
A Classification and Prediction Hybrid Model Construction with the IQPSO-SVM Algorithm for Atrial Fibrillation Arrhythmia

 , , and
, , and
Abstract
:1. Introduction
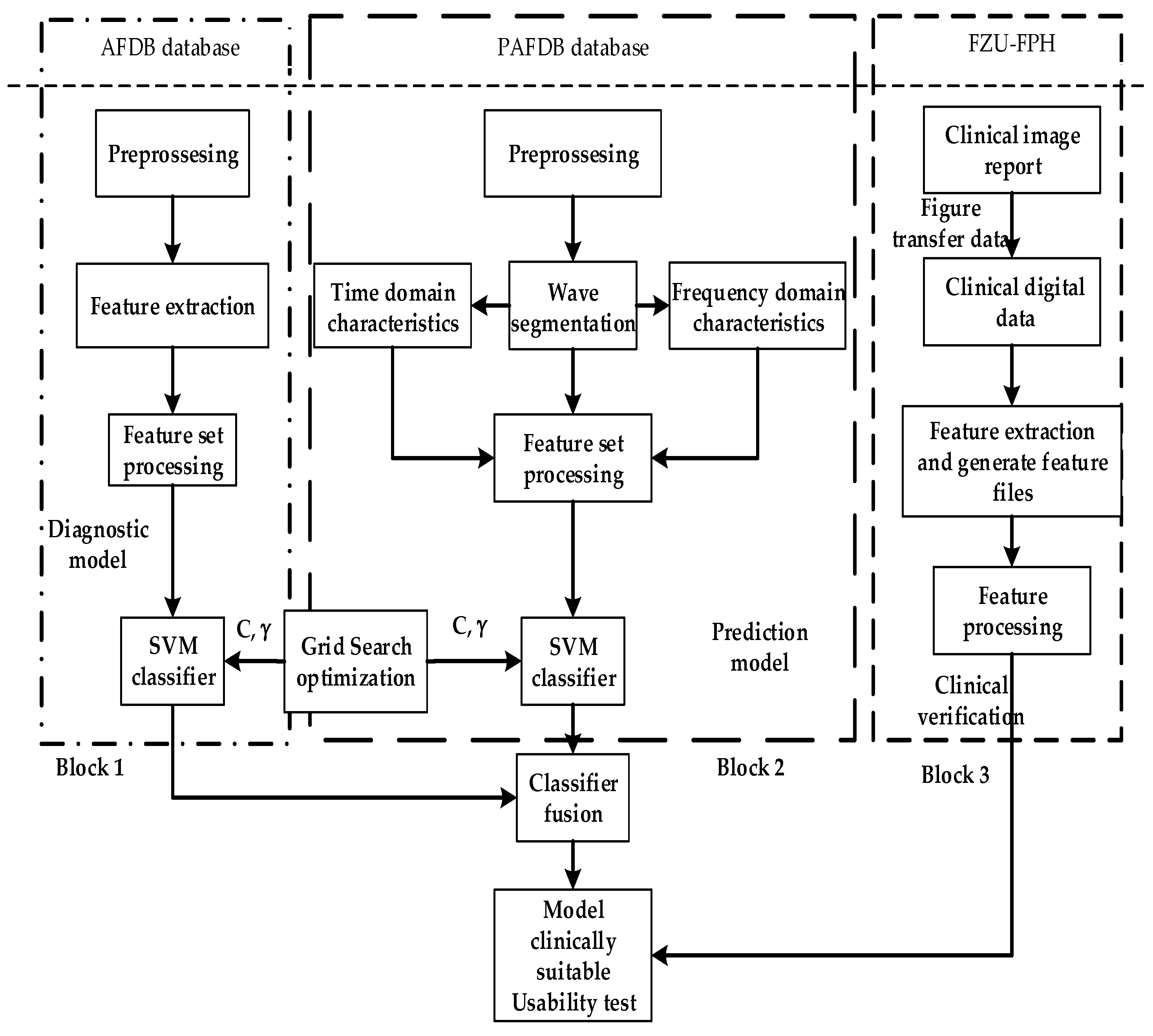
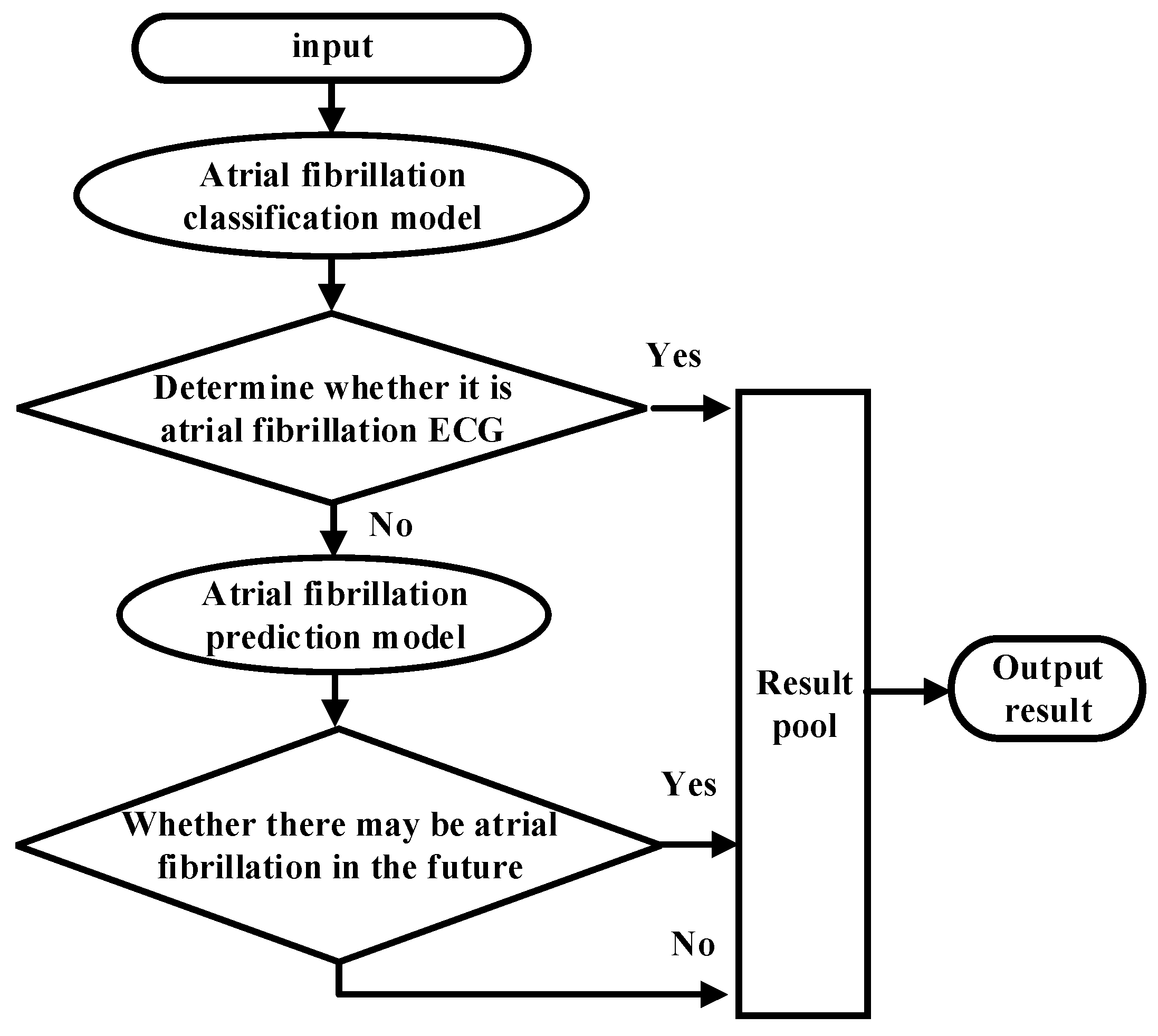
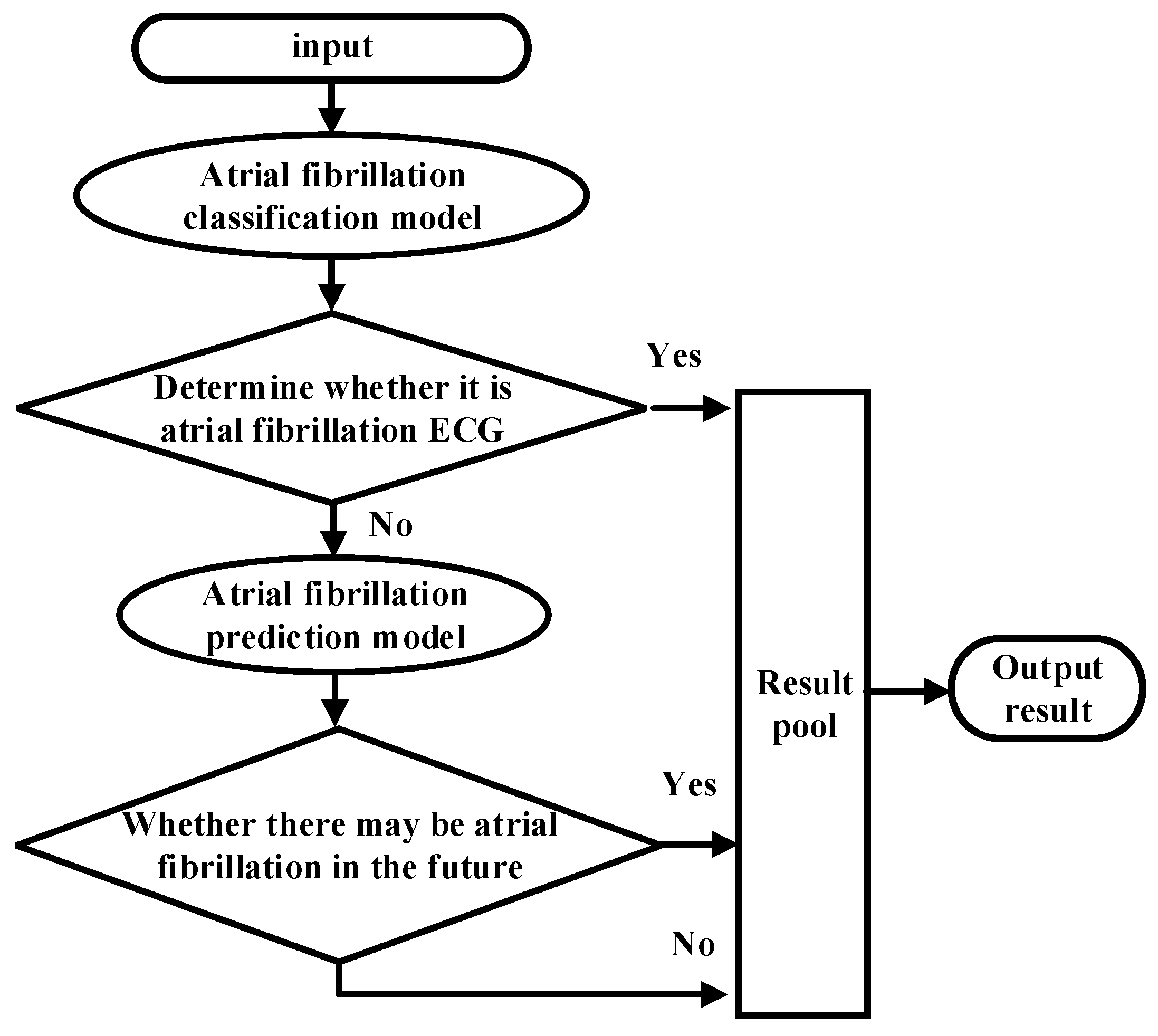
- The proposed classification and prediction hybrid model uses a new waterfall ensemble method. The first step executed the heartbeat classification, classifying normal and AF categories, and then PAF prediction was performed in which the hybrid model was more suitable for clinical applications, with improved accuracy, and realized an intelligent analysis of AF.
- Second, the research focused on classified features and introduced wavelet changes in the features of AF.
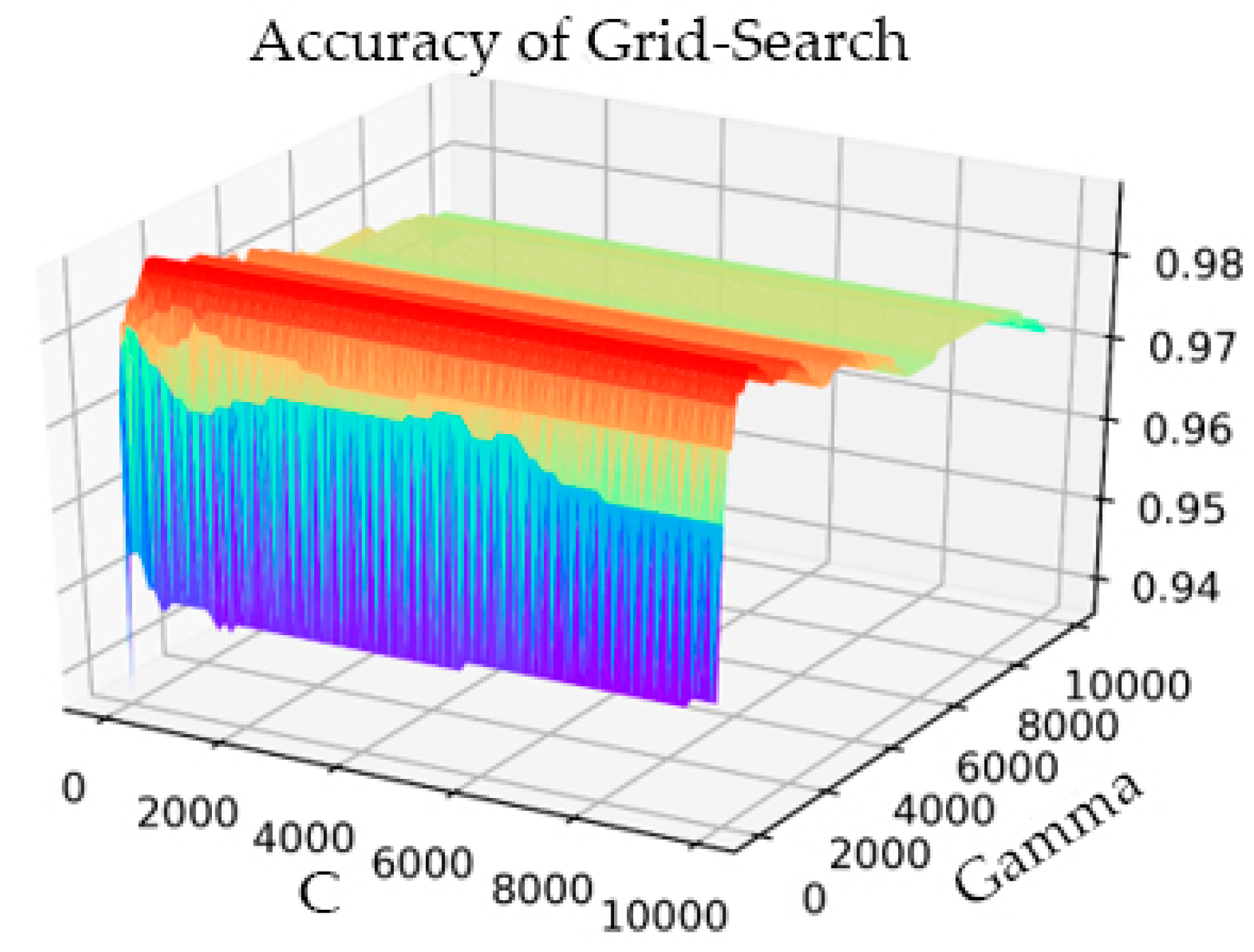
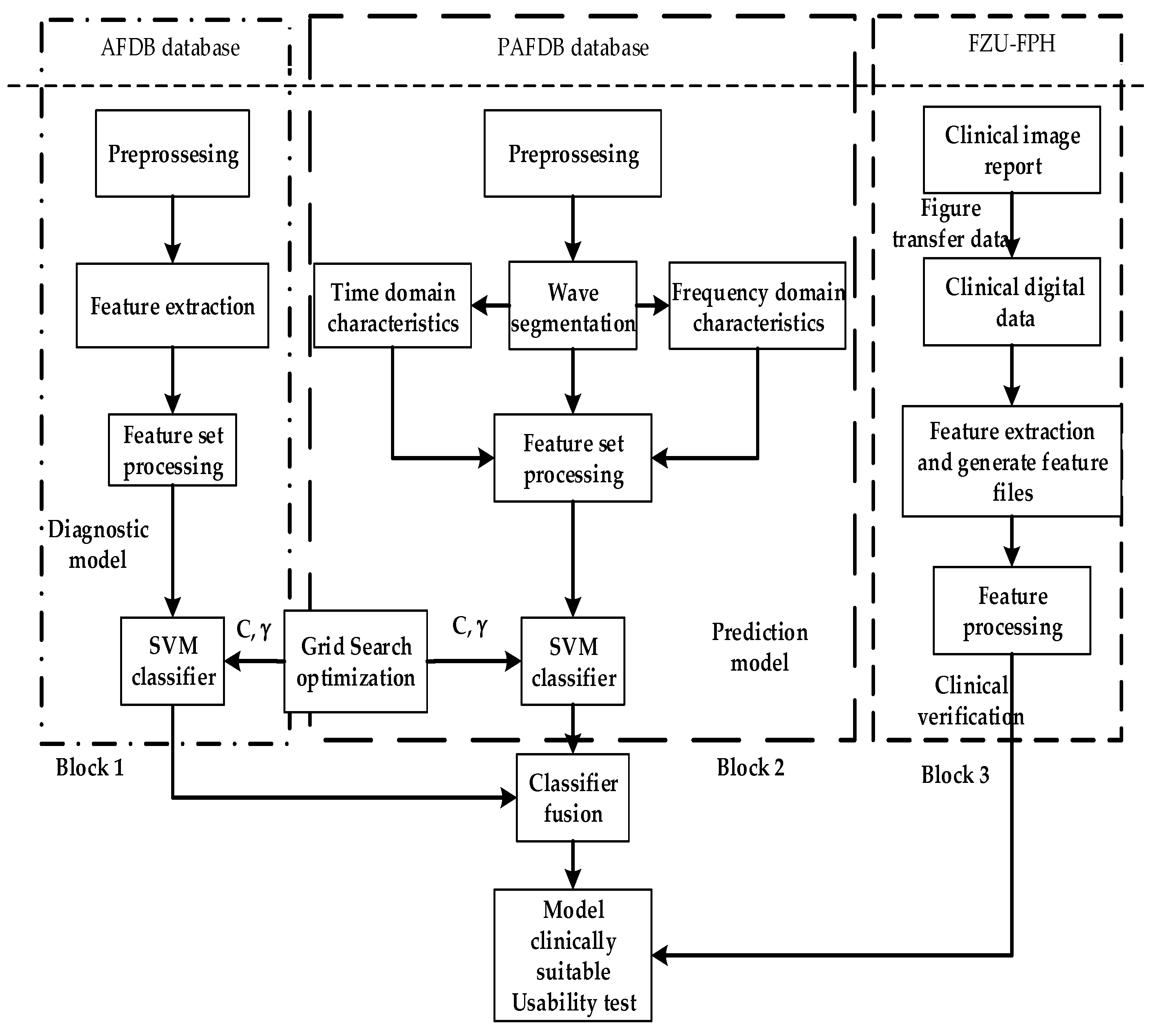
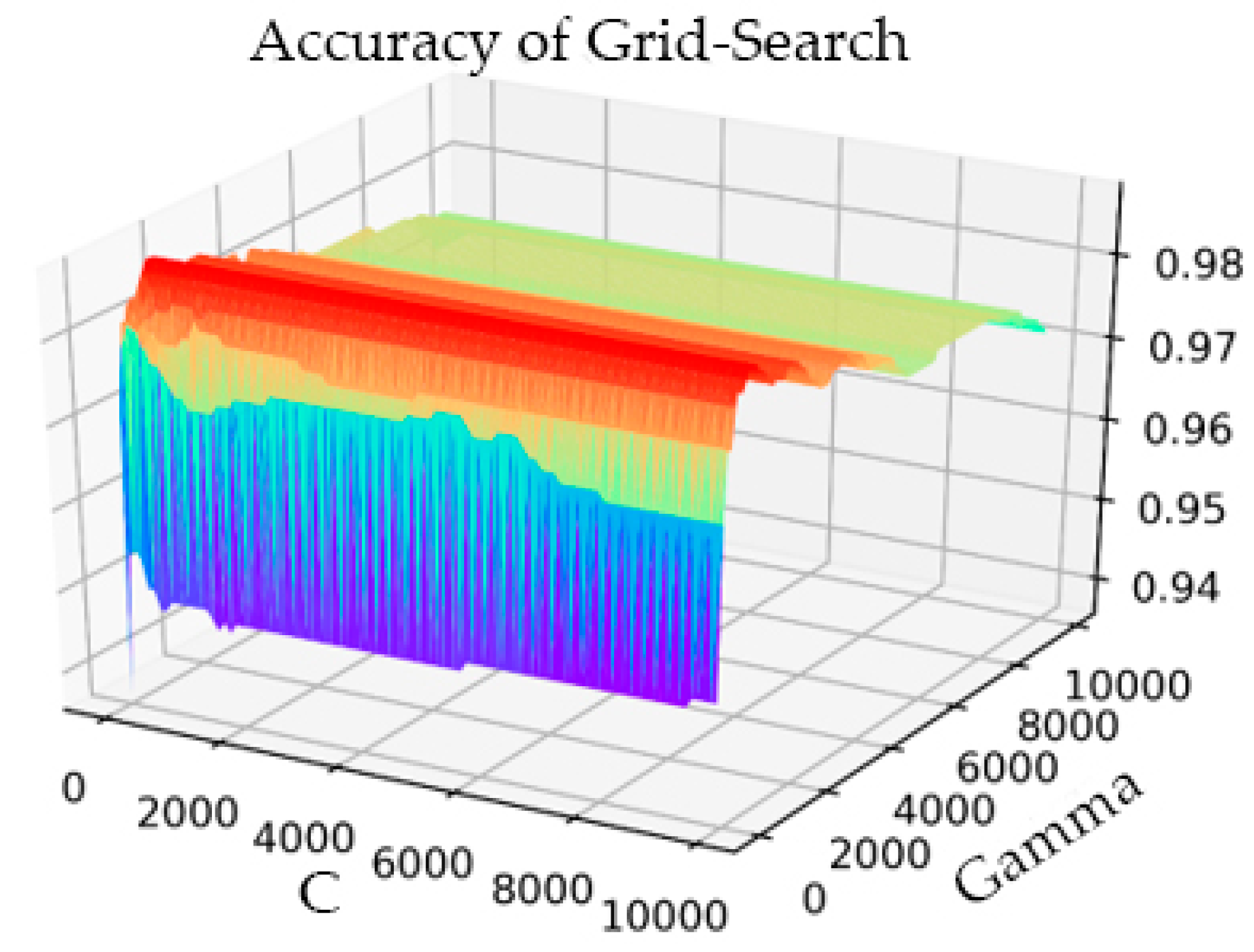
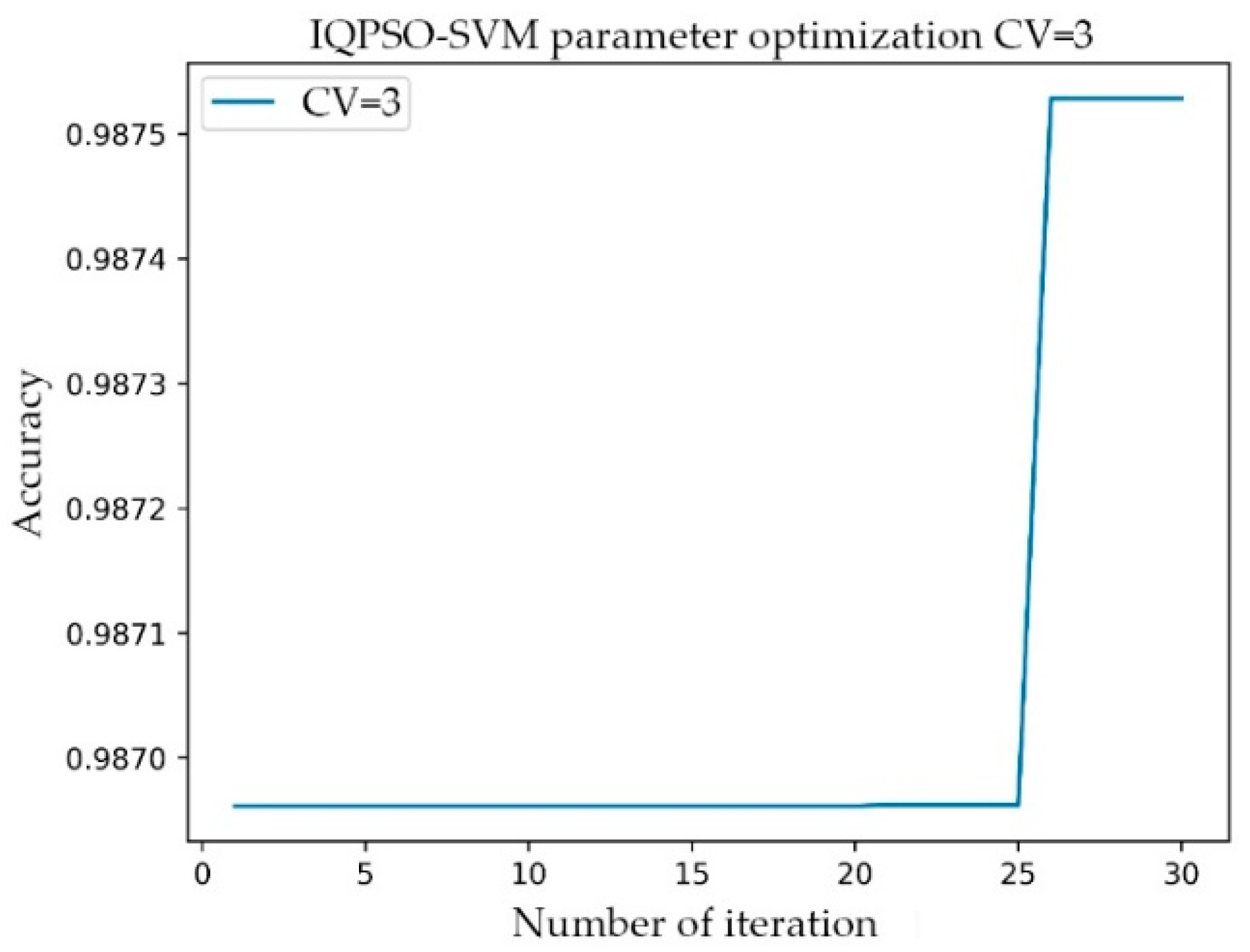
- Third, research was conducted on improved quantum particle swarm optimization SVM (IQPSO-SVM) training acceleration and used cross-validation to compare the improved acceleration algorithm with the traditional Grid-Search SVM optimization method.
- Lastly, the proposed algorithm was converted the clinical ECG to digital data, which were acquired from the Holter monitor in the hospital; Thus, the data of the AF database can be greatly increased. The model was validated on the FZU-FPH database, which further reflects the clinical generalization ability of the model.
2. Materials and Methods
3. Establishment of the Composite Model
3.1. Pre-Processing
3.2. Feature Extraction
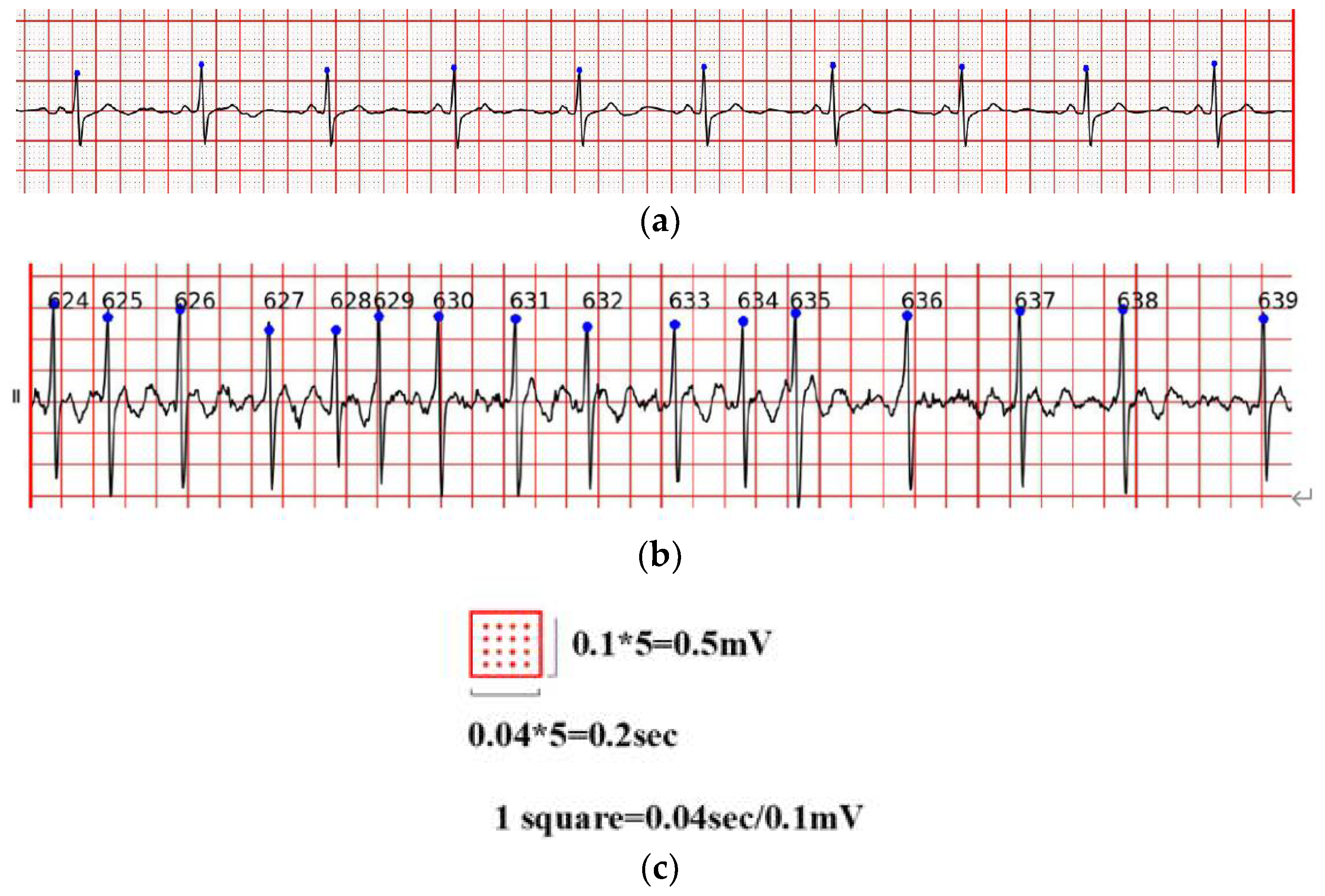
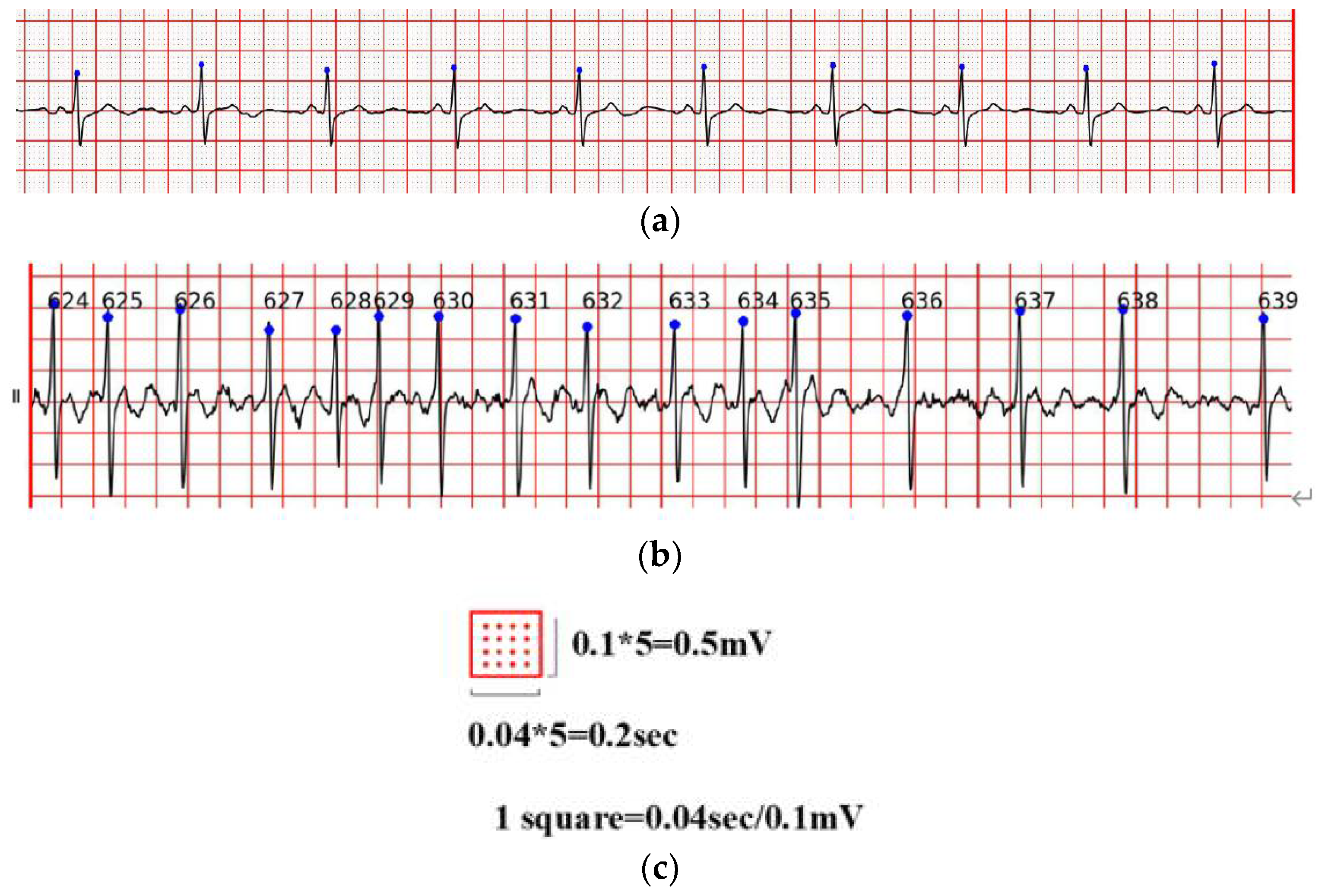
- The P wave disappeared and was replaced by AF waves with different shapes, spacing, and amplitudes. AF waves were generally obvious in leads V1 and II. The frequency was 350–600 times/min, and the amplitude was generally 0.05–0.50 mV.
- The QRS complex morphology is usually normal, but when a ventricular bundle branch block or other diseases occur, the QRS complex widens and the morphology appears abnormal.
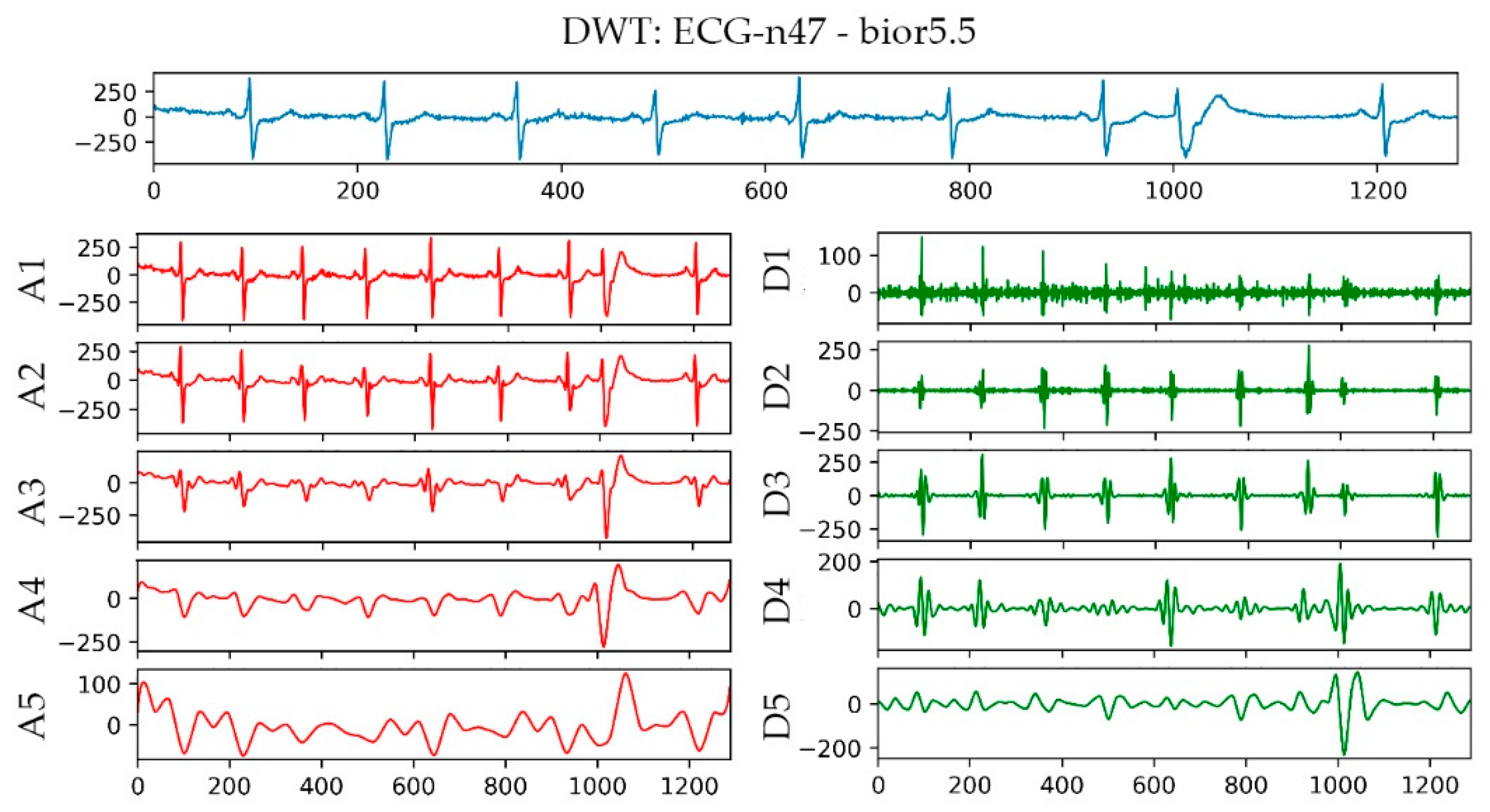
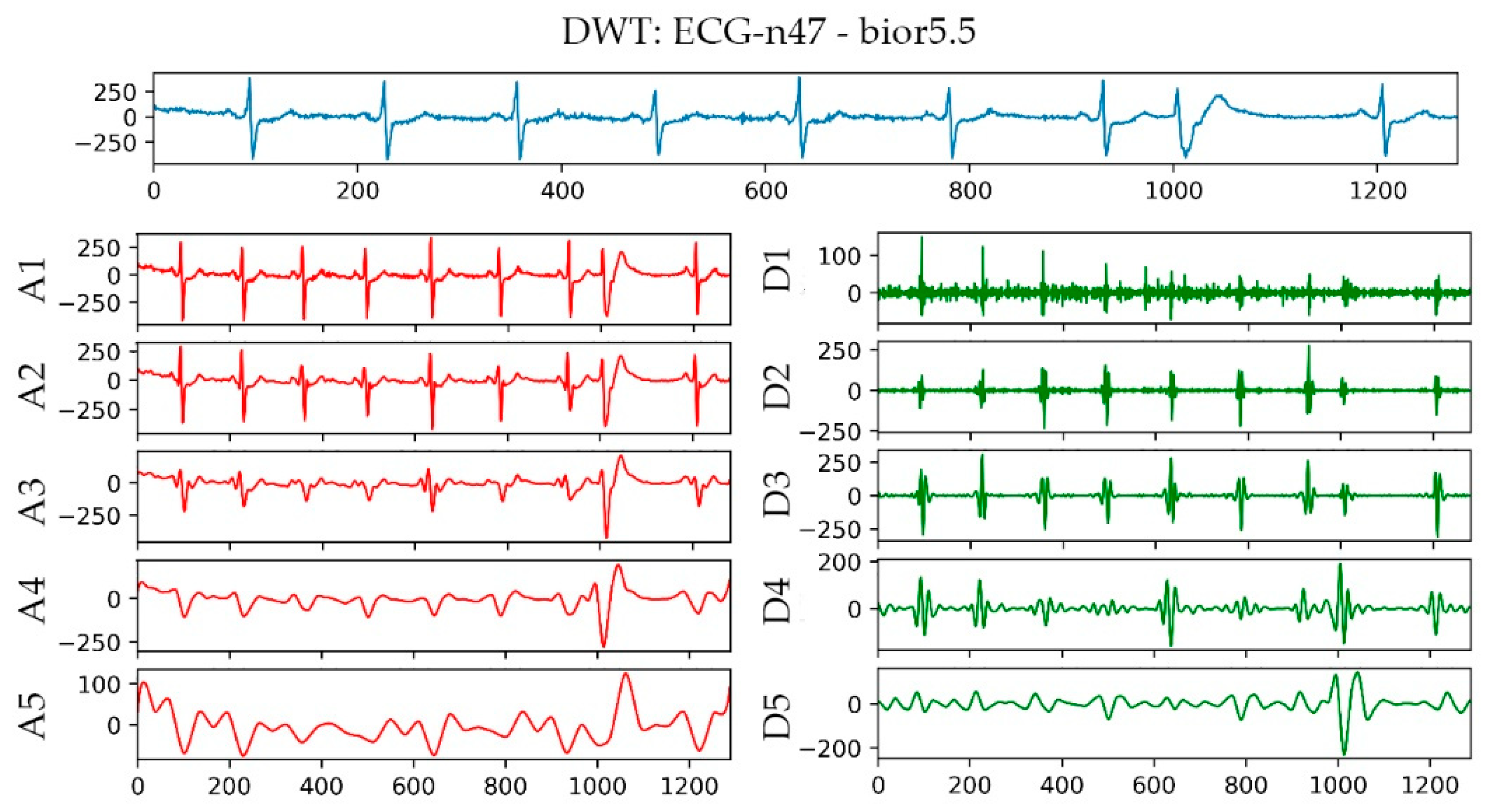
- Choose an appropriate wavelet basis function.
- Decompose the ECG signal into corresponding layers.
- Keep the coefficients decomposed from a specific layer for the next step of processing.
3.3. Construction and Verification of the Atrial Fibrillation Model
3.3.1. Construction of the Atrial Fibrillation Model
3.3.2. Improved Quantum–Particle–Swarm–Optimization Support Vector Machine
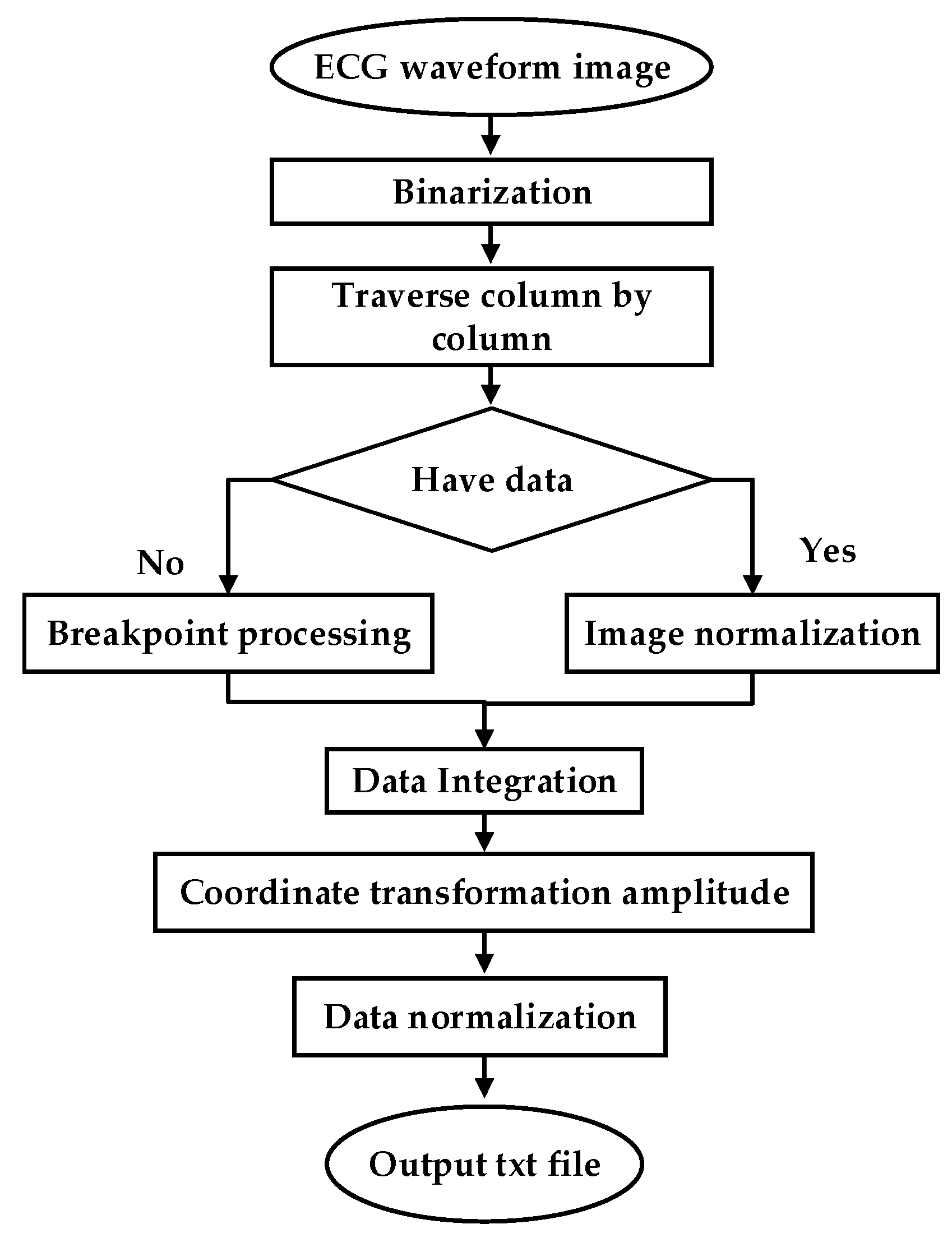
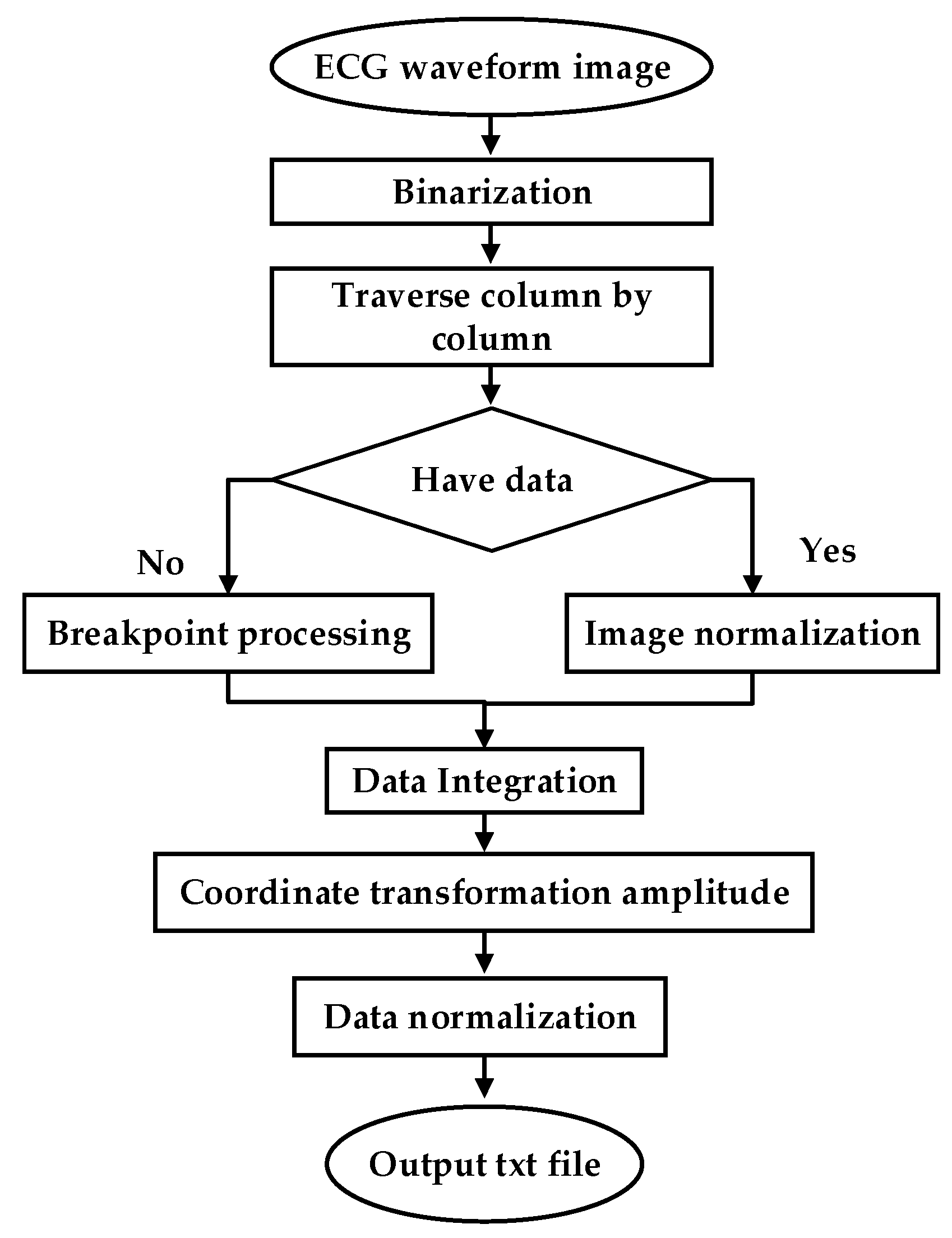
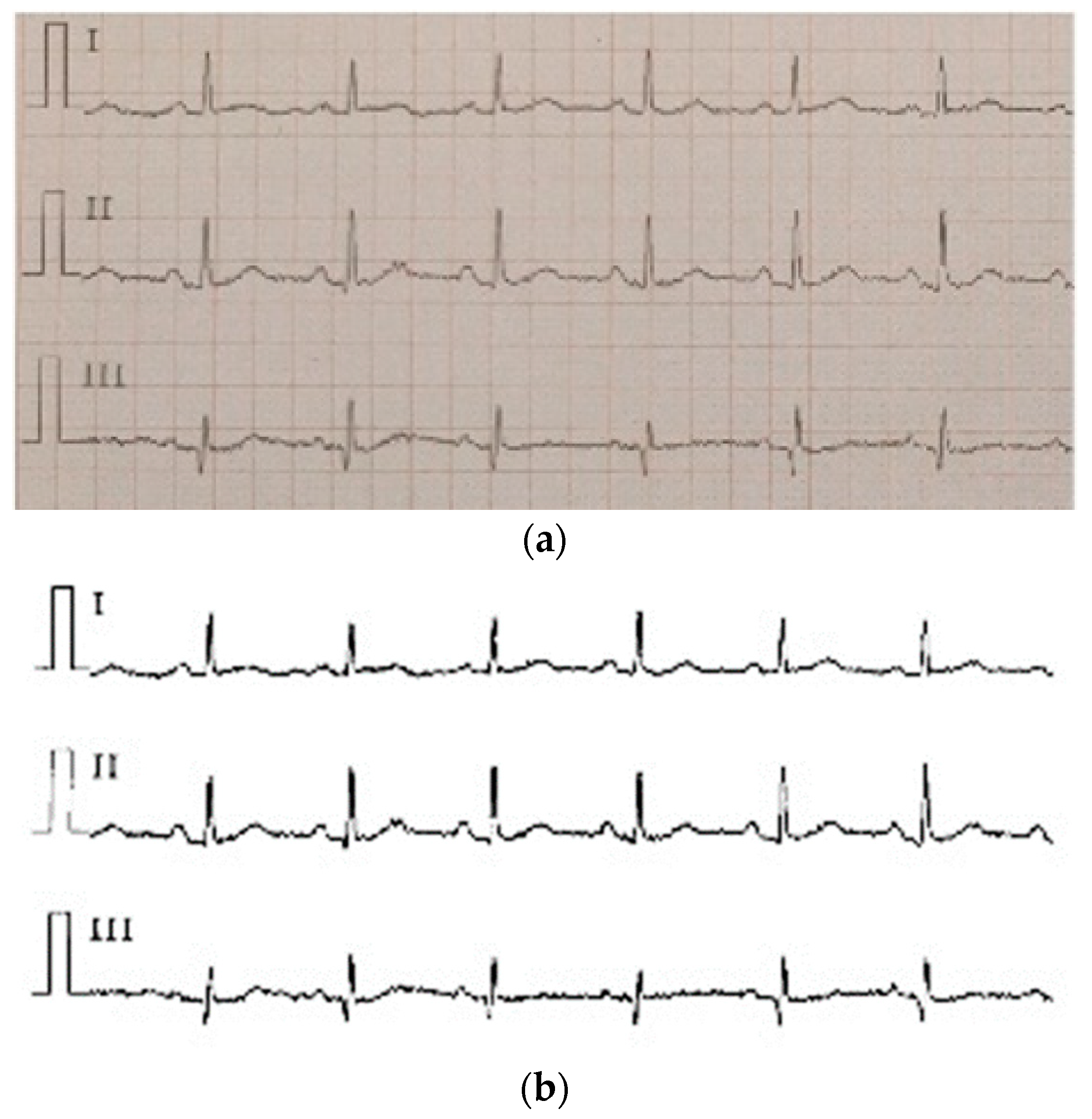
3.3.3. Clinical Image Data to Digital Data
4. Experimental Results and Performance Analysis
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Alonso, A.; Almuwaqqat, Z.; Chamberlain, A. Mortality in atrial fibrillation. Is it changing? Trends Cardiovasc. Med. 2020. [Google Scholar] [CrossRef]
- Margulescu, A.D.; Mont, L. Persistent atrial fibrillation vs paroxysmal atrial fibrillation: Differences in management. Expert Rev. Cardiovasc. Ther. 2017, 15, 601–618. [Google Scholar] [CrossRef] [PubMed]
- Moody, G. A new method for detecting atrial fibrillation using RR intervals. Comput. Cardiol. 1983, 10, 227–230. [Google Scholar]
- Petrucci, E.; Balian, V.; Filippini, G.; Mainardi, L. The use of sequential RR distributions to detect atrial fibrillation episodes in very long term ECG monitoring. In Proceedings of the 2006 Computers in Cardiology, Valencia, Spain, 17–20 September 2006; pp. 945–948. [Google Scholar]
- Tang, W.-H.; Chang, Y.-J.; Chen, Y.J.; Ho, W.-H. Genetic algorithm with Gaussian function for optimal P-wave morphology in electrocardiography for atrial fibrillation patients. Comput. Electr. Eng. 2018, 67, 52–57. [Google Scholar] [CrossRef]
- Nurmaini, S.; Tondas, A.E.; Darmawahyuni, A.; Rachmatullah, M.N.; Umi Partan, R.; Firdaus, F.; Tutuko, B.; Pratiwi, F.; Juliano, A.H.; Khoirani, R. Robust detection of atrial fibrillation from short-term electrocardiogram using convolutional neural networks. Future Gener. Comput. Syst. 2020, 113, 304–317. [Google Scholar] [CrossRef]
- Kennedy, J.; Eberhart, R. Particle swarm optimization. In Proceedings of the ICNN’95-International Conference on Neural Networks, Perth, WA, Australia, 27 November–1 December 1995; pp. 1942–1948. [Google Scholar] [CrossRef]
- Andrikopoulos, G.K.; Dilaveris, P.E.; Richter, D.J.; Gialafos, E.J.; Synetos, A.G.; Gialafos, J.E. Increased variance of P wave duration on the electrocardiogram distinguishes patients with idiopathic paroxysmal atrial fibrillation. Pacing Clin. Electrophysiol. 2000, 23, 1127–1132. [Google Scholar] [CrossRef] [PubMed]
- Lepage, R.; Boucher, J.-M.; Blanc, J.-J.; Cornilly, J.-C. ECG segmentation and P-wave feature extraction: Application to patients prone to atrial fibrillation. In Proceedings of the 2001 Conference Proceedings of the 23rd Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Istanbul, Turkey, 25–28 October 2001; pp. 298–301. [Google Scholar] [CrossRef] [Green Version]
- Abdul-Kadir, N.A.; Safri, N.M.; Othman, M.A. Dynamic ECG features for atrial fibrillation recognition. Comput. Methods Programs Biomed. 2016, 136, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Rubin, J.; Parvaneh, S.; Rahman, A.; Conroy, B.; Babaeizadeh, S. Densely connected convolutional networks for detection of atrial fibrillation from short single-lead ECG recordings. J. Electrocardiol. 2018, 51, S18–S21. [Google Scholar] [CrossRef]
- Attia, Z.I.; Noseworthy, P.A.; Lopez-Jimenez, F.; Asirvatham, S.J.; Deshmukh, A.J.; Gersh, B.J.; Carter, R.E.; Yao, X.; Rabinstein, A.A.; Erickson, B.J. An artificial intelligence-enabled ECG algorithm for the identification of patients with atrial fibrillation during sinus rhythm: A retrospective analysis of outcome prediction. Lancet 2019, 394, 861–867. [Google Scholar] [CrossRef]
- Wang, J. A deep learning approach for atrial fibrillation signals classification based on convolutional and modified Elman neural network. Future Gener. Comput. Syst. 2020, 102, 670–679. [Google Scholar] [CrossRef]
- Cai, W.; Chen, Y.; Guo, J.; Han, B.; Shi, Y.; Ji, L.; Wang, J.; Zhang, G.; Luo, J. Accurate detection of atrial fibrillation from 12-lead ECG using deep neural network. Comput. Biol. Med. 2020, 116, 103378. [Google Scholar] [CrossRef]
- Cao, X.-C.; Yao, B.; Chen, B.-Q. Atrial fibrillation detection using an improved multi-Scale decomposition enhanced residual convolutional neural network. IEEE Access 2019, 7, 89152–89161. [Google Scholar] [CrossRef]
- Erdenebayar, U.; Kim, H.; Park, J.-U.; Kang, D.; Lee, K.-J. Automatic prediction of atrial fibrillation based on convolutional neural network using a short-term normal electrocardiogram signal. J. Korean Med. Sci. 2019, 34, 7. [Google Scholar] [CrossRef]
- Oh, S.L.; Ng, E.Y.; Tan, S.R.; Acharya, U.R. Automated diagnosis of arrhythmia using combination of CNN and LSTM techniques with variable length heart beats. Comput. Biol. Med. 2018, 102, 278–287. [Google Scholar] [CrossRef] [PubMed]
- Andersen, R.S.; Poulsen, E.S.; Puthusserypady, S. A novel approach for automatic detection of Atrial Fibrillation based on Inter Beat Intervals and Support Vector Machine. In Proceedings of the 2017 39th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Jeju Island, Korea, 11–15 July 2017; pp. 2039–2042. [Google Scholar] [CrossRef]
- Gliner, V.; Yaniv, Y. An SVM approach for identifying atrial fibrillation. Physiol. Meas. 2018, 39, 094007. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, A.; Finlay, D.D.; Guldenring, D.; Bond, R.R.; Moran, K.; McLaughlin, J. Automated detection of atrial fibrillation using RR intervals and multivariate-based classification. J. Electrocardiol. 2016, 49, 871–876. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kumar, M.; Pachori, R.B.; Acharya, U. Automated diagnosis of atrial fibrillation ECG signals using entropy features extracted from flexible analytic wavelet transform. Biocybern. Biomed. Eng. 2018, 38, 564–573. [Google Scholar] [CrossRef]
- Pierleoni, P.; Belli, A.; Gentili, A.; Incipini, L.; Palma, L.; Valenti, S.; Raggiunto, S. A eHealth System for Atrial Fibrillation Monitoring. In Proceedings of the Italian Forum of Ambient Assisted Living, Lecce, Italy, 2–4 July 2018; pp. 229–241. [Google Scholar]
- Wrobel, J.; Horoba, K.; Matonia, A.; Kupka, T.; Henzel, N.; Sobotnicka, E. Optimizing the automated detection of atrial fibrillation episodes in long-term recording instrumentation. In Proceedings of the 2018 25th International Conference “Mixed Design of Integrated Circuits and System” (MIXDES), Gdynia, Poland, 21–23 June 2018; pp. 460–464. [Google Scholar]
- Cortes, C.; Vapnik, V. Support-vector networks. Mach. Learn. 1995, 20, 273–297. [Google Scholar] [CrossRef]
- Li, Y.; Tang, X.; Wang, A.; Tang, H. Probability density distribution of delta RR intervals: A novel method for the detection of atrial fibrillation. Australas. Phys. Eng. Sci. Med. 2017, 40, 707–716. [Google Scholar] [CrossRef]
- Czabanski, R.; Horoba, K.; Wrobel, J.; Matonia, A.; Martinek, R.; Kupka, T.; Jezewski, M.; Kahankova, R.; Jezewski, J.; Leski, J.M. Detection of atrial fibrillation episodes in long-term heart rhythm signals using a support vector machine. Sensors 2020, 20, 765. [Google Scholar] [CrossRef] [Green Version]
- Nuryani, N.; Harjito, B.; Yahya, I.; Lestari, A. Atrial fibrillation detection using support vector machine. In Proceedings of the Joint International Conference on Electric Vehicular Technology and Industrial, Mechanical, Electrical and Chemical Engineering (ICEVT & IMECE), Surakarta, Indonesia, 4–5 November 2015; pp. 215–218. [Google Scholar] [CrossRef]
- Meyer, D.; Leisch, F.; Hornik, K.J.N. The support vector machine under test. Neurocomputing 2003, 55, 169–186. [Google Scholar] [CrossRef]
- Nuryani, N.; Harjito, B.; Yahya, I.; Solikhah, M.; Chai, R.; Lestari, A. Atrial fibrillation detection using support vector machine and electrocardiographic descriptive statistics. Int. J. Biomed. Eng. Technol. 2017, 24, 225–236. [Google Scholar] [CrossRef]
- Duin, R.P. Classifiers in almost empty spaces. In Proceedings of the Proceedings 15th International Conference on Pattern Recognition. ICPR-2000, Barcelona, Spain, 3–7 September 2000; pp. 1–7. [Google Scholar] [CrossRef]
- Moody, G.B.; Mark, R.G. The impact of the MIT-BIH Arrhythmia Database. IEEE Eng. Med. Biol. Mag. 2001, 20, 45–50. [Google Scholar] [CrossRef]
- Goldberger, A.; Amaral, L.A.; Glass, L.; Hausdorff, J.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. Components of a New Research Resource for Complex Physiologic Signals; American Heart Association: Dallas, TX, USA, 2000; Volume 101, Issue 23. [Google Scholar]
- Moody, G.; Goldberger, A.L.; McClennen, S.; Swiryn, S.P. Predicting the onset of paroxysmal atrial fibrillation: The Computers in Cardiology Challenge 2001. In Proceedings of the Computers in Cardiology, Rotterdam, The Netherlands, 23–26 September 2001; Volume 28 (Cat. No. 01CH37287), pp. 113–116. [Google Scholar] [CrossRef]
- Fan, M.-H.; Guan, M.-H.; Chen, Q.-C.; Wang, L.-H. Three-lead ECG detection system based on an analog front-end circuit ADS1293. In Proceedings of the 2017 IEEE International Conference on Consumer Electronics-Taiwan (ICCE-TW), Taipei, Taiwan, 12–14 June 2017; pp. 107–108. [Google Scholar] [CrossRef]
- Wang, L.-H.; Chen, T.-Y.; Lin, K.-H.; Fang, Q.; Lee, S.-Y. Implementation of a wireless ECG acquisition SoC for IEEE 802.15. 4 (ZigBee) applications. IEEE J. Biomed. Health Inform. 2014, 19, 247–255. [Google Scholar] [CrossRef]
- Pan, J.; Tompkins, W.J. A real-time QRS detection algorithm. IEEE Trans. Biomed. Eng. 1985, 230–236. [Google Scholar] [CrossRef]
- Tateno, K.; Glass, L. Automatic detection of atrial fibrillation using the coefficient of variation and density histograms of RR and ΔRR intervals. Med. Biol. Eng. Comput. 2001, 39, 664–671. [Google Scholar] [CrossRef]
- Otsu, N. A threshold selection method from gray-level histograms. IEEE Trans. Syst. Man Cybern. 1979, 9, 62–66. [Google Scholar] [CrossRef] [Green Version]
- Boon, K.H.; Khalil-Hani, M.; Malarvili, M.; Sia, C.W. Paroxysmal atrial fibrillation prediction method with shorter HRV sequences. Comput. Methods Programs Biomed. 2016, 134, 187–196. [Google Scholar] [CrossRef]
- Costin, H.; Rotariu, C.; Păsărică, A. Atrial fibrillation onset prediction using variability of ECG signals. In Proceedings of the 2013 8th International Symposium on Advanced Topics in Electrical Engineering (ATEE), Bucharest, Romania, 23–25 May 2013; pp. 1–4. [Google Scholar] [CrossRef]
- Mohebbi, M.; Ghassemian, H. Prediction of paroxysmal atrial fibrillation based on non-linear analysis and spectrum and bispectrum features of the heart rate variability signal. Comput. Methods Programs Biomed. 2012, 105, 40–49. [Google Scholar] [CrossRef]
- Boon, K.H.; Khalil-Hani, M.; Malarvili, M. Paroxysmal atrial fibrillation prediction based on HRV analysis and non-dominated sorting genetic algorithm III. Comput. Methods Programs Biomed. 2018, 153, 171–184. [Google Scholar] [CrossRef] [PubMed]
- Xin, Y.; Zhao, Y. Paroxysmal atrial fibrillation recognition based on multi-scale wavelet alpha-entropy. Biomed. Eng. Online 2017, 16, 121. [Google Scholar] [CrossRef] [Green Version]
- Ebrahimzadeh, E.; Maede, K.; Joulani, M.; Shahraki, R.S.; Fayaz, F.; Ahmadi, F. Prediction of paroxysmal Atrial Fibrillation: A machine learning based approach using combined feature vector and mixture of expert classification on HRV signal. Comput. Methods Programs Biomed. 2018, 165, 53–67. [Google Scholar] [CrossRef]
- Parsi, A.; Glavin, M.; Jones, E.; Byrne, D. Prediction of Paroxysmal Atrial Fibrillation using New Heart Rate Variability Features. Comput. Biol. Med. 2021, 133, 104367. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Works | Year | Model | Features | Methods |
|---|---|---|---|---|
| Abdul-Kadir et al. [10] | 2016 | ANN | ECG features | Deep learning method |
| Rubin et al. [11] | 2018 | CNN | ECG records | Deep learning method |
| Attia et al. [12] | 2019 | CNN | ECG records | Deep learning method |
| Wang [13] | 2020 | CNN/ENN | ECG records | Deep learning method |
| Cai et al. [14] | 2020 | DDNN | ECG records | Deep learning method |
| Cao et al. [15] | 2020 | ResNet | ECG records | Deep learning method |
| Li et al. [25] | 2017 | SVM | RR interval | Traditional machine learning method |
| Czabanski et al. [26] | 2020 | LSVM | HRV | Traditional machine learning method |
| Nuryani et al. [27] | 2015 | SVM | RR interval | Traditional machine learning method |
| Nuryani et al. [29] | 2017 | SVM | RR interval | Traditional machine learning method |
| Algorithm Class | Feature Group | Characterization |
|---|---|---|
| Atrial fibrillation diagnosis algorithm | Time domain characteristics | RR_std, RR_mean, RR_max, RR_rms RR_cha, RR_len |
| Atrial fibrillation prediction algorithm | Time domain characteristics | RR_std, RR_mean, RR_max, RR_rms, RR_cha, RR_len, PR, Pamp |
| Frequency domain characteristics | ca1,ca2,ca3 cd1,cd2,cd3 |
| Features | Impact |
|---|---|
| Pamp | 0.268804 |
| cd3 | 0.220801 |
| RR_std | 0.107348 |
| ca3 | 0.087449 |
| RR_cha | 0.081577 |
| PR | 0.065737 |
| RR_max | 0.058773 |
| ca2 | 0.027738 |
| cd1 | 0.021885 |
| RR_rms | 0.018379 |
| cd2 | 0.018140 |
| RR_len | 0.012802 |
| ca1 | 0.010556 |
| Cross-Validation | Grid Search | IQPSO-SVM | ||
|---|---|---|---|---|
| Accuracy | Time(s) | Accuracy | Time(s) | |
| 3-fold | 0.9836 ± 0.0037 | 1137.865 ± 5.312 | 0.9860 ± 0.0018 | 125.126 ± 1.012 |
| 5-fold | 0.9810 ± 0.0011 | 1558.365 ± 6.352 | 0.9847 ± 0.0009 | 156.344 ± 2.895 |
| 10-fold | 0.9835 ± 0.0033 | 7550.963 ± 5.813 | 0.9879 ± 0.0010 | 363.591 ± 3.552 |
| AF | N | |
|---|---|---|
| AF | 357 | 3 |
| N | 3 | 357 |
| PAF | N | |
|---|---|---|
| PAF | 57 | 3 |
| N | 4 | 56 |
| PAF | N | |
|---|---|---|
| PAF | 65 | 4 |
| N | 8 | 61 |
| N | PAF | AF | |
|---|---|---|---|
| N | 35 | 5 | 0 |
| PAF | 2 | 37 | 1 |
| AF | 0 | 1 | 39 |
| Performance of Atrial Fibrillation Classification Models in the AFDB Test Set. | ||||
|---|---|---|---|---|
| SE | SP | ACC | ||
| AFDB Test Set | AF | 99.2% | 99.2% | 99.2% |
| AFPDB Test Set | PAF | 93.3% | 91.7% | 92.5% |
| FZU-FPH Clinical Test Set of Two Labels | PAF | 94.2% | 79.7% | 87.0% |
| FZU-FPH Clinical Test Set of Three Labels | PAF | 92.5% | 90% | 90.8% |
| AF | 97.5% | 98.8% | 98.3% | |
| N | PAF | AF | |
|---|---|---|---|
| N | NN | NPAF | NAF |
| PAF | PAFN | PAFPAF | PAFAF |
| AF | AFN | AFPAF | AFAF |
| Works | Characteristic | Methods/Database | SE | SP | ACC |
|---|---|---|---|---|---|
| This work | RRI | SVM/AFDB | 99.2% | 99.2% | 99.2% |
| Tateno et al. [37] | RRI | Coefficient of Variation/AFDB | 94.4% | 97.2% | ------ |
| Li et al. [25] | RRI | LSVM/AFDB | 95.9% | 95.3% | 96.3% |
| Kumar et al. [21] | ECG features | Random forest/AFDB | 95.8% | 97.8% | 96.8% |
| Andersen et al. [18] | RRI ECG features | SVM/AFDB | 96.81% | 96.20% | 96.45% |
| Czabanski et al. [26] | HR features | LSVM/AFDB | 98.94% | 98.39% | 98.66% |
| Andrikopoulos et al. [8] | P wave | Statistical methods/Self-built database | 88% | 75% | ------ |
| Lepage et al. [9] | P wave | Markov Models/Self-built database | 70% | 65% | ------ |
| Nurmaini et al. [6] | RRI P wave | CNN DWT/AFDB | 99.91% | 99.91% | 99.98% |
| Works | Signal Length (min) | Feature/Methods/Database | SE | SP | ACC |
|---|---|---|---|---|---|
| This work (AFPDB) | 5 | P wave RRI/SVM/AFPDB | 93.3% | 91.7% | 92.5% |
| This work (FZU-FPH) | 5 | P wave RRI/SVM/FZU-FPH | 94.2% | 79.7% | 87.0% |
| Costin et al. [40] | 30 | HRV and PACs /Statistical analysis/AFPDB | 89.3% | 89.4% | 89.4% |
| Mohebbi et al. [41] | 30 | HRV/SVM/AFPDB | 96.2% | 93.1% | 94.5% |
| Boon et al. [39] | 30 | HRV/SVM/AFPDB | 81.1% | 79.3% | 80.2% |
| Xin et al. [43] | 5 | HRV multi-scale wavelet entropy/SVM/AFPDB | 92.18% | 94.88% | 89.48% |
| Boon et al. [42] | 5 | HRV/SVM/AFPDB | 86.8% | 88.7% | 87.7% |
| Elias et al. [44] | 5 | HRV/ME/AFPDB | 100% | 95.55% | 98.21% |
| Parsi et al. [45] | 5 | HRV/SVM/AFPDB | 98.8% | 96.7% | 97.7% |
| Attia et al. [12] | ---- | …/CNN/Self-built database | 82.3% | 83.4% | 83.3% |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, L.-H.; Yan, Z.-H.; Yang, Y.-T.; Chen, J.-Y.; Yang, T.; Kuo, I.-C.; Abu, P.A.R.; Huang, P.-C.; Chen, C.-A.; Chen, S.-L. A Classification and Prediction Hybrid Model Construction with the IQPSO-SVM Algorithm for Atrial Fibrillation Arrhythmia. Sensors 2021, 21, 5222. https://doi.org/10.3390/s21155222
Wang L-H, Yan Z-H, Yang Y-T, Chen J-Y, Yang T, Kuo I-C, Abu PAR, Huang P-C, Chen C-A, Chen S-L. A Classification and Prediction Hybrid Model Construction with the IQPSO-SVM Algorithm for Atrial Fibrillation Arrhythmia. Sensors. 2021; 21(15):5222. https://doi.org/10.3390/s21155222
Chicago/Turabian StyleWang, Liang-Hung, Ze-Hong Yan, Yi-Ting Yang, Jun-Ying Chen, Tao Yang, I-Chun Kuo, Patricia Angela R. Abu, Pao-Cheng Huang, Chiung-An Chen, and Shih-Lun Chen. 2021. "A Classification and Prediction Hybrid Model Construction with the IQPSO-SVM Algorithm for Atrial Fibrillation Arrhythmia" Sensors 21, no. 15: 5222. https://doi.org/10.3390/s21155222
APA StyleWang, L.-H., Yan, Z.-H., Yang, Y.-T., Chen, J.-Y., Yang, T., Kuo, I.-C., Abu, P. A. R., Huang, P.-C., Chen, C.-A., & Chen, S.-L. (2021). A Classification and Prediction Hybrid Model Construction with the IQPSO-SVM Algorithm for Atrial Fibrillation Arrhythmia. Sensors, 21(15), 5222. https://doi.org/10.3390/s21155222