
Indirect Estimation of Breathing Rate from Heart Rate Monitoring System during Running

 ,
,  , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Set
2.2. Framework of the Breathing Rate Estimation from RR Intervals and Validation
2.3. Pre-Processing Methods
2.3.1. Band-Pass Filtering (BPF)
2.3.2. Relative RR Intervals (rRR)
2.4. Breathing Rate Estimation
2.4.1. Short-Term Fourier Transform (STFT)
2.4.2. Single Frequency Tracking (SFT)
2.4.3. Harmonic Frequency Tracking (HFT)
2.4.4. Peak Detection (Peak)
2.5. Validation Procedure
3. Results
3.1. Estimation of the BR from RR Intervals
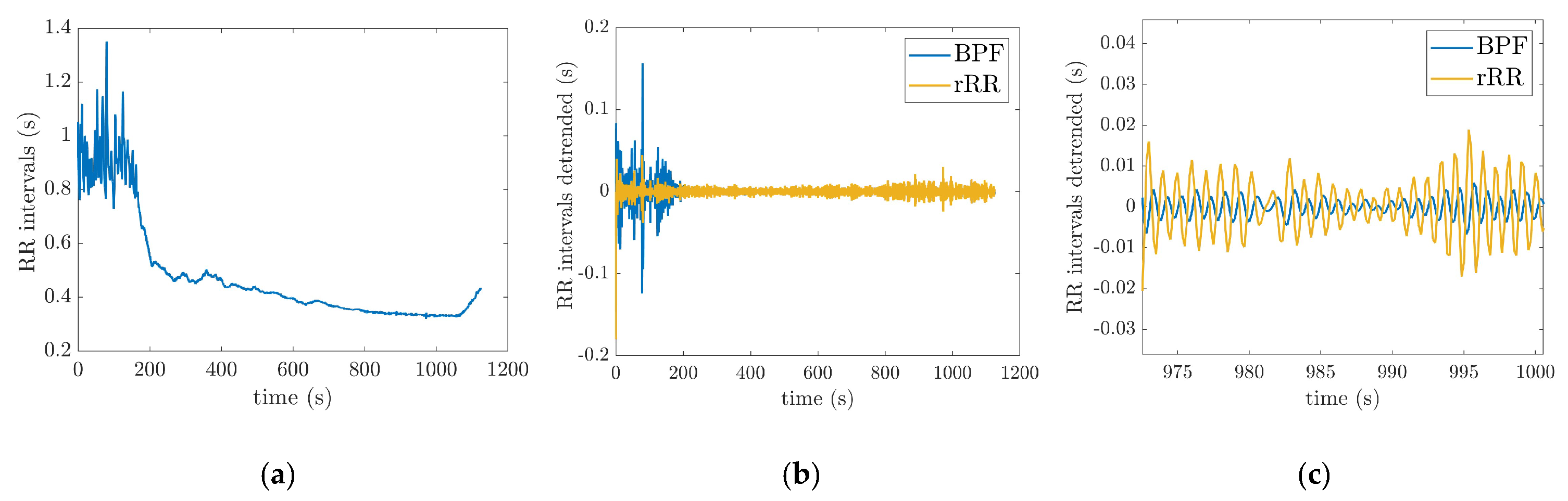
3.1.1. Pre-Processing
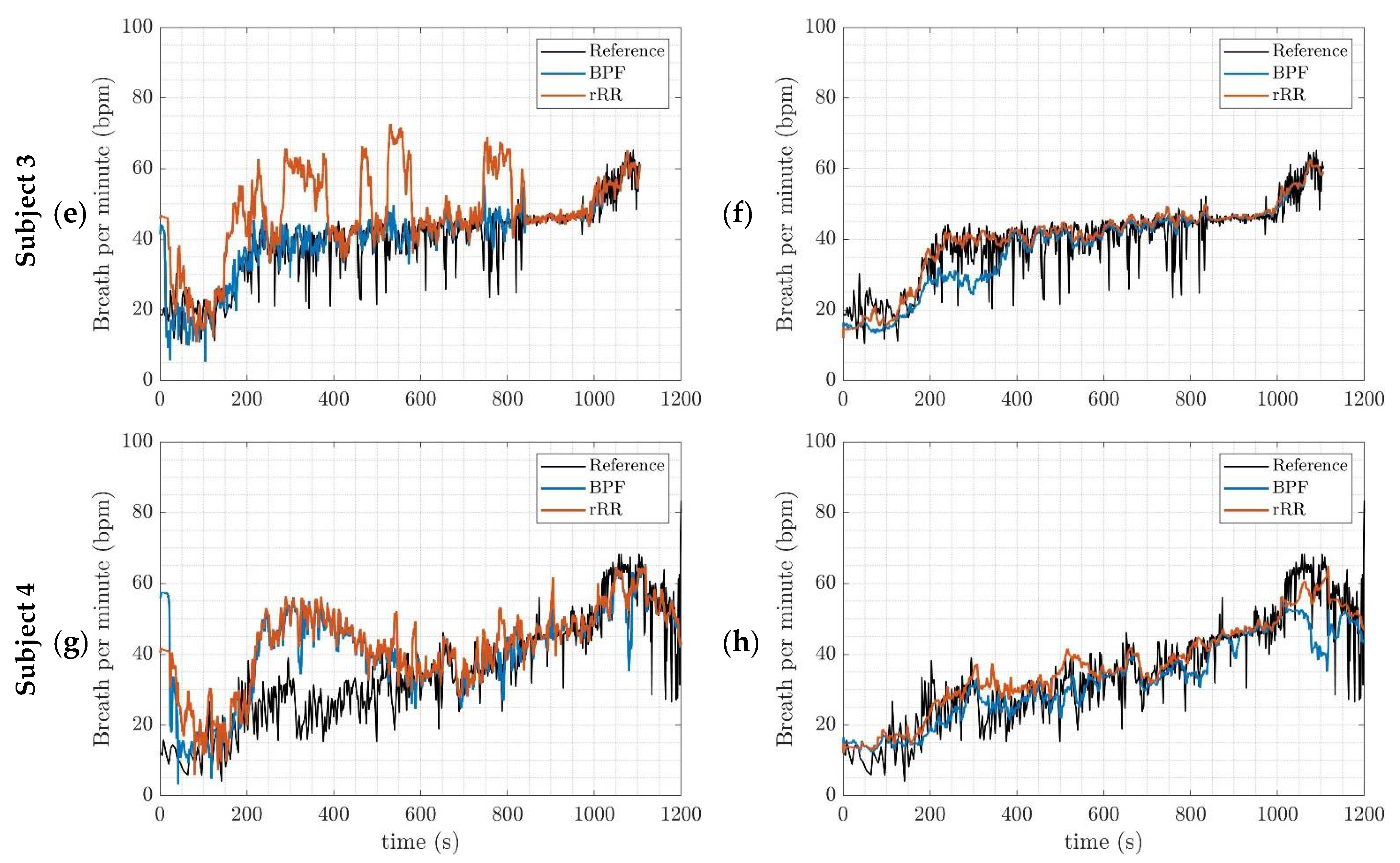
3.1.2. BR Estimation Algorithms
3.2. Validation
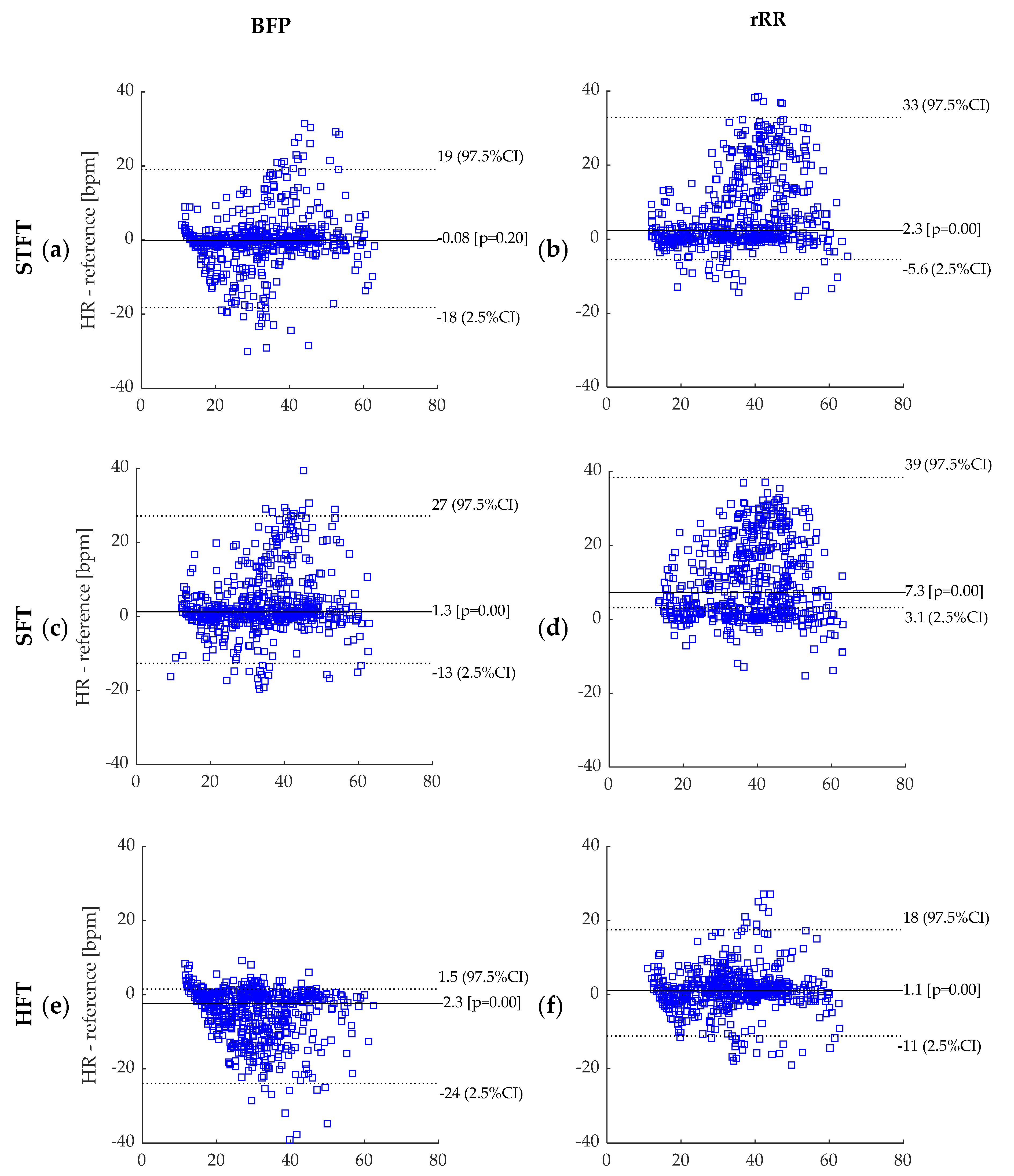
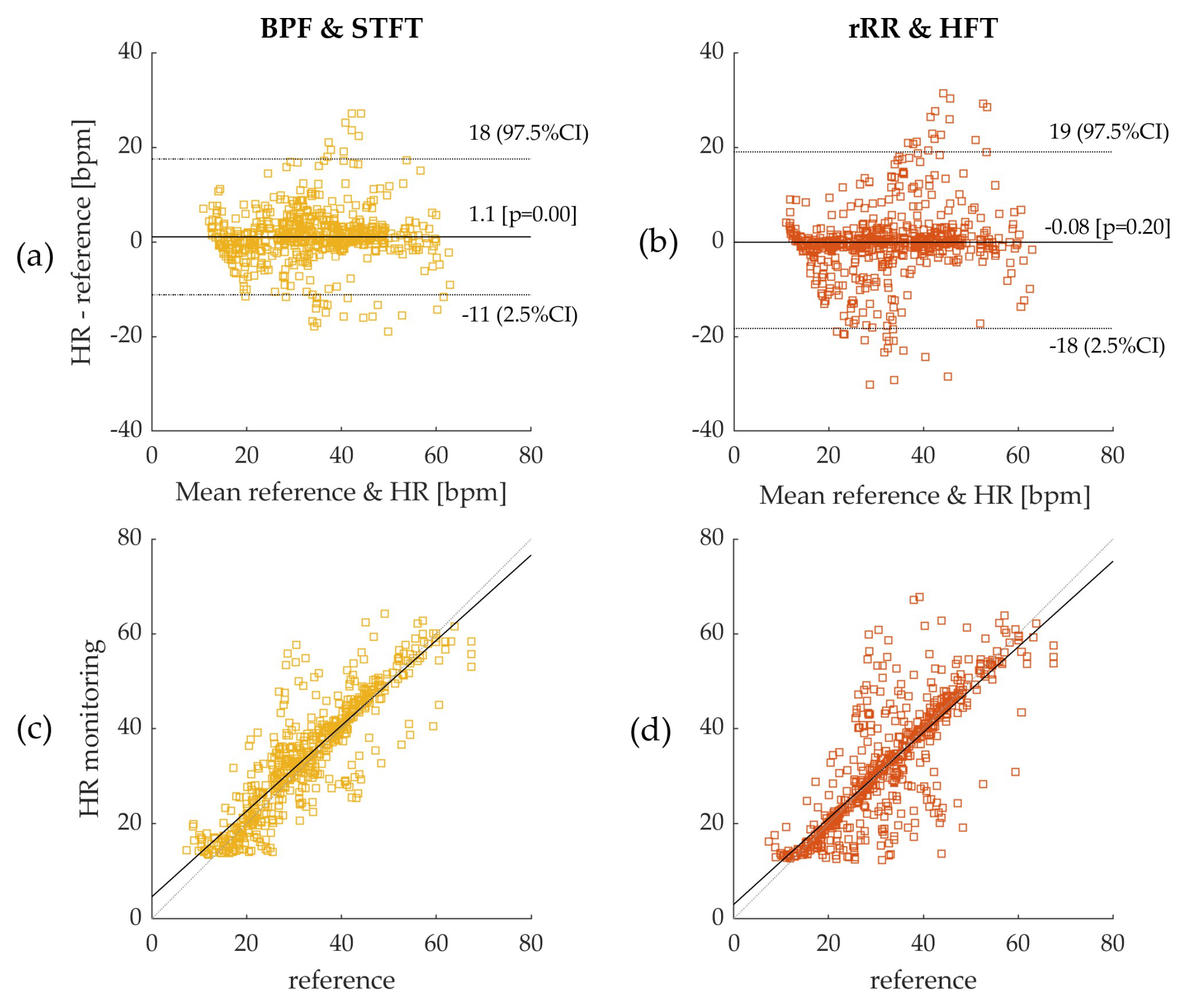
3.2.1. BR Estimation Algorithms and Bland–Altman Plot
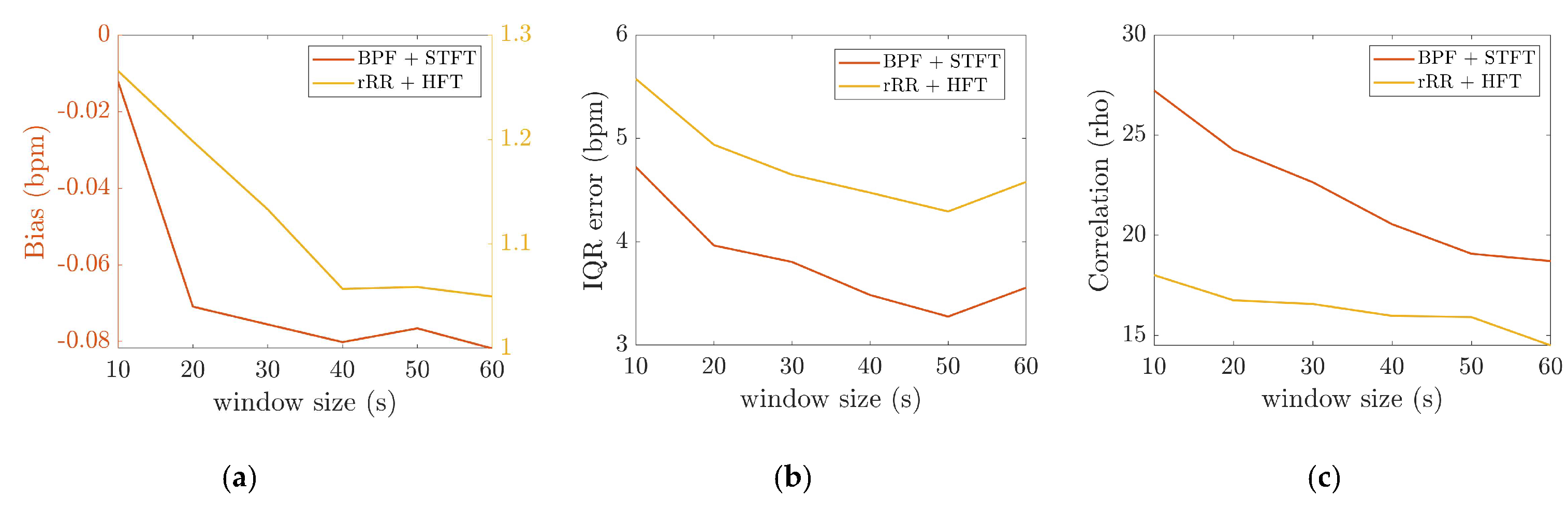
3.2.2. The Effect of Time-Window Duration
3.2.3. Inter Subject Variability
4. Discussion
4.1. Validation of the BR Estimation Algorithms
4.2. Physiological Implications
4.3. Perspective—Applications and Near-Real-Time Computation
4.4. Other Algorithms
4.5. Limitations
4.6. Future Work
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
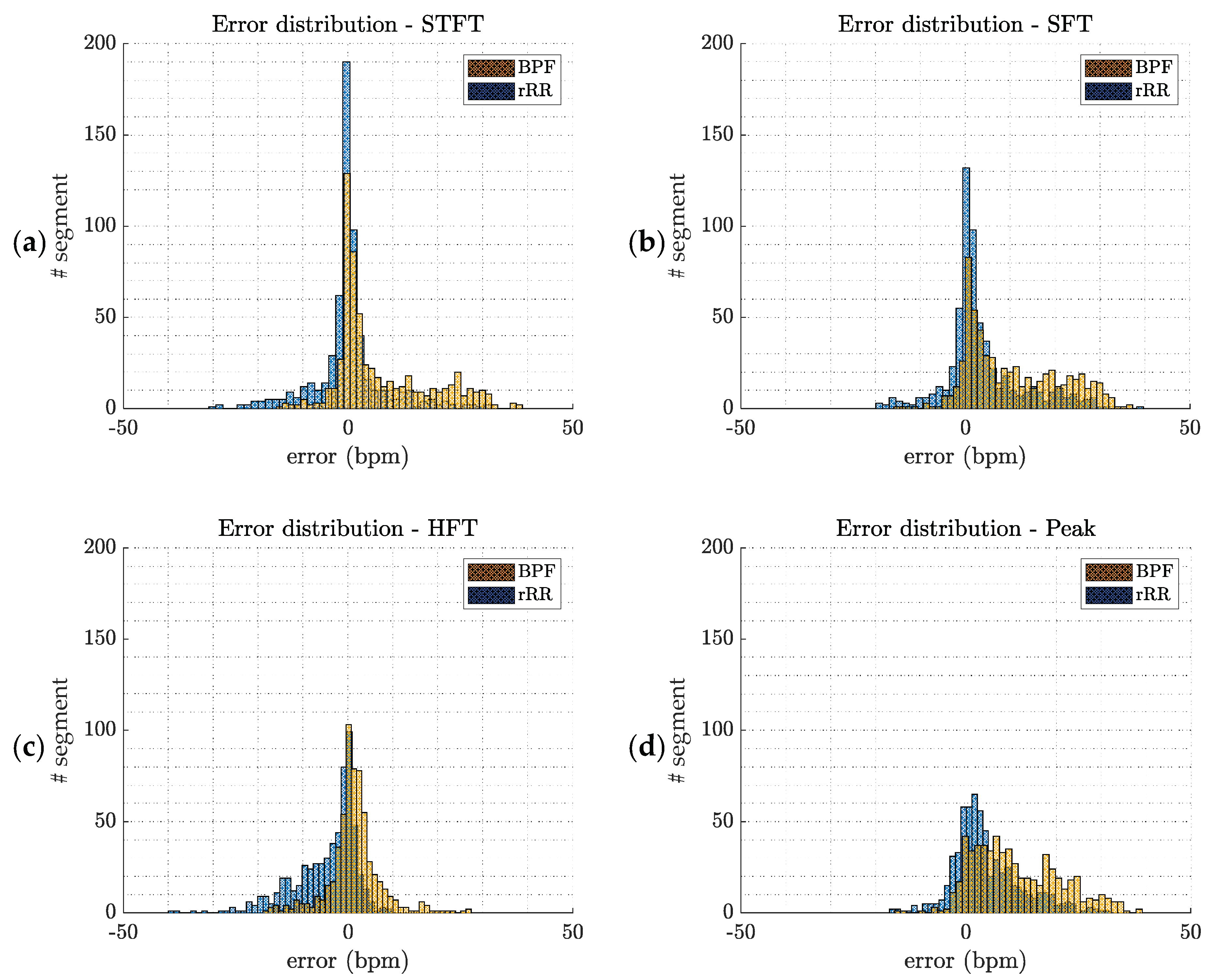
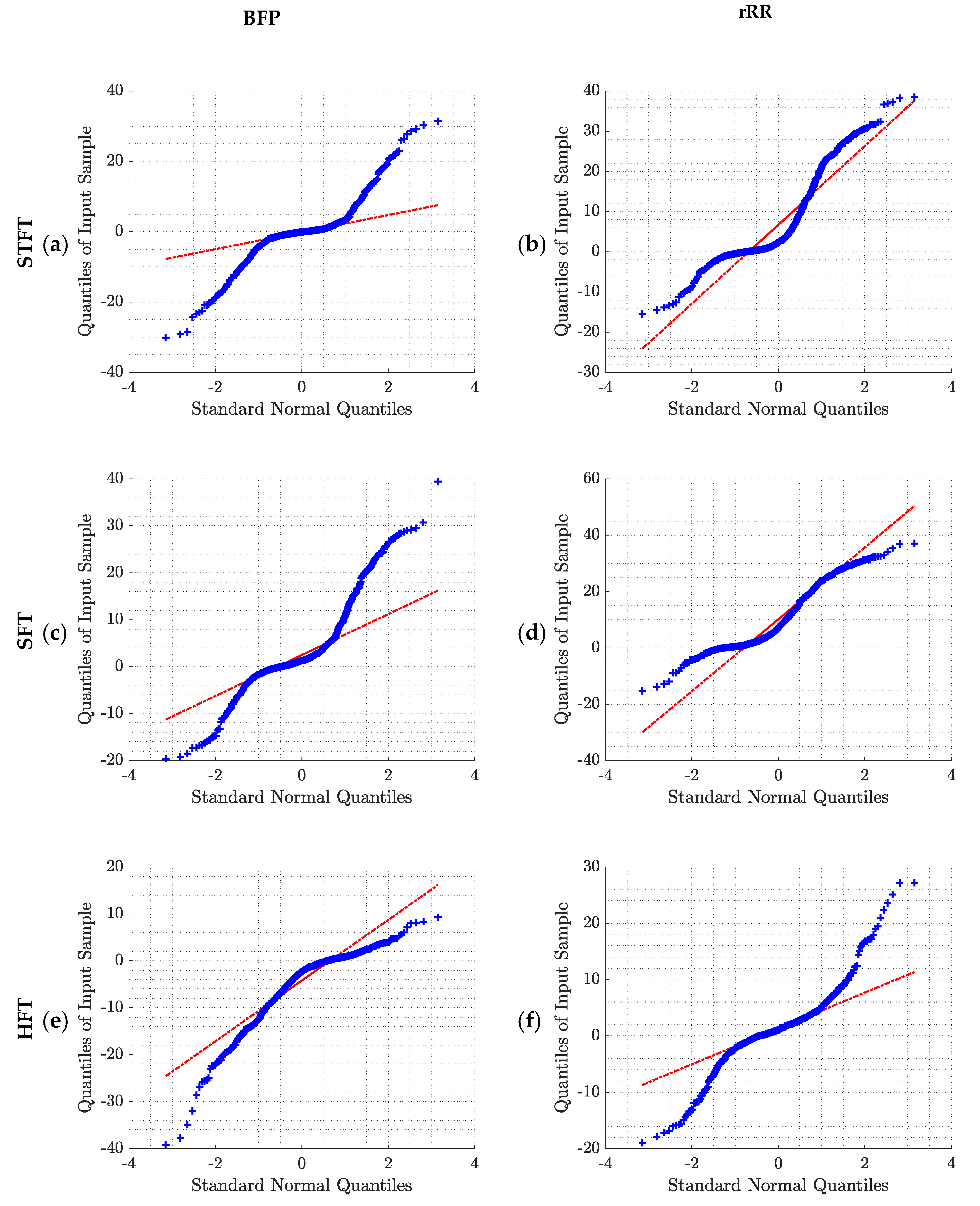
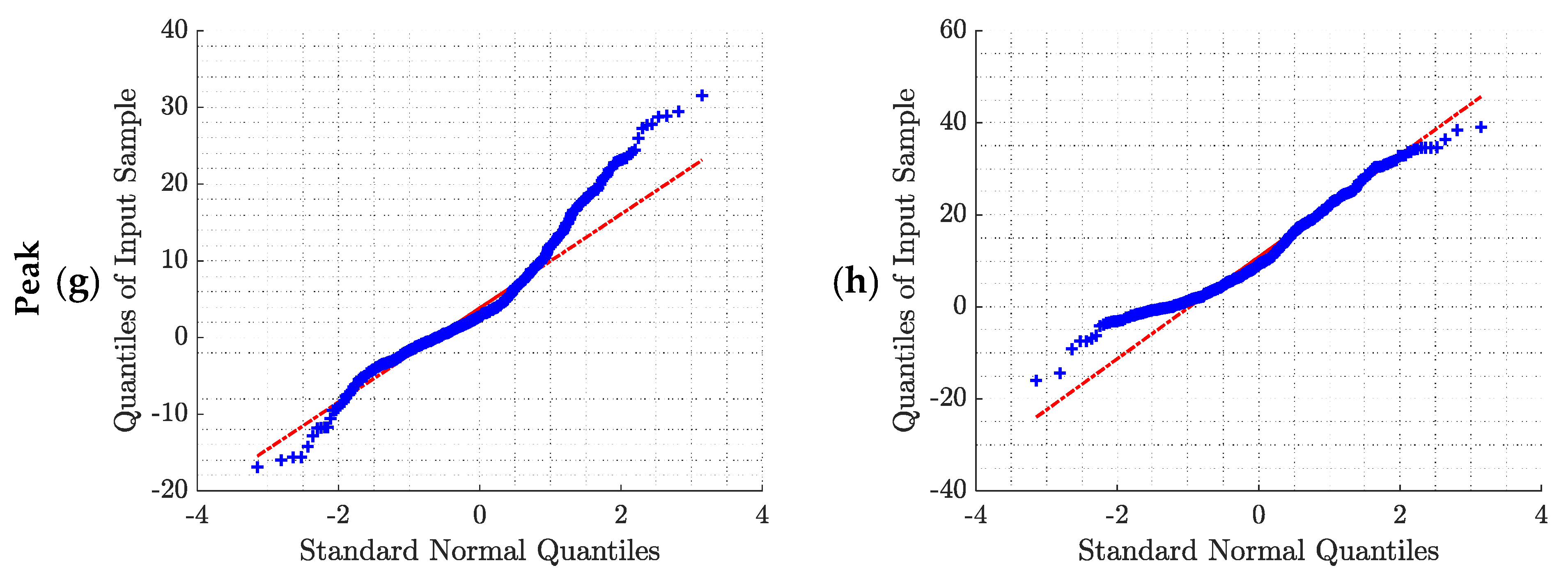
Appendix A. Error Distributions and Normality Tests
Appendix B. Statistical Analysis

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| STFT | SFT | HFT | Peak | |||
|---|---|---|---|---|---|---|
| 10 s | BPF | Bias (IQR) (bpm) | −0.01 (4.72) | 1.36(8.64) | −2.63 (9.21) | 2.31 (10.30) |
| CI (bpm), 2.5 | −21.17 | −15.28 | −22.98 | −14.08 | ||
| CI (bpm), 97.5 | 24.69 | 28.99 | 5.85 | 27.03 | ||
| ϵ%(w) (%) | 8.06 | 11.21 | 13.20 | 13.94 | ||
| ρ | 0.74 * | 0.71 * | 0.79 * | 0.72 * | ||
| rRR | Bias (IQR) (bpm) | 1.81 (14.14) | 7.41(18.78) | 1.26 (5.57) | 8.80 (16.64) | |
| CI (bpm), 2.5 | −10.75 | −6.01 | −14.21 | −5.87 | ||
| CI (bpm), 97.5 | 32.48 | 32.98 | 16.47 | 33.04 | ||
| ϵ%(w) (%) | 13.09 | 24.47 | 9.97 | 27.41 | ||
| ρ | 0.65 * | 0.57 * | 0.86 * | 0.62 * | ||
| 20 s | BPF | Bias (IQR) (bpm) | −0.07 (3.96) | 1.10 (7.96) | −2.45 (9.01) | 2.59 (9.14) |
| CI (bpm), 2.5 | −19.72 | −14.24 | −22.92 | −11.37 | ||
| CI (bpm), 97.5 | 23.01 | 27.52 | 5.09 | 24.57 | ||
| ϵ%(w) (%) | 6.52 | 9.83 | 11.97 | 12.93 | ||
| ρ | 0.77 * | 0.71 * | 0.80 * | 0.76 * | ||
| rRR | Bias (IQR) (bpm) | 2.08 (13.54) | 7.07 (18.51) | 1.20 (4.94) | 8.88 (15.67) | |
| CI (bpm), 2.5 | −9.34 | −4.71 | −13.43 | −4.52 | ||
| CI (bpm), 97.5 | 31.71 | 32.13 | 16.27 | 32.58 | ||
| ϵ%(w) (%) | 12.04 | 22.36 | 8.92 | 27.88 | ||
| ρ | 0.65 * | 0.58 * | 0.87 * | 0.64 * | ||
| 30 s | BPF | Bias (IQR) (bpm) | −0.08 (3.80) | 1.09 (7.68) | −2.51 (8.76) | 2.29 (8.53) |
| CI (bpm), 2.5 | −19.42 | −14.11 | −22.74 | −9.78 | ||
| CI (bpm), 97.5 | 21.90 | 28.14 | 4.89 | 23.34 | ||
| ϵ%(w) (%) | 6.56 | 9.35 | 12.02 | 11.69 | ||
| ρ | 0.79 * | 0.71 * | 0.80 * | 0.78 * | ||
| rRR | Bias (IQR) (bpm) | 2.00 (13.07) | 7.57 (18.63) | 1.13 (4.65) | 9.01 (15.44) | |
| CI (bpm), 2.5 | −9.33 | −4.67 | −13.06 | −3.77 | ||
| CI (bpm), 97.5 | 31.10 | 31.73 | 16.36 | 32.47 | ||
| MdAPE (%) | 11.41 | 23.22 | 8.38 | 27.06 | ||
| ρ | 0.66 * | 0.57 * | 0.88 * | 0.65 * | ||
| 40 s | BPF | Bias (IQR) (bpm) | −0.08 (3.48) | 1.06 (7.04) | −2.34 (8.81) | 2.64 (8.43) |
| CI (bpm), 2.5 | −17.81 | −13.51 | −21.95 | −9.35 | ||
| CI (bpm), 97.5 | 19.65 | 26.03 | 4.61 | 21.66 | ||
| MdAPE (%) | 5.98 | 8.14 | 11.88 | 11.85 | ||
| ρ | 0.82 * | 0.74 * | 0.80 * | 0.79 * | ||
| rRR | Bias (IQR) (bpm) | 1.92 (12.82) | 7.09 (18.23) | 1.06 (4.47) | 8.88 (15.27) | |
| CI (bpm), 2.5 | −15.99 | −21.28 | −12.30 | −3.59 | ||
| CI (bpm), 97.5 | 21.51 | 28.22 | 15.92 | 32.24 | ||
| MdAPE (%) | 10.54 | 22.93 | 7.97 | 28.57 | ||
| ρ | 0.68 * | 0.60 * | 0.88 * | 0.65 * | ||
| BPF | Bias (IQR) (bpm) | −0.08 (3.28) | 1.31 (5.89) | −2.33 (8.73) | 2.85 (8.27) | |
| 50 s | CI (bpm), 2.5 | −18.2 | −13.91 | −21.63 | −8.66 | |
| CI (bpm), 97.5 | 19.1 | 25.85 | 3.87 | 23.03 | ||
| MdAPE (%) | 5.48 | 8.10 | 12.40 | 11.50 | ||
| ρ | 0.82 * | 0.77 * | 0.81 * | 0.80 * | ||
| rRR | Bias (IQR) (bpm) | 2.35 (13.22) | 7.30 (17.20) | 1.06 (4.29) | 9.18 (14.93) | |
| CI (bpm), 2.5 | −7.92 | −4.16 | −12.24 | −2.91 | ||
| CI (bpm), 97.5 | 30.51 | 31.22 | 16.46 | 32.14 | ||
| MdAPE (%) | 11.24 | 23.81 | 7.66 | 30.16 | ||
| ρ | 0.67 * | 0.61 * | 0.88 * | 0.66 * | ||
| 60 s | BPF | Bias (IQR) (bpm) | −0.08 (3.56) | 1.05 (6.08) | −2.36 (8.88) | 2.65 (8.01) |
| CI (bpm), 2.5 | −17.56 | −13.66 | −21.49 | −6.66 | ||
| CI (bpm), 97.5 | 19.79 | 25.68 | 3.97 | 21.76 | ||
| MdAPE (%) | 5.50 | 8.30 | 11.05 | 11.38 | ||
| ρ | 0.81 * | 0.77 * | 0.81 * | 0.81 * | ||
| rRR | Bias (IQR) (bpm) | 1.99 (13.04) | 6.92 (17.28) | 1.05 (4.58) | 9.47 (15.56) | |
| CI (bpm), 2.5 | −8.27 | −3.77 | −12.20 | −2.61 | ||
| CI (bpm), 97.5 | 30.00 | 30.56 | 16.16 | 31.83 | ||
| MdAPE (%) | 10.34 | 22.97 | 8.26 | 29.49 | ||
| ρ | 0.67 * | 0.61 * | 0.88 * | 0.66 * |
Appendix C. Bland–Altman Plots

Appendix D. BR Estimation Using SFT and HFT

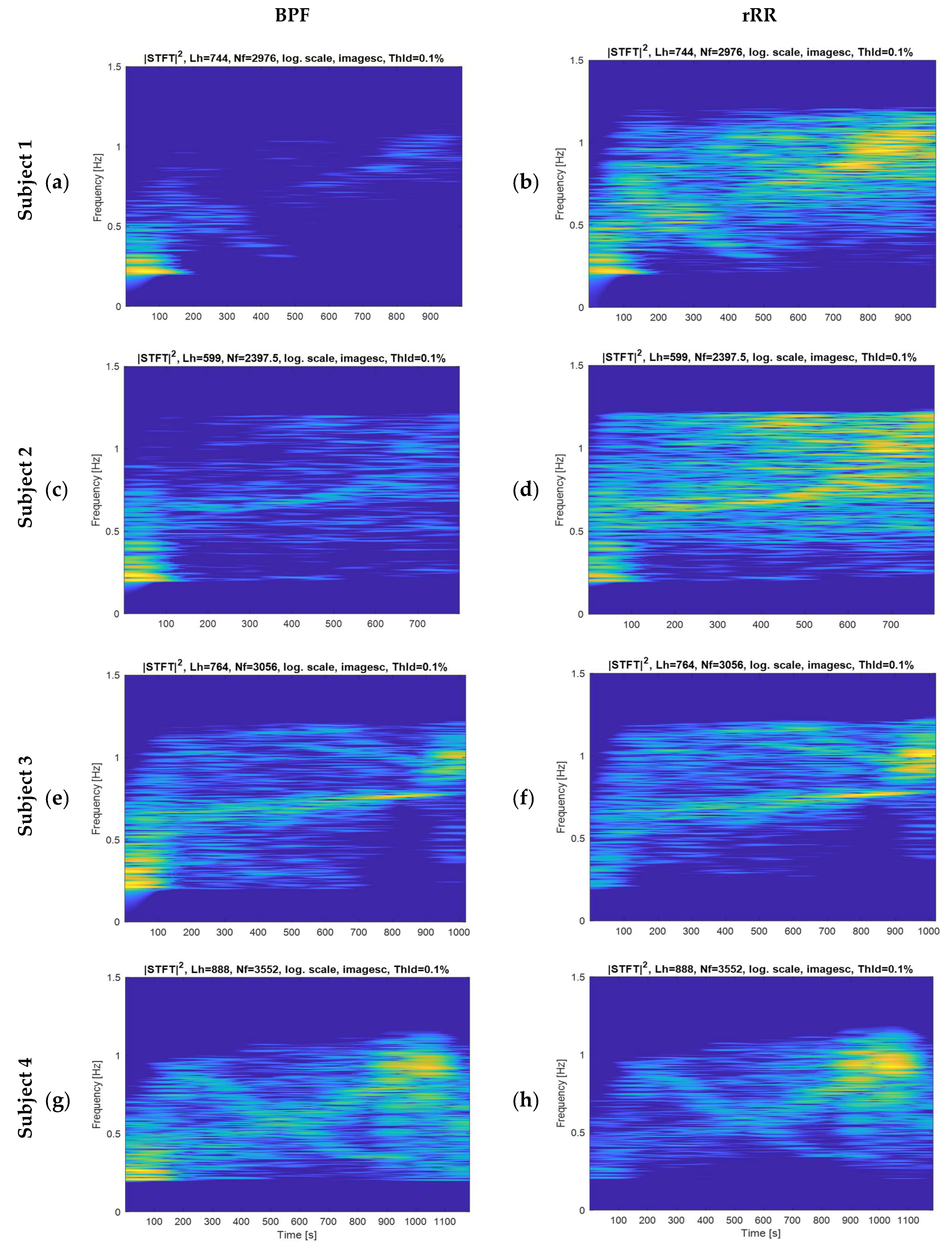
Appendix E. Spectrograms of the Filtered RR-Interval
References
- Duking, P.; Hotho, A.; Holmberg, H.-C.; Fuss, F.K.; Sperlich, B. Comparison of Non-Invasive Individual Monitoring of the Training and Health of Athletes with Commercially Available Wearable Technologies. Front. Physiol. 2016, 7, 71. [Google Scholar] [CrossRef]
- Vanegas, E.; Igual, R.; Plaza, I. Sensing systems for respiration monitoring: A technical systematic review. Sensors 2020, 20, 5446. [Google Scholar] [CrossRef] [PubMed]
- Aubert, A.E.; Seps, B.; Beckers, F. Heart Rate Variability in Athletes. Sport. Med. 2003, 33, 889–919. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, L.; Regnard, J.; Millet, G.P. Monitoring Fatigue Status with HRV Measures in Elite Athletes: An Avenue Beyond RMSSD? Front. Physiol. 2015, 6, 343. [Google Scholar] [CrossRef] [Green Version]
- Nicolò, A.; Massaroni, C.; Passfield, L. Respiratory frequency during exercise: The neglected physiological measure. Front. Physiol. 2017, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Braun, S.R. Respiratory Rate and Pattern-PubMed. In Clinical Methods: The History, Physical, and Laboratory Examinations, 3rd ed.; Walker, H.K., Hall, W.D., Hurst, J.W., Eds.; Butterworths: Boston, MA, USA, 1990. Available online: https://pubmed.ncbi.nlm.nih.gov/21250206/ (accessed on 19 March 2021).
- Schein, R.M.H.; Hazday, N.; Pena, M.; Ruben, B.H.; Sprung, C.L. Clinical antecedents to in-hospital cardiopulmonary arrest. Chest 1990, 98, 1388–1392. [Google Scholar] [CrossRef] [Green Version]
- Goldhill, D.R.; White, S.A.; Sumner, A. Physiological values and procedures in the 24 h before ICU admission from the ward. Anaesthesia 1999, 54, 529–534. [Google Scholar] [CrossRef]
- Ridley, S. The recognition and early management of critical illness. Ann. R. Coll. Surg. Engl. 2005, 87, 315–322. [Google Scholar] [CrossRef]
- Cretikos, M.A.; Bellomo, R.; Hillman, K.; Chen, J.; Finfer, S.; Flabouris, A. Respiratory rate: The neglected vital sign. Med. J. Aust. 2008, 188, 657–659. [Google Scholar] [CrossRef]
- Marcora, S.M.; Bosio, A.; De Morree, H.M. Locomotor muscle fatigue increases cardiorespiratory responses and reduces performance during intense cycling exercise independently from metabolic stress. Am. J. Physiol.-Regul. Integr. Comp. Physiol. 2008, 294, R874–R883. [Google Scholar] [CrossRef] [PubMed]
- Busse, M.W.; Maassen, N.; Konrad, H. Relation between plasma K+ and ventilation during incremental exercise after glycogen depletion and repletion in man. J. Physiol. 1991, 443, 469–476. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Massaroni, C.; Nicolò, A.; Presti, D.L.; Sacchetti, M.; Silvestri, S.; Schena, E. Contact-based methods for measuring respiratory rate. Sensors (Switzerland) 2019, 19, 908. [Google Scholar] [CrossRef] [Green Version]
- Witt, J.D.; Fisher, J.R.K.O.; Guenette, J.A.; Cheong, K.A.; Wilson, B.J.; Sheel, A.W. Measurement of exercise ventilation by a portable respiratory inductive plethysmograph. Respir. Physiol. Neurobiol. 2006, 154, 389–395. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Roberge, R.; Powell, J.B.; Shafer, A.B.; Jon Williams, W. Measurement accuracy of heart rate and respiratory rate during graded exercise and sustained exercise in the heat using the zephyr BioHarness TM. Int. J. Sports Med. 2013, 34, 497–501. [Google Scholar] [CrossRef] [Green Version]
- Liu, Y.; Zhu, S.H.; Wang, G.H.; Ye, F.; Li, P.Z. Validity and reliability of multiparameter physiological measurements recorded by the equivital lifemonitor during activities of various intensities. J. Occup. Environ. Hyg. 2013, 10, 78–85. [Google Scholar] [CrossRef]
- Bailón, R.; Sörnmo, L.; Laguna, P. ECG-Derived Respiratory Frequency Estimation. In Advanced Methods & Tools for ECG data Analysis; Clifford, G.D., Azuaje, F., Mc Sharry, P., Eds.; Artech: London, UK, 2007. [Google Scholar]
- Meredith, D.J.; Clifton, D.; Charlton, P.; Brooks, J.; Pugh, C.W.; Tarassenko, L. Photoplethysmographic derivation of respiratory rate: A review of relevant physiology. J. Med. Eng. Technol. 2012, 36, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hrushesky, W.J.M.; Fader, D.; Schmitt, O.; Gilbertsen, V. The respiratory sinus arrhythmia: A measure of cardiac age. Science 1984, 224, 1001–1004. [Google Scholar] [CrossRef] [PubMed]
- Blain, G.; Meste, O.; Bermon, S. Influences of breathing patterns on respiratory sinus arrhythmia in humans during exercise. Am. J. Physiol. Circ. Physiol. 2005, 288, H887–H895. [Google Scholar] [CrossRef]
- Anosov, O.; Patzak, A.; Kononovich, Y.; Persson, P.B. High-frequency oscillations of the heart rate during ramp load reflect the human anaerobic threshold. Eur. J. Appl. Physiol. 2000, 83, 388–394. [Google Scholar] [CrossRef] [PubMed]
- Bernardi, L.; Salvucci, F.; Suardi, R.; Soldá, P.L.; Calciati, A.; Perlini, S.; Falcone, C.; Ricciardi, L. Evidence for an intrinsic mechanism regulating heart rate variability in the transplanted and the intact heart during submaximal dynamic exercise? Cardiovasc. Res. 1990, 24, 969–981. [Google Scholar] [CrossRef] [PubMed]
- Casadei, B.; Moon, J.; Johnston, J.; Caiazza, A.; Sleight, P. Is respiratory sinus arrhythmia a good index of cardiac vagal tone in exercise? J. Appl. Physiol. 1996, 81, 556–564. [Google Scholar] [CrossRef]
- Potamianos, A.; Maragos, P. A comparison of the energy operator and the Hilbert transform approach to signal and speech demodulation. Signal. Process. 1994, 37, 95–120. [Google Scholar] [CrossRef]
- Chavez, M.; Besserve, M.; Adam, C.; Martinerie, J. Towards a proper estimation of phase synchronization from time series. J. Neurosci. Methods 2006, 154, 149–160. [Google Scholar] [CrossRef]
- Aboy, M.; Márquez, O.W.; Mcnames, J.; Hornero, R.; Trong, T.; Goldstein, B. Adaptive Modeling and Spectral Estimation of Nonstationary Biomedical Signals Based on Kalman Filtering. IEEE Trans. Biomed. Eng. 2005, 52, 1485–1489. [Google Scholar] [CrossRef] [PubMed]
- Charlton, P.H.; Bonnici, T.; Tarassenko, L.; Clifton, D.A.; Beale, R.; Watkinson, P.J. An assessment of algorithms to estimate respiratory rate from the electrocardiogram and photoplethysmogram. Physiol. Meas. 2016, 37, 610–626. [Google Scholar] [CrossRef] [PubMed]
- Charlton, P.H.; Birrenkott, D.A.; Bonnici, T.; Pimentel, M.A.F.; Johnson, A.E.W.; Alastruey, J.; Tarassenko, L.; Watkinson, P.J.; Beale, R.; Clifton, D.A. Breathing Rate Estimation from the Electrocardiogram and Photoplethysmogram: A Review. IEEE Rev. Biomed. Eng. 2018, 11, 2–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buttu, A.; Pruvot, E.; Van Zaen, J.; Viso, A.; Forclaz, A.; Pascale, P.; Narayan, S.M.; Vesin, J.M. Adaptive frequency tracking of the baseline ECG identifies the site of atrial fibrillation termination by catheter ablation. Biomed. Signal. Process. Control. 2013, 8, 969–980. [Google Scholar] [CrossRef]
- Mirmohamadsadeghi, L.; Vesin, J.M. Real-time multi-signal frequency tracking with a bank of notch filters to estimate the respiratory rate from the ECG. Physiol. Meas. 2016, 37, 1573–1587. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Florian, J.P.; Chon, K.H. Respiratory rate extraction from pulse oximeter and electrocardiographic recordings. Physiol. Meas. 2011, 32, 1763–1773. [Google Scholar] [CrossRef] [Green Version]
- Mirmohamadsadeghi, L.; Vesin, J.M. Respiratory rate estimation from the ECG using an instantaneous frequency tracking algorithm. Biomed. Signal. Process. Control. 2014, 14, 66–72. [Google Scholar] [CrossRef]
- Vollmer, M. In Proceedings of the HRVTool-An Open-Source Matlab Toolbox for Analyzing Heart Rate Variability, Singapore, 8–11 September 2019.
- Fleming, S. Measurement and fusion of non-invasive vital signs for routine triage of acute paediatric illness. Ph.D Thesis, Oxford University, Oxford, UK, 2010. [Google Scholar]
- Lamarra, N.; Whipp, B.J.; Ward, S.A.; Wasserman, K. Effect of interbreath fluctuations on characterizing exercise gas exchange kinetics. J. Appl. Physiol. 1987, 62, 2003–2012. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. Measuring agreement in method comparison studies. Stat. Methods Med. Res. 1999, 8, 135–160. [Google Scholar] [CrossRef] [PubMed]
- Ialongo, C. Confidence interval for quantiles and percentiles. Biochem. Med. 2019, 29. [Google Scholar] [CrossRef] [PubMed]
- Kowalski, C.J. On the Effects of Non-Normality on the Distribution of the Sample Product-Moment Correlation Coefficient. Appl. Stat. 1972, 21, 1. [Google Scholar] [CrossRef]
- Fagraeus, L.; Linnarsson, D. Autonomic origin of heart rate fluctuations at the onset of muscular exercise. J. Appl. Physiol. 1976, 40, 679–682. [Google Scholar] [CrossRef] [PubMed]
- Robinson, B.F.; Epstein, S.E.; Beiser, G.D.; Braunwald, E. Control of heart rate by the autonomic nervous system. Studies in man on the interrelation between baroreceptor mechanisms and exercise. Circ. Res. 1966, 19, 400–411. [Google Scholar] [CrossRef] [Green Version]
- Kübler, W. Human cardiovascular control: Edited by Loring B. Rowell, Oxford University Press, New York (1993) 500 pages illustrated $65.00 ISBN: 9-19-507362-2. Clin. Cardiol. 1994, 17, 98. [Google Scholar] [CrossRef]
- Akselrod, S.; Gordon, D.; Ubel, F.A.; Shannon, D.C.; Barger, A.C.; Cohen, R.J. Power spectrum analysis of heart rate fluctuation: A quantitative probe of beat-to-beat cardiovascular control. Science 1981, 213, 220–222. [Google Scholar] [CrossRef]
- Nicolò, A.; Bazzucchi, I.; Haxhi, J.; Felici, F.; Sacchetti, M. Comparing Continuous and Intermittent Exercise: An “Isoeffort” and “Isotime” Approach. PLoS ONE 2014, 9, e94990. [Google Scholar] [CrossRef] [Green Version]
- Dorraki, M.; Fouladzadeh, A.; Allison, A.; Davis, B.R.; Abbott, D. On moment of velocity for signal analysis. R. Soc. Open Sci. 2019, 6, 182001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, S.; Kim, S.-Y. Respiratory Rate Estimation Based on Spectrum Decomposition. Biomed. Chem. Eng. 2018. [Google Scholar] [CrossRef] [Green Version]
- Sin, P.Y.W.; Galletly, D.C.; Tzeng, Y.C. Influence of breathing frequency on the pattern of respiratory sinus arrhythmia and blood pressure: Old questions revisited. Am. J. Physiol. Heart Circ. Physiol. 2010, 298, 1588–1599. [Google Scholar] [CrossRef] [PubMed]
- Gilgen-Ammann, R.; Schweizer, T.; Wyss, T. RR interval signal quality of a heart rate monitor and an ECG Holter at rest and during exercise. Eur. J. Appl. Physiol. 2019, 119, 1525–1532. [Google Scholar] [CrossRef] [PubMed]
- Birrenkott, D.A.; Pimentel, M.A.F.; Watkinson, P.J.; Clifton, D.A. Robust estimation of respiratory rate via ECG- and PPG-derived respiratory quality indices. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, New Orleans, LA, USA, 2016; Volume 2016, pp. 676–679. [Google Scholar]




| STFT | SFT | HFT | Peak | ||
|---|---|---|---|---|---|
| BPF | Bias (IQR) (bpm) | −0.08 (3.28) | 1.31 (5.89) | −2.33 (8.73) | 2.85 (8.27) |
| CI (bpm), 2.5 | −18.2 | −13.91 | −21.63 | −8.66 | |
| CI (bpm), 97.5 | 19.1 | 25.85 | 3.87 | 23.03 | |
| MdAPE (%) | 5.48 | 8.10 | 12.40 | 11.50 | |
| ρ | 0.82 * | 0.77 * | 0.81 * | 0.80 * | |
| rRR | Bias (IQR) (bpm) | 2.35 (13.22) | 7.30 (17.20) | 1.06 (4.29) | 9.18 (14.93) |
| CI (bpm), 2.5 | −7.92 | −4.16 | −12.24 | −2.91 | |
| CI (bpm), 97.5 | 30.51 | 31.22 | 16.46 | 32.14 | |
| MdAPE (%) | 11.24 | 23.81 | 7.66 | 30.16 | |
| ρ | 0.67 * | 0.61 * | 0.88 * | 0.66 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Prigent, G.; Aminian, K.; Rodrigues, T.; Vesin, J.-M.; Millet, G.P.; Falbriard, M.; Meyer, F.; Paraschiv-Ionescu, A. Indirect Estimation of Breathing Rate from Heart Rate Monitoring System during Running. Sensors 2021, 21, 5651. https://doi.org/10.3390/s21165651
Prigent G, Aminian K, Rodrigues T, Vesin J-M, Millet GP, Falbriard M, Meyer F, Paraschiv-Ionescu A. Indirect Estimation of Breathing Rate from Heart Rate Monitoring System during Running. Sensors. 2021; 21(16):5651. https://doi.org/10.3390/s21165651
Chicago/Turabian StylePrigent, Gaëlle, Kamiar Aminian, Tiago Rodrigues, Jean-Marc Vesin, Grégoire P. Millet, Mathieu Falbriard, Frédéric Meyer, and Anisoara Paraschiv-Ionescu. 2021. "Indirect Estimation of Breathing Rate from Heart Rate Monitoring System during Running" Sensors 21, no. 16: 5651. https://doi.org/10.3390/s21165651
APA StylePrigent, G., Aminian, K., Rodrigues, T., Vesin, J.-M., Millet, G. P., Falbriard, M., Meyer, F., & Paraschiv-Ionescu, A. (2021). Indirect Estimation of Breathing Rate from Heart Rate Monitoring System during Running. Sensors, 21(16), 5651. https://doi.org/10.3390/s21165651