
EMG Based Analysis of Gait Symmetry in Healthy Children

 ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
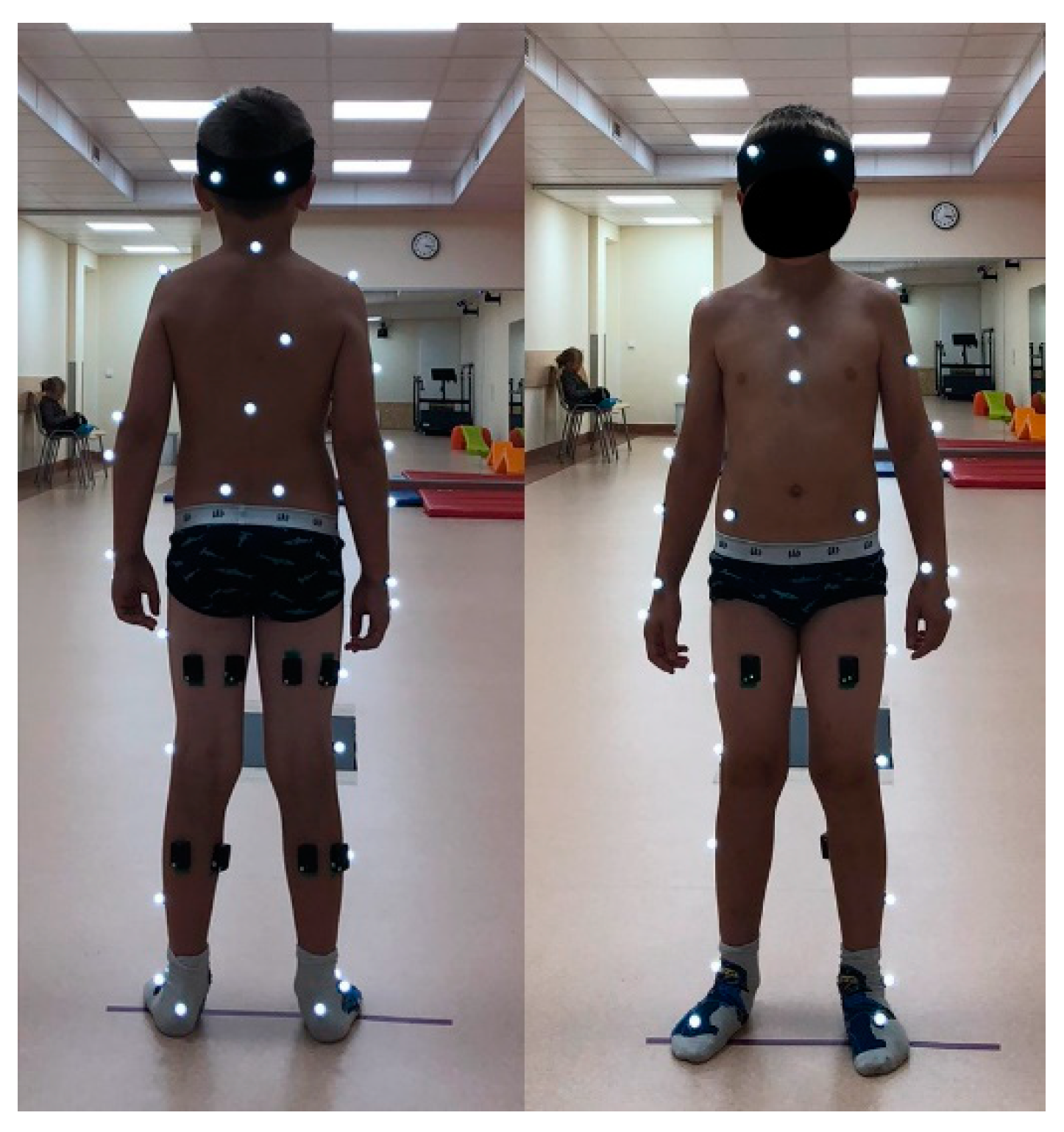
2.1. Subjects and Procedure
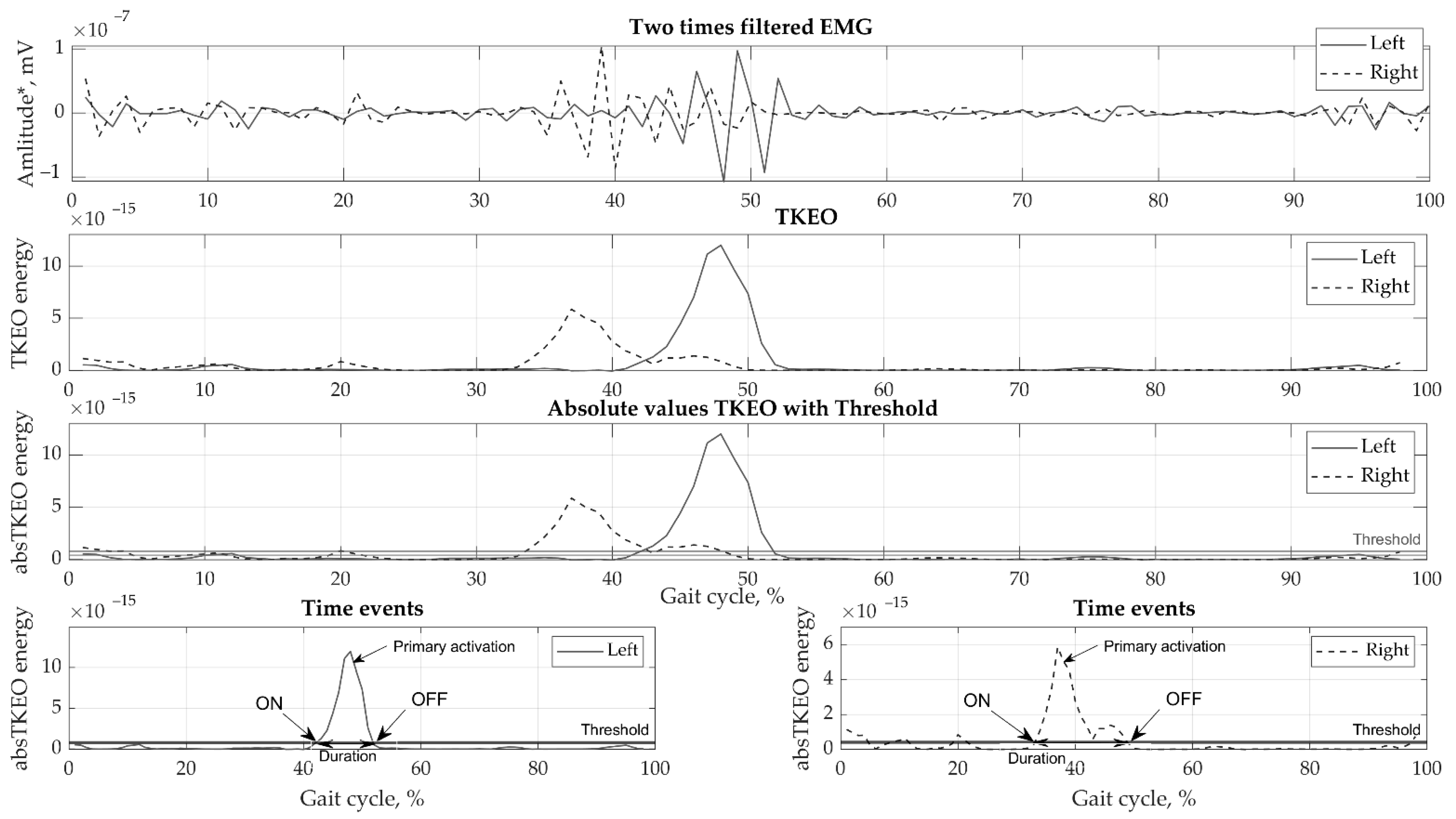
2.2. Signal Acquisition and Processing
2.3. Statistical Analysis
3. Results
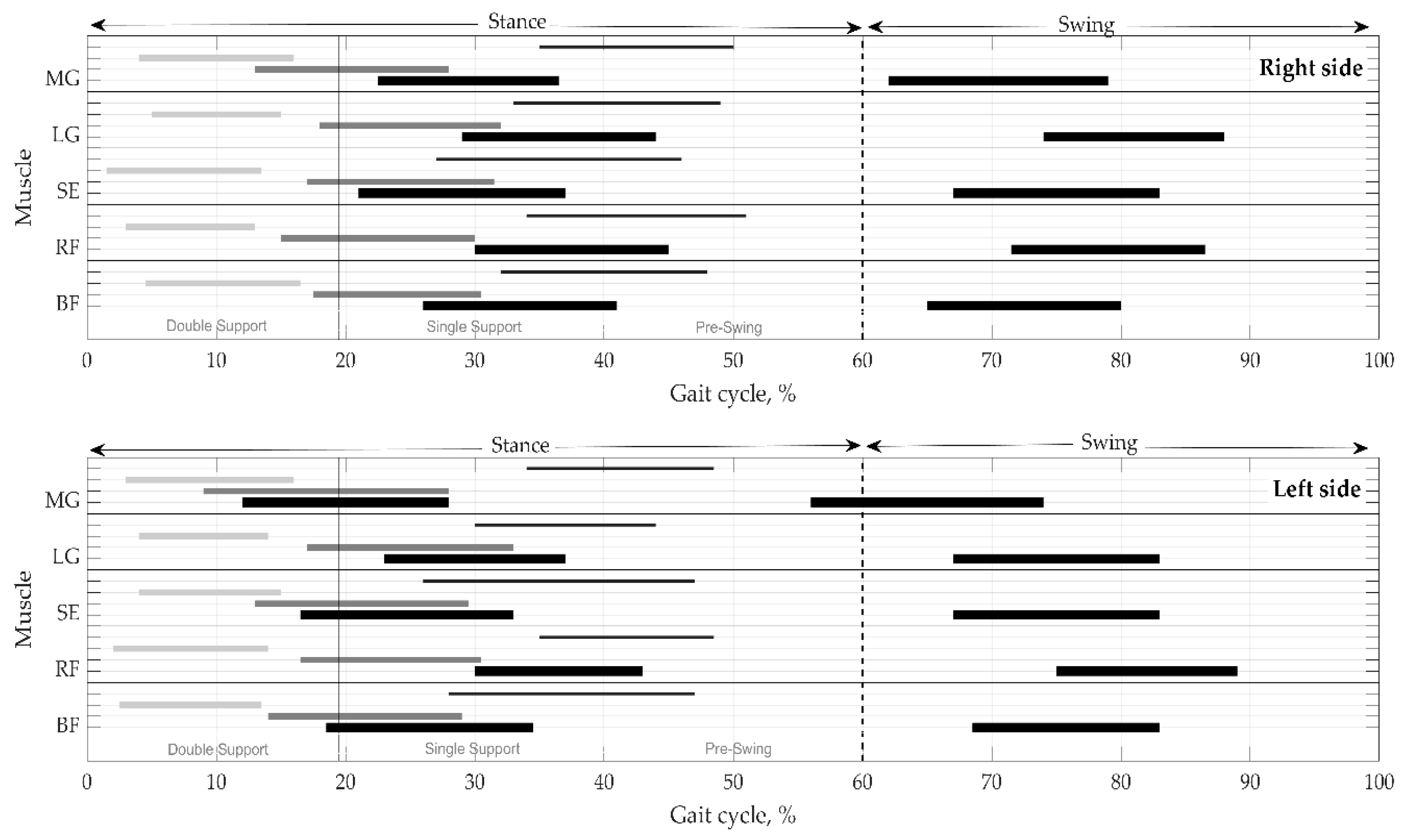
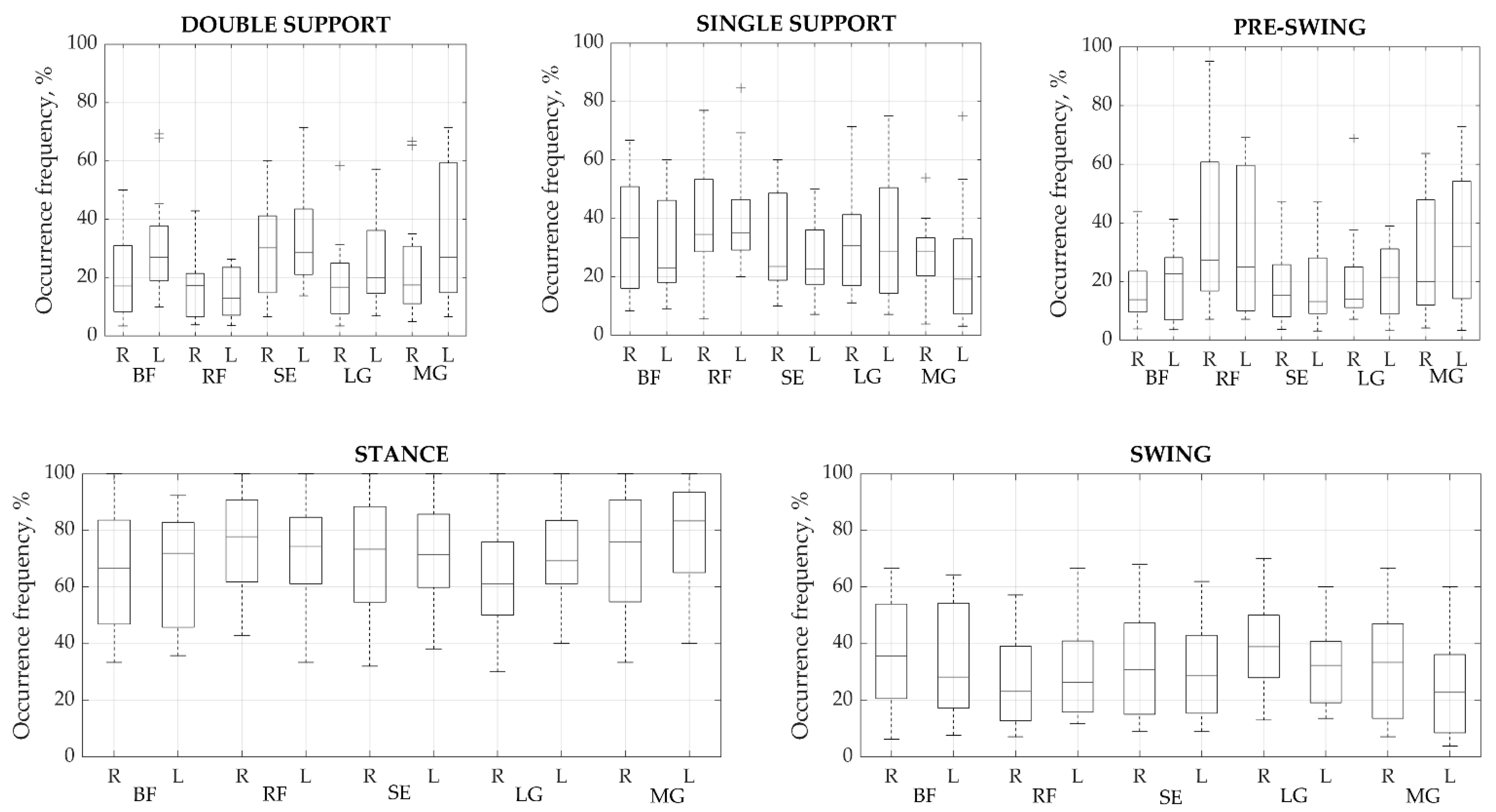
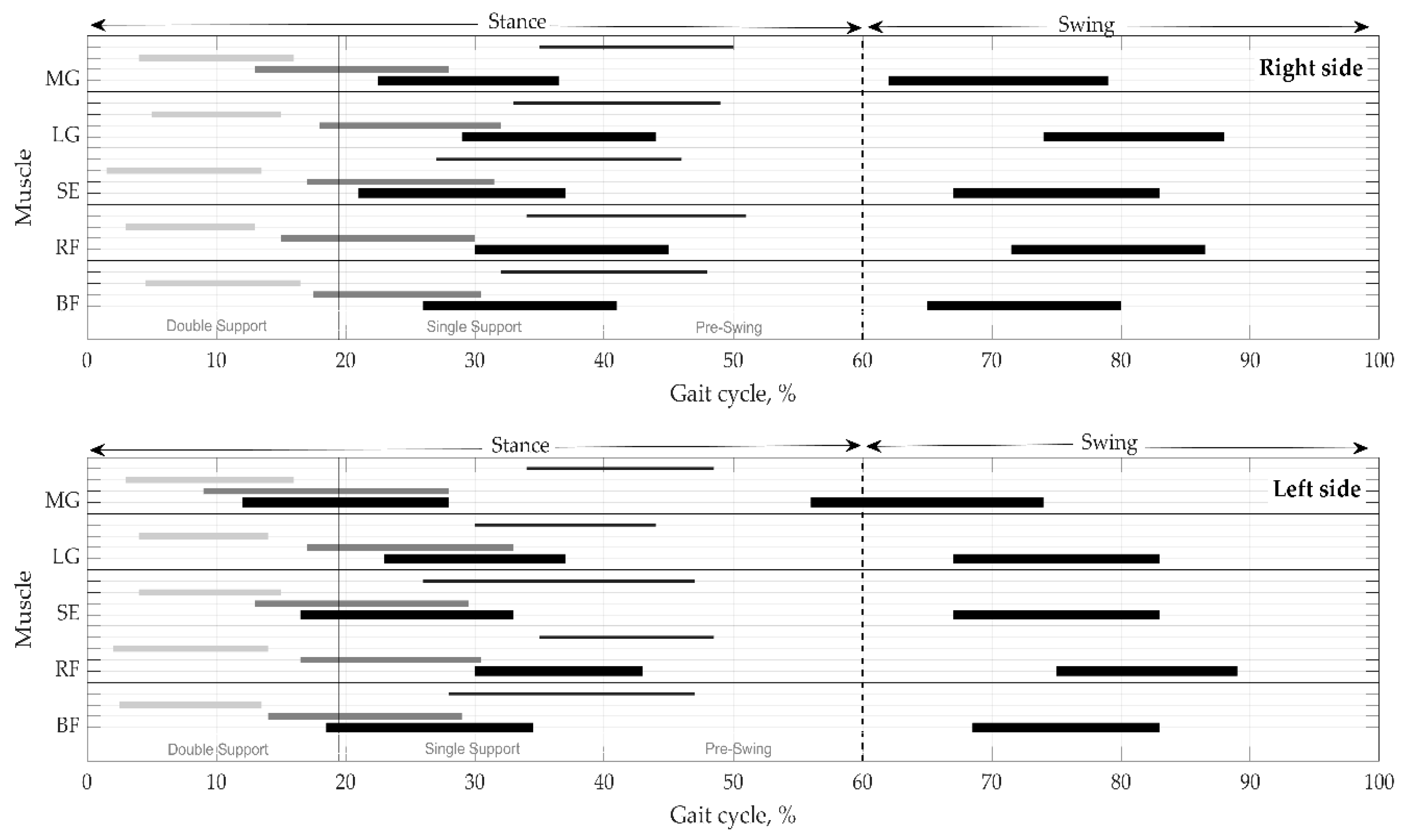
3.1. Primary Activation Modality and Time Parameters
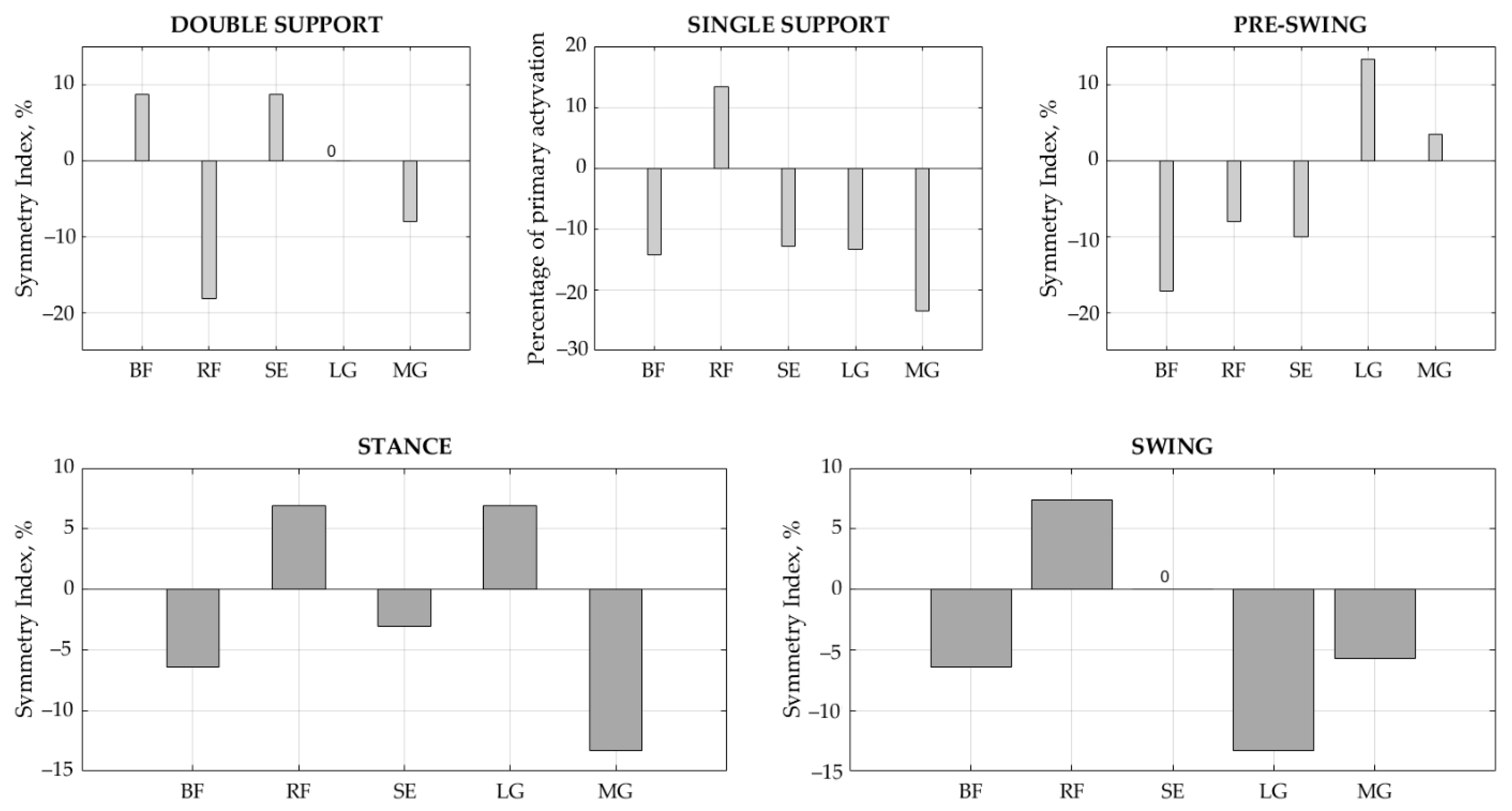
3.2. Symmetry Indices
4. Discussion
4.1. Muscular Activation
4.2. Temporal Parameters and Symmetry Indices
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Di Nardo, F.; Mengarelli, A.; Burattini, L.; Maranesi, E.; Agostini, V.; Nascimbeni, A.; Knaflitz, M.; Fioretti, S. Normative EMG patterns of ankle muscle co-contractions in school-age children during gait. Gait Posture 2016, 46, 161–166. [Google Scholar] [CrossRef]
- Agostini, V.; Nascimbeni, A.; Gaffuri, A.; Imazio, P.; Benedetti, M.G.; Knaflitz, M. Normative EMG activation patterns of school-age children during gait. Gait Posture 2010, 32, 285–289. [Google Scholar] [CrossRef] [Green Version]
- Granata, K.P.; Padua, D.A.; Abel, M.F. Repeatability of surface EMG during gait in children. Gait Posture 2005, 22, 346–350. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knarr, B.A.; Zeni, J.A.; Higginson, J.S. Comparison of electromyography and joint moment as indicators of co-contraction. J. Electromyogr. Kinesiol. 2012, 22, 607–611. [Google Scholar] [CrossRef] [Green Version]
- Patikas, D.; Wolf, S.I.; Schuster, W.; Armbrust, P.; Dreher, T.; Döderlein, L. Electromyographic patterns in children with cerebral palsy: Do they change after surgery? Gait Posture 2007, 26, 362–371. [Google Scholar] [CrossRef]
- Wołczowski, A.; Zdunek, R. Electromyography and mechanomyography signal recognition: Experimental analysis using multi-way array decomposition methods. Biocybern. Biomed. Eng. 2017, 37, 103–113. [Google Scholar] [CrossRef]
- Schutte, L.M.; Narayanan, U.; Stout, J.L.; Selber, P.; Gage, J.R.; Schwartz, M.H. An index for quantifying deviations from normal gait. Gait Posture 2000, 11, 25–31. [Google Scholar] [CrossRef] [Green Version]
- Kadaba, M.P.; Ramakrishnan, H.K.; Wootten, M.E.; Gainey, J.; Gorton, G.; Cochran, G.V.B. Repeatability of kinematic, kinetic, and electromyographic data in normal adult gait. J. Orthop. Res. 1989, 7, 849–860. [Google Scholar] [CrossRef]
- Di Nardo, F.; Laureati, G.; Strazza, A.; Mengarelli, A.; Burattini, L.; Agostini, V.; Nascimbeni, A.; Knaflitz, M.; Fioretti, S. Is child walking conditioned by gender? Surface EMG patterns in female and male children. Gait Posture 2017, 53, 254–259. [Google Scholar] [CrossRef]
- Bisi, M.C.; Riva, F.; Stagni, R. Measures of gait stability: Performance on adults and toddlers at the beginning of independent walking. J. NeuroEng. Rehabil. 2014, 11, 131. [Google Scholar] [CrossRef] [Green Version]
- Bisi, M.C.; Stagni, R. Development of gait motor control: What happens after a sudden increase in height during adolescence? BioMedical Eng. Online 2016, 15, 47. [Google Scholar] [CrossRef] [Green Version]
- Beck, R.J.; Andriacchi, T.P.; Kuo, K.N.; Fermier, R.W.; Galante, J.O. Changes in the gait patterns of growing children. J. Bone Jt. Surg. 1981, 63, 1452–1457. [Google Scholar] [CrossRef]
- Okamoto, T.; Okamoto, K.; Andrew, P.D. Electromyographic developmental changes in one individual from newborn stepping to mature walking. Gait Posture 2003, 17, 18–27. [Google Scholar] [CrossRef]
- Sutherland, D. The development of mature gait. Gait Posture 1997, 6, 163–170. [Google Scholar] [CrossRef]
- Den Otter, A.R.; Geurts, A.C.H.; Mulder, T.; Duysens, J. Speed related changes in muscle activity from normal to very slow walking speeds. Gait Posture 2004, 19, 270–278. [Google Scholar] [CrossRef] [Green Version]
- Hof, A.L.; Elzinga, H.; Grimmius, W.; Halbertsma, J.P.K. Speed dependence of averaged EMG profiles in walking. Gait Posture 2002, 16, 78–86. [Google Scholar] [CrossRef] [Green Version]
- Tirosh, O.; Sangeux, M.; Wong, M.; Thomason, P.; Graham, H.K. Walking speed effects on the lower limb electromyographic variability of healthy children aged 7-16years. J. Electromyogr. Kinesiol. 2013, 23, 1451–1459. [Google Scholar] [CrossRef]
- Di Nardo, F.; Strazza, A.; Mengarelli, A.; Ercolani, S.; Morgoni, N.; Burattini, L.; Agostini, V.; Knaflitz, M.; Fioretti, S. Surface EMG patterns for quantification of thigh muscle co-contraction in school-age children: Normative data during walking. Gait Posture 2018, 61, 25–33. [Google Scholar] [CrossRef]
- Rosengren, K.S.; Deconinck, F.J.A.; DiBerardino, L.A.; Polk, J.D.; Spencer-Smith, J.; De Clercq, D.; Lenoir, M. Differences in gait complexity and variability between children with and without Developmental Coordination Disorder. Gait Posture 2009, 29, 225–229. [Google Scholar] [CrossRef]
- Di Nardo, F.; Strazza, A.; Mengarelli, A.; Cardarelli, S.; Tigrini, A.; Verdini, F.; Nascimbeni, A.; Agostini, V.; Knaflitz, M.; Fioretti, S. EMG-based characterization of walking asymmetry in children with mild hemiplegic cerebral palsy. Biosensors 2019, 9, 82. [Google Scholar] [CrossRef] [Green Version]
- Solnik, S.; Rider, P.; Steinweg, K.; Devita, P.; Hortobágyi, T. Teager-Kaiser energy operator signal conditioning improves EMG onset detection. Eur. J. Appl. Physiol. 2010, 110, 489–498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Currie, S.J.; Myers, C.A.; Krishnamurthy, A.; Enebo, B.A.; Davidson, B.S. Methods of Muscle Activation Onset Timing Recorded during Spinal Manipulation. J. Manip. Physiol. Ther. 2016, 39, 279–287. [Google Scholar] [CrossRef] [Green Version]
- Kaur, A.; Agarwal, R.; Kumar, A. Adaptive threshold method for peak detection of surface electromyography signal from around shoulder muscles. J. Appl. Stat. 2018, 45, 714–726. [Google Scholar] [CrossRef]
- Özgünen, K.T.; Çelik, U.; Kurdak, S.S. Determination of an optimal threshold value for muscle activity detection in EMG analysis. J. Sports Sci. Med. 2010, 9, 620–628. [Google Scholar] [PubMed]
- Strazza, A.; Mengarelli, A.; Fioretti, S.; Burattini, L.; Agostini, V.; Knaflitz, M.; Di Nardo, F. Surface-EMG analysis for the quantification of thigh muscle dynamic co-contractions during normal gait. Gait Posture 2017, 51, 228–233. [Google Scholar] [CrossRef] [PubMed]
- Scott VanZant, R.; McPoil, T.G.; Cornwall, M.W. Symmetry of plantar pressures and vertical forces in healthy subjects during walking. J. Am. Podiatr. Med. Assoc. 2001, 91, 337–342. [Google Scholar] [CrossRef]
- Thevenon, A.; Gabrielli, F.; Lepvrier, J.; Faupin, A.; Allart, E.; Tiffreau, V.; Wieczorek, V. Collection of normative data for spatial and temporal gait parameters in a sample of French children aged between 6 and 12. Ann. Phys. Rehabil. Med. 2015, 58, 139–144. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Nardo, F.; Mengarelli, A.; Maranesi, E.; Burattini, L.; Fioretti, S. Gender differences in the myoelectric activity of lower limb muscles in young healthy subjects during walking. Biomed. Signal Process. Control 2015, 19, 14–22. [Google Scholar] [CrossRef]
- Sadeghi, H.; Allard, P.; Prince, F.; Labelle, H. Symmetry and limb dominance in able-bodied gait: A review. Gait Posture 2000, 12, 34–45. Available online: www.elsevier.com/locate/gaitpost (accessed on 2 June 2021). [CrossRef]
- Ivanenko, Y.P.; Poppele, R.E.; Lacquaniti, F. Five basic muscle activation patterns account for muscle activity during human locomotion. J. Physiol. 2004, 556, 267–282. [Google Scholar] [CrossRef]
- Akl, A.R.; Gonçalves, P.; Fonseca, P.; Hassan, A.; Vilas-Boas, J.P.; Conceição, F. Muscle co-activation around the knee during different walking speeds in healthy females. Sensors 2021, 21, 677. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Age (years) | Height (cm) | BMI (kg/m2) | Pelvic Width (mm) | Knee Joint Width (mm) | Ankle Joint Width (mm) | Leg Length (mm) | Shoulder Offset (mm) | |
|---|---|---|---|---|---|---|---|---|
| Male (n = 6) | 9.0 ± 1.6 | 134.0 ± 10.9 | 15.9 ± 1.8 | 213.3 ± 31.4 | 86 ± 8.7 | 59.8 ± 4.6 | 725.0 ± 80.6 | 49.2 ± 16.6 |
| Female (n = 11) | 7.6 ± 2.0 | 129.9 ± 10.8 | 16.6 ± 2.4 | 205.0 ± 42.6 | 83.8 ± 9.6 | 56.3 ± 4.7 | 609.5 ± 72.2 | 39.8 ± 5.5 |
| All | 8.1 ± 1.9 | 131.4 ± 10.7 | 16.4 ± 2.2 | 207.9 ± 38.2 | 84.6 ± 9.1 | 57.5 ± 4.9 | 702.7 ± 74.7 | 62.4 ± 6.1 |
| Muscle | Actual Number of Activations per Cycle | Difference (Activation) | |
|---|---|---|---|
| Right | Left | ||
| BF | 2.55 | 2.68 | 0.13 |
| RF | 3.29 | 2.94 | 0.35 |
| SE | 2.83 | 2.66 | 0.16 |
| LG | 2.67 | 2.58 | 0.09 |
| MG | 2.16 | 2.32 | 0.16 |
| Muscle | Primary Activation Duration per Cycle, % | |
|---|---|---|
| Right Leg | Left Leg | |
| BF | 15 (5.10) | 16 (5.79) |
| RF | 14 (5.14) | 14 (5.14) |
| SE | 16 (5.97) | 16 (6.21) |
| LG | 14 (4.66) | 15 (5.09) |
| MG | 16 (6.06) | 17 (5.62) |
| Phases * | Right Leg | Left Leg |
|---|---|---|
| Mean ± SD | Mean ± SD | |
| Stance phase (double support + single support + pre-swing; %) | 0–59.7 ± 4.9 | 0–59.3 ± 4.8 |
| Double support (heelstrike + load response; %) | 0–19.5 ± 9.0 | 0–19.5 ± 8.9 |
| Single support (%) | 19.5 ± 9.0–40.2 ± 5.1 | 19.5 ± 8.9–39.7 ± 5.5 |
| Pre-swing (%) | 40.2 ± 5.1–59.7 ± 4.9 | 39.7 ± 5.5–59.3 ± 4.8 |
| Swing phase (stance phase–100; %) | 59.7 ± 4.9–100 ± 4.9 | 59.3 ± 4.8–100 ± 4.8 |
| Muscle | Time Inst. | Stance (%) | Swing (%) | Double Support (%) | Single Support (%) | Pre-Swing (%) | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Right | Left | Right | Left | Right | Left | Right | Left | Right | Left | ||
| BF | ON | 26 (9.9) | 18.5 (9.3) | 73 (10.4) | 71 (11.9) | 4.5 (2.6) | 2.5 (2.0) | 17.5 (7.8) | 14 (6.5) | 32(6.9) | 28 (6.5) |
| OFF | 43 (9.7) | 38.5 (10.14) | 91 (9.2) | 89 (10.1) | 16 (1.7) | 13.5 (2.5) | 31.5 (5.6) | 30 (5.3) | 48.5(4.5) | 47 (4.2) | |
| RF | ON | 30 (11.2) | 30 (11.3) | 62 (14.63) | 69 (16.3) | 2 (2.1) | 2.5 (1.4) | 15 (8.5) | 15.50 (7.4) | 34(6.3) | 35 (5.7) |
| OFF | 47 (11.2) | 46 (11.3) | 79 (12.8) | 86 (13.6) | 14 (2.5) | 15.5 (3.2) | 34 (7.2) | 26.50 (6.1) | 52.5(4.4) | 50 (4.4) | |
| SE | ON | 21 (8.9) | 16.5 (9.0) | 67 (11.5) | 67 (11.2) | 1.5 (2.1) | 4 (1.9) | 17 (5.4) | 13 (6.2) | 27(7.3) | 26 (7.4) |
| OFF | 41 (9.5) | 37 (10.5) | 86 (9.8) | 85 (8.7) | 14.5 (2.4) | 15.5 (2.2) | 33 (5.2) | 31.50 (4.9) | 47(4.1) | 47 (4.4) | |
| LG | ON | 29 (9.9) | 23 (10.4) | 74 (10.4) | 67 (11.6) | 5 (2.8) | 4 (2.0) | 18 (7.5) | 17 (7.2) | 33(5.4) | 30 (5.5) |
| OFF | 44 (9.8) | 38 (9.9) | 90 (9.5) | 86 (9.8) | 15 (2.5) | 15 (2.0) | 32 (5.3) | 34 (4.2) | 48(4.1) | 46 (4.2) | |
| MG | ON | 22.5 (12.5) | 12 (11.6) | 56(12.6) | 56 (12.7) | 4 (3.1) | 3 (2.2) | 13 (5.3) | 9 (5.8) | 35(6.0) | 34 (5.6) |
| OFF | 37 (11.7) | 32 (10.8) | 80 (9.9) | 77 (9.8) | 17 (2.4) | 16 (1.7) | 30 (5.3) | 30 (5.0) | 49(4.3) | 48 (3.7) | |
| Phase | Parameter | BF | RF | SE | LG | MG | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Right | Left | Right | Left | Right | Left | Right | Left | Right | Left | ||
| Stance (%) | Duration (%) | 15 (5.0) | 16 (5.7) | 14 (5.3) | 13 (4.5) | 16 (5.9) | 16.50 (6.4) | 15 (4.6) | 14 (4.7) | 14 (4.6) | 16 (4.4) |
| IQR 25% | 11 | 12 | 11 | 11 | 12 | 13 | 11 | 11 | 12.50 | 10 | |
| IQR 75% | 19 | 22 | 20 | 19 | 22 | 23 | 18 | 19 | 20 | 19 | |
| Wilcoxon | 0.048 | 0.184 | 0.352 | 0.944 | 0.001 | ||||||
| SI (%) | −6.45 | 14.29 | −3.08 | 6.89 | −13.33 | ||||||
| Swing (%) | Duration (%) | 15 (5.2) | 16 (5.9) | 15 (5.4) | 14.50 (6.1) | 16 (6.0) | 16 (6.0) | 14 (4.7) | 16 (5.5) | 17 (6.9) | 18 (6.7) |
| IQR 25% | 12 | 12 | 11 | 11 | 12 | 11 | 12 | 12 | 12 | 13 | |
| IQR 75% | 19.25 | 22 | 19.75 | 20 | 22 | 21.25 | 19 | 21.75 | 24.25 | 25 | |
| Wilcoxon | 0.105 | 0.771 | 0.269 | 0.026 | 0.343 | ||||||
| SI (%) | −6.45 | 3.39 | 0 | −13.33 | −5.71 | ||||||
| Double support (%) | Duration (%) | 12 (3.2) | 11 (2.0) | 10 (2.5) | 12 (2.6) | 12(1.9) | 11(1.8) | 10 (2.5) | 10 (1.6) | 12 (2.6) | 13 (1.8) |
| IQR 25% | 7 | 9 | 9 | 10 | 11 | 10 | 8 | 10 | 10 | 12 | |
| IQR 75% | 14 | 13 | 14 | 14 | 14 | 12.50 | 13 | 12 | 13.75 | 15 | |
| Wilcoxon | 0.845 | 0.237 | 0.064 | 0.555 | 0.107 | ||||||
| SI, | 8.70 | −18.18 | 8.70 | 0 | −8.00 | ||||||
| Single support (%) | Duration, % | 13 (4.2) | 15 (4.5) | 15 (4.6) | 14 (3.1) | 14.50 (4.2) | 16.50 (3.8) | 14 (4.0) | 16 (4.6) | 15 (4.7) | 19 (4.3) |
| IQR 25% | 11 | 12 | 10.25 | 10 | 12 | 14 | 11 | 12 | 11 | 15 | |
| IQR 75% | 17 | 20 | 19 | 16 | 19 | 20 | 17.25 | 20 | 20 | 23 | |
| Wilcoxon | 0.021 | 0.425 | 0.037 | 0.056 | 0.0003 | ||||||
| SI | −14.29 | 6.90 | −12.90 | −13.33 | −23.53 | ||||||
| Pre-Swing (%) | Duration, % | 16 (5.4) | 19 (6.4) | 17 (5.4) | 13.50 (5.3) | 19 (6.98) | 21 (7.9) | 16 (4.8) | 14 (5.0) | 15 (4.9) | 14.50 (4.3) |
| IQR 25% | 12 | 14 | 12 | 11 | 14 | 15 | 12 | 12 | 10.75 | 11 | |
| IQR 75% | 21.50 | 25 | 21 | 20 | 27.50 | 31 | 19 | 21.25 | 19 | 19 | |
| Wilcoxon | 0.031 | 0.157 | 0.176 | 0.813 | 0.626 | ||||||
| SI | −17.14 | 22.95 | −10.00 | 13.33 | 3.39 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daunoraviciene, K.; Ziziene, J.; Pauk, J.; Juskeniene, G.; Raistenskis, J. EMG Based Analysis of Gait Symmetry in Healthy Children. Sensors 2021, 21, 5983. https://doi.org/10.3390/s21175983
Daunoraviciene K, Ziziene J, Pauk J, Juskeniene G, Raistenskis J. EMG Based Analysis of Gait Symmetry in Healthy Children. Sensors. 2021; 21(17):5983. https://doi.org/10.3390/s21175983
Chicago/Turabian StyleDaunoraviciene, Kristina, Jurgita Ziziene, Jolanta Pauk, Giedre Juskeniene, and Juozas Raistenskis. 2021. "EMG Based Analysis of Gait Symmetry in Healthy Children" Sensors 21, no. 17: 5983. https://doi.org/10.3390/s21175983
APA StyleDaunoraviciene, K., Ziziene, J., Pauk, J., Juskeniene, G., & Raistenskis, J. (2021). EMG Based Analysis of Gait Symmetry in Healthy Children. Sensors, 21(17), 5983. https://doi.org/10.3390/s21175983