
- Luo, M.; Wu, K. Heart rate prediction model based on neural network. IOP Conf. Ser. Mater. Sci. Eng. 2020, 715, 012060. [Google Scholar] [CrossRef]
- Christini, D.J.; Bennett, F.H.; Lutchen, K.R.; Ahmed, H.M.; Hausdroff, J.M.; Oriol, N. Application of linear and nonlinear time series modeling to heart rate dynamics analysis. IEEE Trans. Biomed. Eng. 1995, 42, 411–415. [Google Scholar] [CrossRef]
- Saalasti, S. Neural Networks for Heart Rate Time Series Analysis. In Jyväskylä Studies in Computing; Jyväskylä University: Jyväskylä, Finland, 2003. [Google Scholar]
- Reiss, A.; Indlekofer, I.; Schmidt, P.; Van Laerhoven, K. Deep PPG: Large-Scale Heart Rate Estimation with Convolutional Neural Networks. Sensors 2019, 19, 3079. [Google Scholar] [CrossRef] [Green Version]
- Gonzalez Viejo, C.; Fuentes, S.; Torrico, D.D.; Dunshea, F.R. Non-Contact Heart Rate and Blood Pressure Estimations from Video Analysis and Machine Learning Modelling Applied to Food Sensory Responses: A Case Study for Chocolate. Sensors 2018, 18, 1802. [Google Scholar] [CrossRef] [Green Version]
- Henriques, T.; Ribeiro, M.; Teixeira, A.; Castro, L.; Antunes, L.; Costa-Santos, C. Nonlinear Methods Most Applied to Heart-Rate Time Series: A Review. Entropy 2020, 22, 309. [Google Scholar] [CrossRef] [Green Version]
- Wearable Technology Market Report and Forecast 2021–2026. Available online: https://www.expertmarketresearch.com/reports/wearable-technology-market (accessed on 25 April 2021).
- Benedetto, S.; Caldato, C.; Bazzan, E.; Greenwood, D.C.; Pensabene, V.; Actis, P. Assessment of the Fitbit Charge 2 for monitoring heart rate. PLoS ONE 2018, 13, e0192691. [Google Scholar] [CrossRef] [Green Version]
- Yuchi, M.; Jo, J. Heart Rate Prediction Based on Physical Activity Using Feedforward Neural Network. In Proceedings of the 2008 International Conference on Convergence and Hybrid Information Technology, Daejeon, Korea, 28–30 August 2008; pp. 344–350. [Google Scholar] [CrossRef] [Green Version]
- Xiao, F.; Chen, Y.; Yuchi, M.; Ding, M.; Jo, J. Heart Rate Prediction Model Based on Physical Activities Using Evolutionary Neural Network. In Proceedings of the Fourth International Conference on Genetic and Evolutionary Computing, Washington, DC, USA, 13–15 December 2010; pp. 198–201. [Google Scholar] [CrossRef] [Green Version]
- Briganti, G.; Le Moine, O. Artificial Intelligence in Medicine: Today and Tomorrow. Front. Med. 2020, 7, 27. [Google Scholar] [CrossRef]
- Johnson, K.B.; Wei, W.Q.; Weeraratne, D.; Frisse, M.E.; Misulis, K.; Rhee, K.; Zhao, J.; Snowdon, J.L. Precision Medicine, AI, and the Future of Personalized Health Care. Clin. Transl. Sci. 2021, 14, 86–93. [Google Scholar] [CrossRef]
- Bates, D.W.; Levine, D.; Syrowatka, A.; Kuznetsovsa, M.; Craig, K.J.T.; Rui, A.; Jackson, G.P.; Rhee, K. The potential of artificial intelligence to improve patient safety: A scoping review. NPJ Digit. Med. 2021, 4, 54. [Google Scholar] [CrossRef]
- Kang, E.Y.C.; Hsieh, Y.T.; Li, C.H.; Huang, Y.H.; Kuo, C.F.; Kang, J.H.; Chen, K.J.; Lai, C.C.; Wu, W.C.; Hwang, Y.S. Deep Learning-Based Detection of Early Renal Function Impairment Using Retinal Fundus Images: Model Development and Validation. JMIR Med. Inform. 2020, 8, e23472. [Google Scholar] [CrossRef]
- Al-masni, M.A.; Al-antari, M.A.; Park, J.M.; Gi, G.; Kim, T.Y.; Rivera, P.; Valarezo, E.; Choi, M.T.; Han, S.M.; Kim, T.S. Simultaneous detection and classification of breast masses in digital mammograms via a deep learning YOLO-based CAD system. Comput. Methods Programs Biomed. 2018, 157, 85–94. [Google Scholar] [CrossRef]
- Kang, E.Y.C.; Yeung, L.; Lee, Y.L.; Wu, C.H.; Peng, S.Y.; Chen, Y.P.; Gao, Q.Z.; Lin, C.; Kuo, C.F.; Lai, C.C. A Multimodal Imaging-Based Deep Learning Model for Detecting Treatment-Requiring Retinal Vascular Diseases: Model Development and Validation Study. JMIR Med. Inform. 2021, 9, e28868. [Google Scholar] [CrossRef]
- Kim, H.M.; Lee, S.J.; Park, S.J.; Choi, I.Y.; Hong, S.H. Machine Learning Approach to Predict the Probability of Recurrence of Renal Cell Carcinoma After Surgery: Prediction Model Development Study. JMIR Med. Inform. 2021, 9, e25635. [Google Scholar] [CrossRef]
- Diao, X.; Huo, Y.; Yan, Z.; Wang, H.; Yuan, J.; Wang, Y.; Cai, J.; Zhao, W. An Application of Machine Learning to Etiological Diagnosis of Secondary Hypertension: Retrospective Study Using Electronic Medical Records. JMIR Med. Inform. 2021, 9, e19739. [Google Scholar] [CrossRef]
- Park, H.Y.; Bae, H.J.; Hong, G.S.; Kim, M.; Yun, J.H.; Park, S.; Chung, W.J.; Kim, N. Realistic High-Resolution Body Computed Tomography Image Synthesis by Using Progressive Growing Generative Adversarial Network: Visual Turing Test. JMIR Med. Inform. 2021, 9, e23328. [Google Scholar] [CrossRef]
- Middel, L.; Palm, C.; Erdt, M. Synthesis of Medical Images Using GANs. In Uncertainty for Safe Utilization of Machine Learning in Medical Imaging and Clinical Image-Based Procedures; Springer: Berlin/Heidelberg, Germany, 2019; pp. 125–134. [Google Scholar] [CrossRef]
- Islam, S.; Jahan, N.; Kathun, M.E. Cardiovascular Disease Forecast using Machine Learning Paradigms. In Proceedings of the 2020 Fourth International Conference on Computing Methodologies and Communication (ICCMC), Erode, India, 11–13 March 2020; pp. 487–490. [Google Scholar] [CrossRef]
- Maini, E.; Venkateswarlu, B.; Gupta, A. Applying Machine Learning Algorithms to Develop a Universal Cardiovascular Disease Prediction System. In Proceedings of the International Conference on Intelligent Data Communication Technologies and Internet of Things (ICICI), Coimbatore, India, 7–8 August 2018. [Google Scholar] [CrossRef]
- Aada, A.; Sakshi, T. Predicting diabetes in medical datasets using machine learning techniques. Int. J. Sci. Res. Eng. Trends 2019, 5, 257–267. [Google Scholar]
- McCoy, T.H.; Pellegrini, A.M.; Perlis, R.H. Assessment of time-series machine learning methods for forecasting hospital discharge volume. JAMA Netw. Open 2018, 1, 3–11. [Google Scholar] [CrossRef] [PubMed]
- Vyasm, P.; Pandit, D. Heartbeat Abnormality Detection using Machine Learning Models and Rate Variability (HRV) Data. Preprints 2018. [Google Scholar] [CrossRef]
- Ludwig, M.; Meenakshi Sundaram, A.; Füller, M.; Asteroth, A.; Prassler, E. On Modeling the Cardiovascular System and Predicting the Human Heart Rate under Strain. In Proceedings of the International Conference on Information and Communication Technologies for Ageing Well and eHealth, Lisbon, Portugal, 20–22 May 2015. [Google Scholar] [CrossRef] [Green Version]
- Emerenziani, G.P.; Ferrari, D.; Vaccaro, M.G.; Gallotta, M.C.; Migliaccio, S.; Lenzi, A.; Baldari, C.; Guidetti, L. Prediction equation to estimate heart rate at individual ventilatory threshold in female and male obese adults. PLoS ONE 2018, 13, e0197255. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agliari, E.; Barra, A.; Barra, O.A.; Fachechi, A.; Franceschi Vento, L.; Moretti, L. Detecting Cardiac Pathologies via Machine Learning on Heart-Rate Variability Time Series and Related Markers. Sci. Rep. 2020, 10, 8845. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Scirica, B.M.; Stultz, C.M.; Guttag, J.V. Beatquency domain and machine learning improve prediction of cardiovascular death after acute coronary syndrome. Sci. Rep. 2016, 6, srep34540. [Google Scholar] [CrossRef] [Green Version]
- Pietilä, J.; Mehrang, S.; Tolonen, J.; Helander, E.; Jimison, H.; Pavel, M.; Korhonen, I. Evaluation of the accuracy and reliability for photoplethysmography based heart rate and beat-to-beat detection during daily activities. IFMBE Proc. 2017, 65, 145–148. [Google Scholar] [CrossRef]
- Nelson, B.W.; Allen, N.B. Accuracy of Consumer Wearable Heart Rate Measurement during an Ecologically Valid 24-Hour Period: Intraindividual Validation Study. JMIR mHealth uHealth 2019, 7, e10828. [Google Scholar] [CrossRef]
- Lipovetsky, S. Pareto 80/20 law: Derivation via random partitioning. Int. J. Math. Educ. 2009, 40, 271–277. [Google Scholar] [CrossRef]
- Ghysels, E.; Marcellino, M. Applied Economic Forecasting Using Time Series Methods; Oxford University Press: Oxford, UK, 2018; ISBN 0190622016. [Google Scholar]
- Hochreiter, S.; Schmidhuber, J. Long short-time memory. Neural Comput. 1997, 9, 1735–1780. [Google Scholar] [CrossRef]
- Mozer, M.C. A Focused Backpropagation Algorithm for Temporal Pattern Recognition. Complex Syst. 1989, 3, 349–381. [Google Scholar]
- Goodfellow, I.; Bengio, Y.; Courville, A. Deep Learning; MIT Press: Cambridge, MA, USA, 2016; ISBN 0262035618. [Google Scholar]
- Srivastava, N.; Hinton, G.; Krizhevsky, A.; Sutskever, I.; Salakhutdinov, R. Dropout: A simple way to prevent neural networks from overfitting. J. Mach. Learn. Res. 2014, 15, 1929–1958. [Google Scholar]
- Kingma, D.P.; Ba, J. Adam: A Method for Stochastic Optimization. arXiv 2014, arXiv:1412.6980. Available online: https://arxiv.org/abs/1412.6980 (accessed on 1 May 2021).
- LeCun, Y.; Bottou, L.; Orr, G.B.; Muller, K.R. Efficient BackProp. In Neural Networks: Tricks of the Trade; Springer: Berlin/Heidelberg, Germany, 1998. [Google Scholar]
- Glorot, X.; Bengio, Y. Understanding the difficulty of training deep feedforward neural networks. J. Mach. Learn. Res. 2010, 9, 249–256. [Google Scholar]
- Calin, O. Deep Learning Architectures: A Mathematical Approach; Series in the Data Sciences; Springer: Berlin/Heidelberg, Germany, 2020; ISBN 978-3-030-36721-3. [Google Scholar]
- Shi, X.; Chen, Z.; Wang, H.; Yeung, D.Y. Convolutional LSTM Network: A Machine Learning Approach for Precipitation Nowcasting. arXiv 2015, arXiv:1506.04214. Available online: https://arxiv.org/abs/1506.04214 (accessed on 1 May 2021).
- Mathers, J.A.L.; Levy, R.L. Correlation of the Oxygen Saturation of the Blood and Changes in the Electrocardiogram, Blood Pressure, and Heart Rate During the Anoxemia Test. Circulation 1950, 1, 426–432. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.G.; Cheon, E.J.; Bai, D.S.; Lee, Y.H.; Koo, B.H. Stress and Heart Rate Variability: A Meta-Analysis and Review of the Literature. Psychiatry Investig. 2018, 15, 235–245. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
| Age (Decade) | Sex | Past Diseases | Present Diseases | Smoking/Drinking Habit | Exercise Habit | Examination Period | |
|---|---|---|---|---|---|---|---|
| Participant 1 | 30s | Female | No diseases | No diseases | Non-smoker; consumes alcohol 2–3 times per week | Exercises 1–2 days per week | 10 days |
| Participant 2 | 40s | Male | 3 diseases | No diseases | Past smoker; consumes alcohol 4 or more times per week | No exercise | 10 days |
| Participant 3 | 50s | Male | 2 diseases | 1 disease | Current smoker; consumes alcohol 4 or more times per week | Exercises 1–2 days per week | 10 days |
| Participant 4 | 30s | Male | No diseases | No diseases | Current smoker; consumes alcohol 2–3 times per week | No exercise | 10 days |
| Participant 5 | 30s | Male | No diseases | No diseases | Non-smoker; consumes alcohol 2–4 times per month | Exercises 3 or more days per week | 10 days |
| Participant 6 | 50s | Female | 1 disease | 1 disease | Non-smoker; consumes alcohol 4 or more times per week | Exercises 3 or more days per week | 10 days |
| Participant 7 | 40s | Female | 1 disease | 1 disease | Non-smoker; consumes alcohol 2–4 times per month | No exercise | 10 days |
| Participant 8 | 40s | Female | No diseases | No diseases | Non-smoker; consumes alcohol 2–3 times per week | No exercise | 10 days |
| Participant 9 | 30s | Male | 3 diseases | 3 diseases | Current smoker; consumes alcohol 4 or more times per week | No exercise | 10 days |
| Participant 10 | 40s | Female | No diseases | No diseases | Non-smoker; consumes alcohol 1 time or less per month | Exercises 1–2 days per week | 10 days |
| Participant 11 | 50s | Male | No diseases | No diseases | Past smoker; consumes alcohol 2–4 times per month | Exercises 1–2 days per week | 10 days |
| Participant 12 | 50s | Male | 1 disease | 1 disease | Non-smoker; consumes alcohol 4 or more times per week | Exercises 3 or more days per week | 10 days |
| Model | AR(3) | Stacked LSTM | ConvLSTM |
|---|---|---|---|
| Participant 1 | |||
| MAE | 3.058 | 3.104 (0.004) | 3.231 (0.011) |
| RMSE | 4.617 | 4.649 (0.018) | 4.984 (0.018) |
| Participant 2 | |||
| MAE | 2.644 | 2.716 (0.039) | 2.732 (0.004) |
| RMSE | 4.048 | 4.150 (0.066) | 4.271 (0.013) |
| Participant 3 | |||
| MAE | 2.557 | 2.585 (0.021) | 2.593 (0.007) |
| RMSE | 3.722 | 3.759 (0.021) | 3.792 (0.018) |
| Participant 4 | |||
| MAE | 3.194 | 3.331 (0.005) | 3.294 (0.006) |
| RMSE | 5.130 | 5.281 (0.050) | 5.453 (0.013) |
| Participant 5 | |||
| MAE | 2.069 | 2.173 (0.024) | 2.138 (0.024) |
| RMSE | 3.194 | 3.569 (0.079) | 3.420 (0.047) |
| Participant 6 | |||
| MAE | 2.879 | 3.056 (0.036) | 3.044 (0.008) |
| RMSE | 4.546 | 5.054 (0.058) | 5.026 (0.022) |
| Participant 7 | |||
| MAE | 2.731 | 2.794 (0.022) | 2.945 (0.007) |
| RMSE | 4.600 | 4.761 (0.049) | 5.038 (0.006) |
| Participant 8 | |||
| MAE | 2.767 | 2.814 (0.051) | 2.865 (0.009) |
| RMSE | 4.132 | 4.273 (0.101) | 4.425 (0.018) |
| Participant 9 | |||
| MAE | 2.907 | 2.926 (0.008) | 3.059 (0.013) |
| RMSE | 4.307 | 4.332 (0.014) | 4.471 (0.044) |
| Participant 10 | |||
| MAE | 2.236 | 2.494 (0.082) | 2.368 (0.005) |
| RMSE | 3.513 | 4.292 (0.198) | 3.857 (0.010) |
| Participant 11 | |||
| MAE | 2.253 | 2.306 (0.012) | 2.325 (0.010) |
| RMSE | 3.472 | 3.612 (0.020) | 3.693 (0.019) |
| Participant 12 | |||
| MAE | 3.128 | 3.167 (0.010) | 3.358 (0.008) |
| RMSE | 5.868 | 6.058 (0.027) | 6.527 (0.021) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Staffini, A.; Svensson, T.; Chung, U.-i.; Svensson, A.K. Heart Rate Modeling and Prediction Using Autoregressive Models and Deep Learning. Sensors 2022, 22, 34. https://doi.org/10.3390/s22010034
Staffini A, Svensson T, Chung U-i, Svensson AK. Heart Rate Modeling and Prediction Using Autoregressive Models and Deep Learning. Sensors. 2022; 22(1):34. https://doi.org/10.3390/s22010034
Chicago/Turabian StyleStaffini, Alessio, Thomas Svensson, Ung-il Chung, and Akiko Kishi Svensson. 2022. "Heart Rate Modeling and Prediction Using Autoregressive Models and Deep Learning" Sensors 22, no. 1: 34. https://doi.org/10.3390/s22010034
APA StyleStaffini, A., Svensson, T., Chung, U.-i., & Svensson, A. K. (2022). Heart Rate Modeling and Prediction Using Autoregressive Models and Deep Learning. Sensors, 22(1), 34. https://doi.org/10.3390/s22010034