
A Way of Bionic Control Based on EI, EMG, and FMG Signals

 , ,
, ,  ,
,  ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Equipment
2.1.1. Simultaneous EI and EMG Acquisition
2.1.2. Prototype of Sensor Systems
2.2. Isometric Grasping Stand
2.3. A Laboratory Complex for Simultaneous Acquisition of EI, EMG, and FMG Signals
2.4. Subjects
2.5. Experiments
2.5.1. The Basic Wristed Movements Considered
2.5.2. Location of Sensor Systems
2.5.3. Experiments Protocol
3. Results
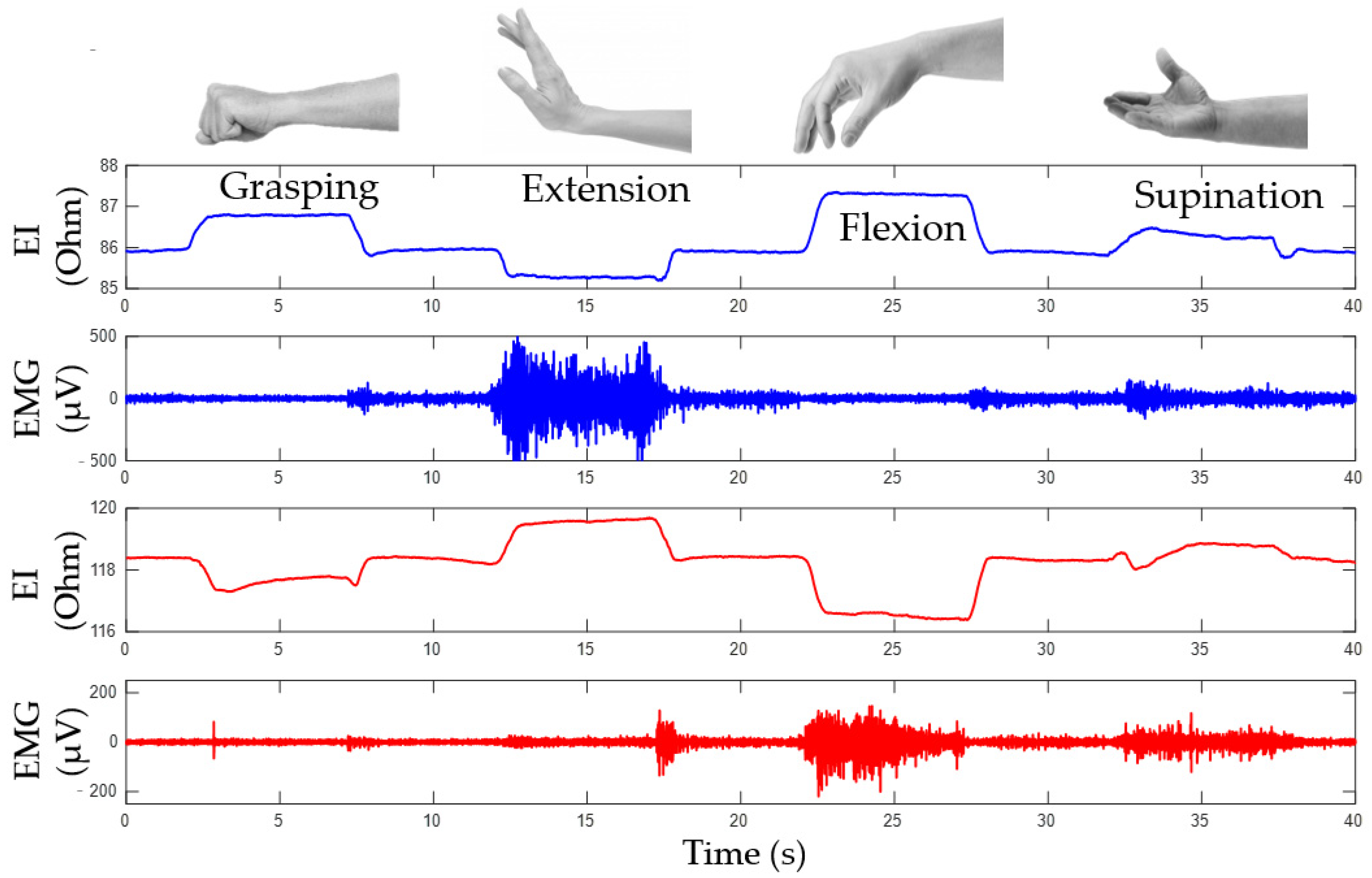
3.1. Simultaneous Analysis of EI and EMG Signals during Basic Wrist Movements
3.1.1. Determining Movement Type Based on EI Signal
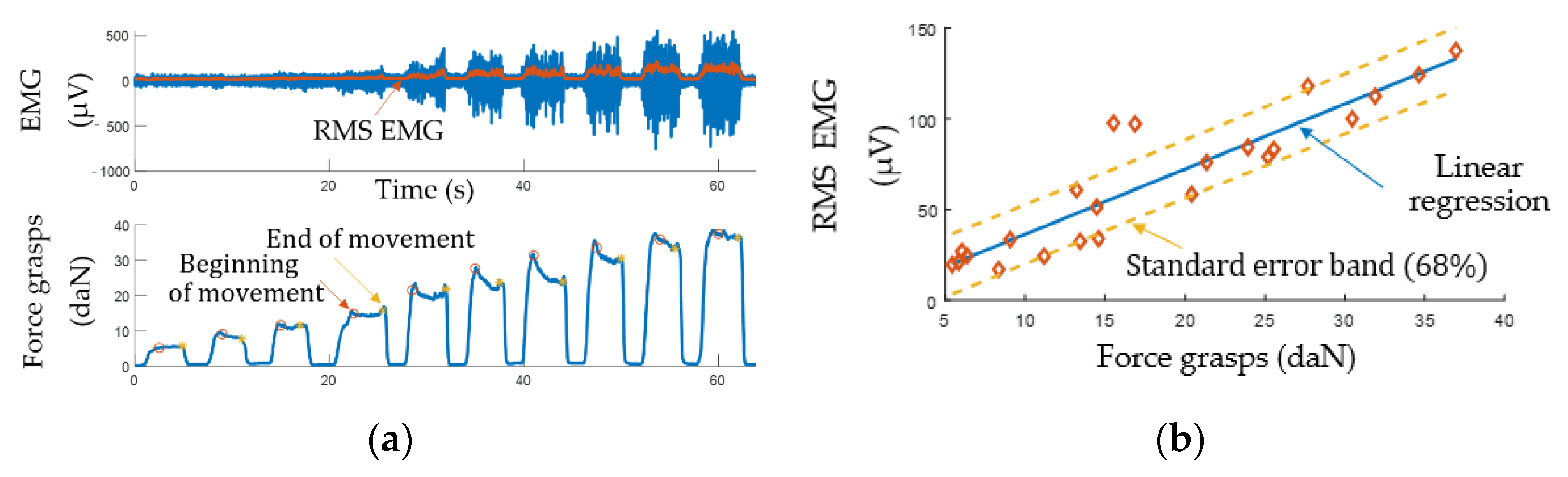
3.1.2. Determining Movement Intensity Based on EMG Signal
3.2. Simultaneous Analysis of EI and EMG Signals during Basic Wrist Movements
4. Discussion
4.1. Combining EMG, EI, and FMG Signals
4.2. Limitations
4.3. Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ingram, J.N.; Körding, K.P.; Howard, I.S.; Wolpert, D.M. The statistics of natural hand movements. Exp. Brain Res. 2008, 188, 223–236. [Google Scholar] [CrossRef] [PubMed]
- Mooney, L.M.; Rouse, E.J.; Herr, H.M. Autonomous exoskeleton reduces metabolic cost of human walking during load carriage. J. Neuroeng. Rehabil. 2014, 11, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Shahsavari, H.; Matourypour, P.; Ghiyasvandian, S.; Ghorbani, A.; Bakhshi, F.; Mahmoudi, M.; Golestannejad, M. Upper limb amputation; Care needs for reintegration to life: An integrative review. Int. J. Orthop. Trauma Nurs. 2020, 38, 100773. [Google Scholar] [CrossRef] [PubMed]
- Bajaj, N.M.; Spiers, A.J.; Dollar, A.M. State of the art in prosthetic wrists: Commercial and research devices. In Proceedings of the 2015 IEEE International Conference on Rehabilitation Robotics (ICORR), Singapore, 11–14 August 2015; pp. 331–338. [Google Scholar] [CrossRef]
- Belter, B.M.J.T.; Segil, J.L.; Dollar, B.S.P.A.M.; Weir, R.F. Mechanical design and performance specifications of anthropomorphic prosthetic hands: A review. J. Rehabil. Res. Dev. 2013, 50, 599–618. [Google Scholar] [CrossRef]
- Das, N.; Nagpal, N.; Bankura, S.S. A review on the advancements in the field of upper limb prosthesis. J. Med. Eng. Technol. 2018, 42, 532–545. [Google Scholar] [CrossRef] [PubMed]
- Wang, N.; Lao, K.; Zhang, X. Design and Myoelectric Control of an Anthropomorphic Prosthetic Hand. J. Bionic Eng. 2017, 14, 47–59. [Google Scholar] [CrossRef]
- Park, S.; Meeker, C.; Weber, L.M.; Bishop, L.; Stein, J.; Ciocarlie, M. Multimodal Sensing and Interaction for a Robotic Hand Orthosis. IEEE Robot. Autom. Lett. 2019, 4, 315–322. [Google Scholar] [CrossRef]
- Silveira, A.T.; De Souza, M.A.; Fernandes, B.L.; Nohama, P. From the past to the future of therapeutic orthoses for upper limbs rehabilitation. Res. Biomed. Eng. 2018, 34, 368–380. [Google Scholar] [CrossRef]
- Clement, R.; Bugler, K.; Oliver, C.W. Bionic prosthetic hands: A review of present technology and future aspirations. Surgeon 2011, 9, 336–340. [Google Scholar] [CrossRef] [PubMed]
- Lo, H.S.; Xie, S.Q. Exoskeleton robots for upper-limb rehabilitation: State of the art and future prospects. Med. Eng. Phys. 2012, 34, 261–268. [Google Scholar] [CrossRef]
- Cordella, F.; Ciancio, A.L.; Sacchetti, R.; Davalli, A.; Cutti, A.G.; Guglielmelli, E.; Zollo, L. Literature Review on Needs of Upper Limb Prosthesis Users. Front. Neurosci. 2016, 10, 209. [Google Scholar] [CrossRef] [PubMed]
- Fougner, A.; Stavdahl, Ø.; Kyberd, P.J.; Losier, Y.G.; Parker, P.A. Control of Upper Limb Prostheses: Terminology and Proportional Myoelectric Control—A Review. IEEE Trans. Neural Syst. Rehabil. Eng. 2012, 20, 663–677. [Google Scholar] [CrossRef] [PubMed]
- Kobelev, A.V.; Schukin, S.I. Antropomorphic control of forearm prosthesis based on electric impedance myography. Phys. Bases Instrum. 2019, 8, 62–68. [Google Scholar] [CrossRef]
- Sears, H.H.; Shaperman, J. Proportional myoelectric hand control: An evaluation. Am. J. Phys. Med. Rehabil. 1991, 70, 20–28. [Google Scholar] [CrossRef]
- Micera, S.; Carpaneto, J.; Raspopovic, S. Control of Hand Prostheses Using Peripheral Information. IEEE Rev. Biomed. Eng. 2010, 3, 48–68. [Google Scholar] [CrossRef]
- Smith, L.H.; Hargrove, L.J.; Lock, B.A.; Kuiken, T.A. Determining the Optimal Window Length for Pattern Recognition-Based Myoelectric Control: Balancing the Competing Effects of Classification Error and Controller Delay. IEEE Trans. Neural Syst. Rehabil. Eng. 2010, 19, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Fougner, A.; Scheme, E.; Chan, A.D.C.; Englehart, K.; Stavdahl, O. A multi-modal approach for hand motion classification using surface EMG and accelerometers. In Proceedings of the 2011 Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Boston, MA, USA, 30 August–3 September 2011; Volume 2011, pp. 4247–4250. [Google Scholar]
- Kusche, R.; Ryschka, M. Combining Bioimpedance and EMG Measurements for Reliable Muscle Contraction Detection. IEEE Sens. J. 2019, 19, 11687–11696. [Google Scholar] [CrossRef]
- Herrmann, S.; Attenberger, A.; Buchenrieder, K. Prostheses Control with Combined Near-Infrared and Myoelectric Signals. In Proceedings of the International Conference on Computer Aided Systems Theory, Las Palmas de Gran Canaria, Spain, 6–11 February 2011; Volume 6928, pp. 601–608. [Google Scholar]
- Wang, J.; Tang, L.; E Bronlund, J. Surface EMG Signal Amplification and Filtering. Int. J. Comput. Appl. 2013, 82, 15–22. [Google Scholar] [CrossRef]
- Mills, K.R. The basics of electromyography. J. Neurol. Neurosurg. Psychiatry 2005, 76, ii32–ii35. [Google Scholar] [CrossRef]
- Merletti, R.; Botter, A.; Troiano, A.; Merlo, E.; Minetto, M.A. Technology and instrumentation for detection and conditioning of the surface electromyographic signal: State of the art. Clin. Biomech. 2009, 24, 122–134. [Google Scholar] [CrossRef] [PubMed]
- Zwarts, M.J.; Stegeman, D.F. Multichannel surface EMG: Basic aspects and clinical utility. Muscle Nerve 2003, 28, 1–17. [Google Scholar] [CrossRef]
- Hogan, N. A review of the methods of processing EMG for use as a proportional control signal. Biomed. Eng. 1976, 11, 81–86. [Google Scholar]
- Zhang, T.; Wang, X.Q.; Jiang, L.; Wu, X.; Feng, W.; Zhou, D.; Liu, H. Biomechatronic design and control of an anthropomorphic artificial hand for prosthetic applications. Robotica 2016, 34, 2291–2308. [Google Scholar] [CrossRef]
- Tavakoli, M.; Benussi, C.; Lopes, P.A.; Osorio, L.B.; de Almeida, A.T. Robust hand gesture recognition with a double channel surface EMG wearable armband and SVM classifier. Biomed. Signal Process. Control. 2018, 46, 121–130. [Google Scholar] [CrossRef]
- Mao, H.; Fang, P.; Li, G. Simultaneous estimation of multi-finger forces by surface electromyography and accelerometry signals. Biomed. Signal Process. Control. 2021, 70, 103005. [Google Scholar] [CrossRef]
- Olsson, A.E.; Malešević, N.; Björkman, A.; Antfolk, C. Learning regularized representations of categorically labelled surface EMG enables simultaneous and proportional myoelectric control. J. Neuroeng. Rehabil. 2021, 18, 35. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Yu, Y.; Ma, S.; Sheng, X.; Lin, C.; Farina, D.; Zhu, X. Hand gesture recognition based on motor unit spike trains decoded from high-density electromyography. Biomed. Signal Process. Control. 2020, 55, 101637. [Google Scholar] [CrossRef]
- Del Vecchio, A.; Holobar, A.; Falla, D.; Felici, F.; Enoka, R.; Farina, D. Tutorial: Analysis of motor unit discharge characteristics from high-density surface EMG signals. J. Electromyogr. Kinesiol. 2020, 53, 102426. [Google Scholar] [CrossRef]
- Žagar, T.; Krizaj, D. Electrical impedance of relaxed and contracted skeletal muscle. In Proceedings of the 13th International Conference on Electrical Bioimpedance and the 8th Conference on Electrical Impedance Tomography, Graz, Austria, 29 August–2 September 2007; pp. 711–714. [Google Scholar]
- Rutkove, S.B. Electrical impedance myography: Background, current state, and future directions. Muscle Nerve 2009, 40, 936–946. [Google Scholar] [CrossRef]
- Sanchez, B.; Rutkove, S.B. Electrical Impedance Myography and Its Applications in Neuromuscular Disorders. Neurotherapeutics 2017, 14, 107–118. [Google Scholar] [CrossRef]
- A Shiffman, C.; Aaron, R.; Rutkove, S.B. Electrical impedance of muscle during isometric contraction. Physiol. Meas. 2003, 24, 213–234. [Google Scholar] [CrossRef]
- Al-Harosh, M.B.; Shchukin, S. Peripheral vein detection using electrical impedance method. J. Electr. Bioimpedance 2019, 8, 79–83. [Google Scholar] [CrossRef][Green Version]
- Sanchez, B.; Rutkove, S.B. Present Uses, Future Applications, and Technical Underpinnings of Electrical Impedance Myography. Curr. Neurol. Neurosci. Rep. 2017, 17, 86. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Jiang, D.; Liu, X.; Bayford, R.; Demosthenous, A. A Human–Machine Interface Using Electrical Impedance Tomography for Hand Prosthesis Control. IEEE Trans. Biomed. Circuits Syst. 2018, 12, 1322–1333. [Google Scholar] [CrossRef] [PubMed]
- Radmand, A.; Scheme, E.; Englehart, K. High-density force myography: A possible alternative for upper-limb prosthetic control. J. Rehabil. Res. Dev. 2016, 53, 443–456. [Google Scholar] [CrossRef]
- Echo, E.; Echen, R.; Emerhi, L.-K.; Exiao, Z.G.; Epousett, B.; Emenon, C. Force Myography to Control Robotic Upper Extremity Prostheses: A Feasibility Study. Front. Bioeng. Biotechnol. 2016, 4, 18. [Google Scholar] [CrossRef]
- Xiao, Z.G.; Menon, C. A Review of Force Myography Research and Development. Sensors 2019, 19, 4557. [Google Scholar] [CrossRef] [PubMed]
- Ravindra, V.; Ecastellini, C. A Comparative Analysis of Three Non-Invasive Human-Machine Interfaces for the Disabled. Front. Neurorobot. 2014, 8, 24. [Google Scholar] [CrossRef]
- Belyea, A.; Englehart, K.; Scheme, E. FMG Versus EMG: A Comparison of Usability for Real-Time Pattern Recognition Based Control. IEEE Trans. Biomed. Eng. 2019, 66, 3098–3104. [Google Scholar] [CrossRef]
- I Yaniger, S. Force Sensing Resistors: A Review Of The Technology. In Electro International, 1991; IEEE: New York, NY, USA, 1991; pp. 666–668. [Google Scholar]
- Castellini, C.; Artemiadis, P.; Ewininger, M.; Ajoudani, A.; Ealimusaj, M.; Ebicchi, A.; Caputo, B.; Ecraelius, W.; Dosen, S.; Eenglehart, K.; et al. Proceedings of the first workshop on Peripheral Machine Interfaces: Going beyond traditional surface electromyography. Front. Neurorobot. 2014, 8, 22. [Google Scholar] [CrossRef]
- Jiang, X.; Merhi, L.-K.; Xiao, Z.G.; Menon, C. Exploration of Force Myography and surface Electromyography in hand gesture classification. Med. Eng. Phys. 2017, 41, 63–73. [Google Scholar] [CrossRef] [PubMed]
- Connan, M.; Ramírez, E.R.; Vodermayer, B.; Castellini, C. Assessment of a Wearable Force- and Electromyography Device and Comparison of the Related Signals for Myocontrol. Front. Neurorobot. 2016, 10, 17. [Google Scholar] [CrossRef] [PubMed]
- Ha, N.; Withanachchi, G.P.; Yihun, Y. Performance of Forearm FMG for Estimating Hand Gestures and Prosthetic Hand Control. J. Bionic Eng. 2019, 16, 88–98. [Google Scholar] [CrossRef]
- Kobelev, A.; Shchukin, S.I. Anthropomorphic prosthesis control based on the electrical impedance signals analysis. In Proceedings of the 2018 Ural Symposium on Biomedical Engineering, Radioelectronics and Information Technology (USBEREIT), Yekaterinburg, Russia, 7–8 May 2018; pp. 33–36. [Google Scholar]
- Pliquett, U. XV International Conference on Electrical Bio-Impedance (ICEBI) & XIV Conference on Electrical Impedance Tomography (EIT). J. Phys. Conf. Ser. 2013, 434, 011001. [Google Scholar] [CrossRef]
- Luzhnov, P.V.; Kobelev, A.; Shchukin, S.I. Development of the method for impedance calibration in rheography. AIP Conf. Proc. 2019, 2140, 020039. [Google Scholar] [CrossRef]
- Briko, A.N.; Kobelev, A.; Shchukin, S.I. Electrodes interchangeability during electromyogram and bioimpedance joint recording. In Proceedings of the 2018 Ural Symposium on Biomedical Engineering, Radioelectronics and Information Technology (USBEREIT), Yekaterinburg, Russia, 7–8 May 2018; pp. 17–20. [Google Scholar]
- ABriko, N.; Chvanova, J.A.; Seliutina, S.E.; Ivanov, E.A.; Kobelev, A.V.; Shchukin, S.I. Stand of neuromuscular activity registration during isometric hand grab. Biomed. Radioelectron. 2018, 9–14. [Google Scholar] [CrossRef]
- Nakamura, Y.; Nagai, K.; Yoshikawa, T. Mechanics of coordinative manipulation by multiple robotic mechanisms. J. Robot. Soc. Jpn. 1986, 4, 489–498. [Google Scholar] [CrossRef]
- Cutkosky, M.; Kao, I. Computing and controlling compliance of a robotic hand. IEEE Trans. Robot. Autom. 1989, 5, 269–279. [Google Scholar] [CrossRef]
- Briko, A.; Kapravchuk, V.; Selutina, S.; Shchukin, S.; Gulyaev, Y.; Leonhardt, S. Amplitude Parameters of Electrical Impedance Myography with Different Pressure of the Electrode System Research. In Proceedings of the 2021 Ural Symposium on Biomedical Engineering, Radioelectronics and Information Technology (USBEREIT), Yekaterinburg, Russia, 13–14 May 2021; pp. 0129–0132. [Google Scholar]
- Hakonen, M.; Piitulainen, H.; Visala, A. Current state of digital signal processing in myoelectric interfaces and related applications. Biomed. Signal Process. Control. 2015, 18, 334–359. [Google Scholar] [CrossRef]
- Ebied, A.; Kinney-Lang, E.; Escudero, J. Higher order tensor decomposition for proportional myoelectric control based on muscle synergies. Biomed. Signal Process. Control. 2021, 67, 102523. [Google Scholar] [CrossRef]
- Briko, A.; Chvanova, J.; Kobelev, A.; Shchukin, S. Evaluation of the electrode system pressure force influence on neuro muscular activity signals. Int. J. Bioelectromagn. 2018, 20, 28–31. [Google Scholar]
- Briko, A.; Parnovskaya, A.; Larionova, M.; Dyachencova, S. Effect of Electrode Pressure on Neuromuscular Signals During Hand Movements. In Proceedings of the 2019 Ural Symposium on Biomedical Engineering, Radioelectronics and Information Technology (USBEREIT), Yekaterinburg, Russia, 25–26 April 2019; pp. 120–123. [Google Scholar]















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Value | ||
|---|---|---|---|
| Number of channels | 2 | ||
| Sampling frequency | 1 kHz | ||
| Types of acquired signals | EI | FMG | EMG |
| Maximum amplitude | 300 Ω | 10 daN | 3 mV |
| Measurement error | 10 mΩ | 0.01 daN | 10 μV |
| Signal frequency range | 0–40 Hz | 0–10 Hz | 50–500 Hz |
| Probing current amplitude | 5 mA | - | - |
| Probing current frequency | 75 kHz | - | - |
| Movement Type | ||||||
|---|---|---|---|---|---|---|
| Channel | Signal | Opening | Grasping | Flexion | Extension | Rotation |
| EI | “0” | “+1” | “+1” | “−1” | “+1” | |
| Upper | EMG | “0” | “0”/“+1” | “0” | “+1” | “+1” |
| FMG | “0” | “+1” | “+1” | “+1” | “+1” | |
| EI | “0” | “−1” | “−1” | “+1” | “+1” | |
| Lower | EMG | “0” | “0”/“+1” | “+1” | “0” | “+1” |
| FMG | “0” | “+1” | “+1” | “+1” | “+1” | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Briko, A.; Kapravchuk, V.; Kobelev, A.; Hammoud, A.; Leonhardt, S.; Ngo, C.; Gulyaev, Y.; Shchukin, S. A Way of Bionic Control Based on EI, EMG, and FMG Signals. Sensors 2022, 22, 152. https://doi.org/10.3390/s22010152
Briko A, Kapravchuk V, Kobelev A, Hammoud A, Leonhardt S, Ngo C, Gulyaev Y, Shchukin S. A Way of Bionic Control Based on EI, EMG, and FMG Signals. Sensors. 2022; 22(1):152. https://doi.org/10.3390/s22010152
Chicago/Turabian StyleBriko, Andrey, Vladislava Kapravchuk, Alexander Kobelev, Ahmad Hammoud, Steffen Leonhardt, Chuong Ngo, Yury Gulyaev, and Sergey Shchukin. 2022. "A Way of Bionic Control Based on EI, EMG, and FMG Signals" Sensors 22, no. 1: 152. https://doi.org/10.3390/s22010152
APA StyleBriko, A., Kapravchuk, V., Kobelev, A., Hammoud, A., Leonhardt, S., Ngo, C., Gulyaev, Y., & Shchukin, S. (2022). A Way of Bionic Control Based on EI, EMG, and FMG Signals. Sensors, 22(1), 152. https://doi.org/10.3390/s22010152